Pathology Module 2 Lab
1/92
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
93 Terms
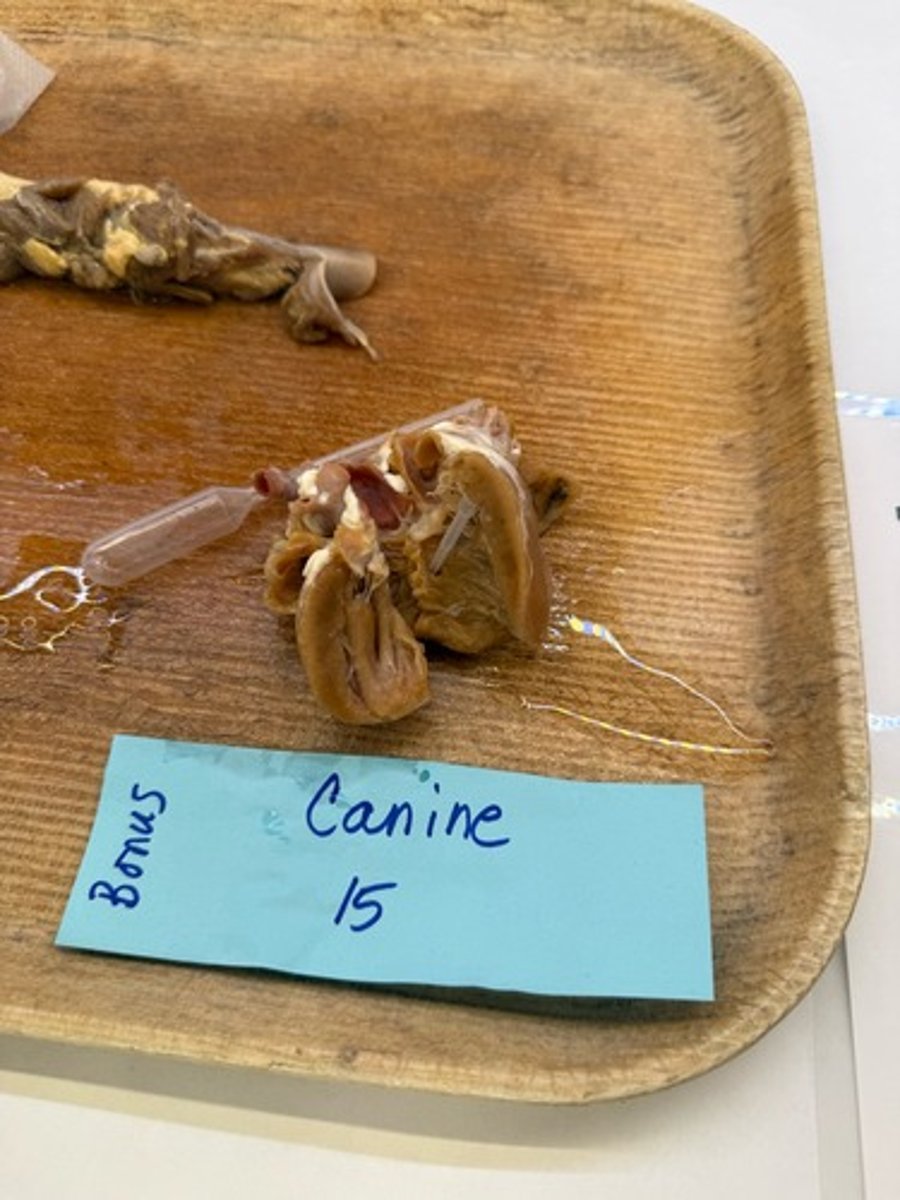
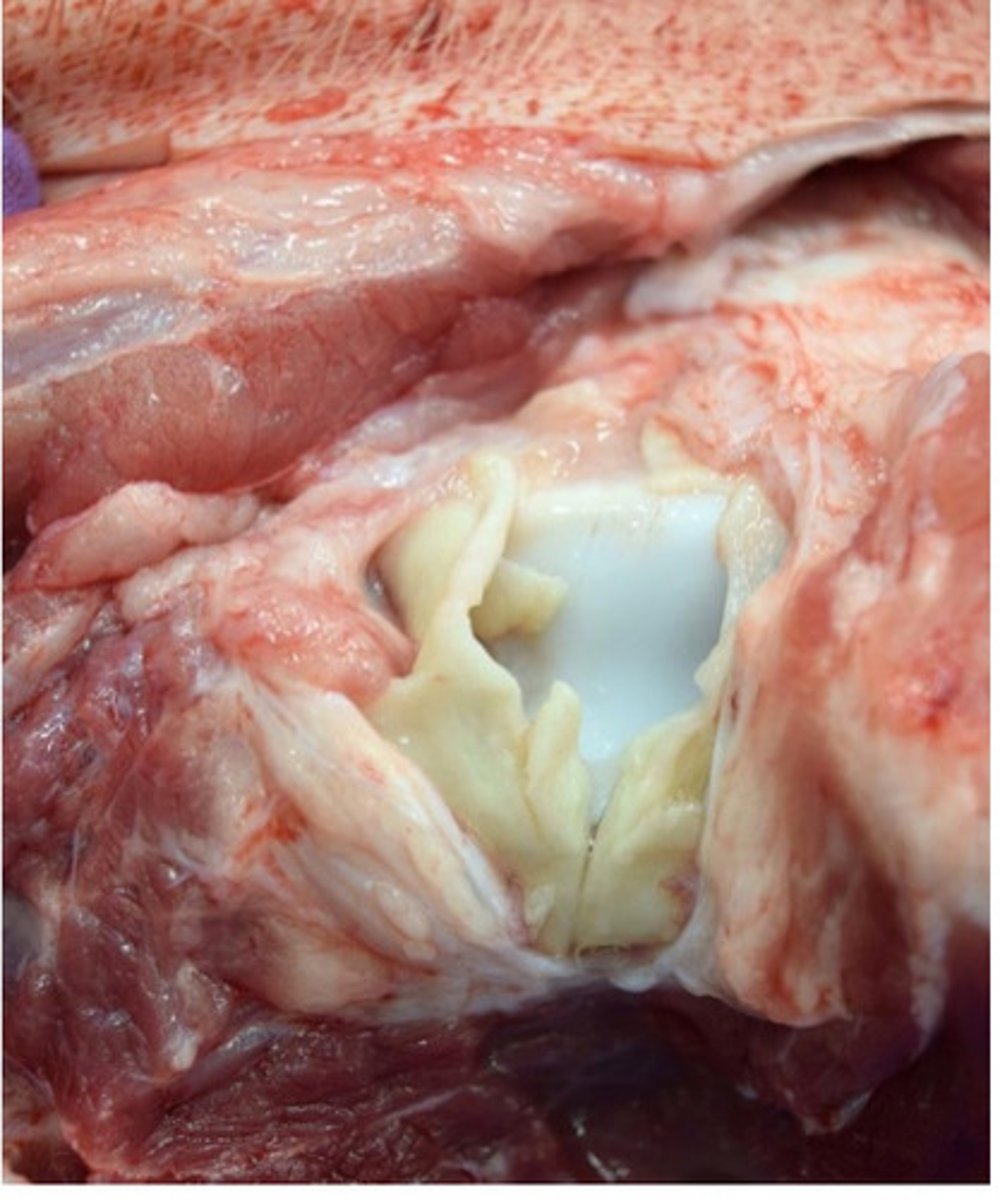
Endocarditis
Inflammation of heart valves
Initiated by bacteremia
Sequelae: septic thromboembolism leading to multi-organ infarction
*endothelial injury —> turbulent blood flow —> thrombus formation
What is this lesion?
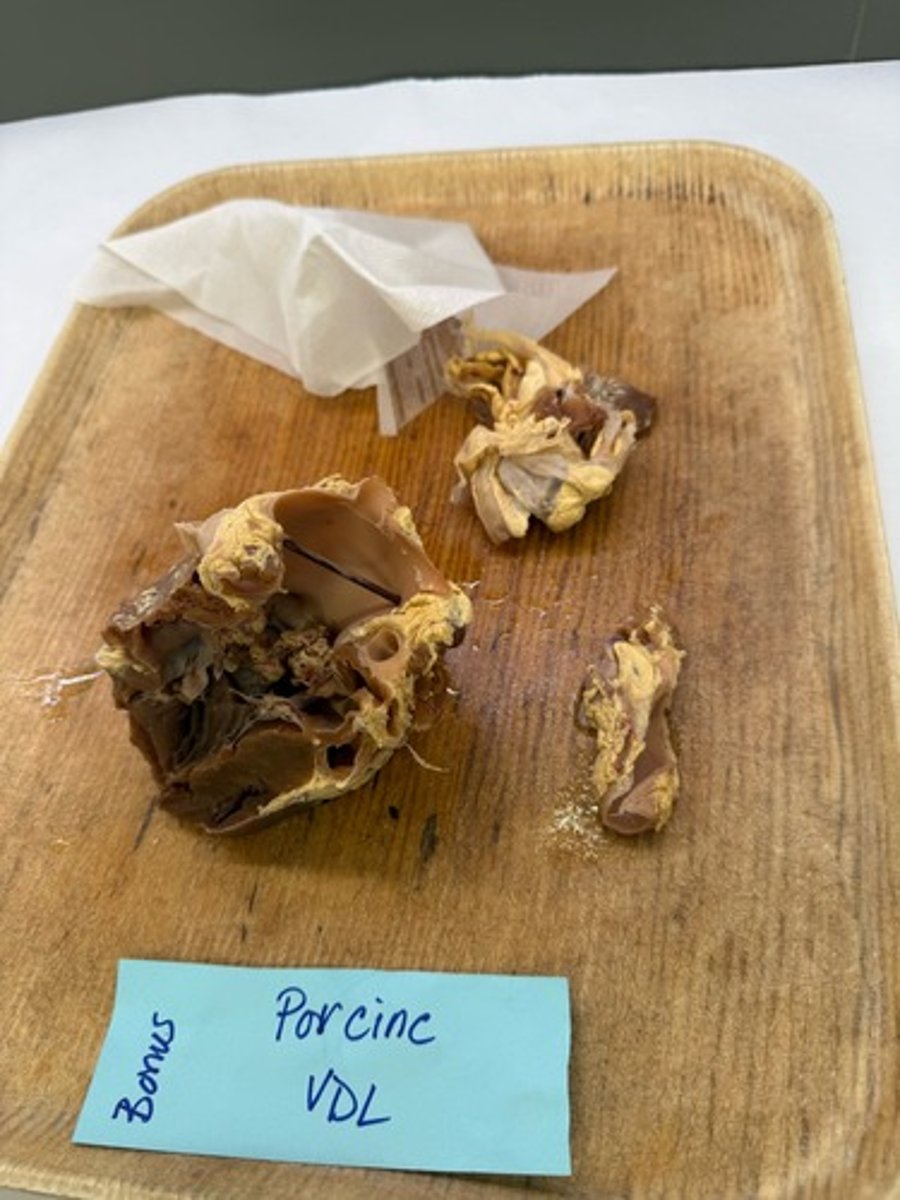
Endocarditis
Thickening of heart valves
Sequelae: thromboembolism, valvular regurgitation, l side heart failure
How it occurs: endothelial injury from mechanical jetting of blood —> abnormal blood flow/turbulence arising from valvular regurgitation —> thrombus
What is this lesion?
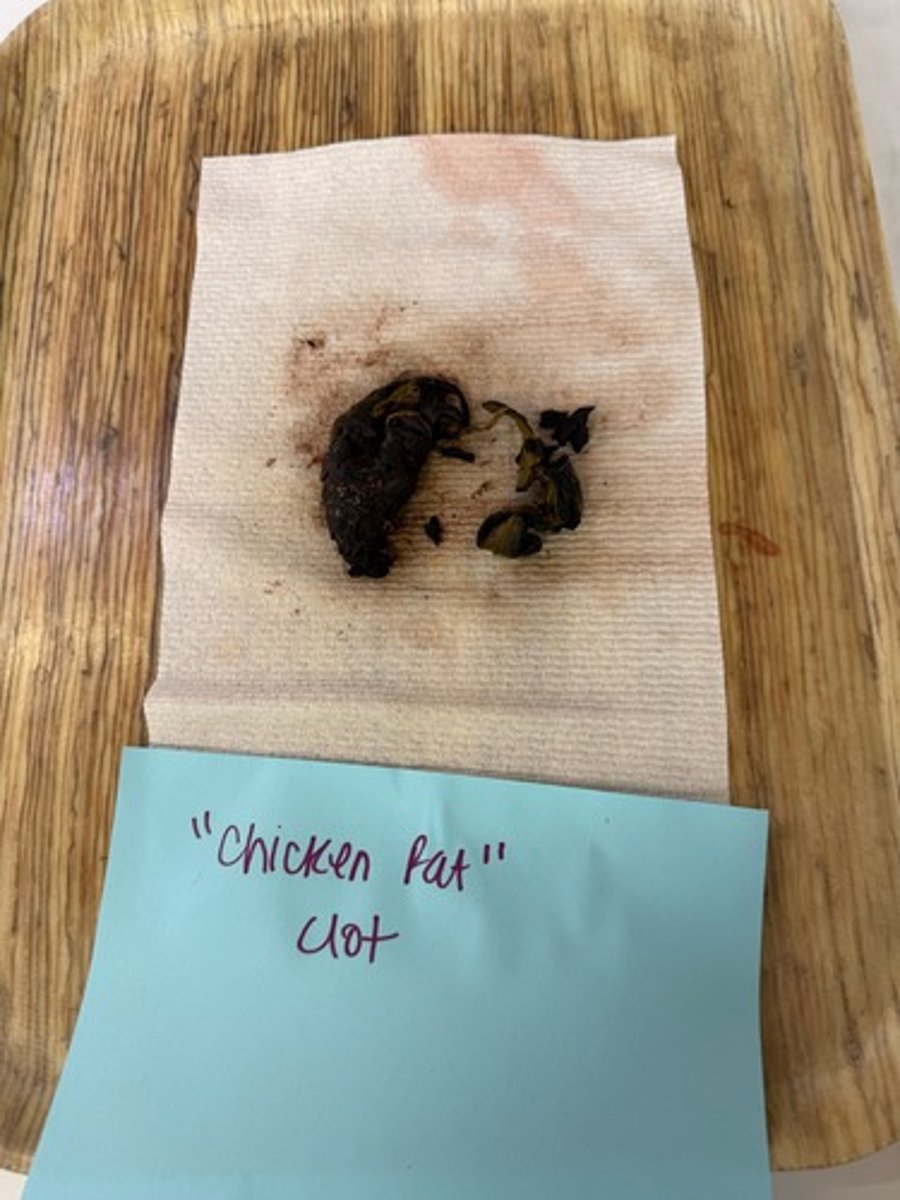
Chicken fat clot
What is this lesion?
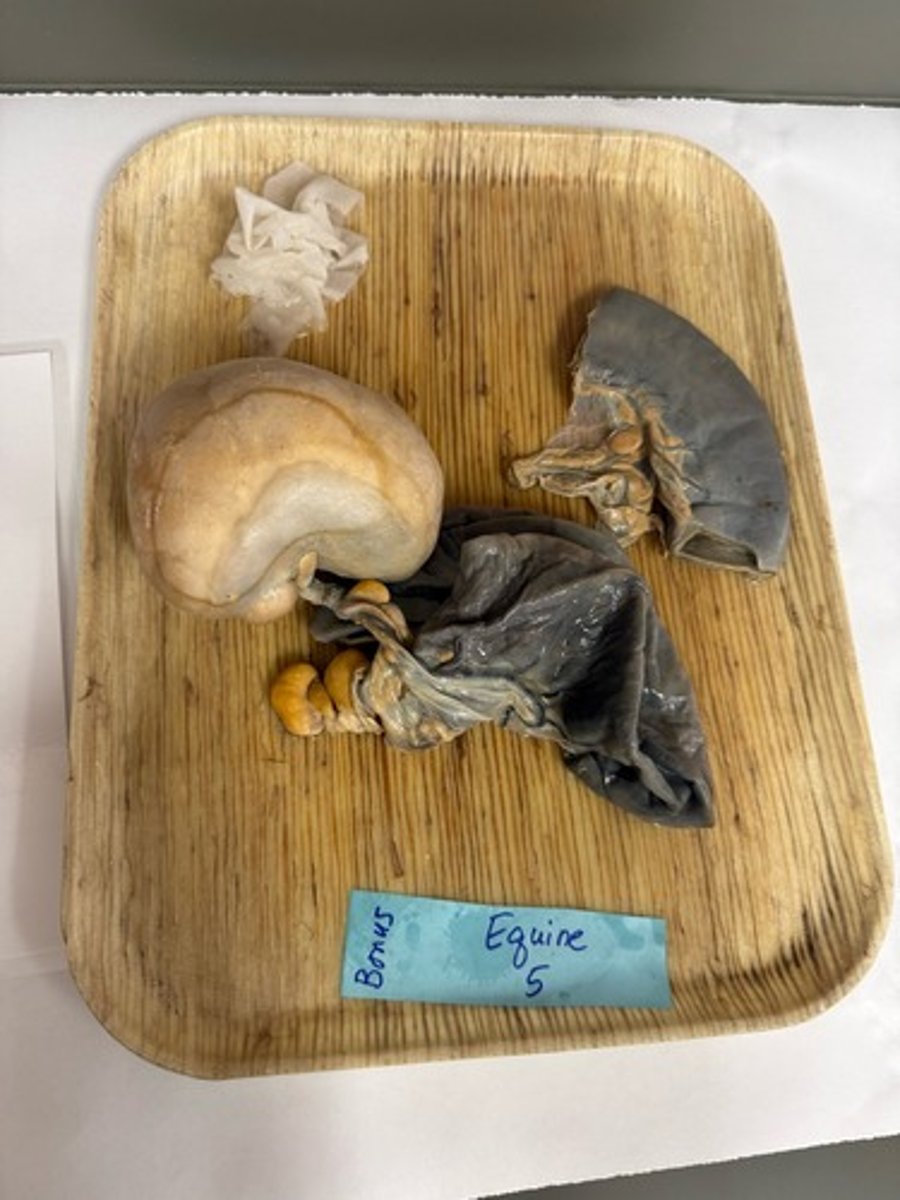
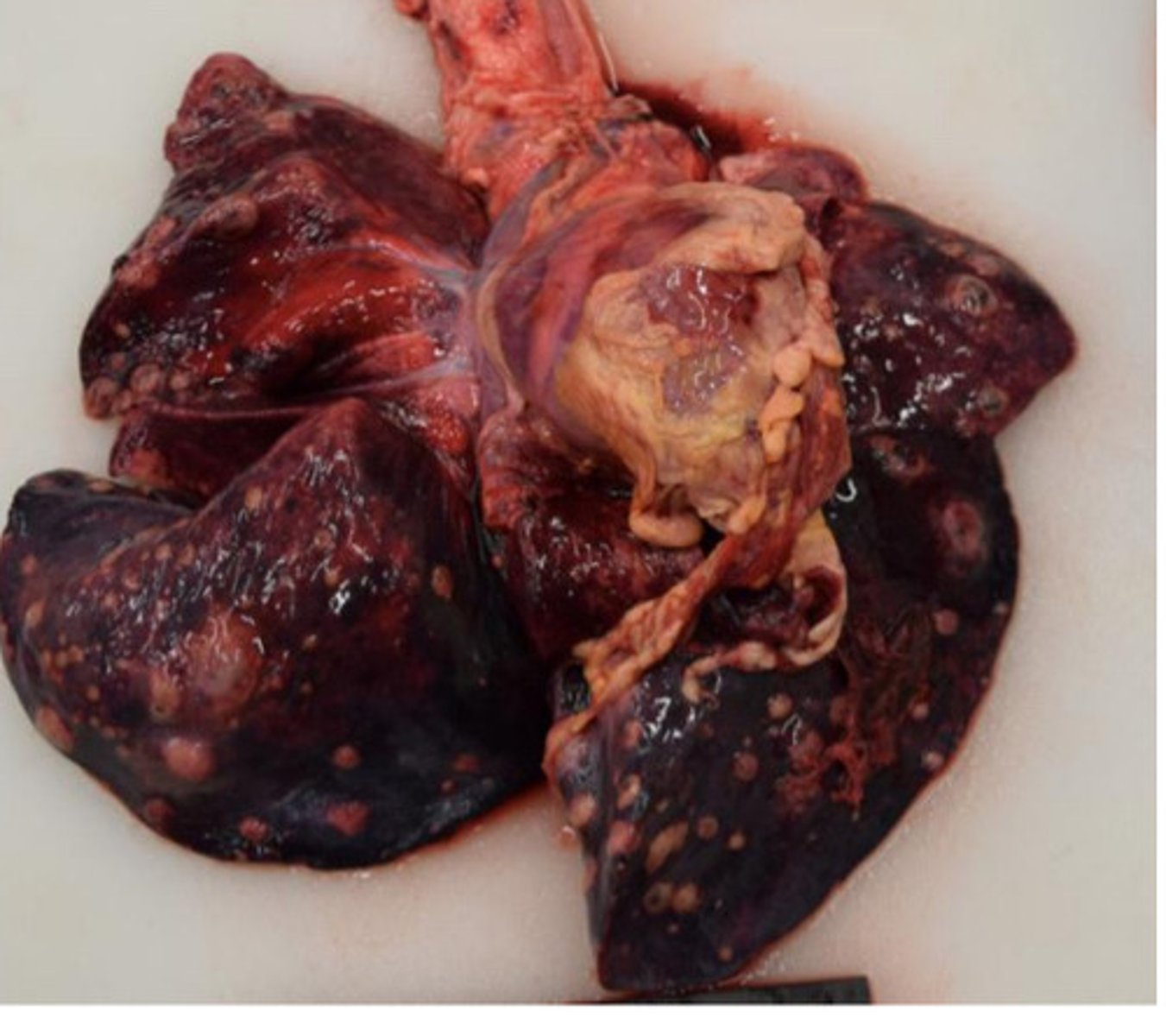
Lung lobe torsion
Lung lobe wrapped around hilus
Occludes venous return and lymphatic drainage, arterial inflow continues
Pulmonary venous congestion and edema
Blood supply is restricted (ischemia) leading to hypoxia and eventually necrosis (venous infarction)
What is this lesion?
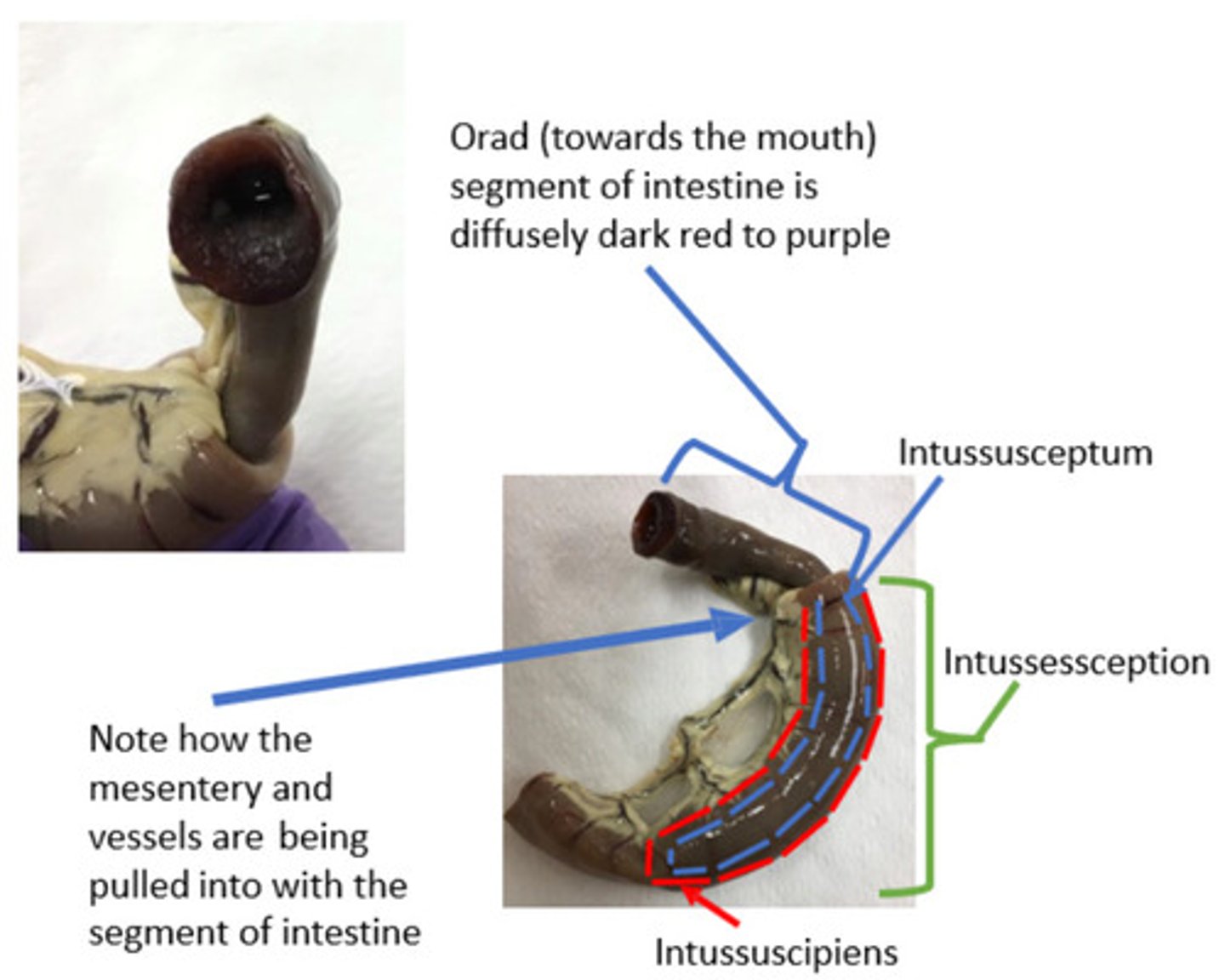
Intestinal intussusception
Venous congestion, edema, venous infarction
What is this lesion?

Whats the lesion?

Strangulating lipoma
Benign mesenteric fat tumor, loops around a segment of small intestine
Constricts bowel and blood supply
Venous congestion and venous infarction
Whats the lesion?
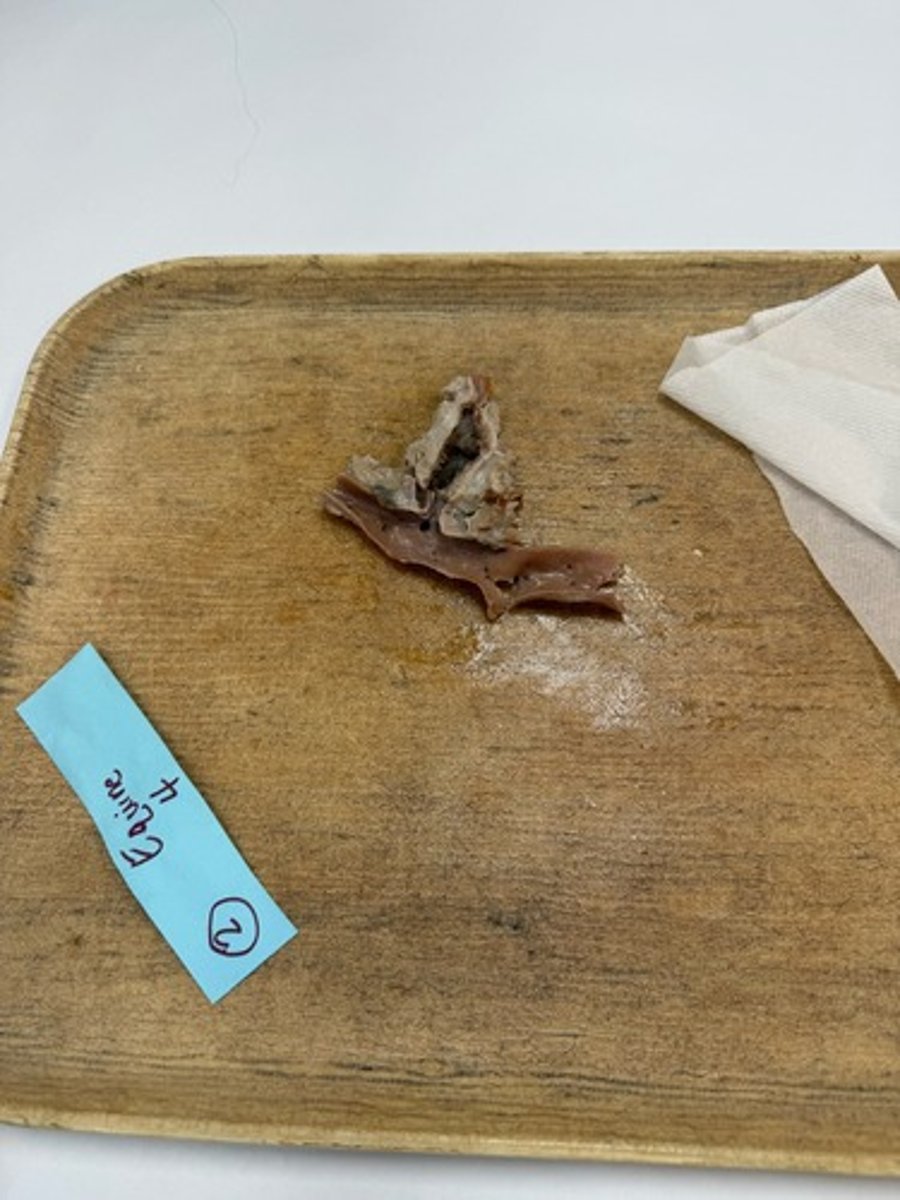
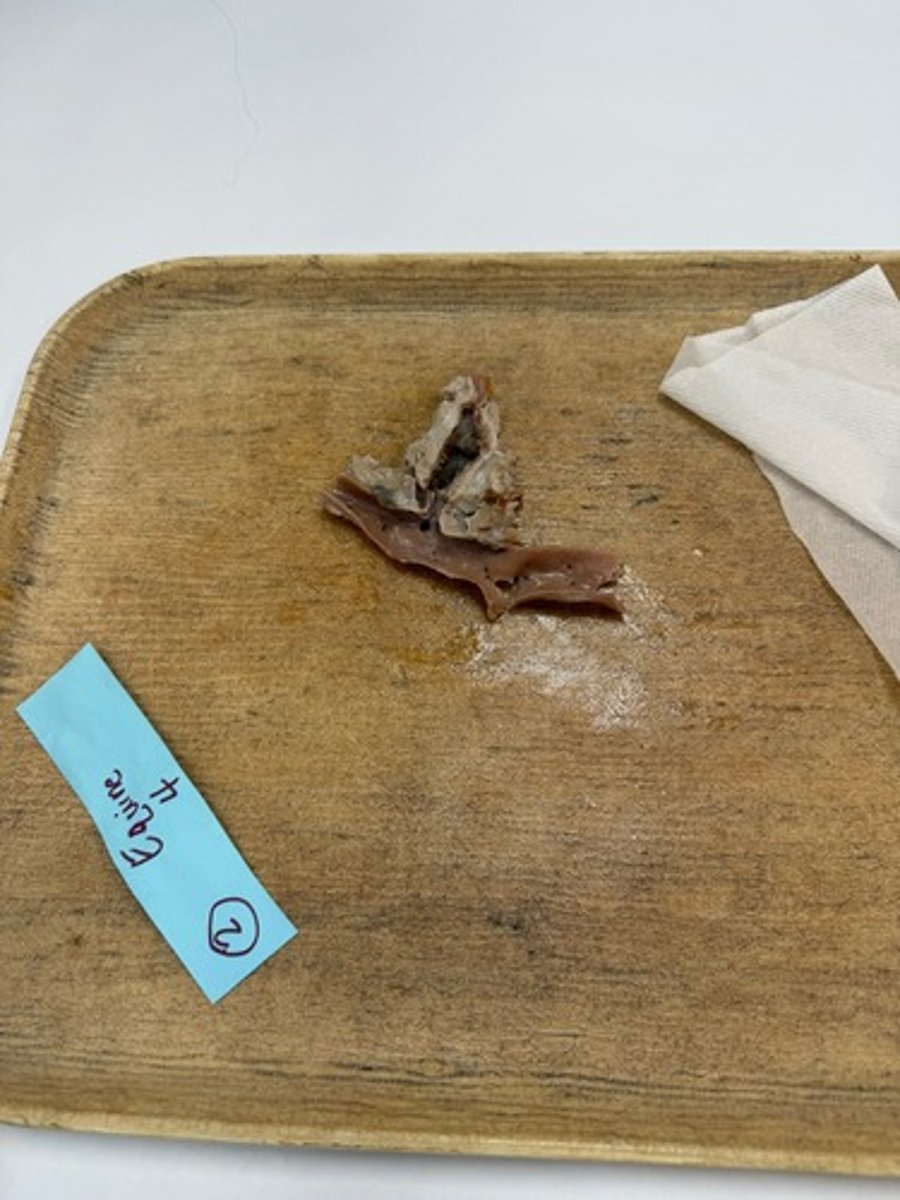
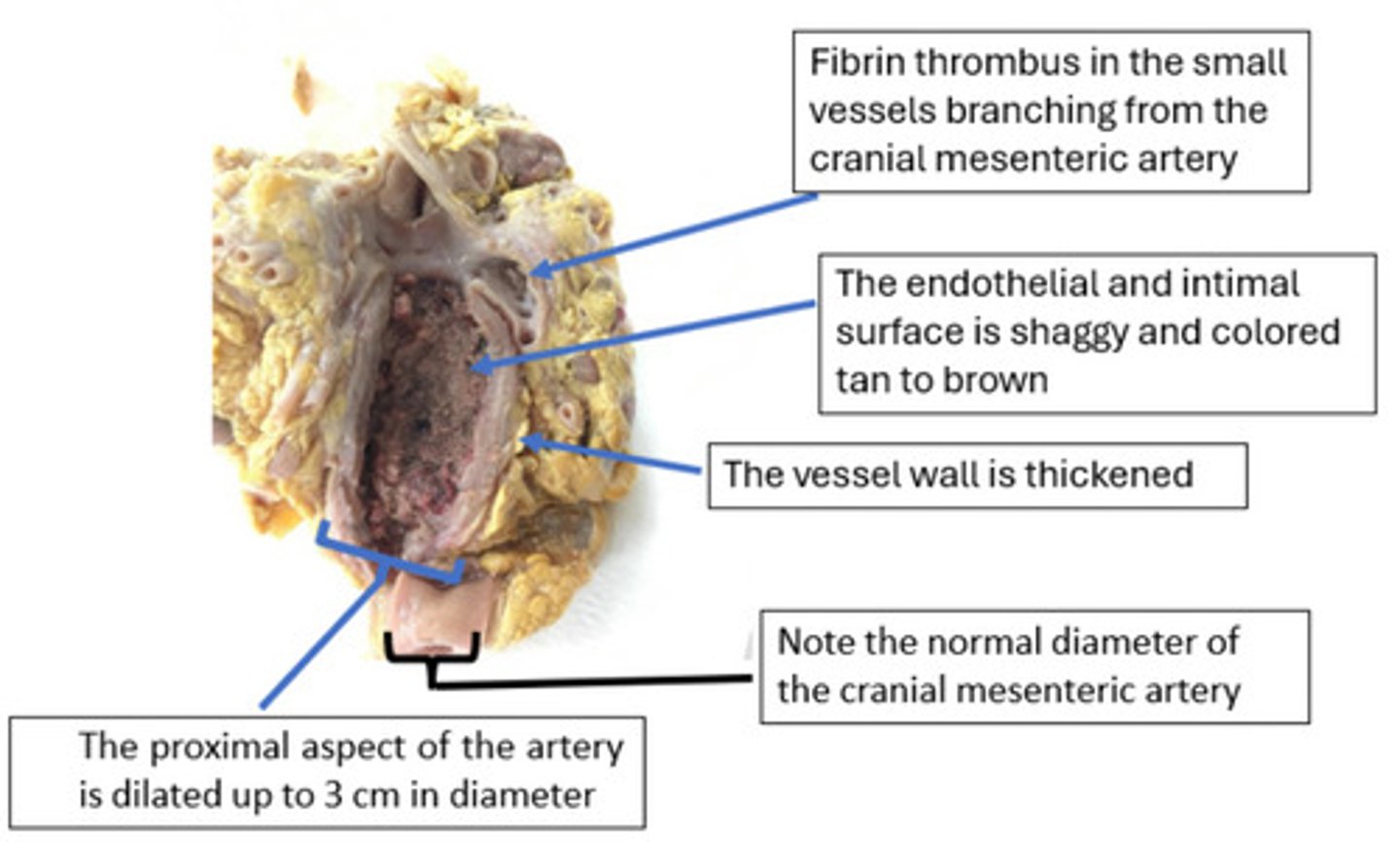
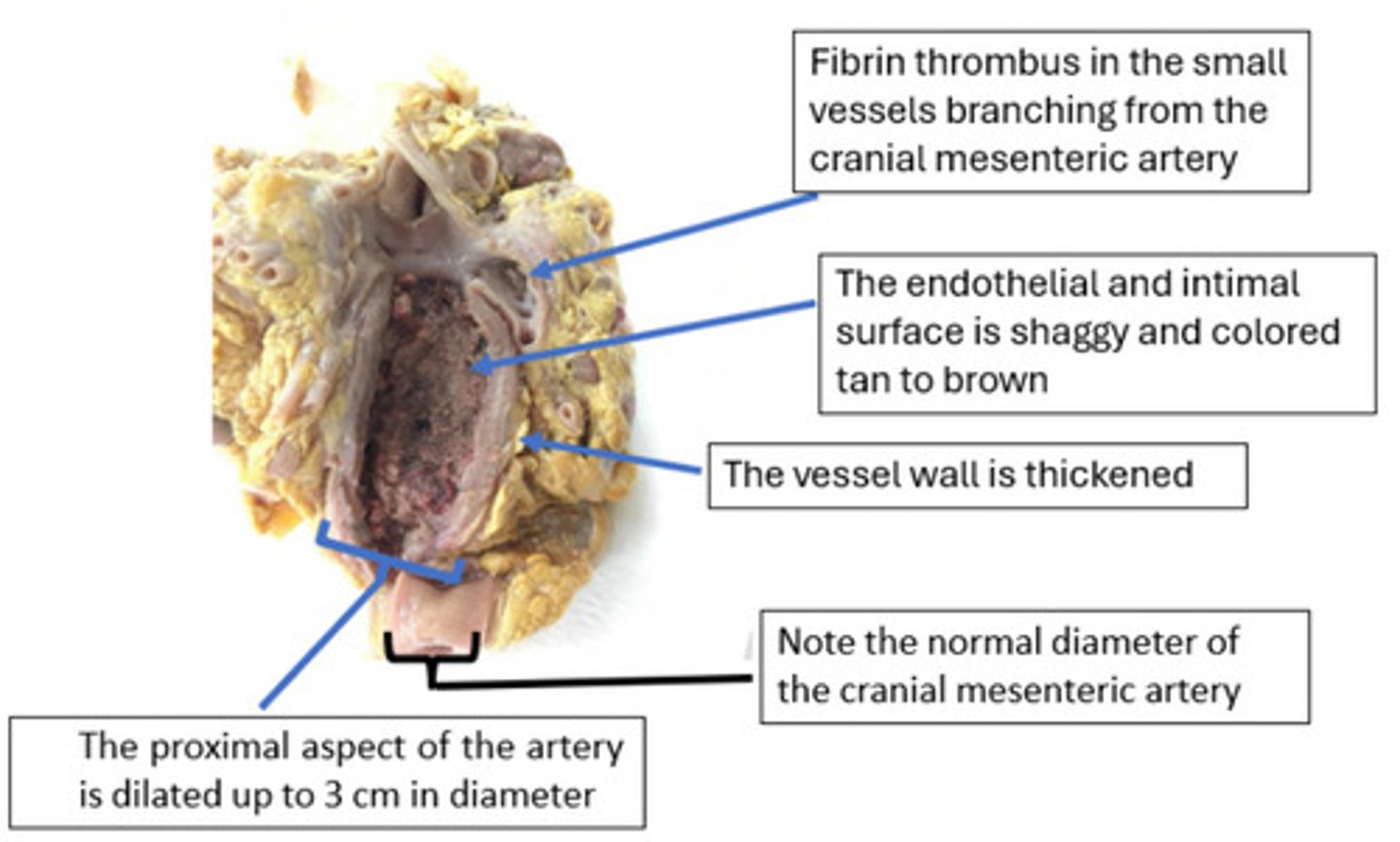
This lesion is consistent with cranial mesenteric arteritis due to Strongylus vulgaris larvae. L4 (one of the stages of development) larvae of Strongylus vulgaris migrate through the intimal layer of the cranial mesenteric artery. The migration through the artery results in endothelium damage (inflammation /arteritis) as well as proliferation of the intimal layer and endothelium of the artery.
Migration of S. vulgaris larvae through the Cr. Mesenteric artery à endothelial damage and inflammation à vWF released and coats exposed collagen à platelet adhesion to vWF à TF released and subendothelial TF exposed à TF initiates the extrinsic coagulation cascade à Fibrin polymerization of the aggregated platelets à fibrin thrombus
The rapid flow through the cranial mesenteric artery tends to exclude most erythrocytes, making the thrombi appear red-gray or tan
How did this lesion develop?
Fibrin Thrombus
What is the lesion?
Fibrin thrombus
What is the lesion?
The significance of the thrombus is determined by its ability to disrupt perfusion to the intestines. Thromboembolism is when portions of the mural thrombus (the "tail") can break loose and enter the circulation as thromboemboli. These emboli travel downstream and lodge in smaller end-arteries of the intestinal segments. This sudden vascular occlusion leads to acute hemorrhagic infarction of the bowel, which is a major cause of severe colic and death in affected horses.
While modern deworming regimens have made this condition less common, the damage can act as a "ticking time bomb," where clinical symptoms or vascular accidents occur long after the initial larval insult
What is the significance of this lesion?
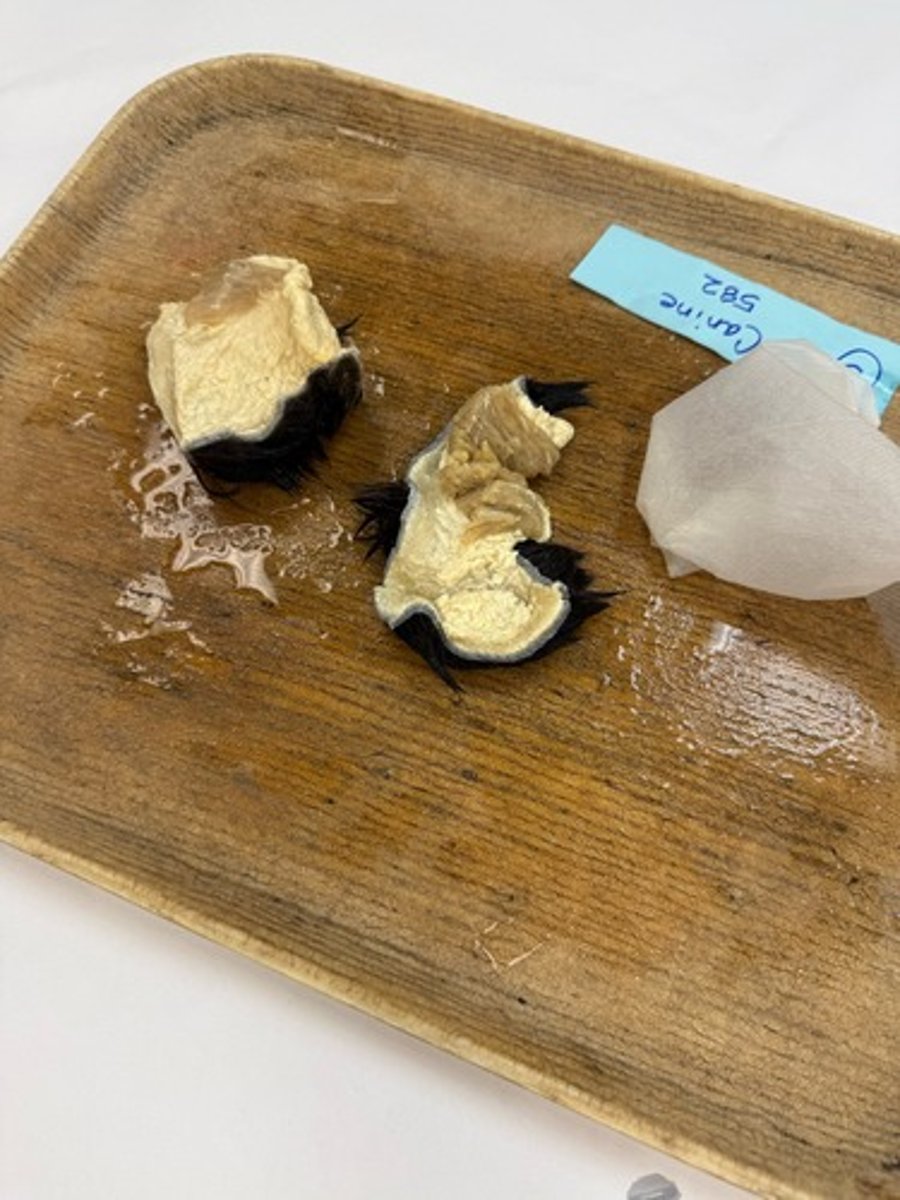
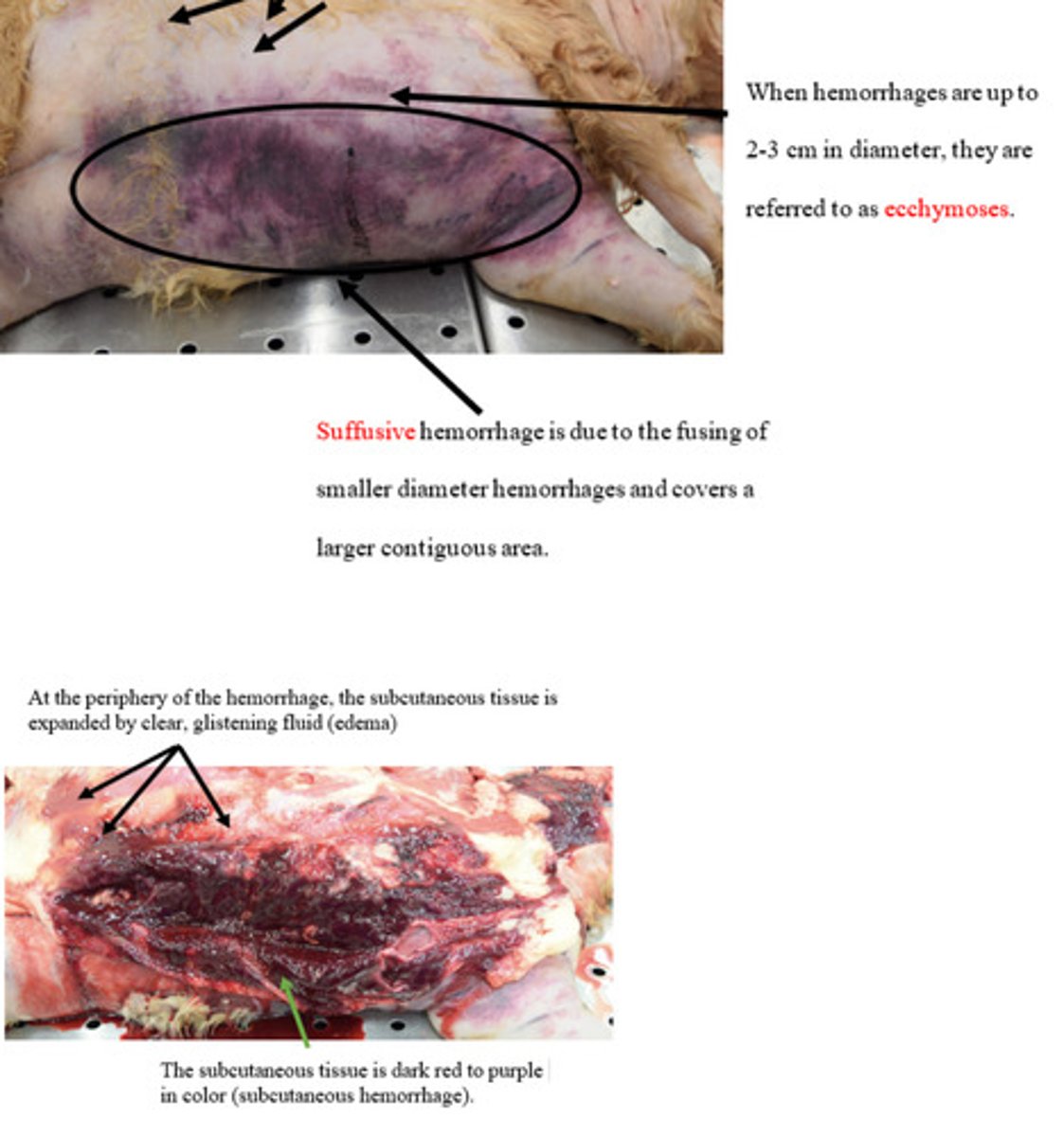
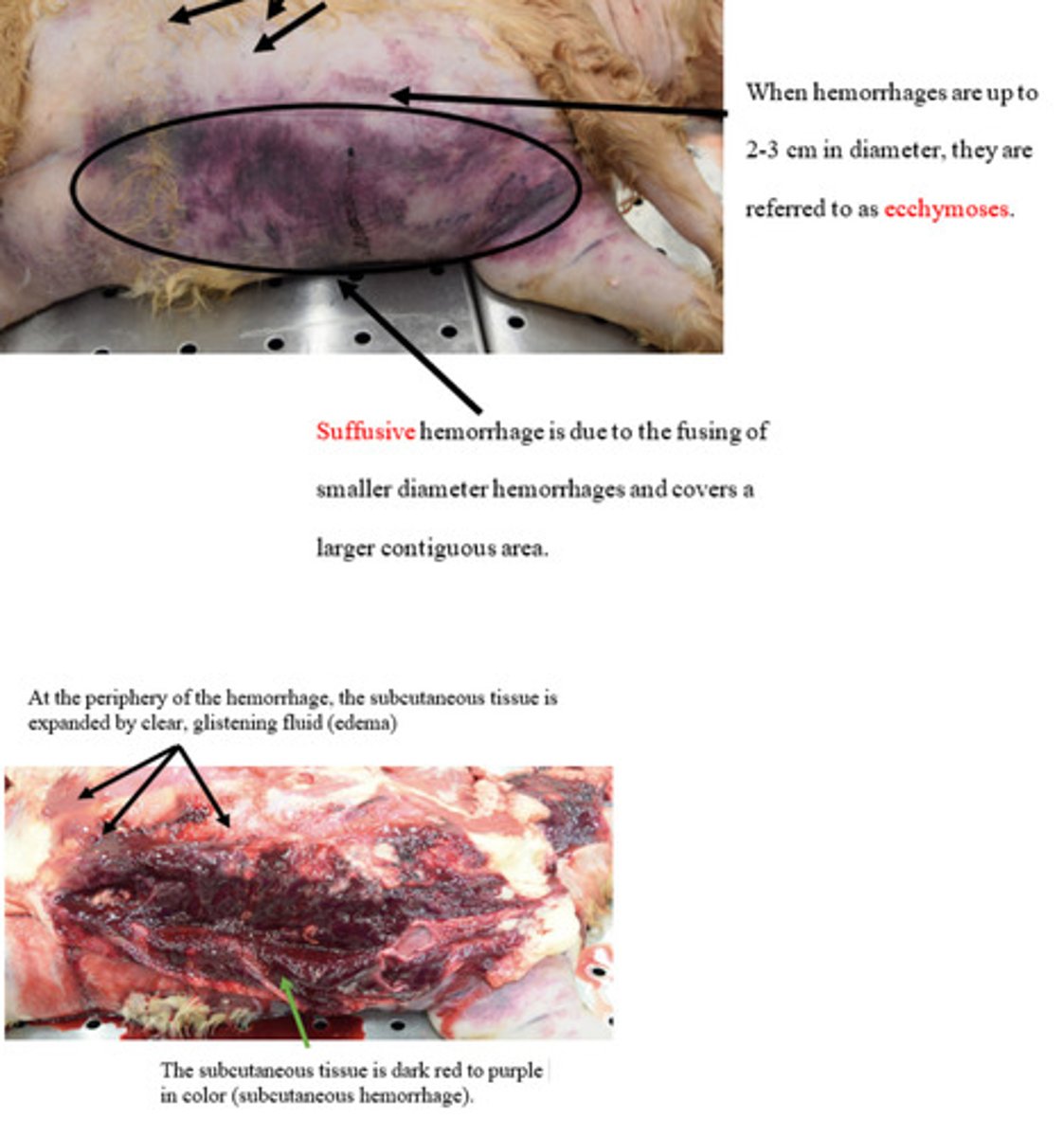
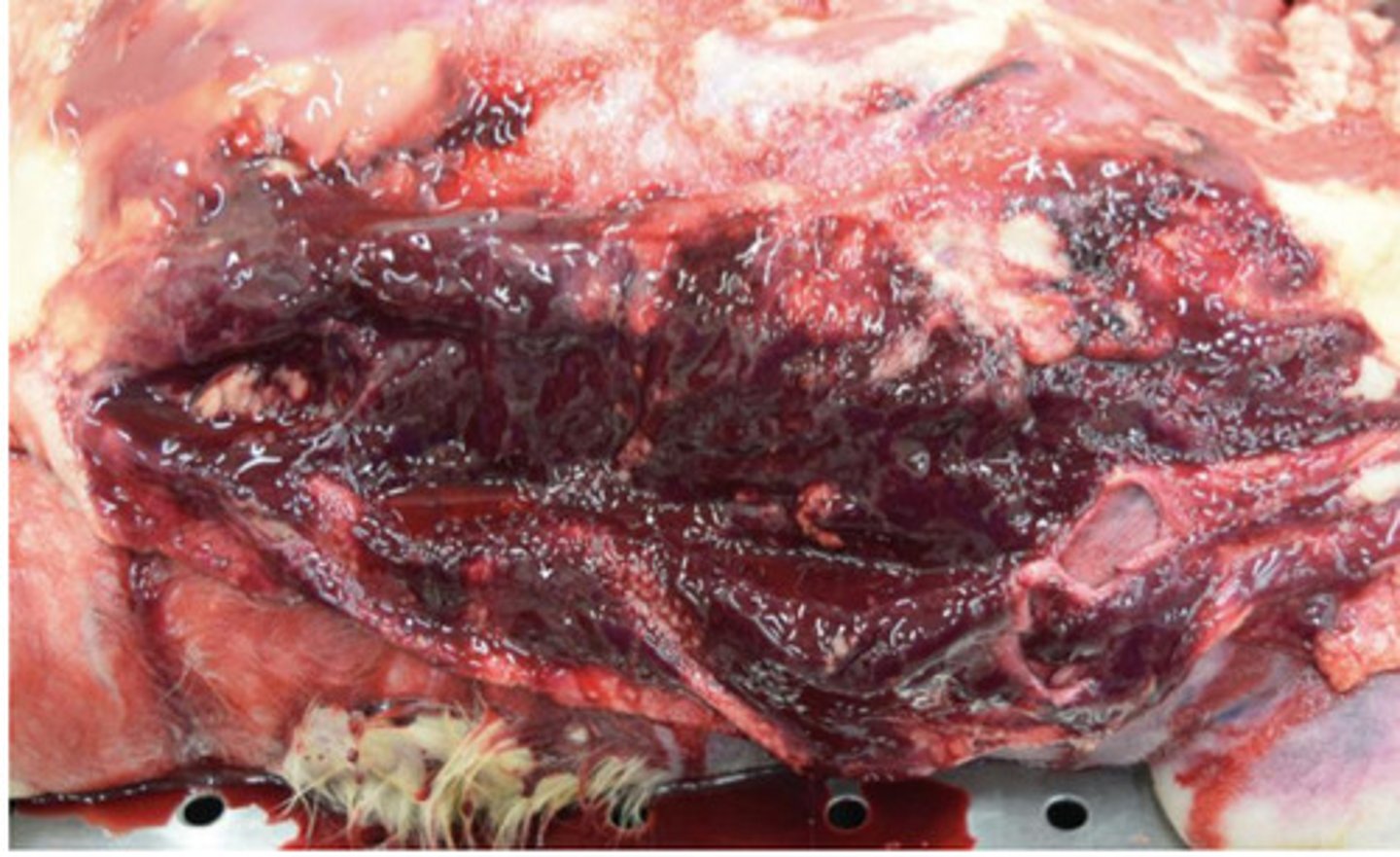
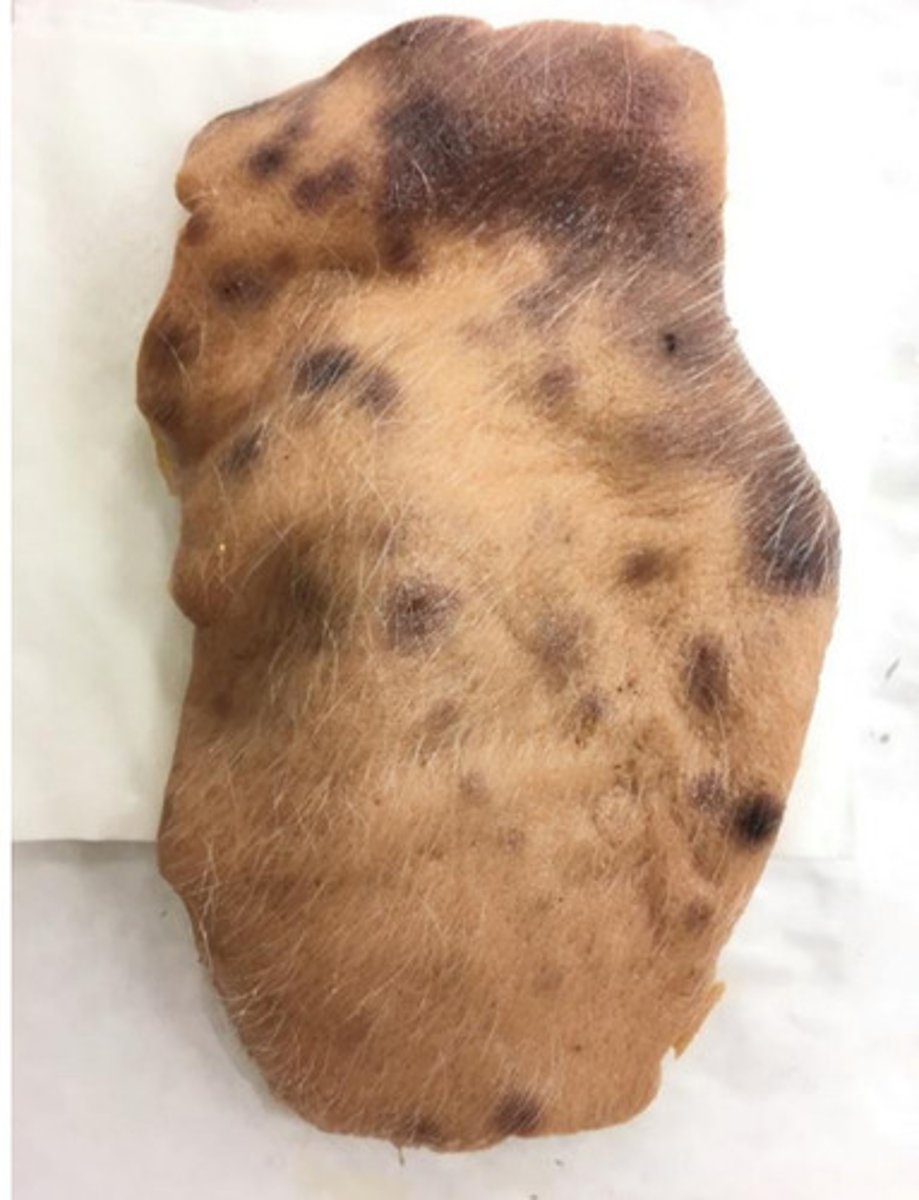
Subcutaneous edema
Ventral integument with subcutis
What is the lesion?
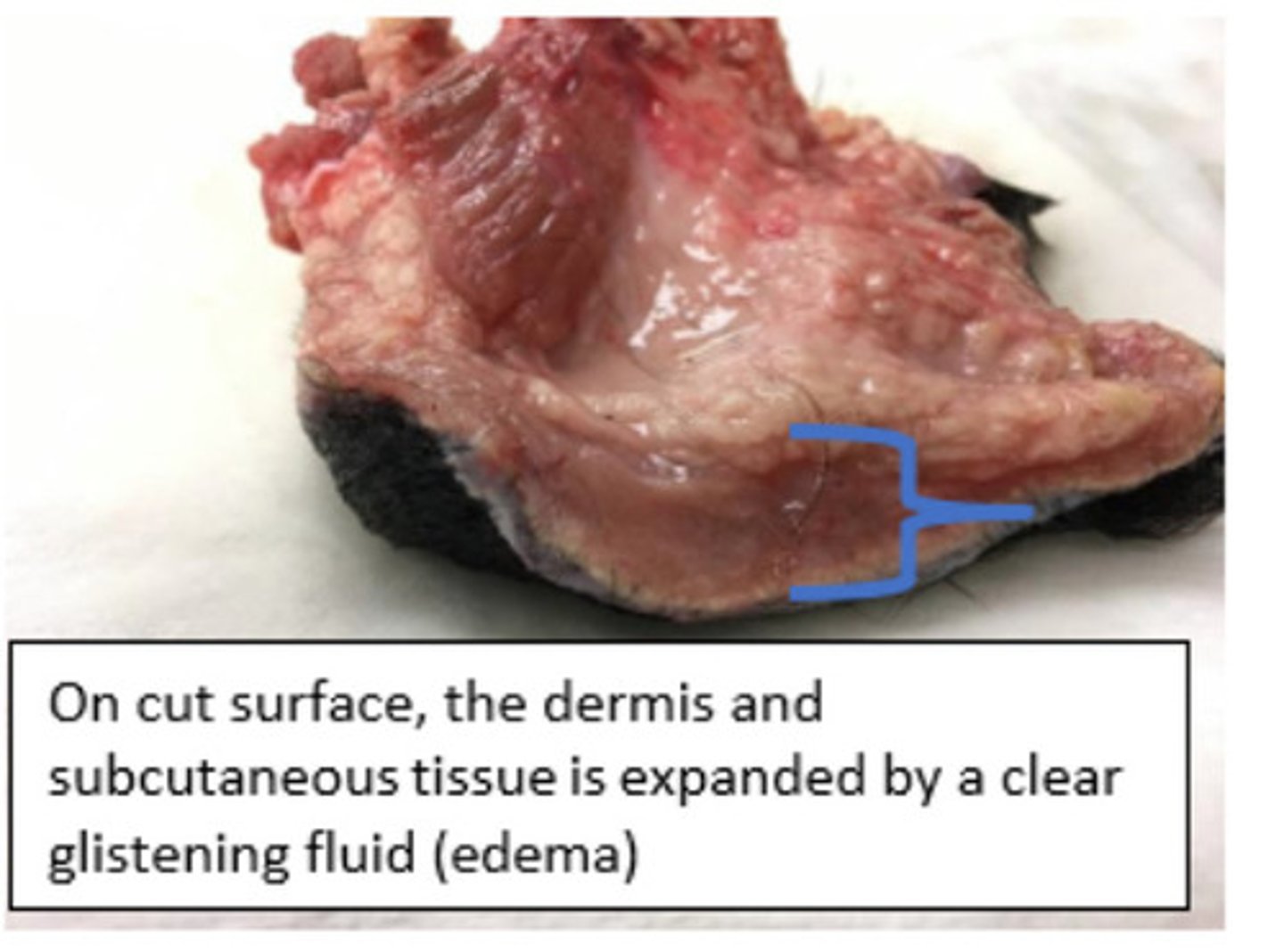
Increased microvascular permeability
▪ Increased intravascular hydrostatic pressure
▪ Decreased intravascular osmotic pressure
▪ Decreased lymphatic drainage
What are 4 mechanisms for this lesion?
Increased microvascular permeability
This specimen was from the ventrum. Pretend that you observed this lesion on the muzzle skin of a dog that had just been stung by a bee or received a vaccination. Which mechanism would you propose is responsible for the development of the lesion?
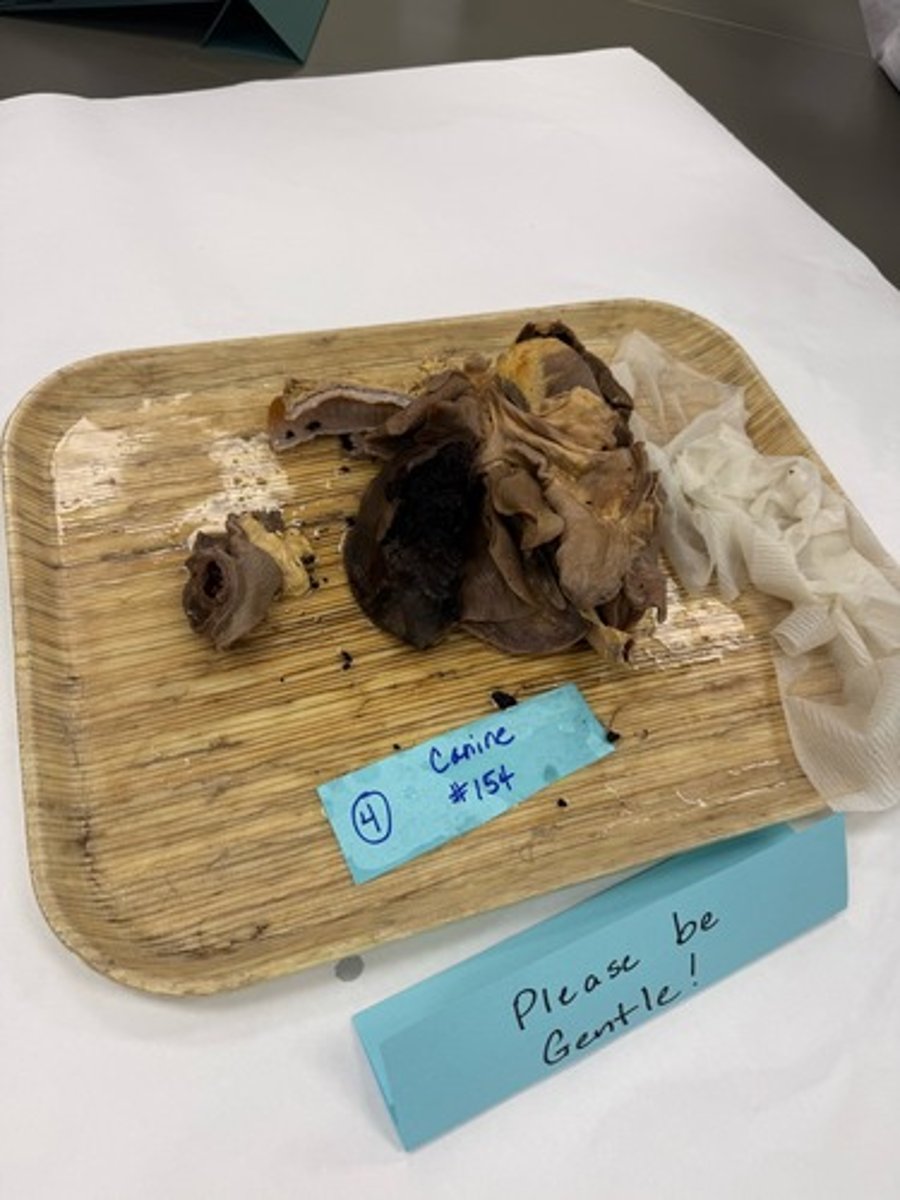
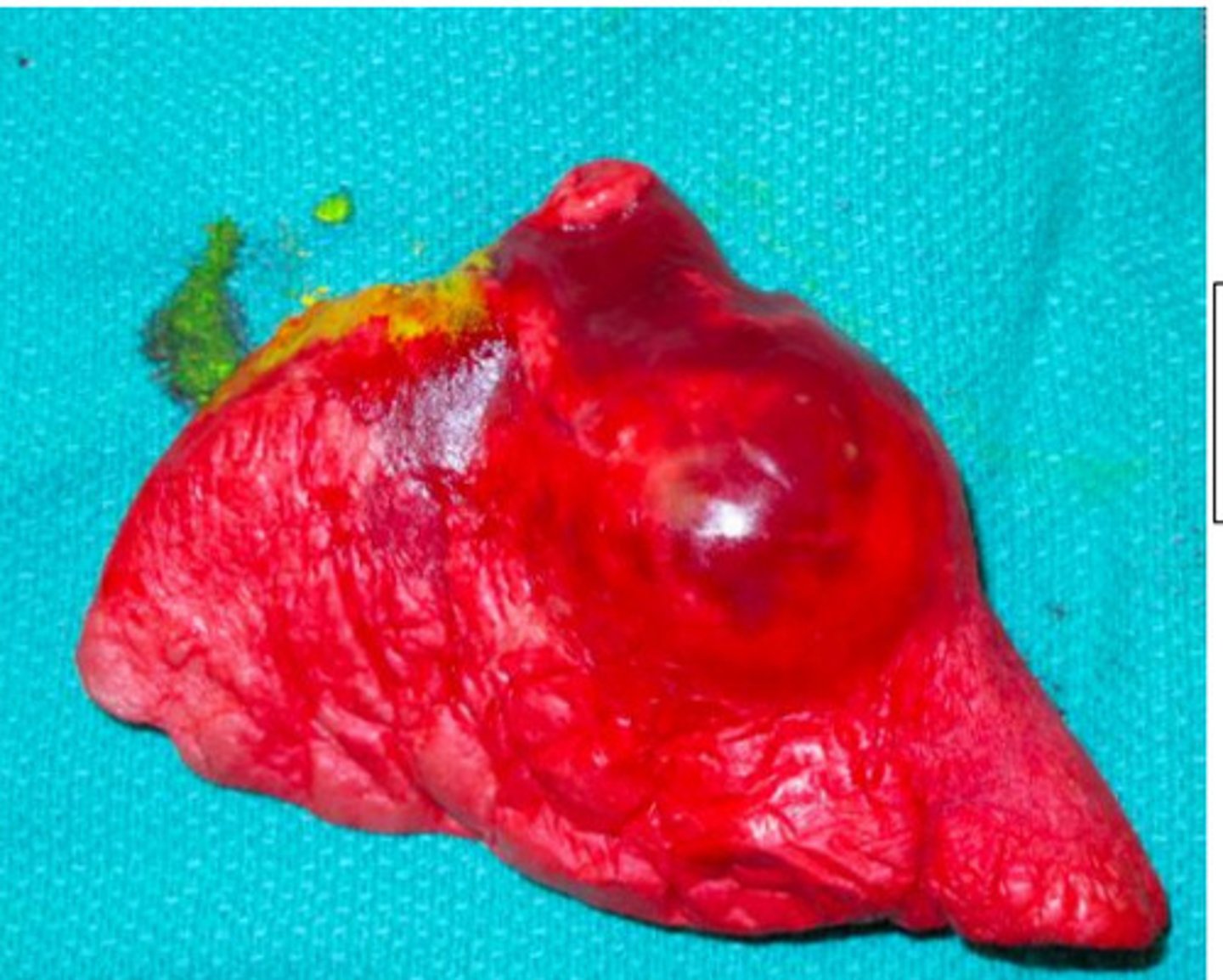
Cranial right lung lobe torsion with venous congestion and infarction
(it would be okay to add edema)
What is lesion?
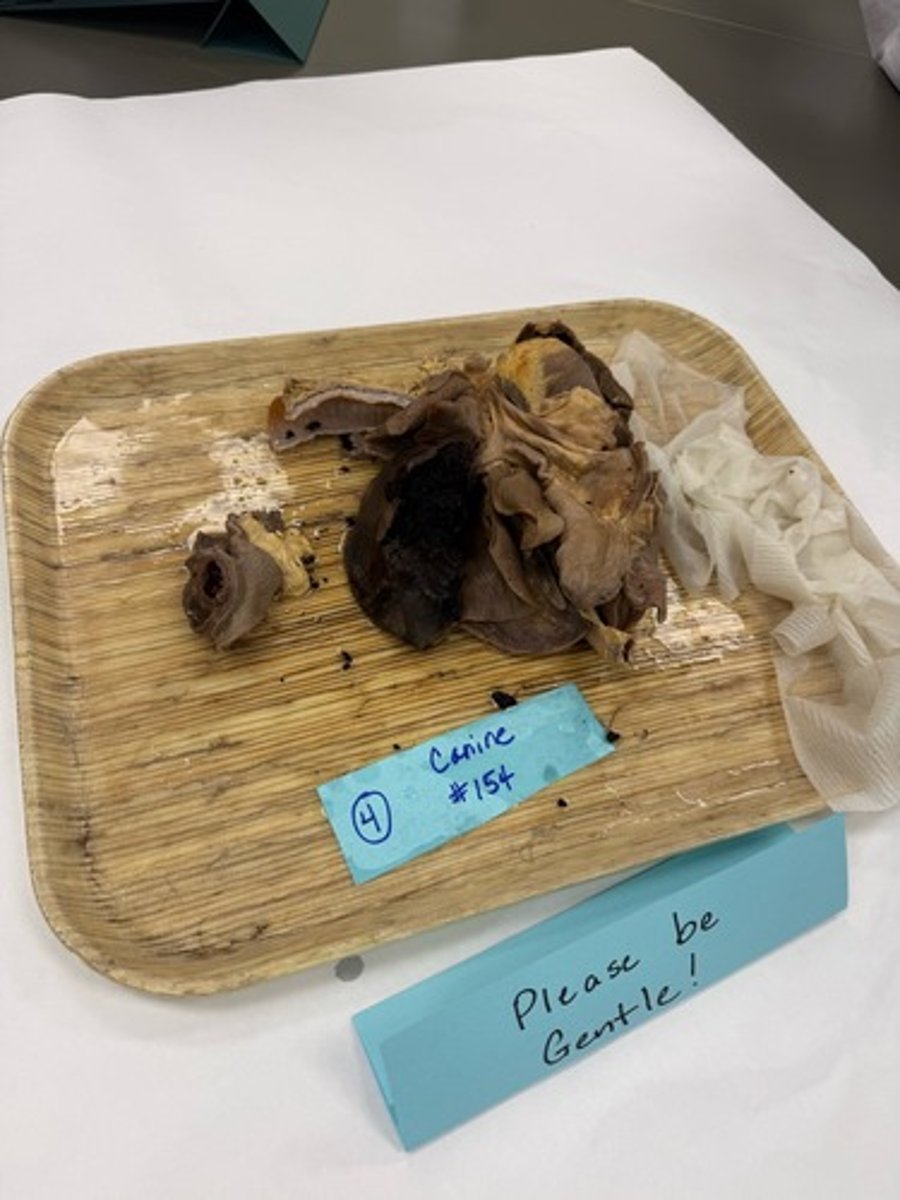
Cranial right lung lobe torsion with venous congestion and infarction
(it would be okay to add edema)
Waht is lesion?
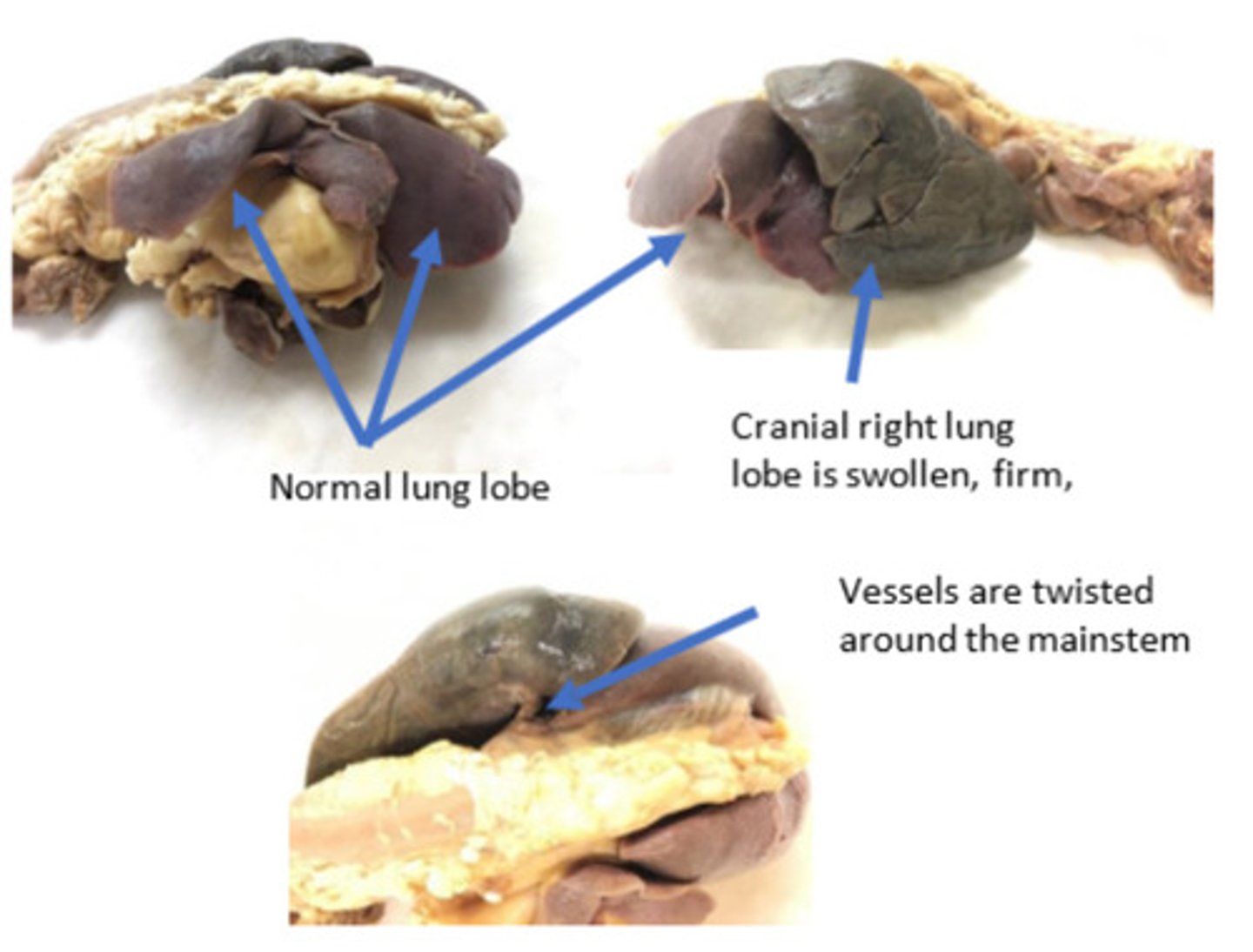
The pleural fluid led to atelectasis of the lung lobes. The lobes had increased mobility due to atelectasis and because they were floating in pleural fluid. As the lobes collapse and become heavier (more consolidated), the are predisposed to rotate at the narrow hilus.
The color change is due to venous congestion and infarction, and this is a passive process. Venous congestion results when there is obstruction of a vein. In this case, the obstruction is due to the twisting of the vessels around the hilus or mainstem bronchi. The torsion is not enough to collapse the thick-walled, high-pressure arteries which remain patent. Blood continues to be pumped into the lung lobe but cannot flow out of the lobe due to the venous obstruction. This is the reason for the venous congestion. This ultimately results in ischemia, hypoxia, and necrosis (venous infarction).
This lesion can occur in other tissues/organs. For example,
Descripe pathogenesis of lesion
Multifocal acute renal infarctions
What is lesion?

Multifocal acute renal infarctions
What is lesion?
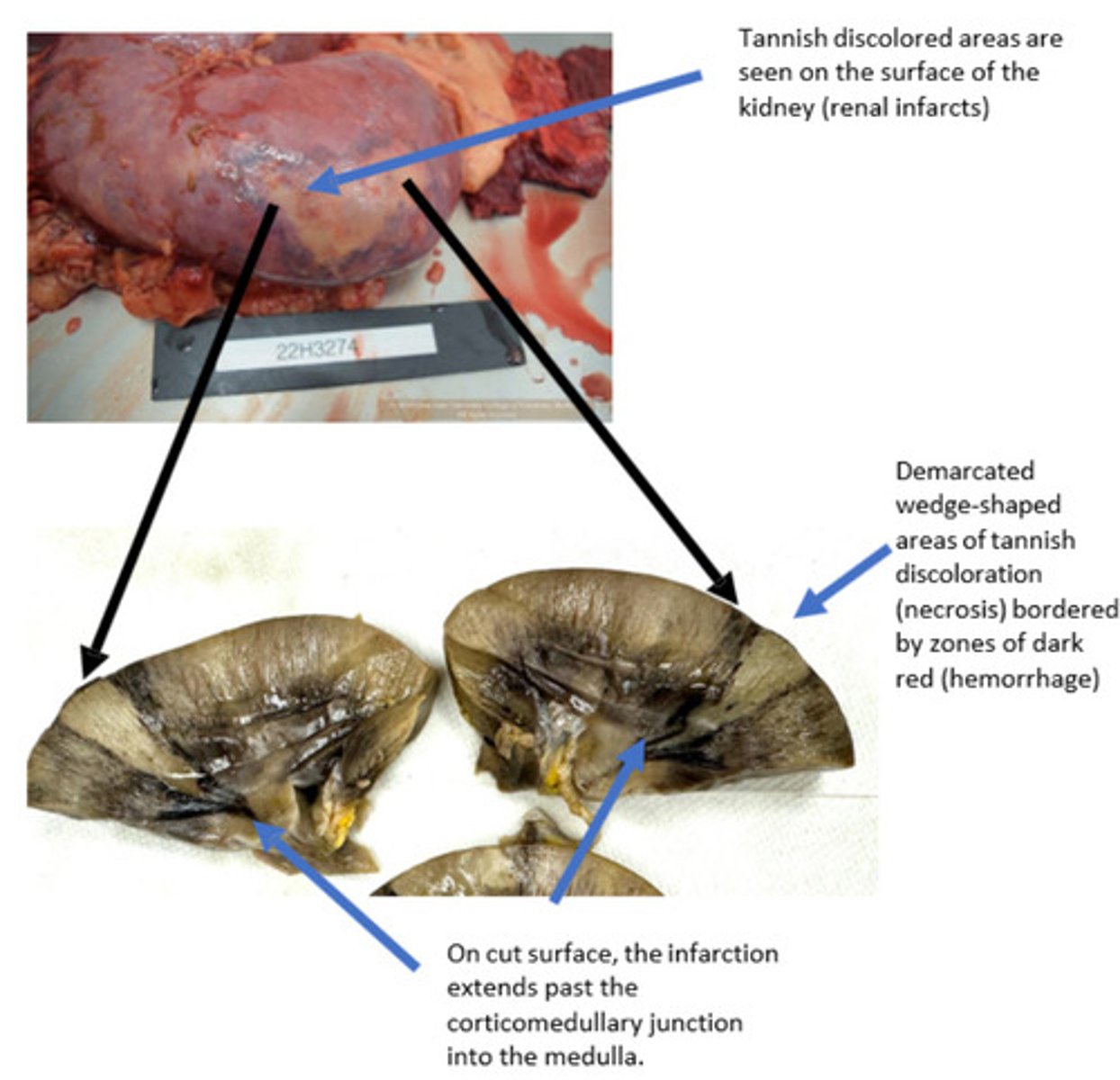
Complete arterial blockage results in immediate infarctions. Usually, arterial obstruction is due to a thrombus or thromboembolism. Arterial obstruction results in loss of blood flow to downstream tissues, resulting in abrupt coagulative necrosis.
Initially all arterial infarcts are hemorrhagic (red). Due to hemorrhage into the parenchyma from necrotic endothelium. In some tissues like the kidney, arterial infarcts eventually turn white/pale due to cellular swelling that pushes out red blood cells from the affected area.
Venous obstruction results in stagnation of blood flow and reduction or loss of venous return. There is progressive ischemia, hypoxia, and coagulative necrosis. Grossly, venous infarcts are always red/purple/dark red/ black due to back flow and accumulation of deoxygenated blood and necrosis.
How do arterial infarctions differ from venous infarctions? Why are the infarcts in the present case pale / white?
There are three main ways a thrombus can form (Virchow's Triad)
1. Abnormal blood flow (stasis or turbulence)- Changes in blood flow can be due to heart worm disease, cardiomyopathies or cardiac valvular deformities
2. Endothelial damage- pathogens (bacteria, viruses, fungi), toxins.
3. Hypercoagulability- protein losing nephropathies (antithrombin III loss), decreased clotting factors, liver failure
How can thrombus form?
Hemorrhage
Whats the lesion?
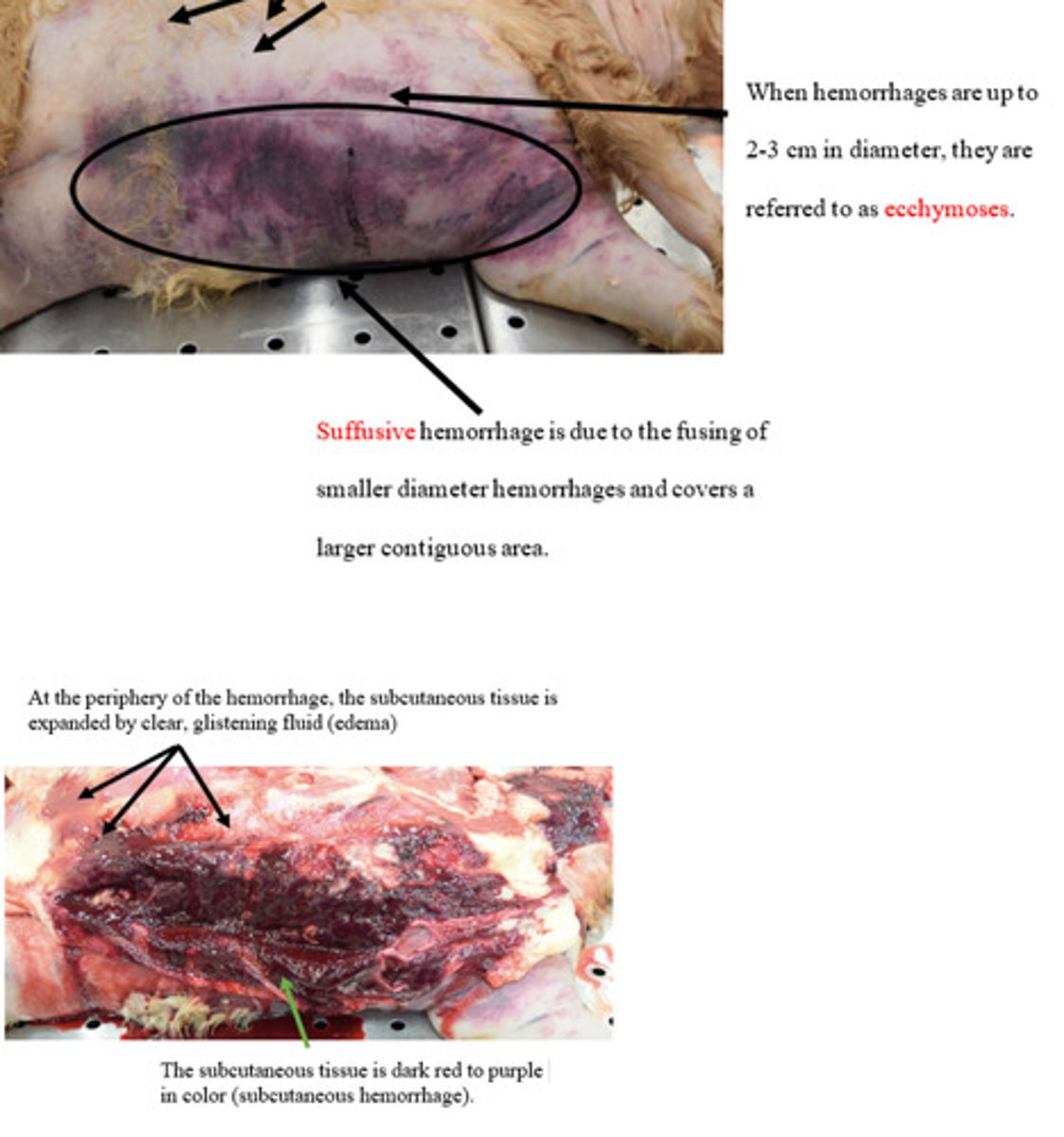
Petechiae
Ecchymoses
Suffusive/paint brush
What are 3 patters of hemmorrhage we have learned?
Hemorrhage occurs because of abnormal function in one or the more of the following:
A. Endothelium/ vessel structure
a. Trauma- physical or mechanic disruption of vessels
b. Inflammation or neoplasia can erode or invade blood vessels
c. Septicemia (bacterial blood infection)- causes damage to the endothelium and blood vessel walls resulting in hemorrhage
d. Inherited diseases that result in dysfunction collagen can create fragile vessel walls that are easily disrupted
B. Platelets
a. Decrease numbers (thrombocytopenia) or functionality of the platelets (thrombocytopathy)
C. Coagulation factors
a. Decreased numbers/ functionality of the coagulation factors. Functionality can be compromised due to Inherited diseases (genetic defects in coagulation factors) or acquired dysfunction (rodenticides or toxins)
How does hemmhorage occur?
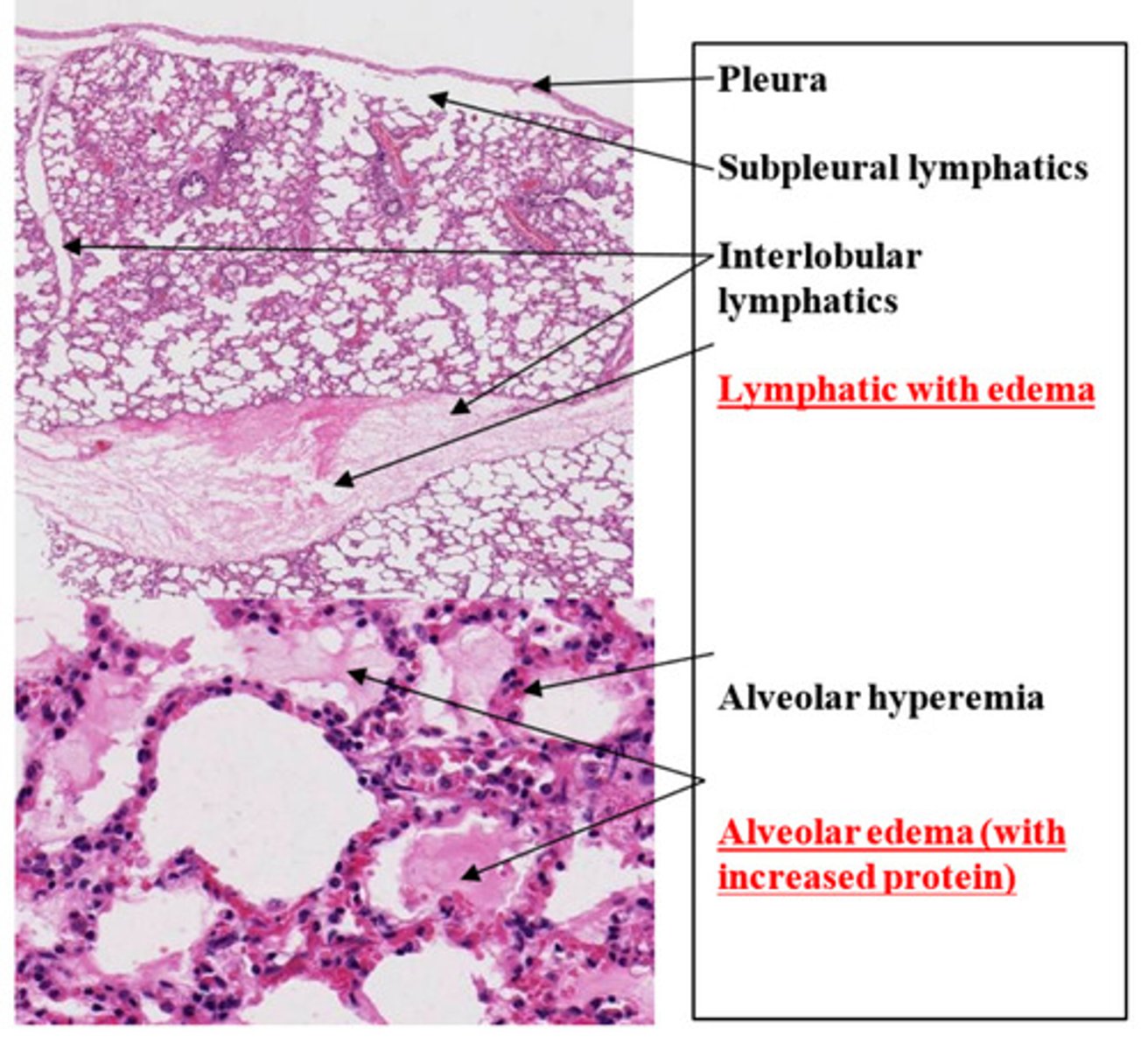
Lung: diffuse passive congestion and edema
What is the lesion?
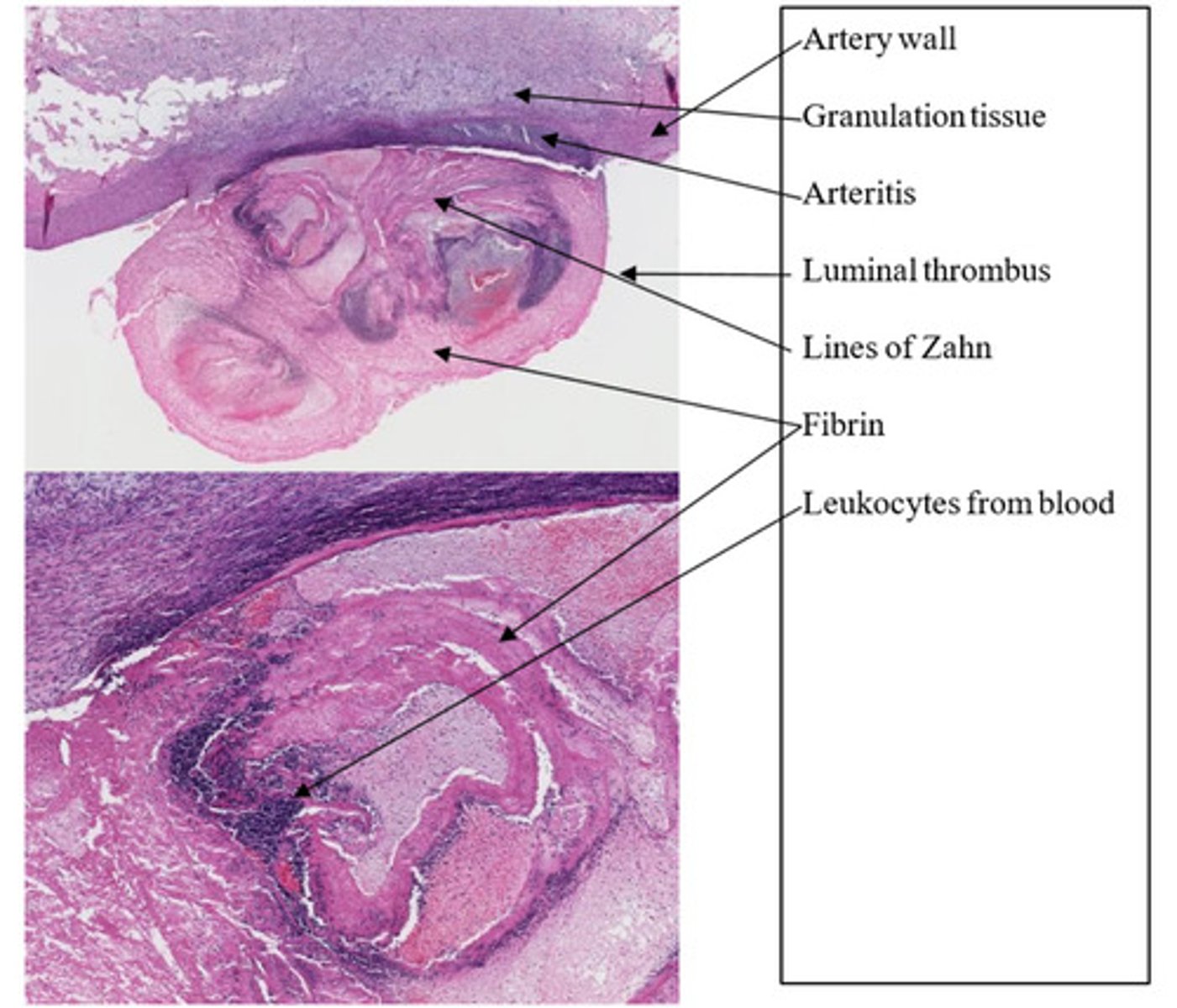
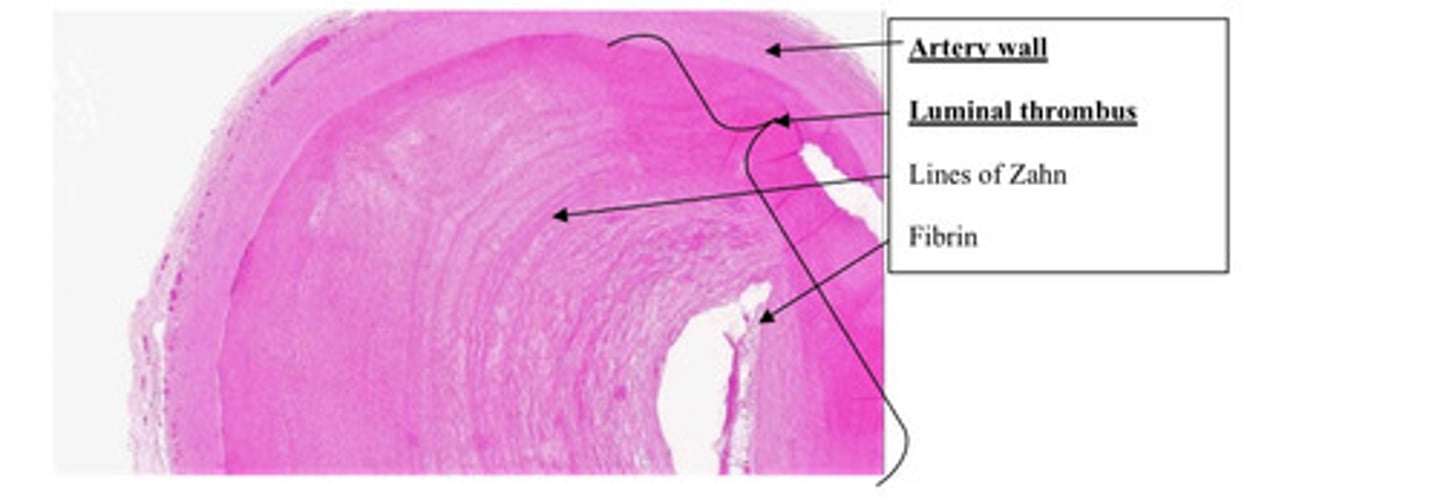
Arterial thrombus with chronic arteritis
What is the lesion?
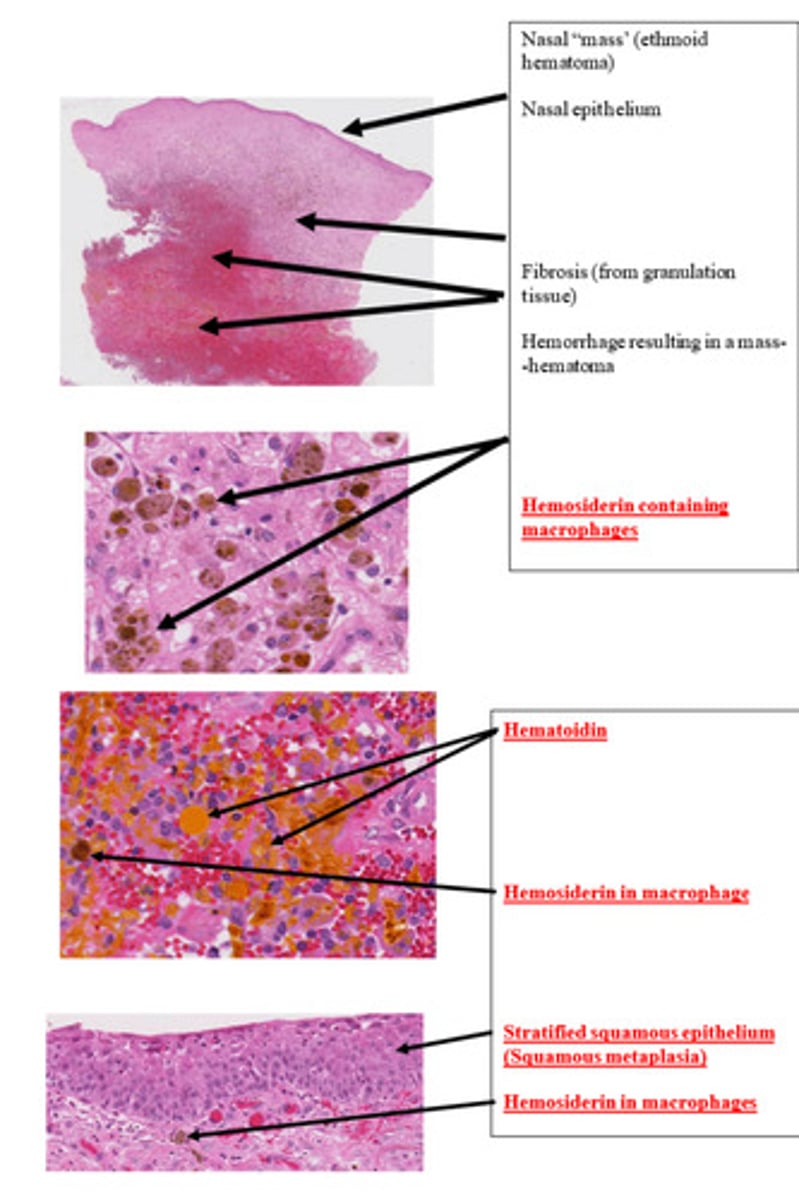
Hemmhorrhage ?? Idk
What is the lesion?
Intussusception with edema, venous congestion, and infarction
What is the lesion?

Intussusception with edema, venous congestion, and infarction
What is the lesion?
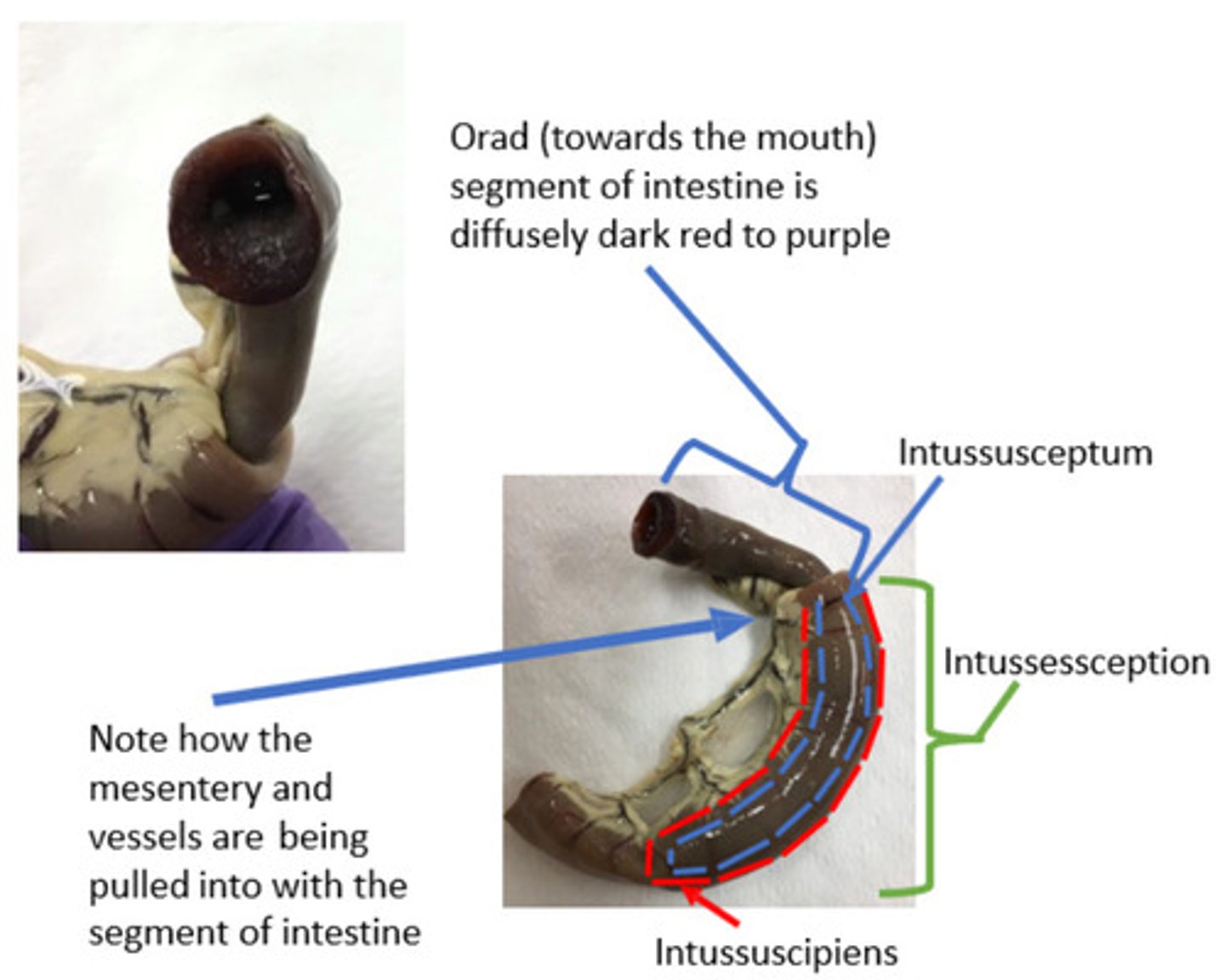
The mesentery connected to the intussusceptum is also enveloped by the intussuscipiens. The pressure applied by the intussuscipiens will compress the veins within the mesentery. Remember that veins have relatively thin and flaccid walls since they are low pressure vessels. The mesenteric arteries, however, are not compressed or collapsed. Remember that arteries are thick-walled, high-pressure vessels, thus, blood continues to flow through them
What do you expect to happen to the mesenteric arteries and veins supplying these segments of intestines?

Edema, venous congestion, and necrosis (venous infarction) are expected.
The decreased outflow of venous blood results in a passive accumulation of blood in the vasculature (venous congestion). Increased hydrostatic pressure in the venous vasculature results in edema. The pooling blood ultimately results in decreased blood flow (ischemia) and decreased tissue oxygenation (hypoxia) and is severe enough / exacerbated by lack of collateral blood supply, that tissue necrosis occurs (venous infarction).
What are three sequelae due to the vascular changes you predicted and why?
A lesion with venous infarction will always technically also have venous congestion. However venous congestion can occur in the absence of venous infarction, because venous congestion precedes venous infarction in the pathogenesis sequence (i.e. it hasn't gone on long enough or the pooled blood is oxygenated enough to prevent necrosis).
Explain the relationship between venous congestion and venous infarction.
Focal
What is pattern of distribution?
Multifocal
What is pattern of distribution?
Locally extensive
What is pattern of distribution?
Diffuse
What is pattern of distribution?

Multifocal to coalescing
What is pattern of distribution?
Small intestine, severe, acute, Multifocal, ulcerative enteritis
Provide morphological diagnosis
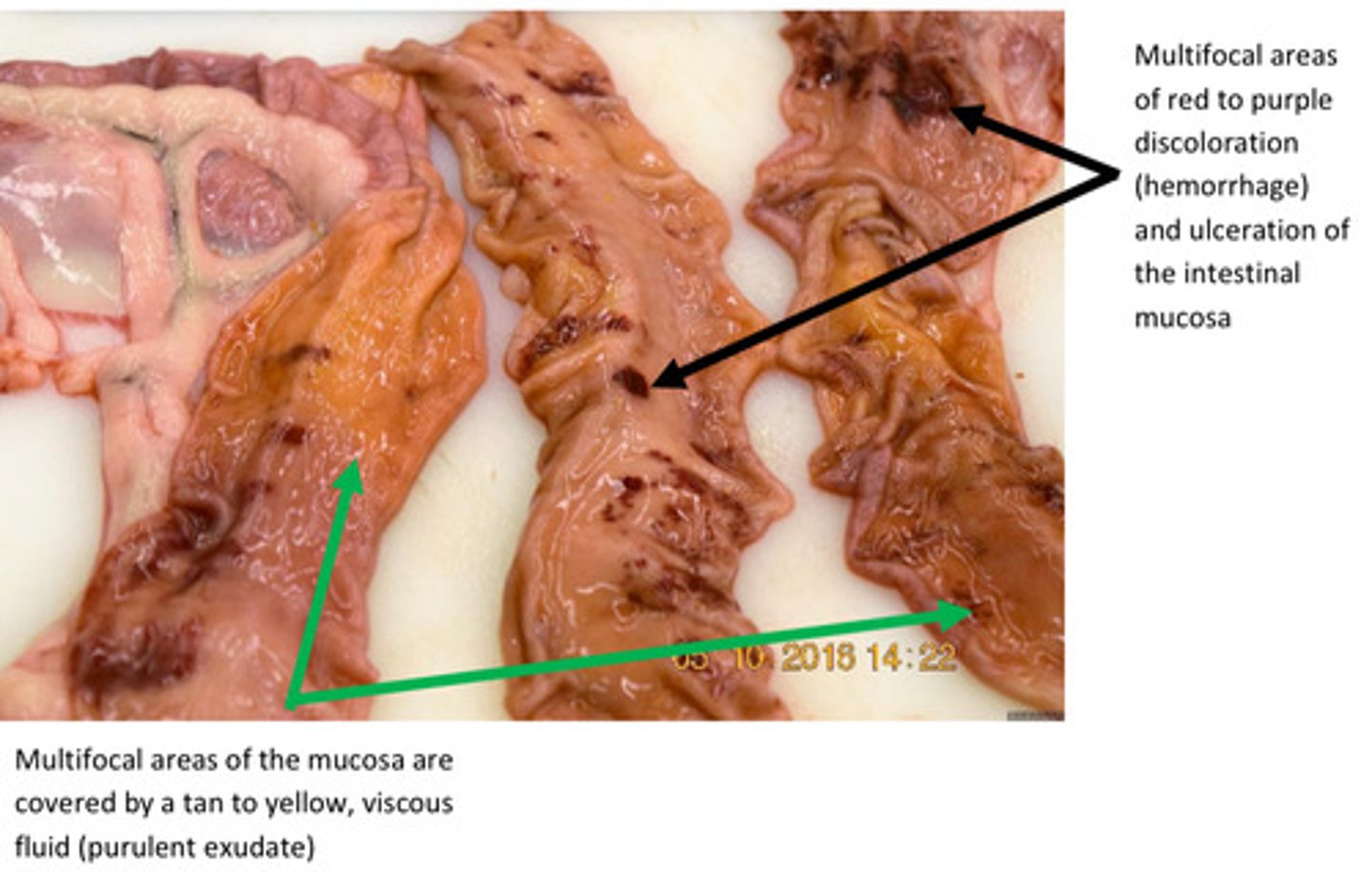
Small intestine, severe, acute, Multifocal, ulcerative enteritis
Provide morphological diagnosis

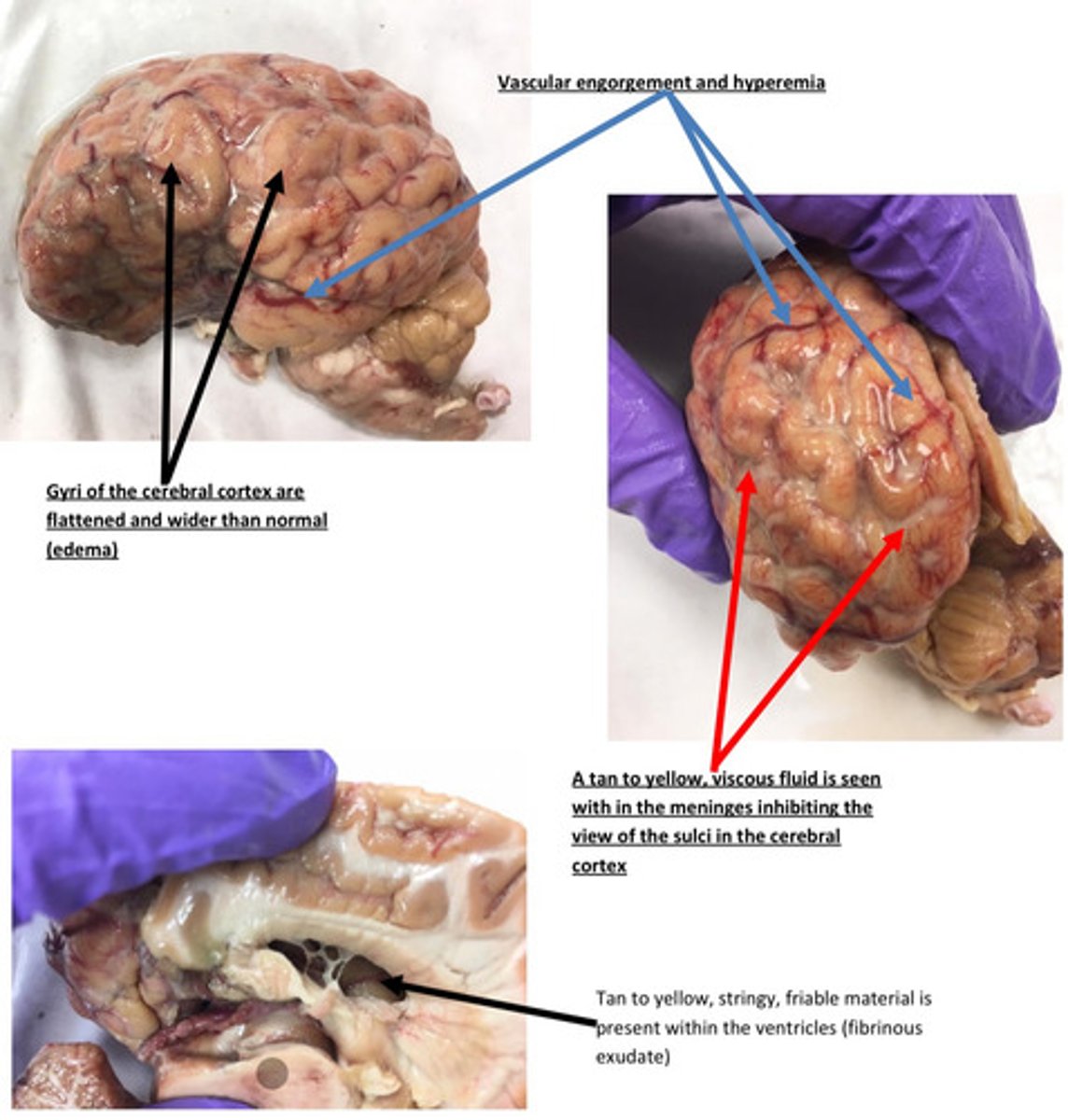
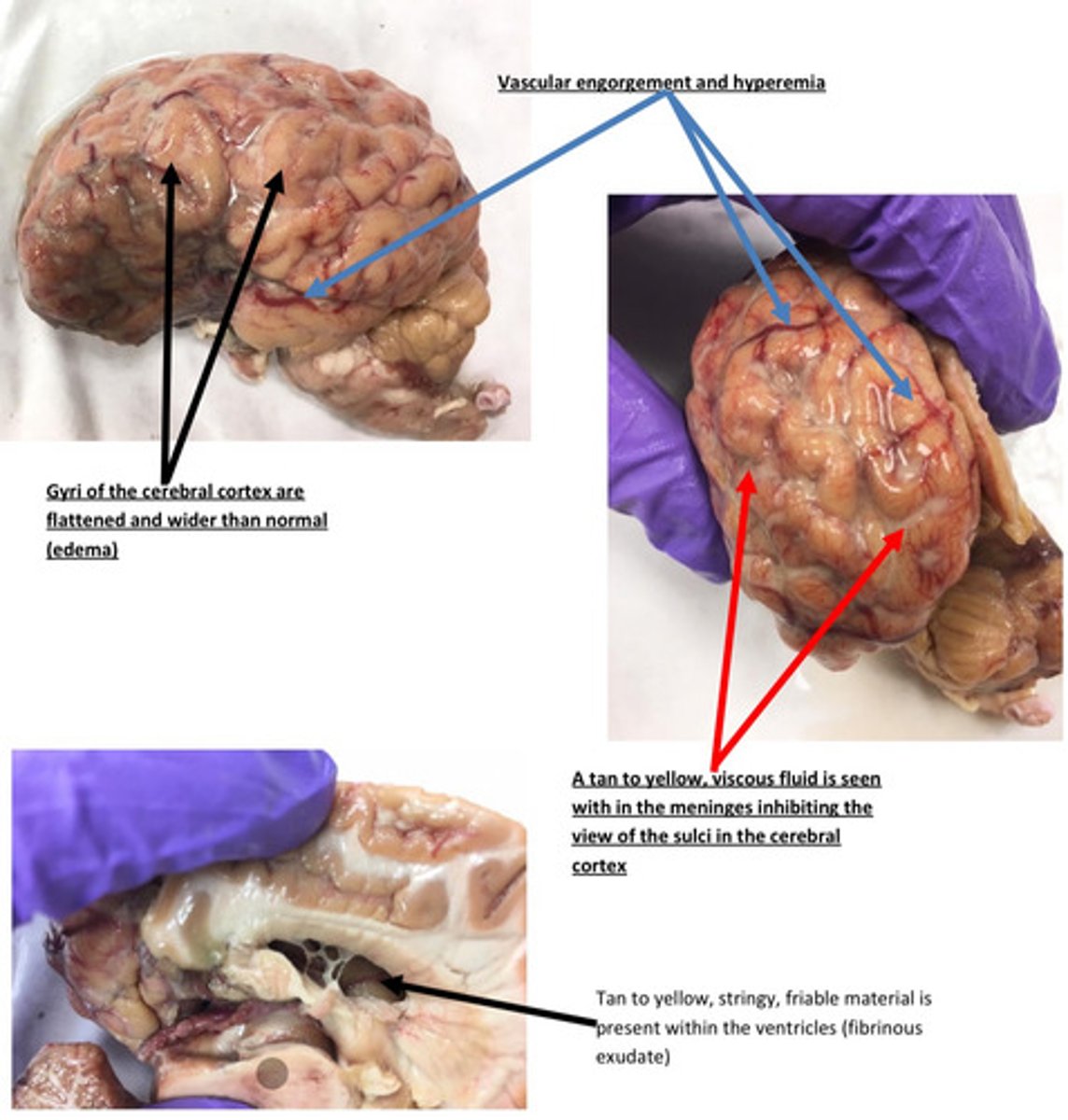
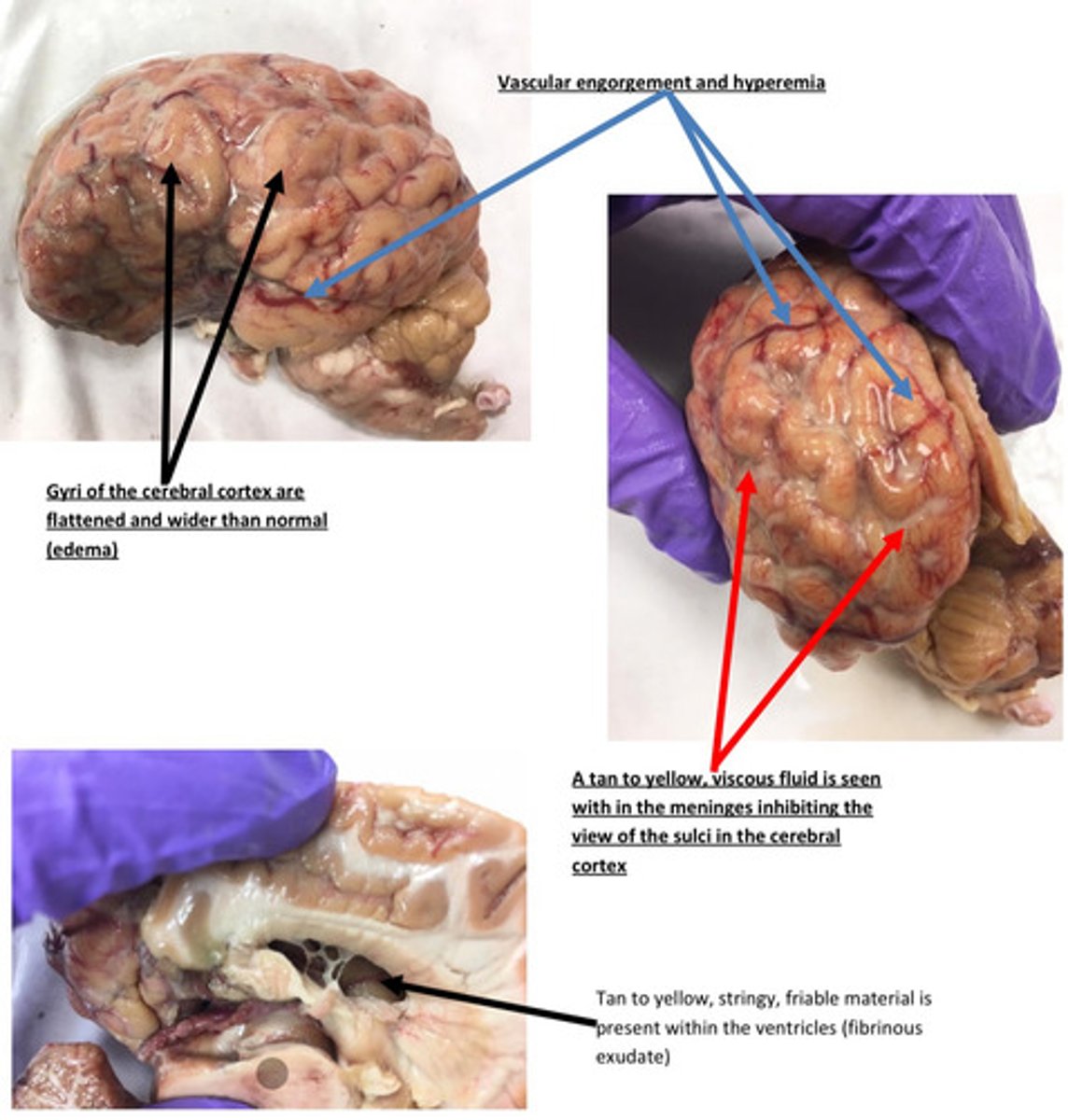
Brain: severe, acute, diffuse, cerebral and cerebellar edema with fibrinous ventricular is
Meninges: severe, acute, diffuse, fibrinopurulent meningitis
Provide morphological diagnosis
Brain: severe, acute, diffuse, cerebral and cerebellar edema with fibrinous ventricular is
Meninges: severe, acute, diffuse, fibrinopurulent meningitis
Provide morphological diagnosis
The sulci are hard to see in this case because there is a fibrinous exudate within the
meninges. The exudate is present because there is inflammation associated with the
meninges. The exudate in this case is composed of fluid, fibrin, other plasma proteins,
and some neutrophils. Fewer sulci will be seen as more exudate accumulates within the
meninges. It is common for the exudate to settle towards the ventral aspect of the brain.
Remember that there is a fluid component to the exudate and gravity tends to pull fluid
to the ventral aspect of the animal.
Why are sulci hard to see in this case?
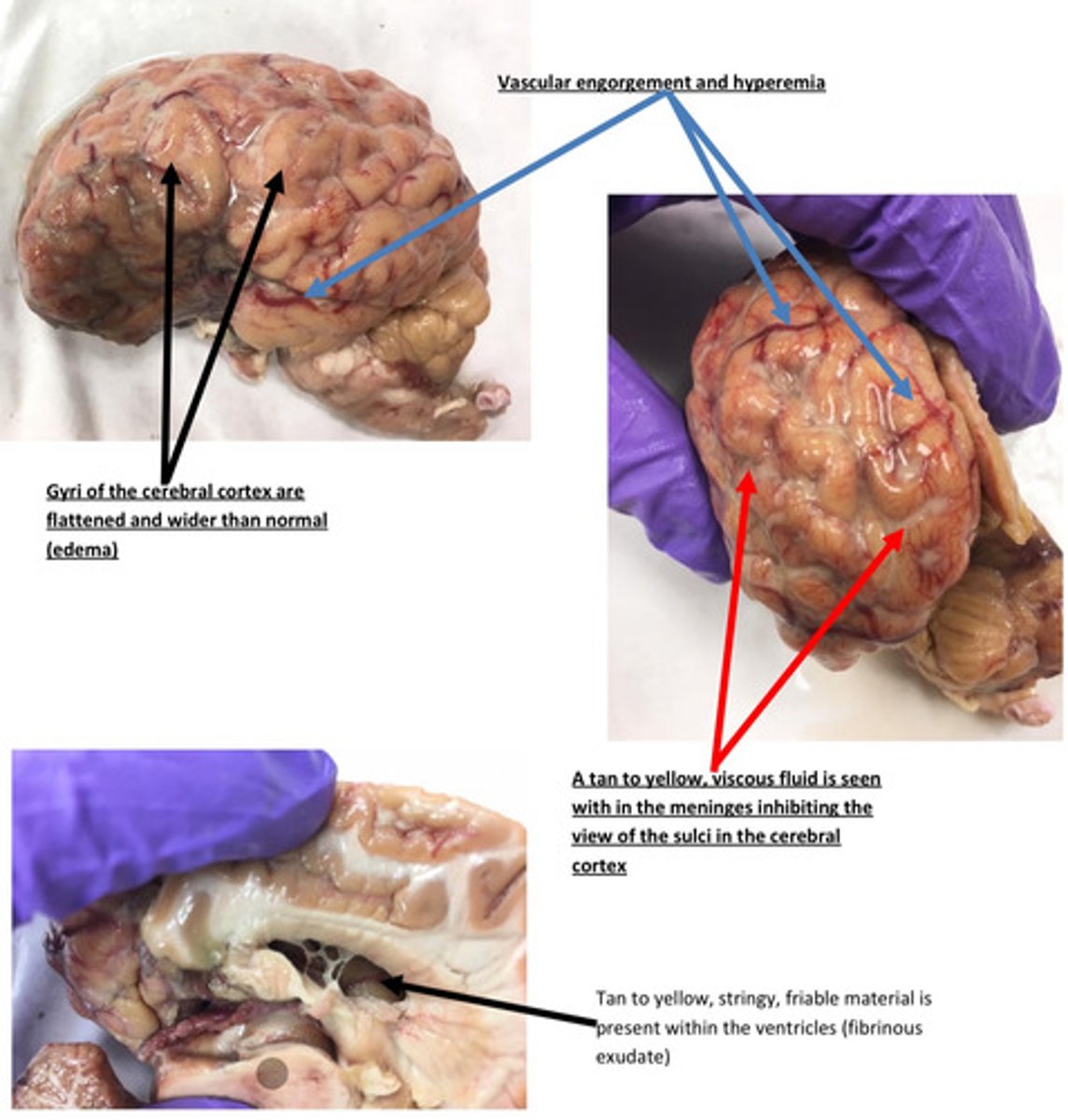
The prominent blood vessels and engorgement are due to a process known as active
hyperemia, which commonly occurs in acute inflammation. In this case, bacteria have
hematogenously (via blood) spread to the meninges where they colonize. The bacteria
elicit an inflammatory response that is mediated by inflammatory mediators such as
prostaglandins, endothelin, histamine, neuropeptides, kinins, and nitric oxide. These
inflammatory mediators act as vasodilators, increase blood flow in arterioles/ capillaries,
slow the blood flow, and allows times for plasma and plasma proteins to leak out of the
vessels. Active hyperemia is responsible for the redness seen in the inflamed tissues.
The meninges are diffuse bright red with prominent blood vessels. Why do think the
meningeal vessels are engorged with blood?
Decreased immunity and increased susceptibility in neonate calf (usually due to failure
of passive transfer)→ exposure to bacteria (E. coli, Pasteurella multocida, histophilus
somni, etc.) → septicemia → hematogenous spread to the meninges→ colonization→
initiation of the acute inflammatory response→ meningitis
**entry of bacteria can occur in utero, via the oral cavity, via umbilical stump, or via
surgical procedure*
Provide a pathogenesis for this lesion?
Urethra: A locally extensive area of the urethral lumen contains a tan, friable material
admixed with a tannish, viscous material (purulent exudate). The underlying urethral
mucosa is discolored black to purple and there are multifocal ulcerations. The
surrounding soft tissue is expanded by a clear, glistening fluid (edema) and there are
multifocal irregularly sized purplish discolored areas (hemorrhage and hyperemia)
Urinary Bladder: There were multifocal hemorrhages on the mucosal surface of the
bladder that extended to the serosal surface. The bladder wall was edematous and
friable multifocally. There were numerous calculi ranging in size from a few mm to 2 cm
present in the bladder. The calculi were yellow to white in color and firm.
Describe lesions of bladder and urethra

Urethra: severe acute locally extensive, fibrinoecrotic urethritis
Bladder: severe acute locally extensive, necrohemorrhagic cystitis
Provide morphological diagnosis

Urethra: severe acute locally extensive, fibrinoecrotic urethritis
Bladder: severe acute locally extensive, necrohemorrhagic cystitis
Provide morphological diagnosis

Uroliths (stones) formation (commonly due to diets high in phosphorus and magnesium) occurs in the urinary collecting system→ uroliths move into the urethra andgets lodged in either the sigmoid flexure or the urethral process → urine flow is blocked
(inability to urinate) and back pressure builds up→ increased pressure within the urethra
and bladder results in pressure necrosis of the uroepithelium → necrosis result in
inflammation (fibrin deposition and neutrophil infiltration) and hemorrhage.
Propose a pathogenesis for the lesion

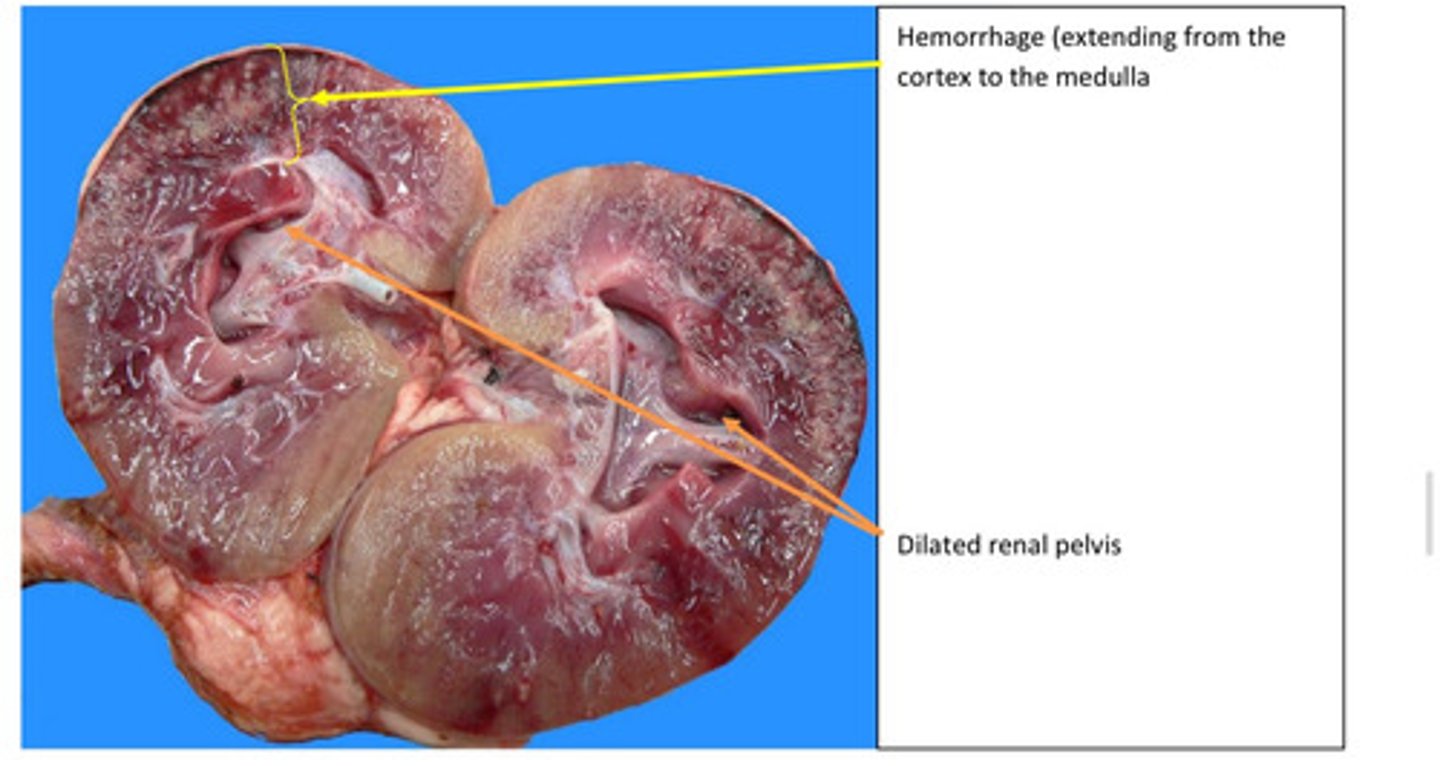
Blockage of the ureter by the uroliths occlude flow of urine which backs up into the renal
pelvis. This causes pressure build-up in the pelvis and compresses adjacent structures-
pressure necrosis and pressure atrophy. This increased pressure, as well as bacterial
emboli, results in occlusion of renal capillaries that leak and rupture resulting in the
hemorrhage. Since the renal arcuate arteries and veins have a distinct flow entering
from the renal pelvis, it is not unexpected that the hemorrhage would extend from the
cortex to the medulla.
Propose a pathogenesis for observed change in the kidney
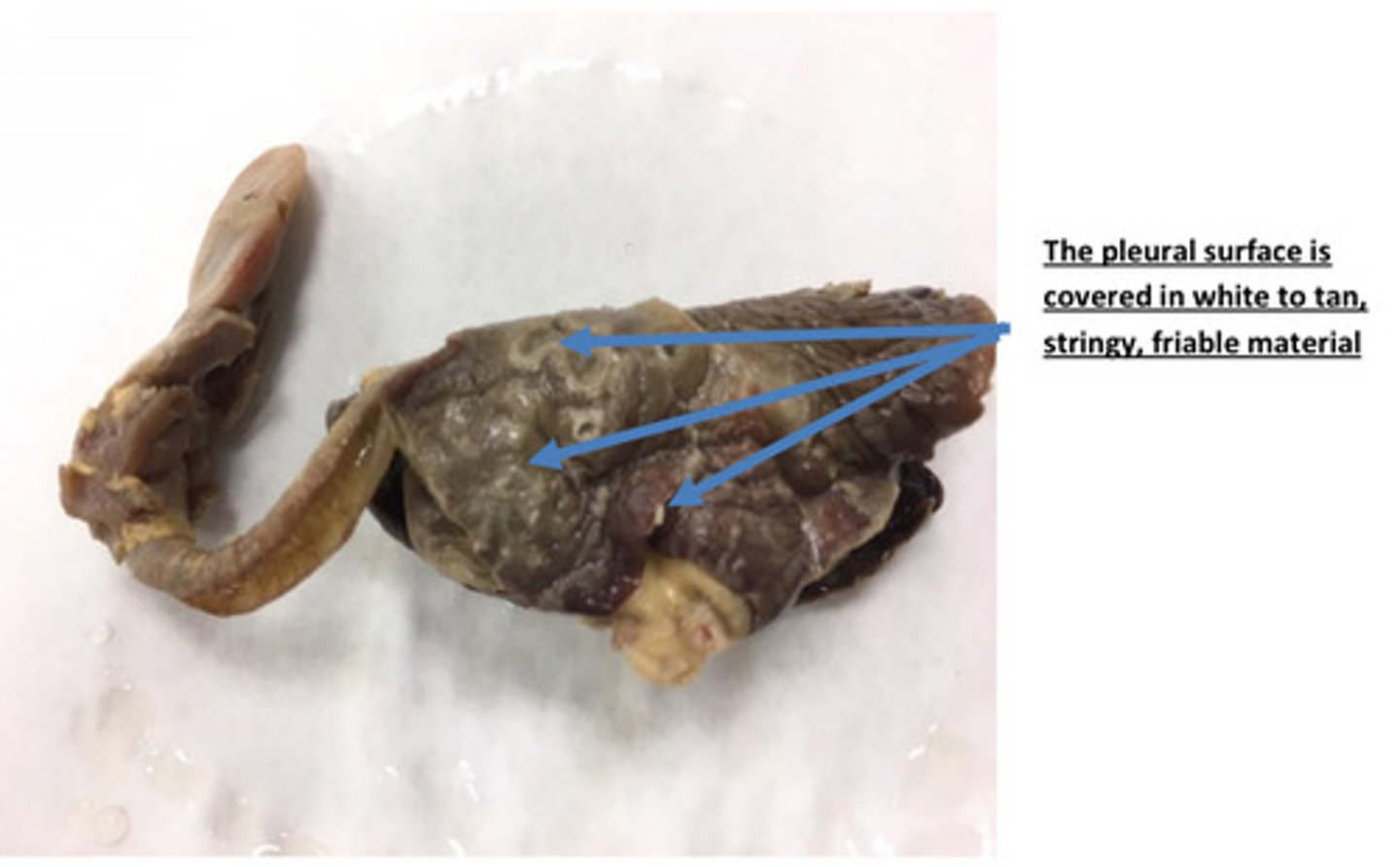
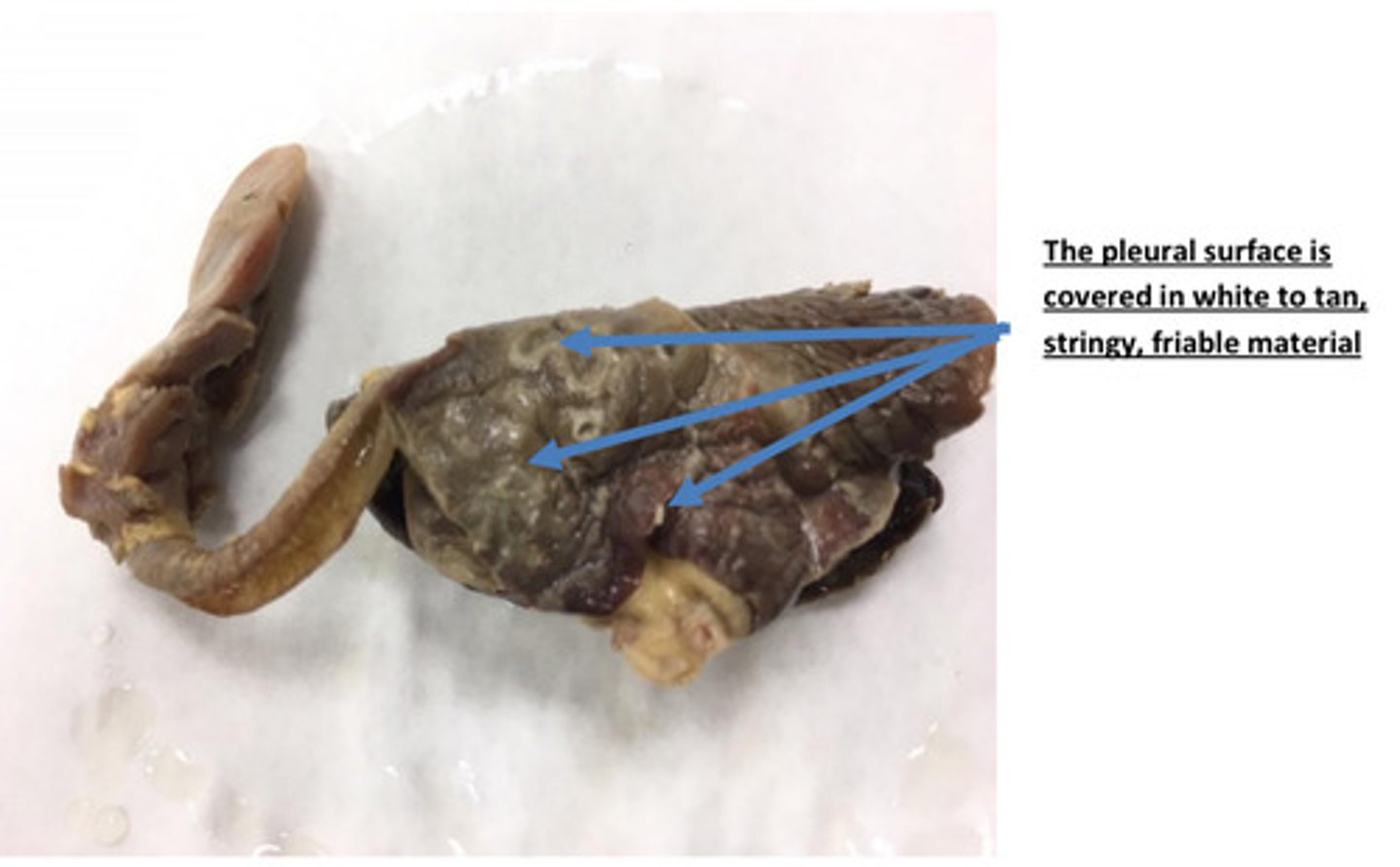
Lungs, severe acute diffuse fibrinous pleuritis
Provide morphological diagnosis
Lungs, severe acute diffuse fibrinous pleuritis
Provide morphological diagnosis

Fibrinous inflammation is a term used to describe acute inflammation in which the tissue
response consists of accumulation of fluid with a high concentration of plasma protein
and lower numbers of neutrophils. Fibrinous inflammation occurs when endothelial
damage allows large molecular weight plasma protein such as fibrinogen to leak into the
tissues. Fibrinogen leaks out of capillaries and post capillary venules during the fluidic
phase of acute inflammation and polymerizes to fibrin.
How did this material get on to the surface of the lung?
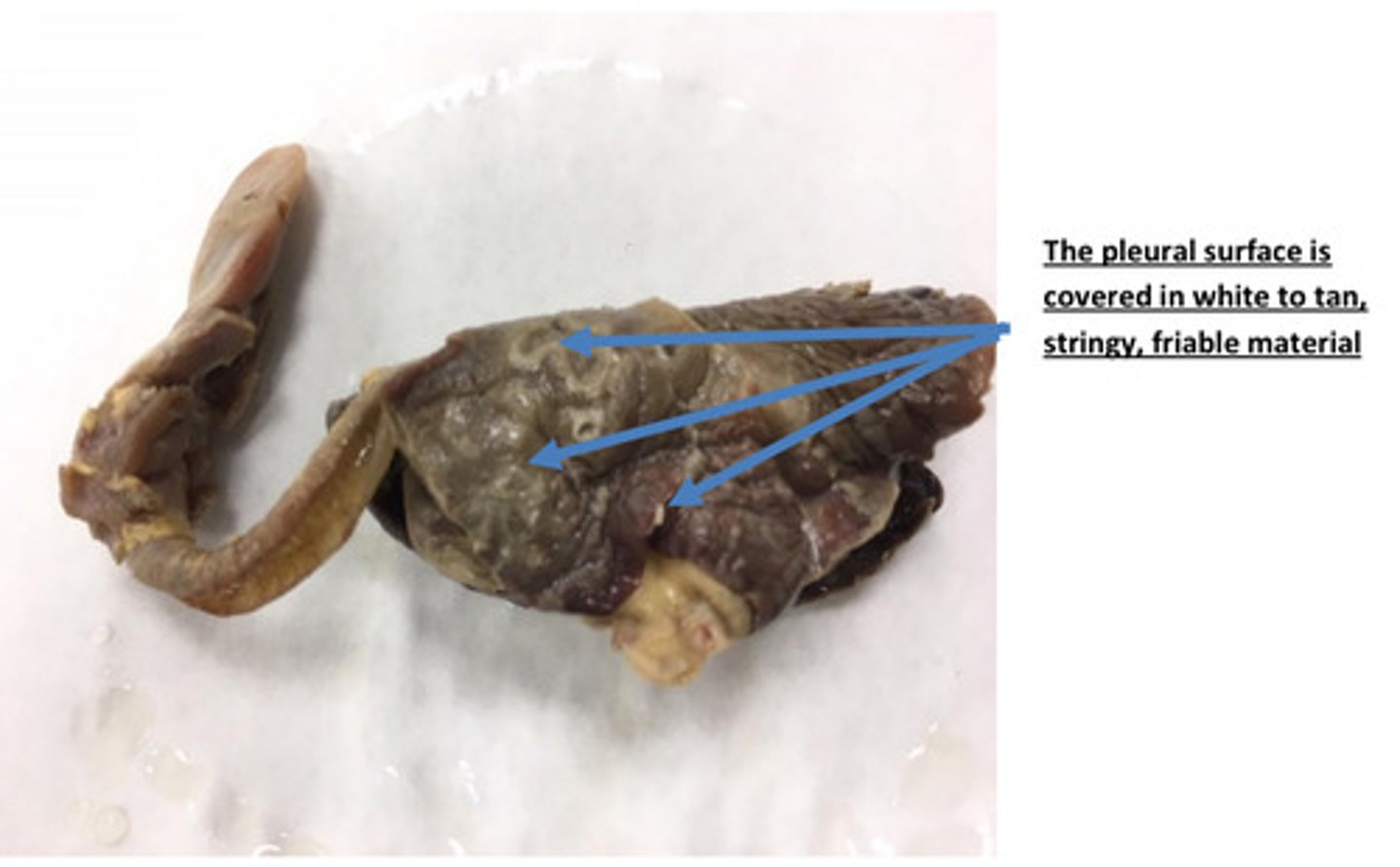
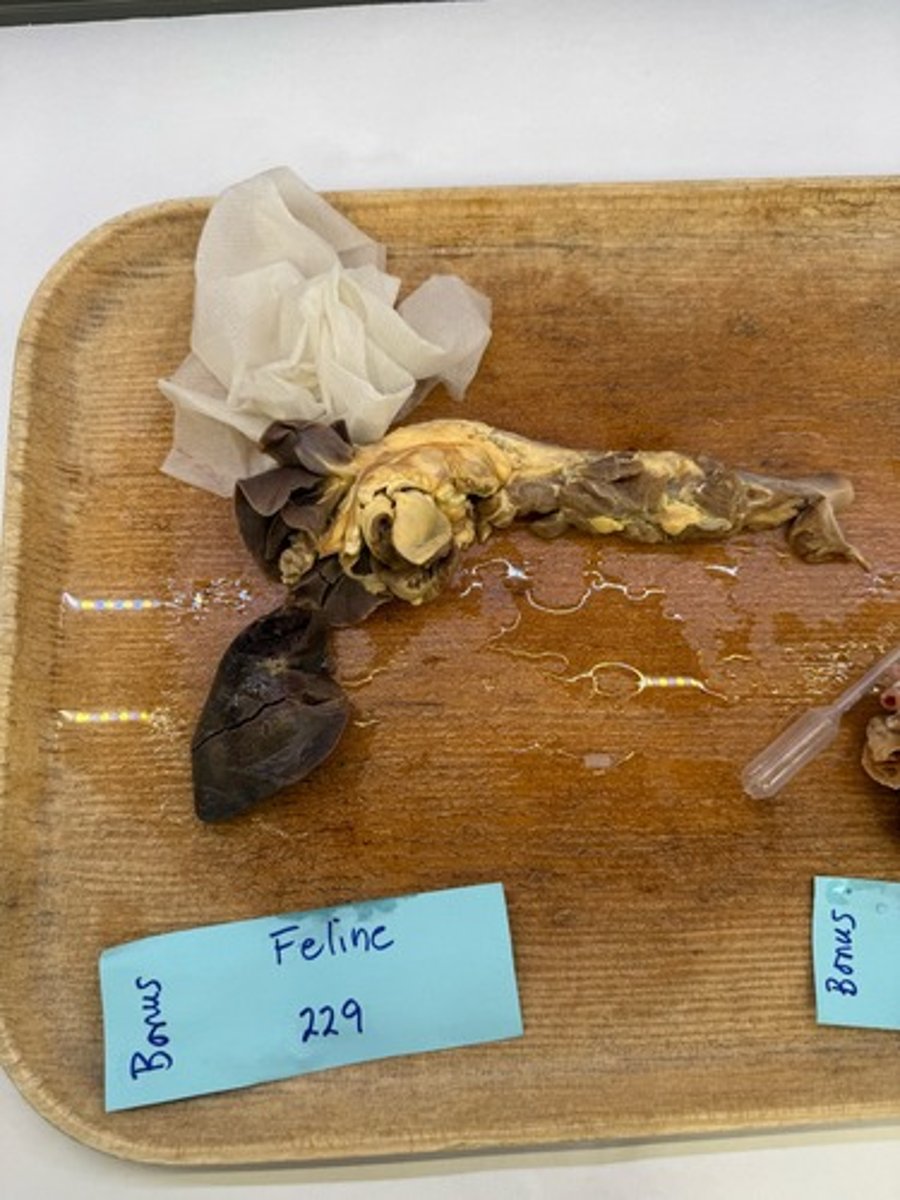
Pyothorax
The pleural space in this cat was filled with fibrinopurulent fluid. Fibrinopurulent fluid
consists of fibrin and neutrophils. What is the medical term used to describe a
pleural space that is filled with this purulent fluid?
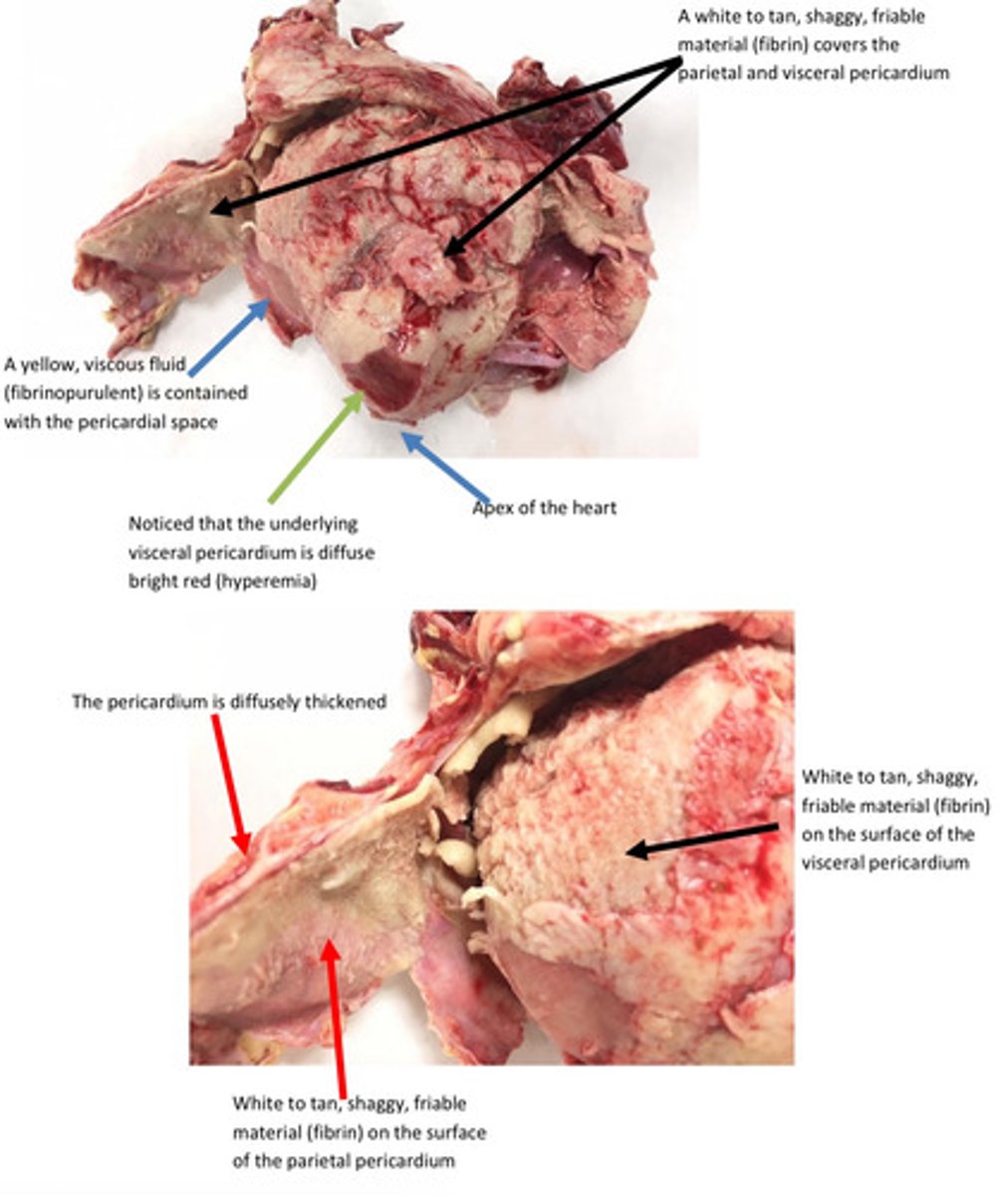
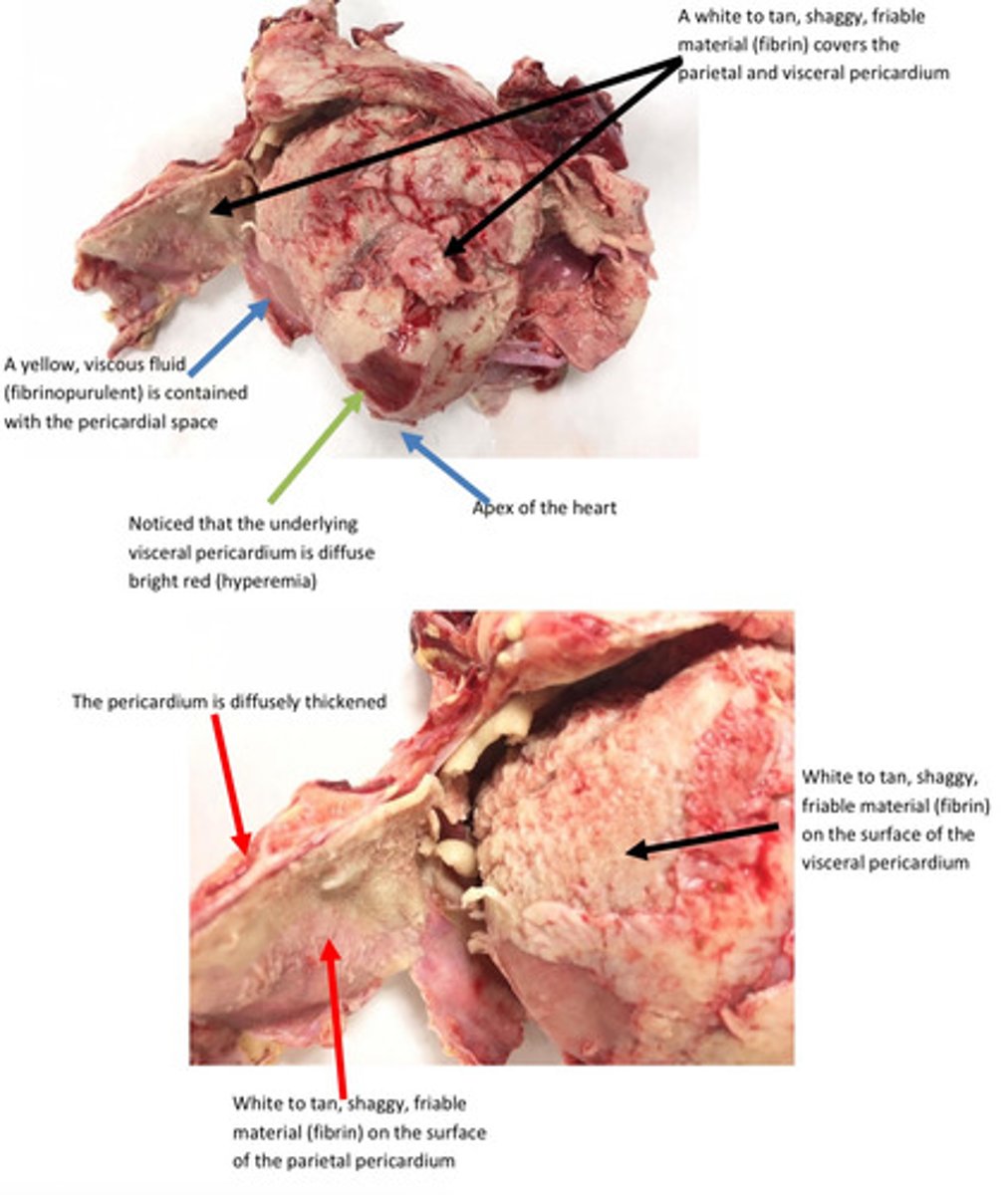
Pericardium, severe acute diffuse fibrinous pericarditis and pleuritis
Give morphological diagnosis
Pericardium, severe acute diffuse fibrinous pericarditis and pleuritis
Give morphological diagnosis

Infectious microbes are the most common cause of pericarditis, pleuritis, synovitis, and
peritonitis. Septicemia (bacteria within the bloodstream) usually results in
hematogenous spread of bacteria to serosal membranes and result in polyserositis
(inflammation of multiple serosal membranes).
What is the most likely cause for fibrinous inflammation in serous membranes
(pleura, pericardial, peritoneum)?
Hock joint: severe, acute, diffuse, purulent, synovitis and arthritis
Provide morphological diagnosis
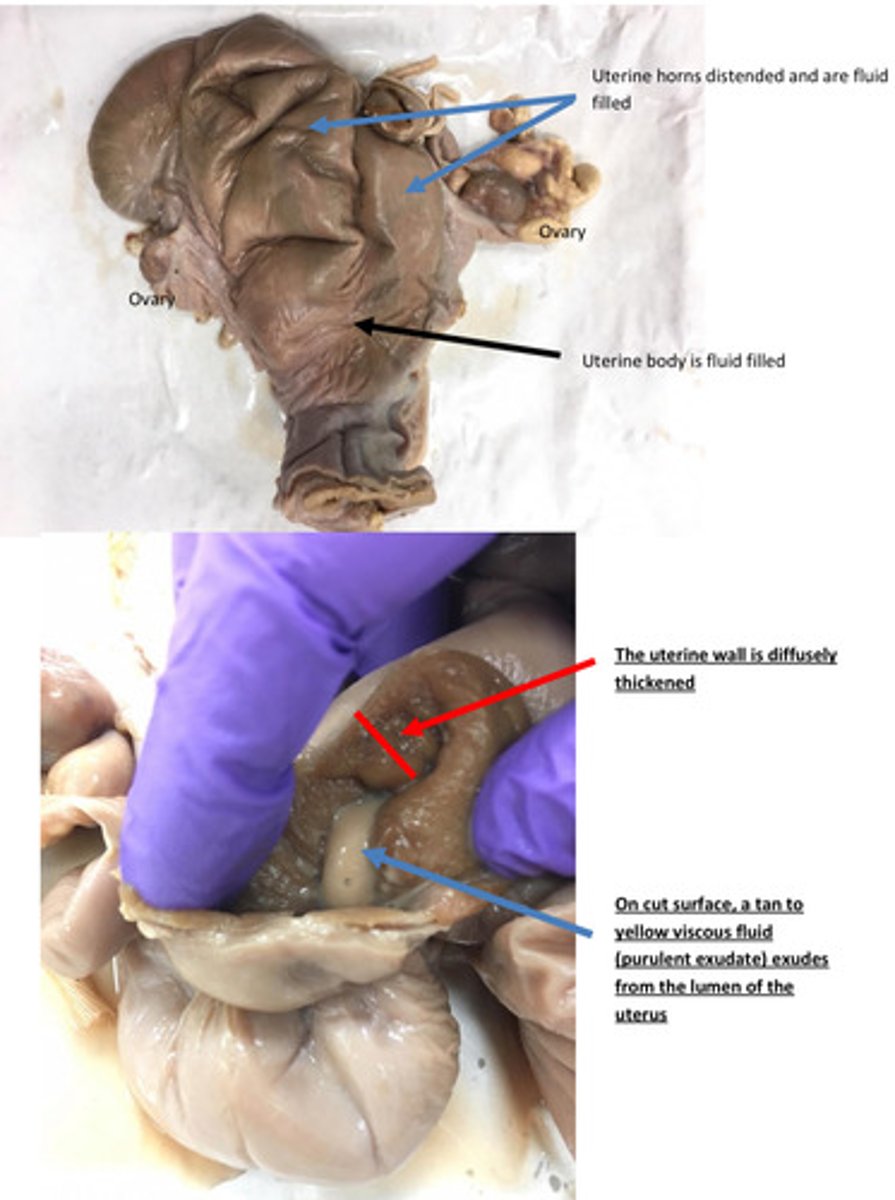
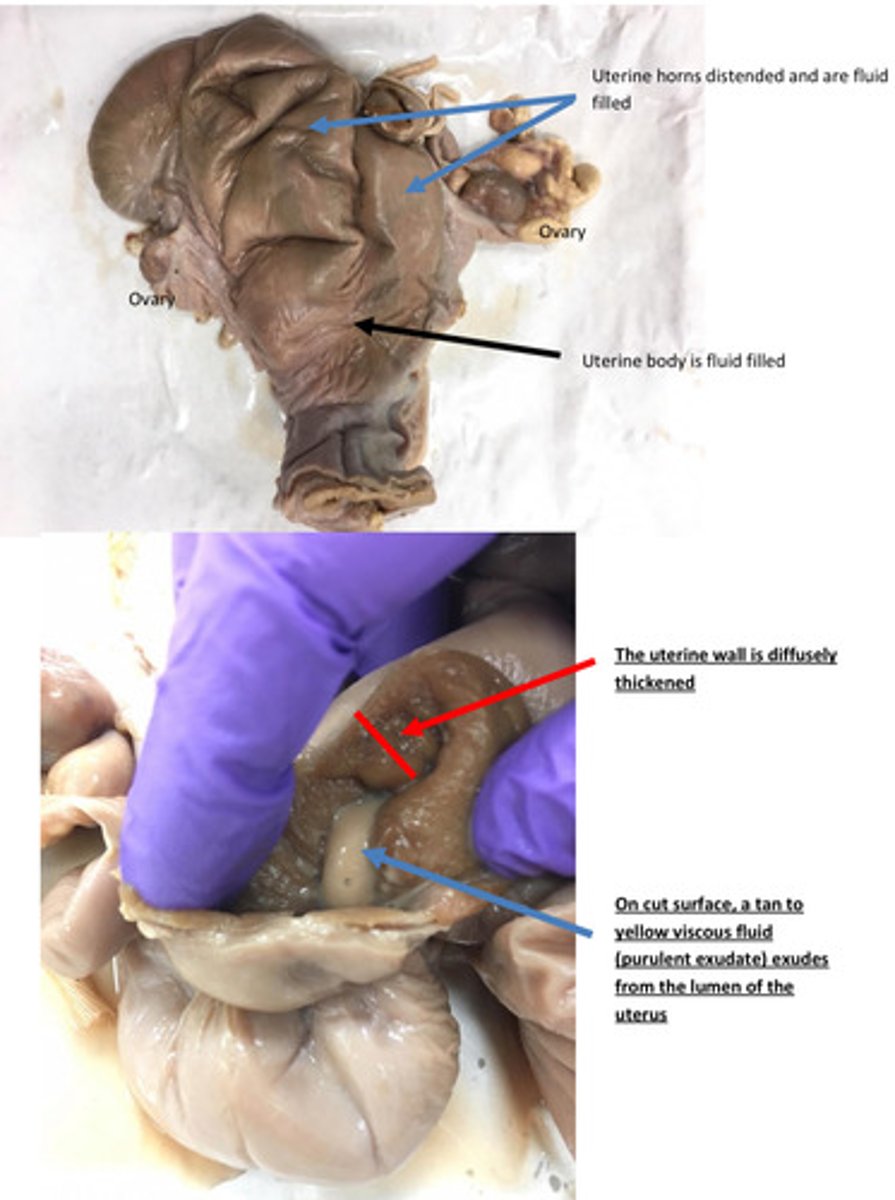
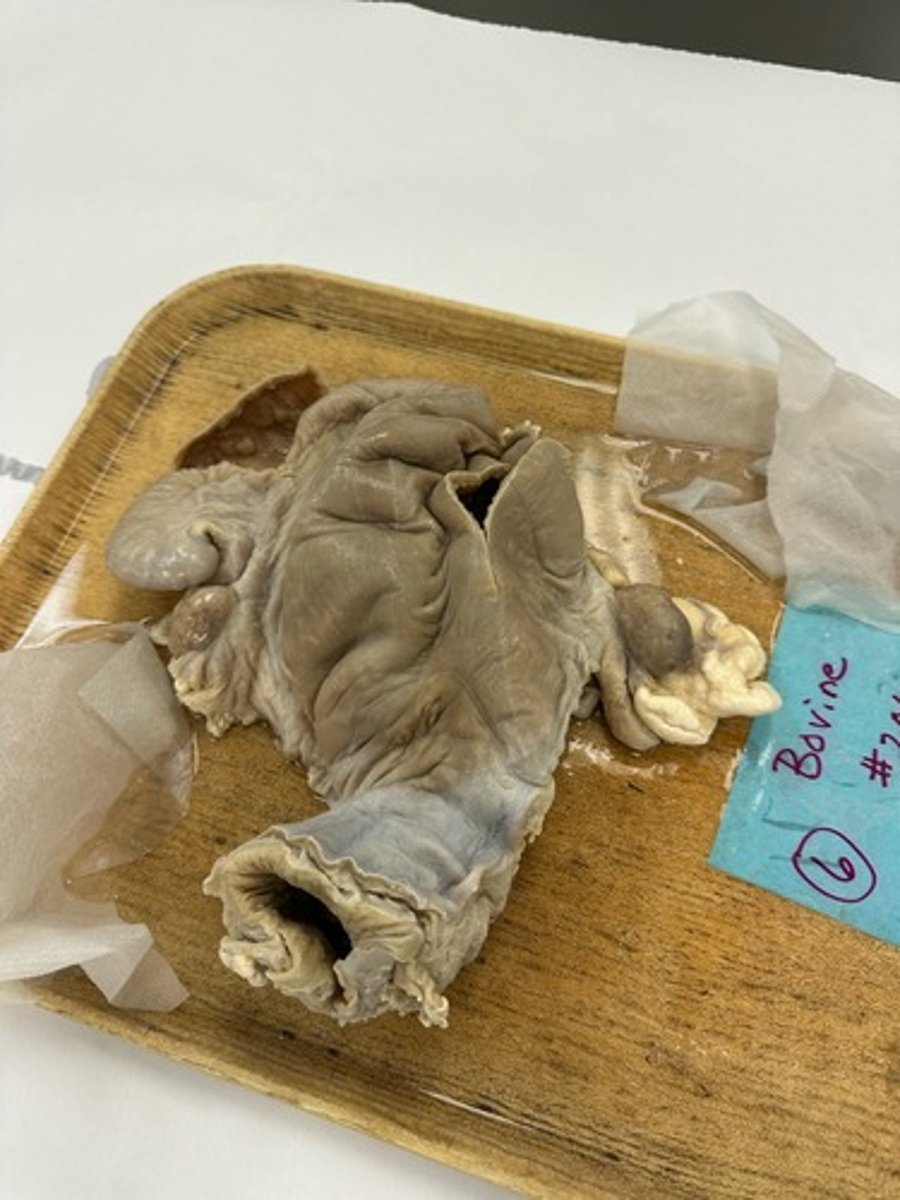
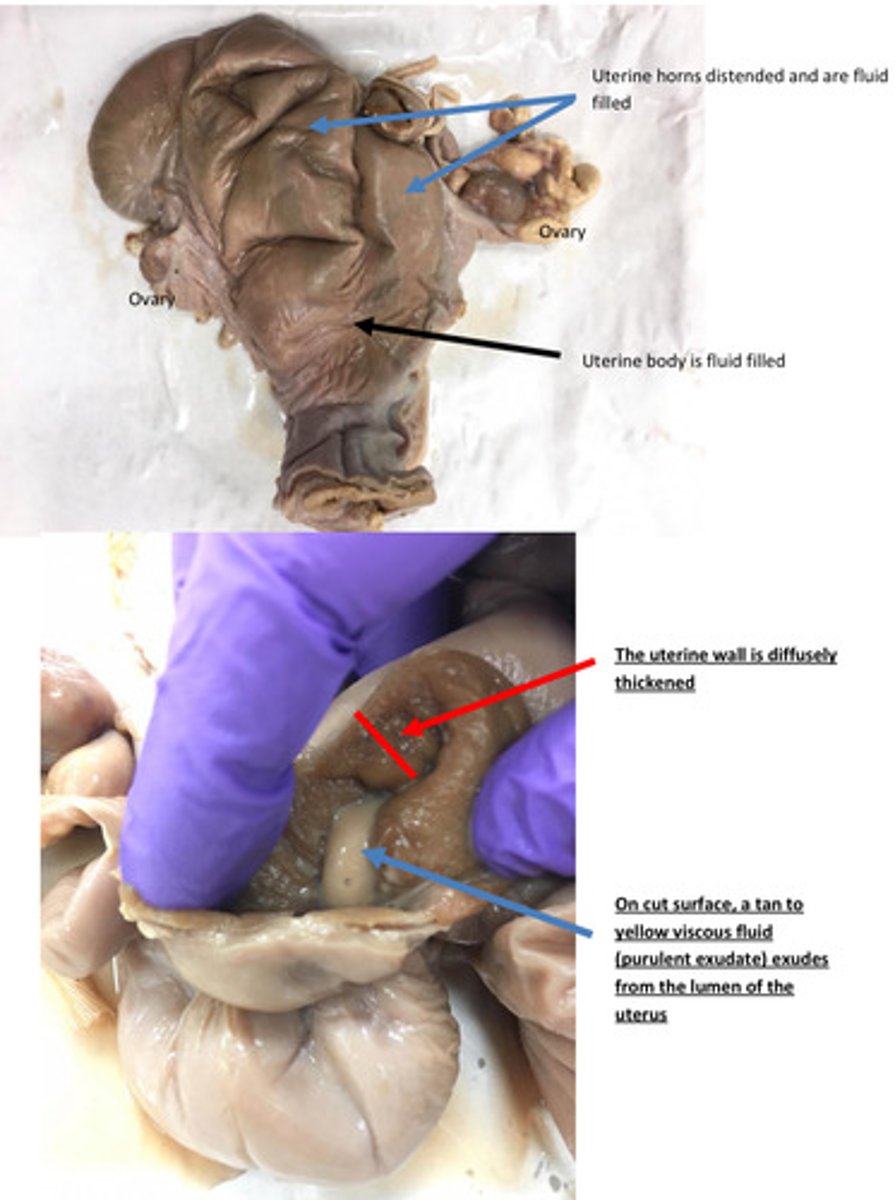
Pyometra
Name lesion
Pyometra
Name lesion
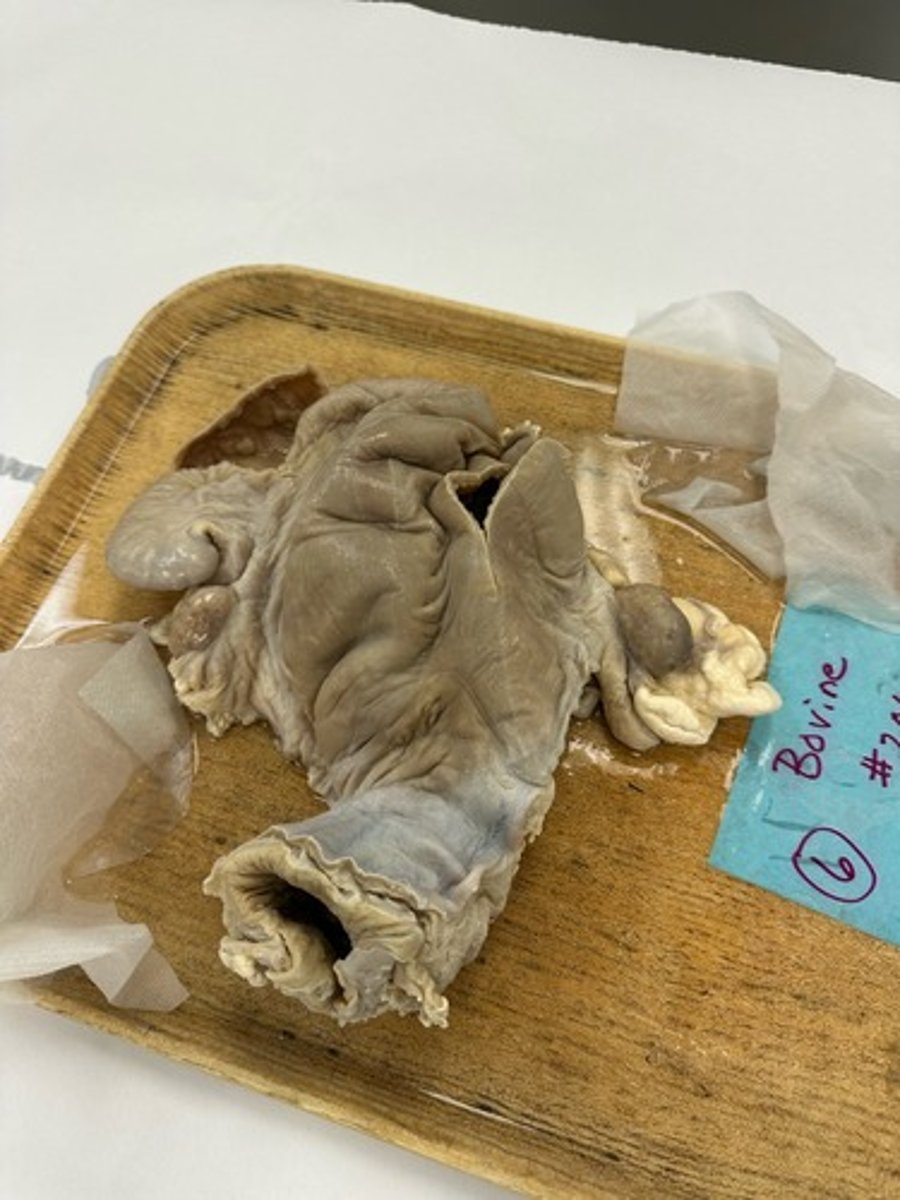
Uterus: severe acute diffuse purulent endometriosis
Provide morphological diagnosisq
Uterus: severe acute diffuse purulent endometriosis
Provide morphological diagnosis
The inflammation seen in this case is purulent or suppurative inflammation, meaning
neutrophil rich. The material is a purulent exudate. Purulent inflammation is a term used
to describe a pattern of acute inflammation in which the tissue response consists of
accumulation of fluid with a high concentration of plasma proteins and high numbers
neutrophils. Purulent exudate can be very liquid like or firm and crumbly depending on
the hydration status of the exudate
What is material within the lumen of uterus?
Uterus become contaminated with bacteria after parturition (usually after dystocia)→
early postpartum ovulation→ development of a persistent corpus luteum→ elevated
serum progesterone levels → Progesterone results in continued closure of the cervix
and stimulation for endometrial gland development and glandular secretion→ uterine
environment is ideal culture media for bacteria→ colonization of the endometrium
results in inflammation and formation of mucopurulent exudate
Provide a pathogenesis for this lesion in a bovine

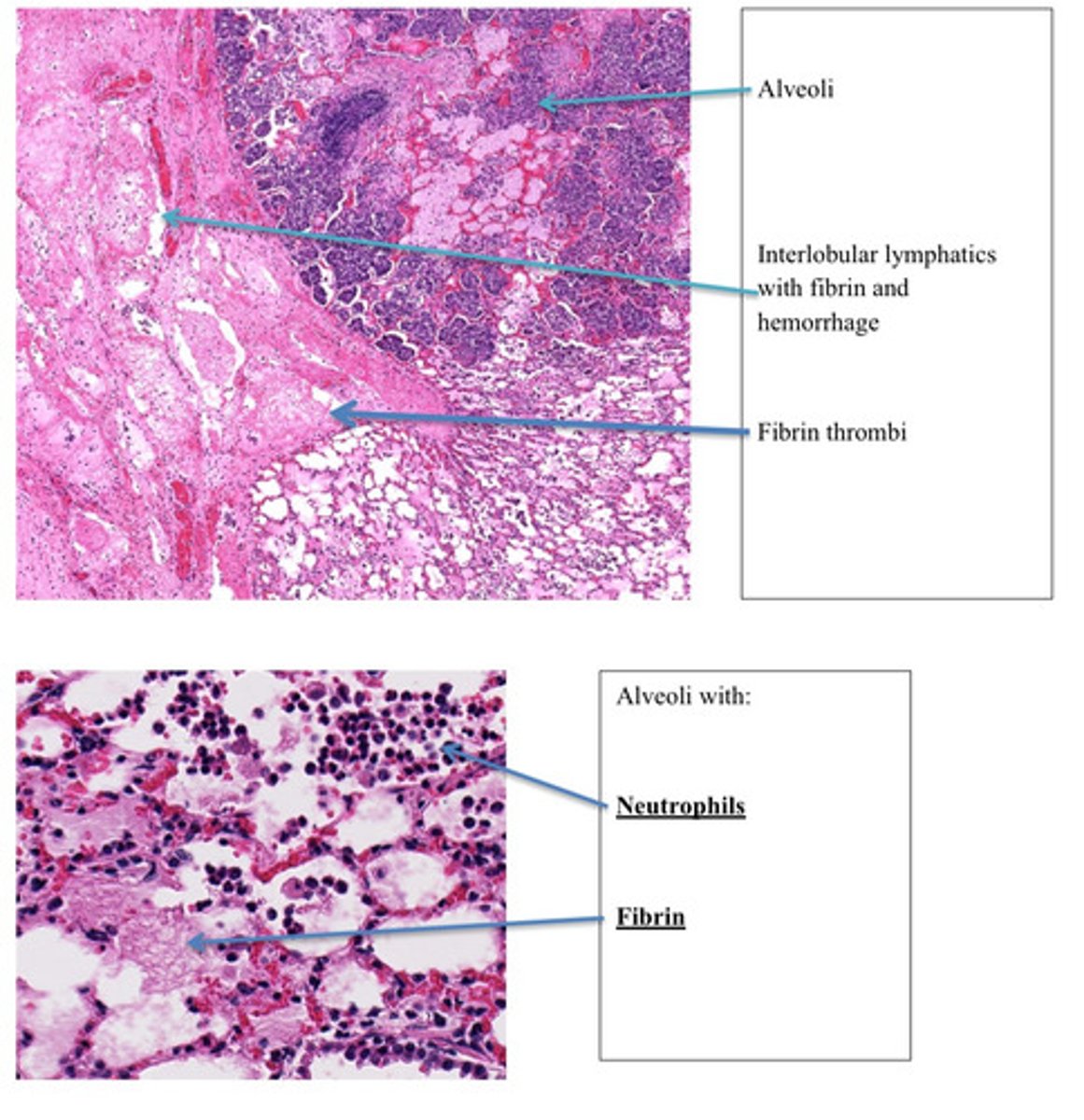
Lung, severe acute diffuse fibropurulent bronchipneumonia
Provide morphological diagnosis
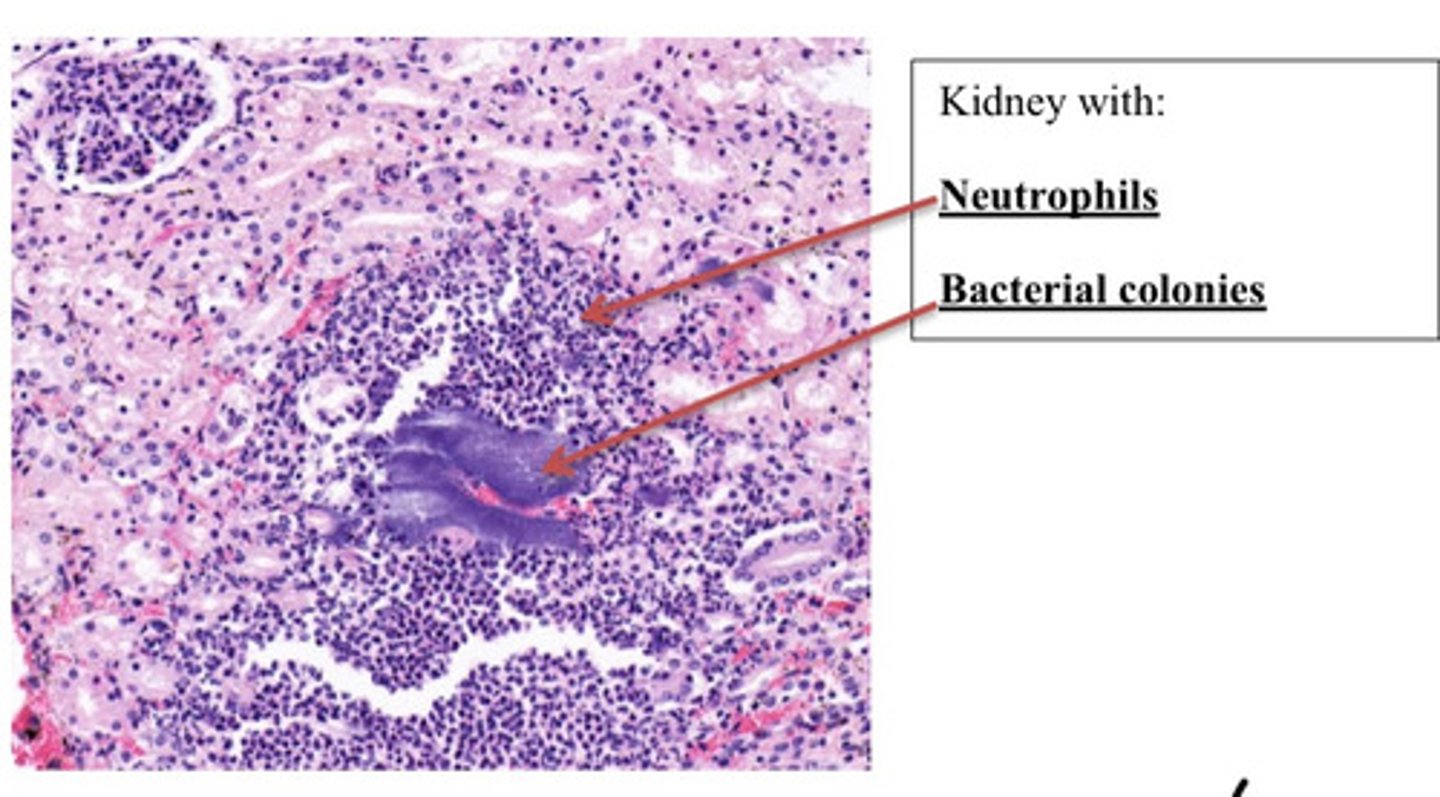
Kidney, severe acute Multifocal, purulent glomerulonephritis with bacterial colonies
Provide morphological diagnosis
Thrombus
What is this?
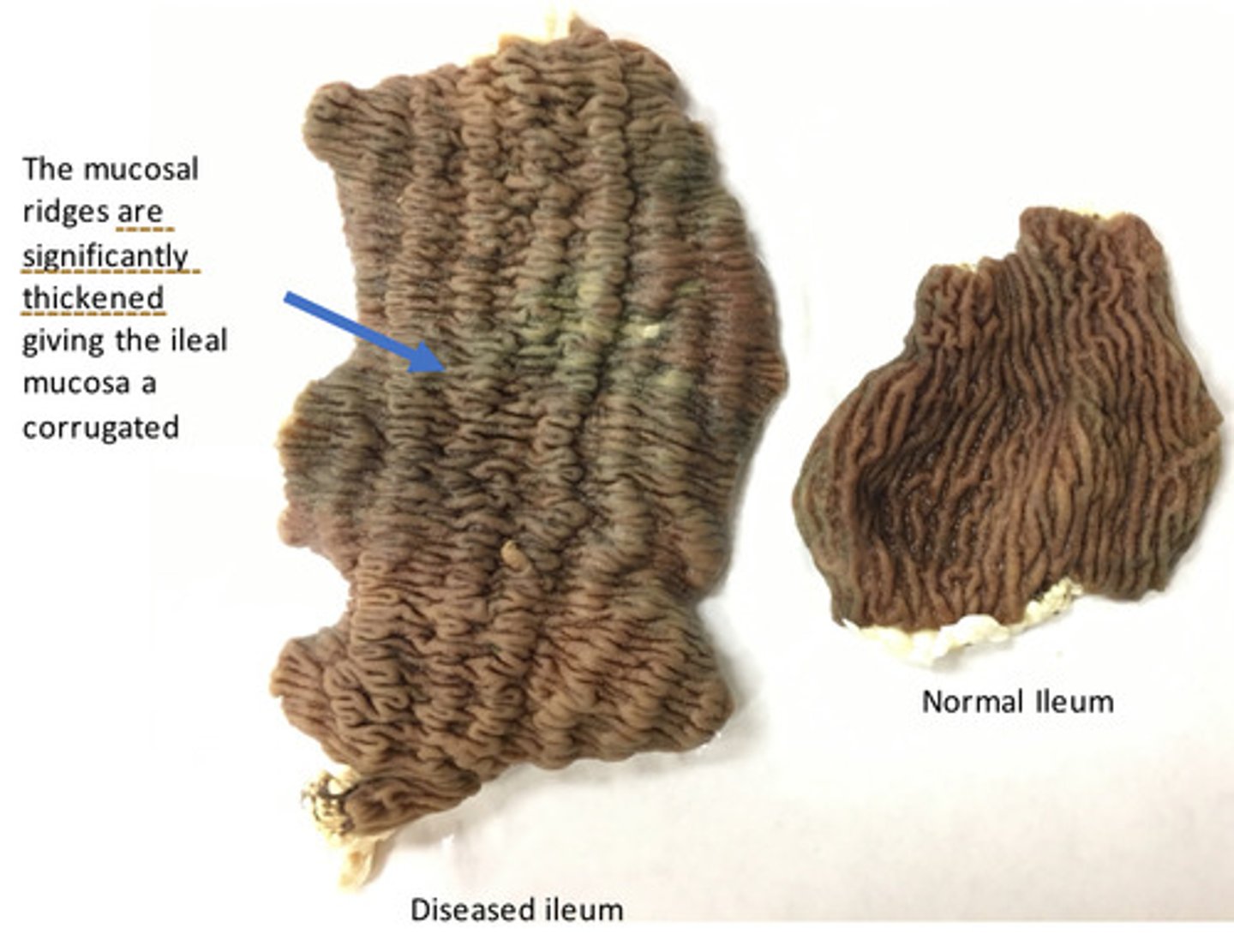
Ileum: severe, chronic, diffuse, granulomatous ileitis
Provide morphological diagnosis
Ileum: severe, chronic, diffuse, granulomatous ileitis
Provide morphological diagnosis
Macrophages
What cells are seen in granulomatous inflammation?
Certain pathogens like Mycobacterium avium subspecies paratuberculosis and Mycobacterium leprae are a cause of chronic inflammation that is characterized by non- caseating (does not form nodules) aggregates of macrophages. These lesions are poorly delineated, have a widespread distribution, a heavy intracellular bacterial burden, and numerous macrophages that expand the tissues without any fibrous capsule. (DRIVEN BY A TH2 Helper Response)
Describe diffuse granulomatous inflammation
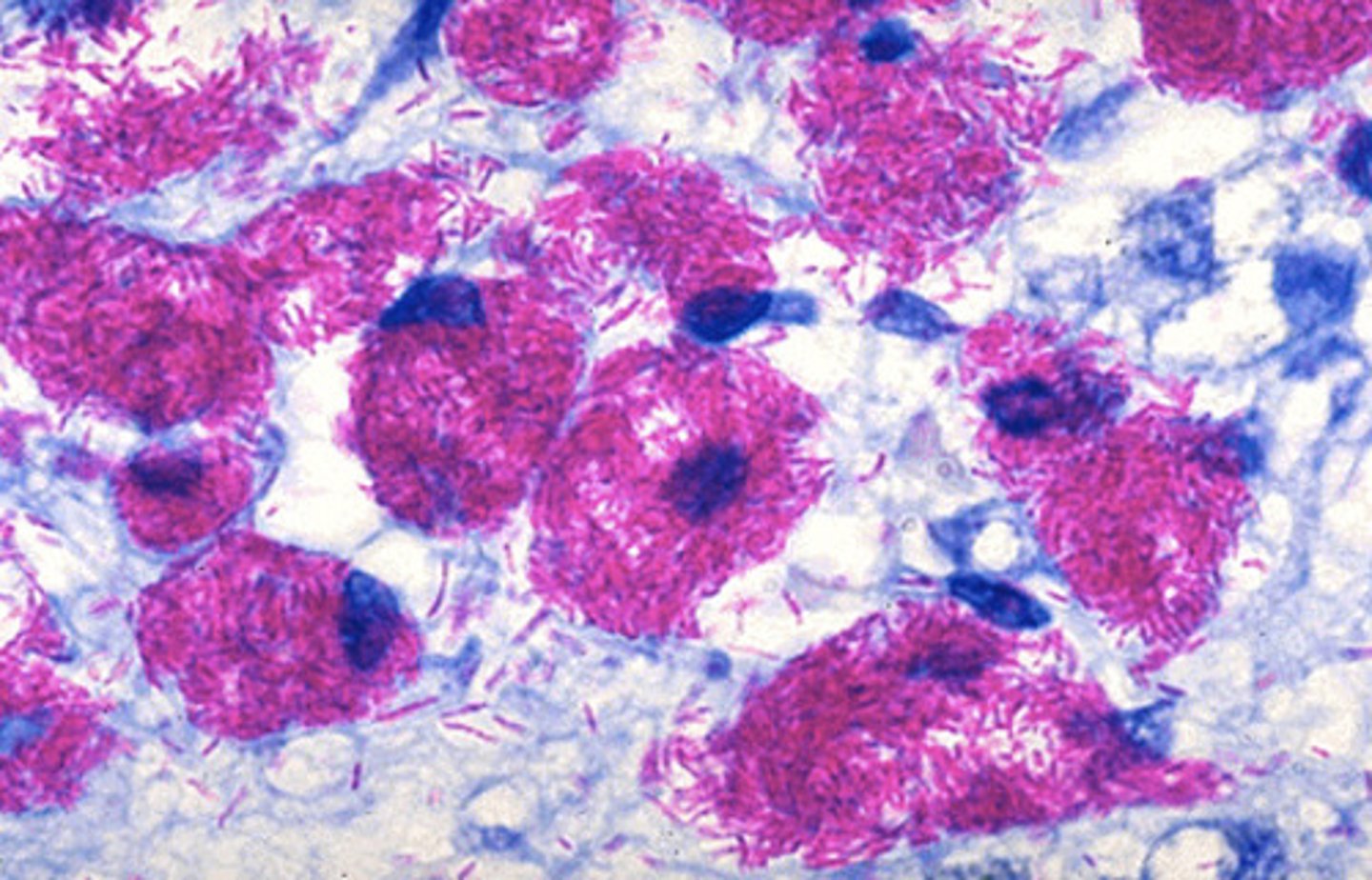
Tuberculoid (nodular) granulomas are those seen in Mycobacterium bovis or sometimes Mycoplasma bovis (examine case 2 for an example). Grossly, nodular granulomas are gray to white, round to oval, firm to hard, and are well demarcated. Tuberculoid granulomas are well delineated, have a confined distribution, and commonly have a fibrous component. (DRIVEN BY A TH1 Response)
Describe tuberculoid/nodular granulomatous inflammation
The bacteria taking up stain in this case is mycobacterium avium subspecies paratuberculosis. M. avium subspecies paratuberculosis is the cause of Johne's disease in cattle.
An acid fast stain was performed on the ileum, what pathogen is taking up the stains in the slide?
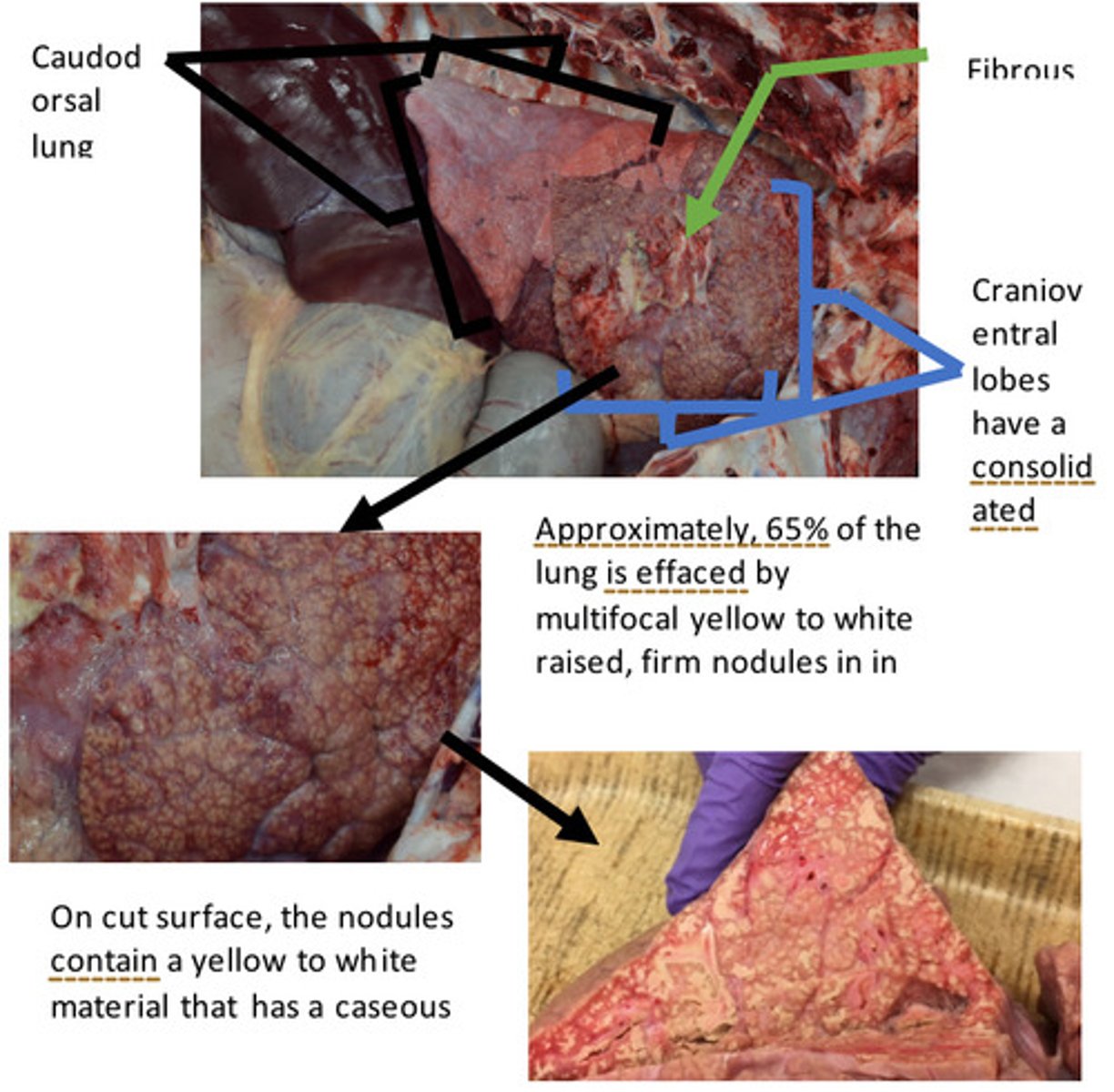
Lungs: Severe, chronic, bilateral, locally extensive, cranioventral bronchopneumonia with multifocal abscesses, caseating granulomas, and extensive fibrous adhesions
Provide morphological diagnosis
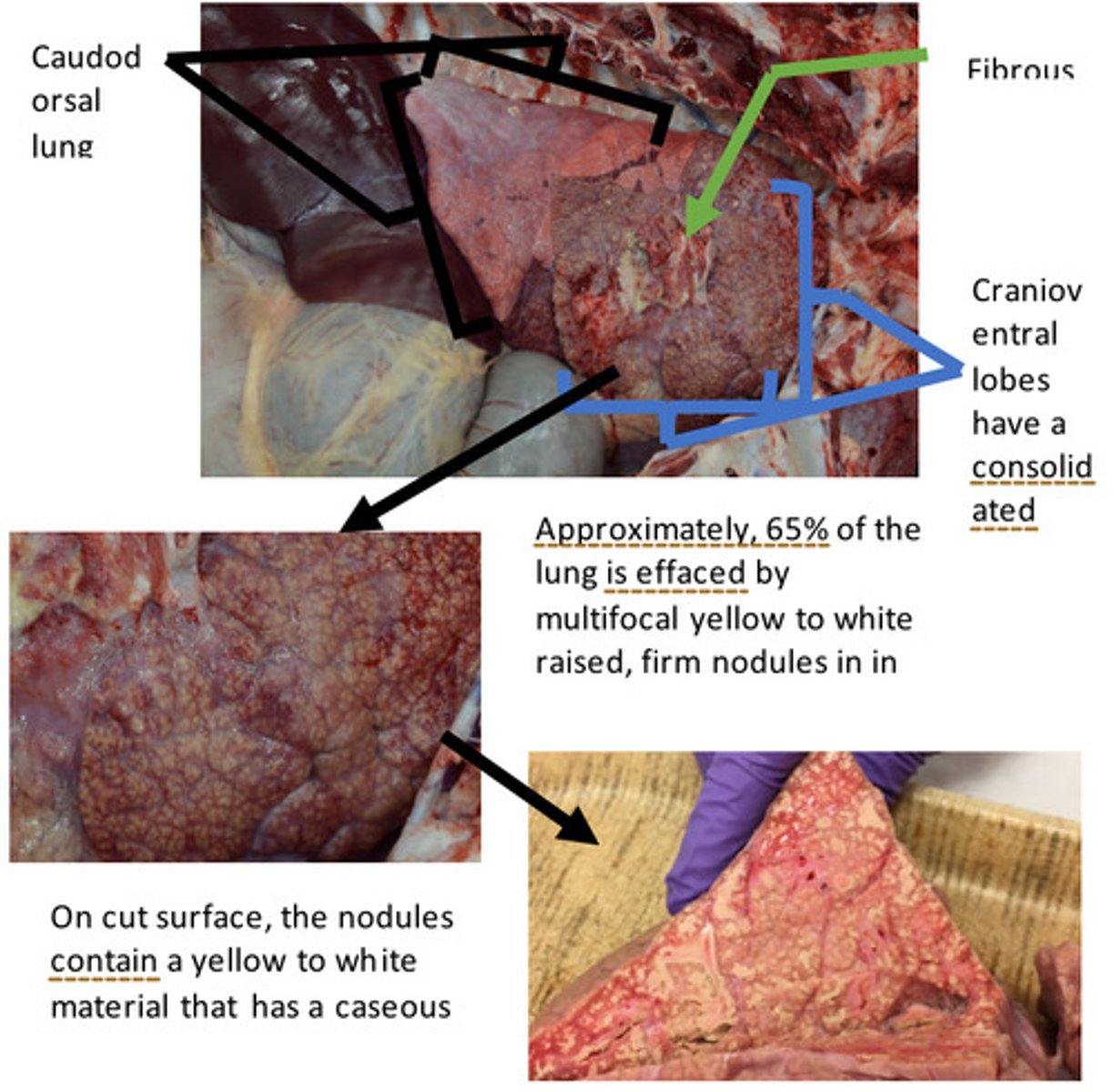
Lungs: Severe, chronic, bilateral, locally extensive, cranioventral bronchopneumonia with multifocal abscesses, caseating granulomas, and extensive fibrous adhesions
Provide morphological diagnosis
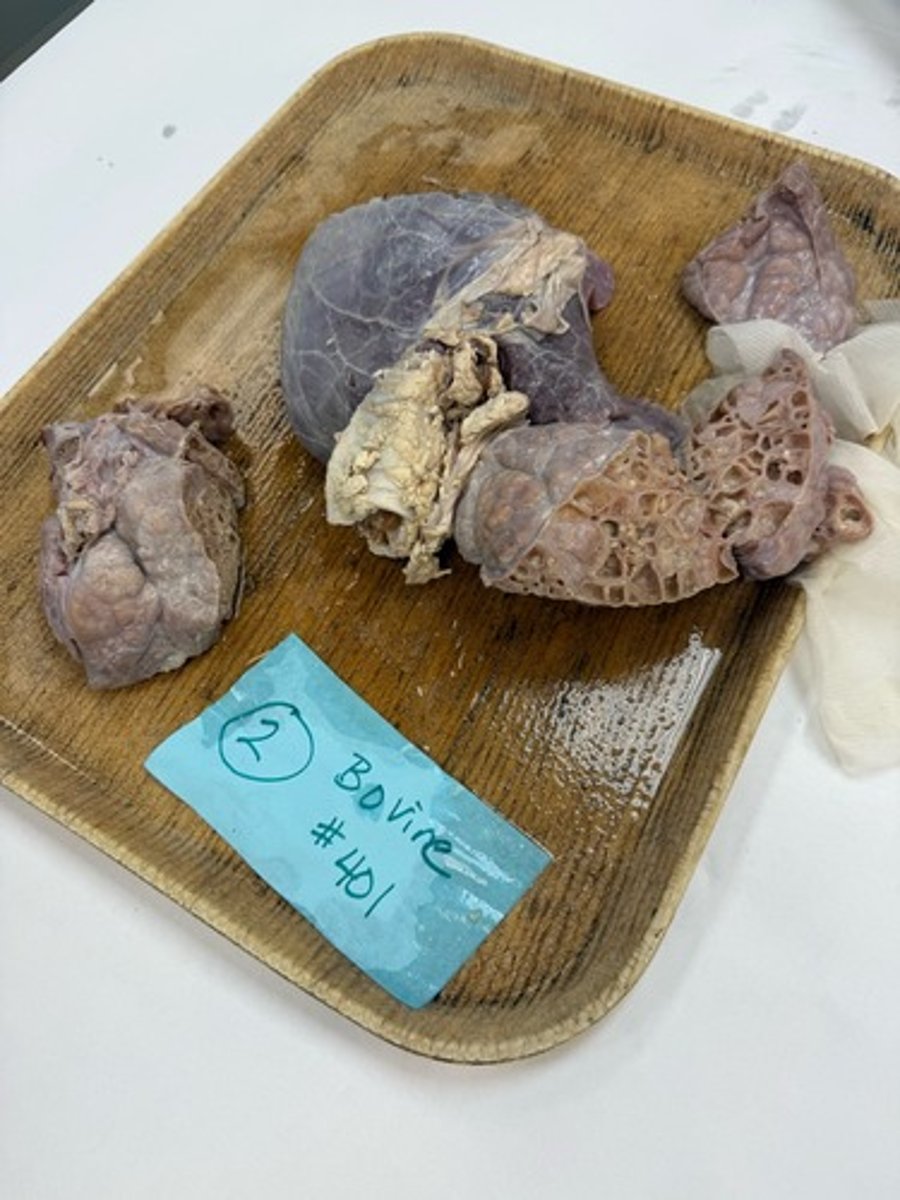
There are several features seen in this lesion that represent chronic inflammation. There is presence of fibrous tags on the pleural surface and the interlobular septa are expanded by fibrous connective tissue. It takes days to weeks for fibrous connective tissue to form, thus, its presence indicates a CHRONIC process. The cranioventral aspect of the lungs contains numerous foci of caseous necrosis (remember back to the discussion and lab on necrosis). Caseous necrosis is a more chronic lesion and is characterized by a coagulum of cellular debris inflammatory cells (macrophages and neutrophils). There are also multiple abscesses through the cranioventral aspect of the lungs (see case 1 for more information on abscesses).
What makes this lesion chronic?
Fibrin is the main protein in a fibrinous exudate. Fibrinous exudate results from increased vascular permeability that allows fibrinogen to get out of the vasculature into the tissue. In the tissue fibrinogen is cleaved by proteases to fibrin, which polymerizes. Grossly, fibrin is yellow to white to tan, stringy material that is easily peeled off.
Fibrous tags occur in areas of chronic inflammation. Fibrous tags are composed of fibroblasts and collagen fibers. In contrast to fibrin, fibrous tags are tough, not easily broken down, and are adherent
How does fibrous tag differ from fibrin?
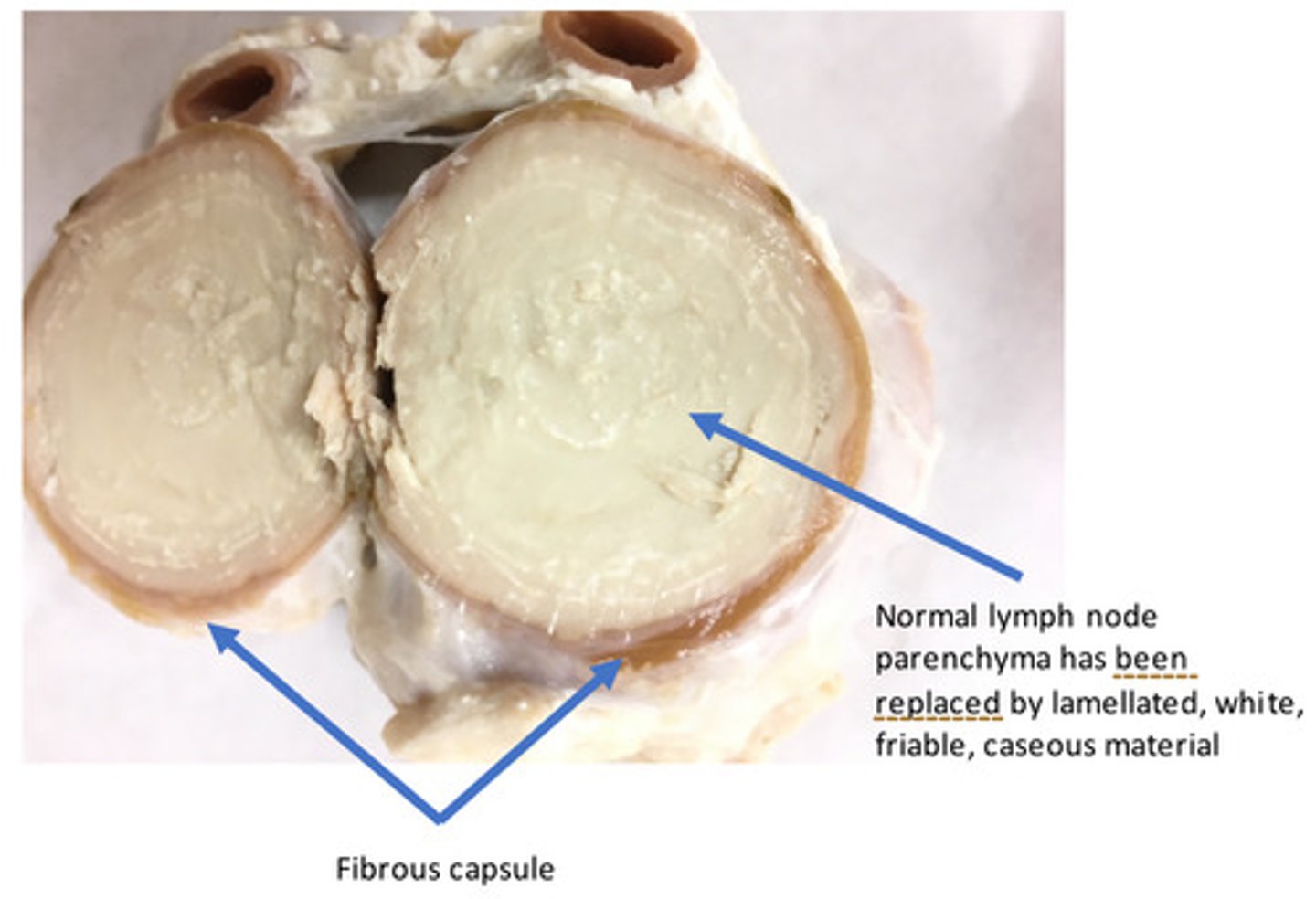
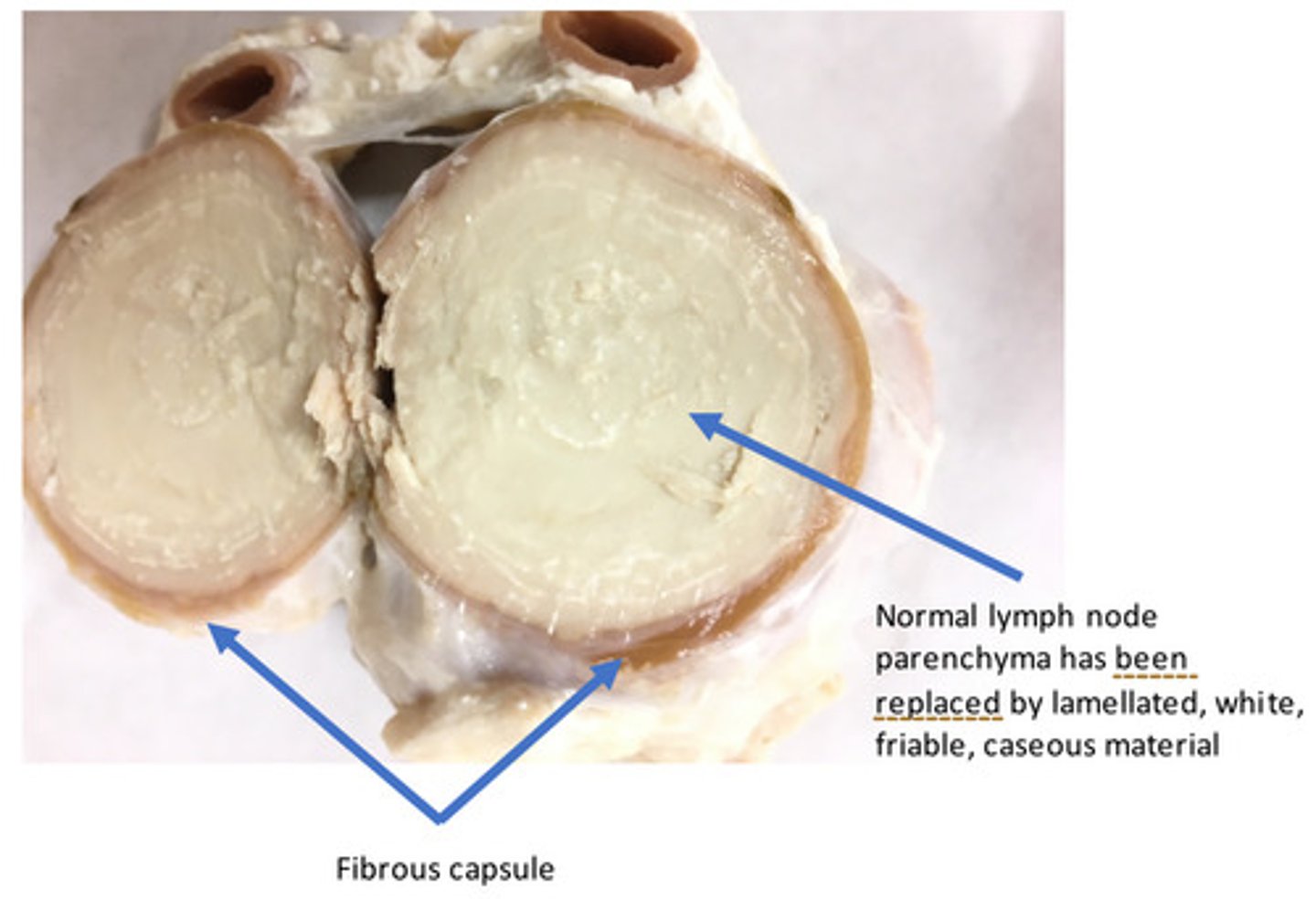
Lymph nodes: Severe, chronic, diffuse (within each lymph node affected), caseous, lymphadenitis
Provide morphological diagnosis
Lymph nodes: Severe, chronic, diffuse (within each lymph node affected), caseous, lymphadenitis
Provide morphological diagnosis

Corynebacterium pseudotuberculosis (formerly C. ovis)
What bacterial organism would cause this lesion in a sheep?
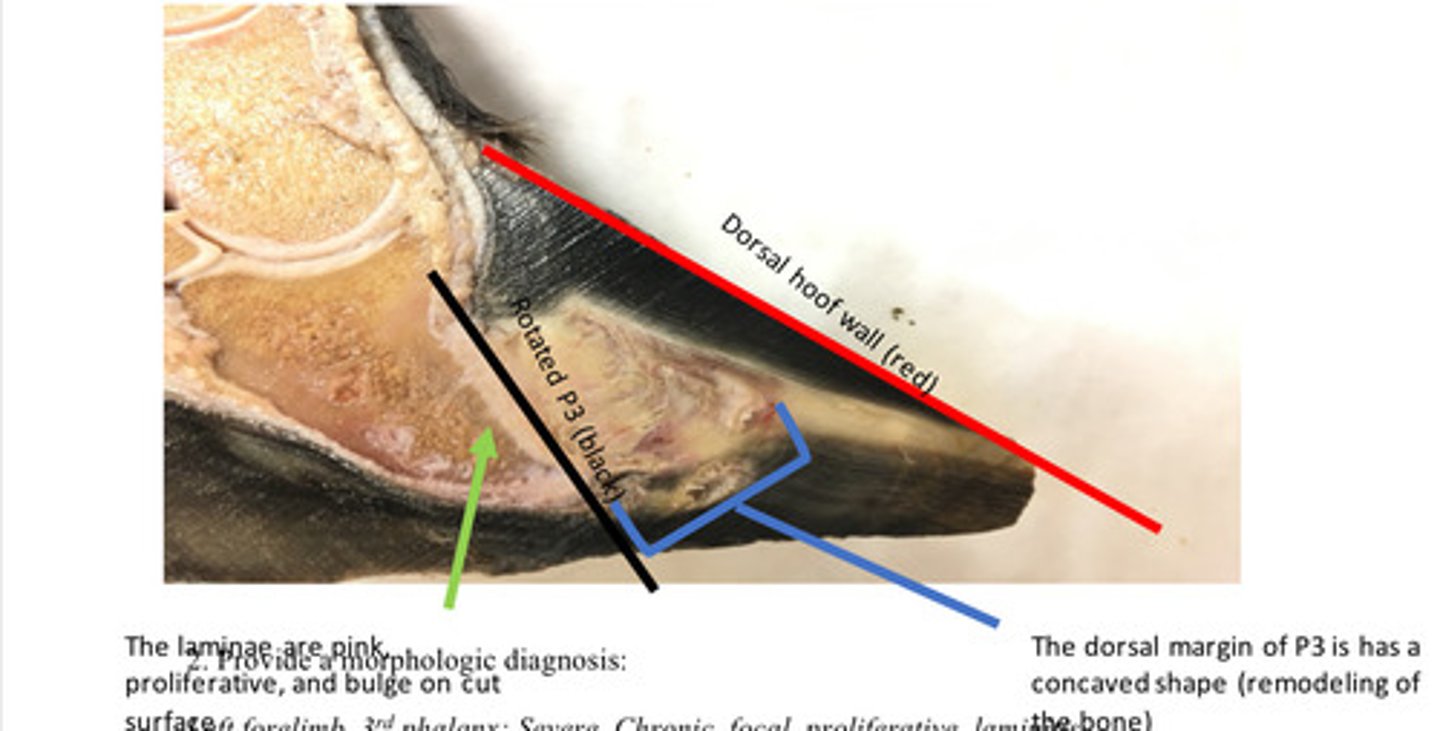
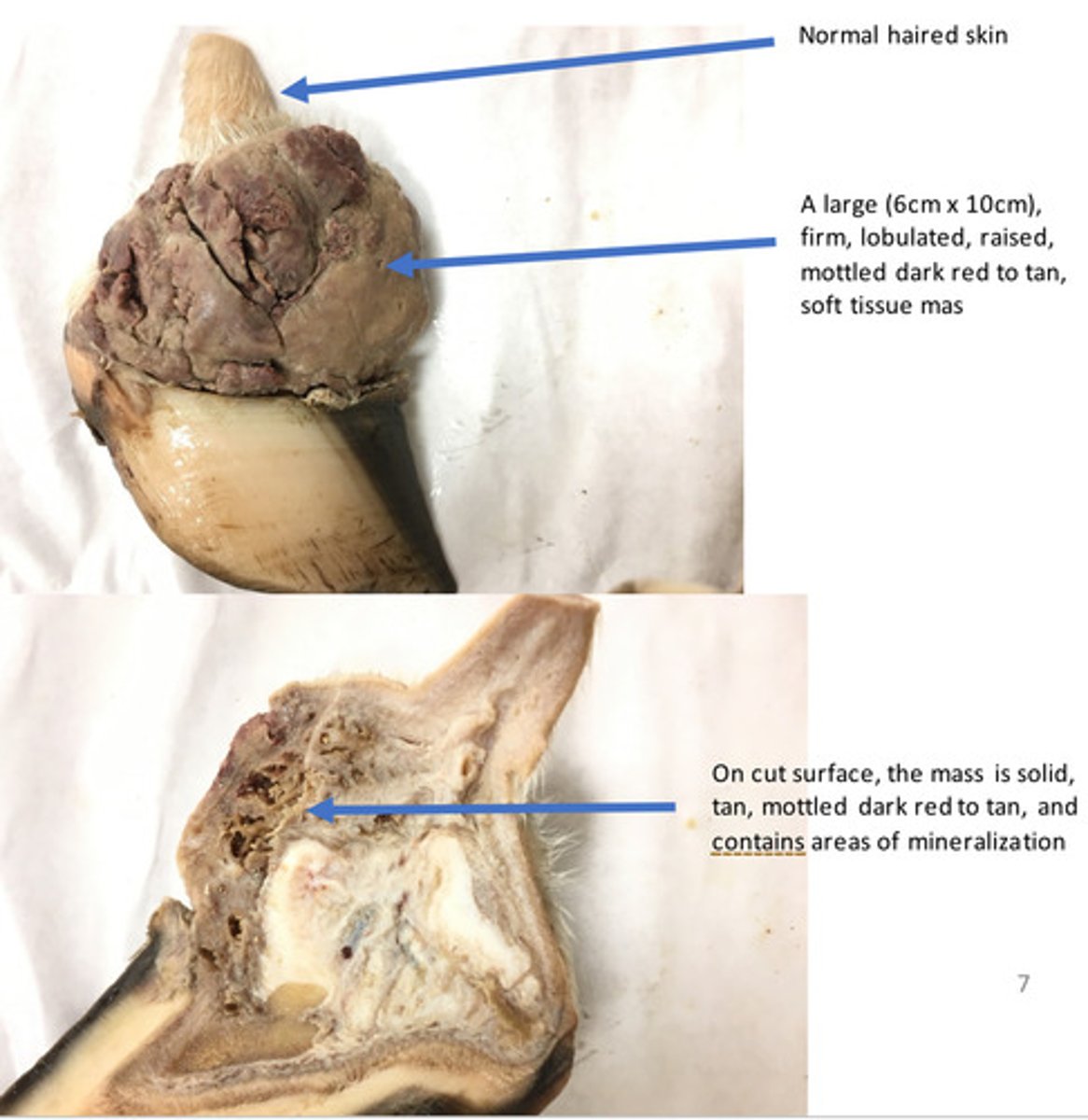
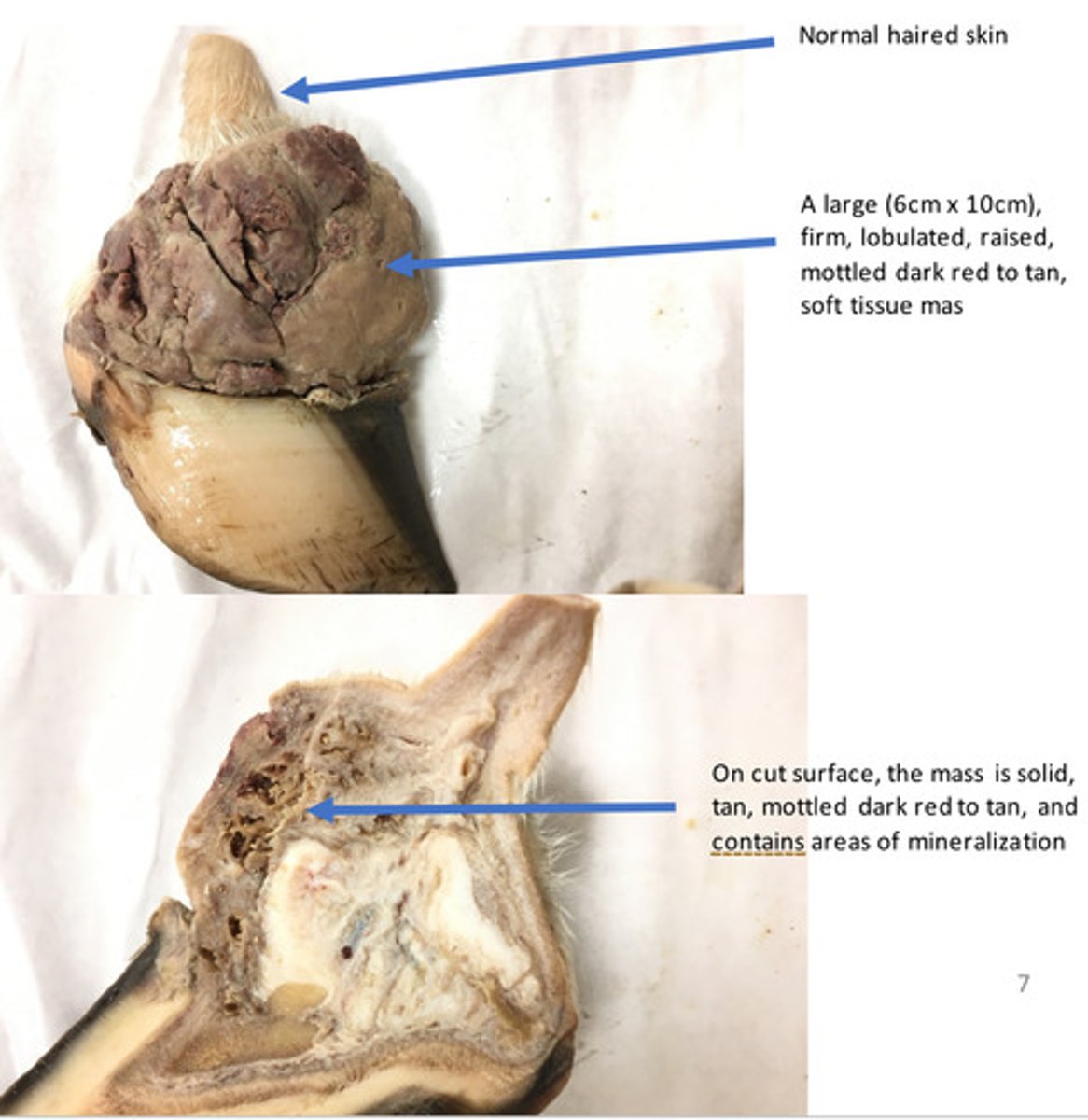
Left forelimb, 3rd phalanx: Severe, Chronic, focal, proliferative, laminitis
Provide morphological diagnosis
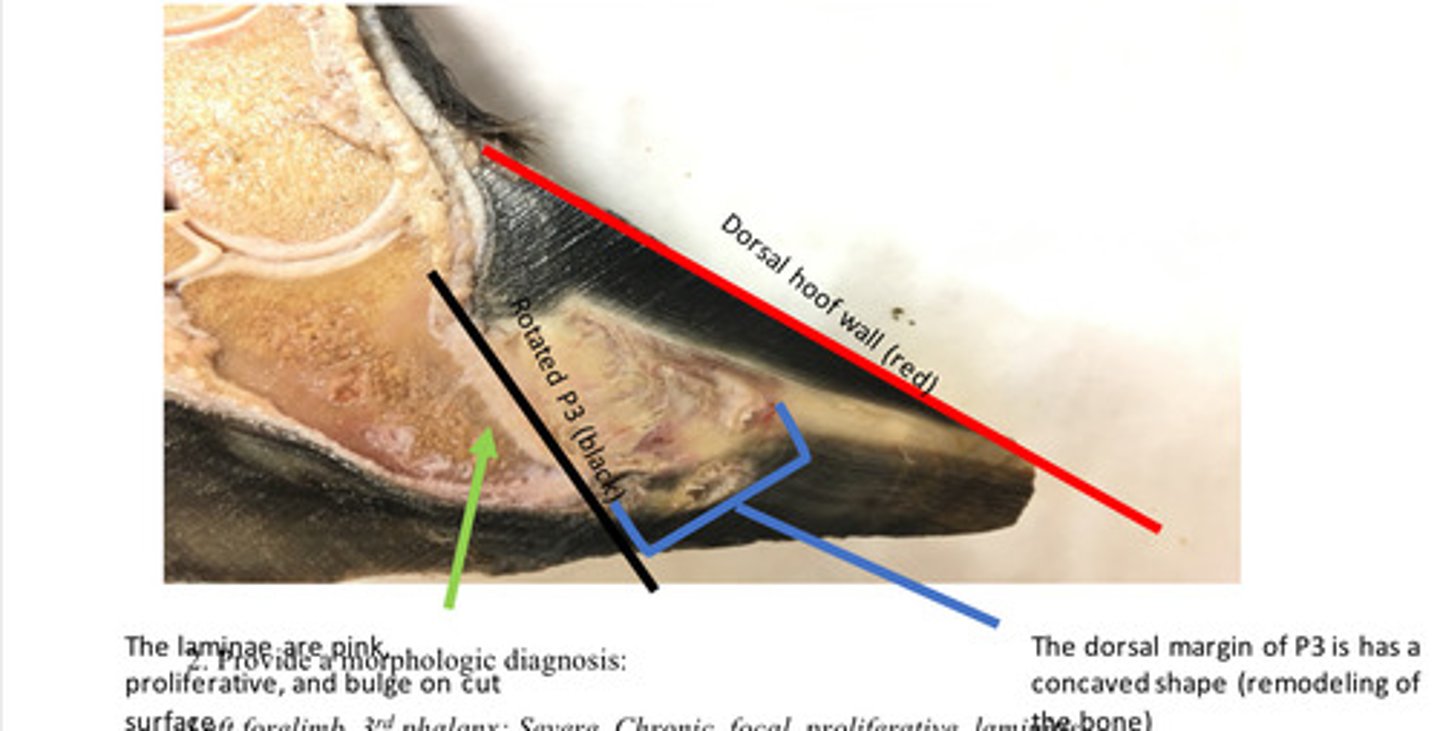
This is a chronic lesion. Chronic laminitis (sometimes called founder) is characterized by rotation of P3 away from the dorsal hoof wall. The features that make this a chronic lesion are the remodeling of P3 (boney changes) and the proliferation or hyperplasia of the laminae. Chronic laminitis results from damage to the laminae (interdigitation between the dermis and epidermis of the hoof). When the laminae are damaged, the interdigitation between the dermis and epidermis is disrupted. The disruption of the dermis and epidermis is the reason that P3 rotates away from the dorsal hoof wall. Irregular hyperplasia of the epidermal lamellae commonly form an irregular triangle shaped mass called the lamellar wedge.
Is this chronic or acute and why?
Right forelimb, coronary band: Severe, chronic, focal, exuberant granulation tissue (proud flesh)
Provide morphological diagnosis
Granulation tissue is a fibrovascular tissue that is produced by the body to fill in spaces or defects. Granulation tissue forms in about 1-2 weeks. Grossly, granulation tissues is tan to gray, friable tissue that readily bleeds when debrided away. Histologically, granulation tissue consists of numerous blood vessels that are perpendicular to fibroblasts. Normally, in about 3-6 weeks granulation tissue will organize and will be replaced by immature fibrous connective tissue that is poorly collagenized. After several weeks to months, this immature fibrous connective tissue will collagenize and form mature fibrous tissue (scar) and the healing process will be complete. In horse, the formation of granulation tissue in the distal limb can be excessive. This is known as exuberant granulation tissue and this can lead to a type of hypertrophic scar called proud flesh.
What is granulation tissue?
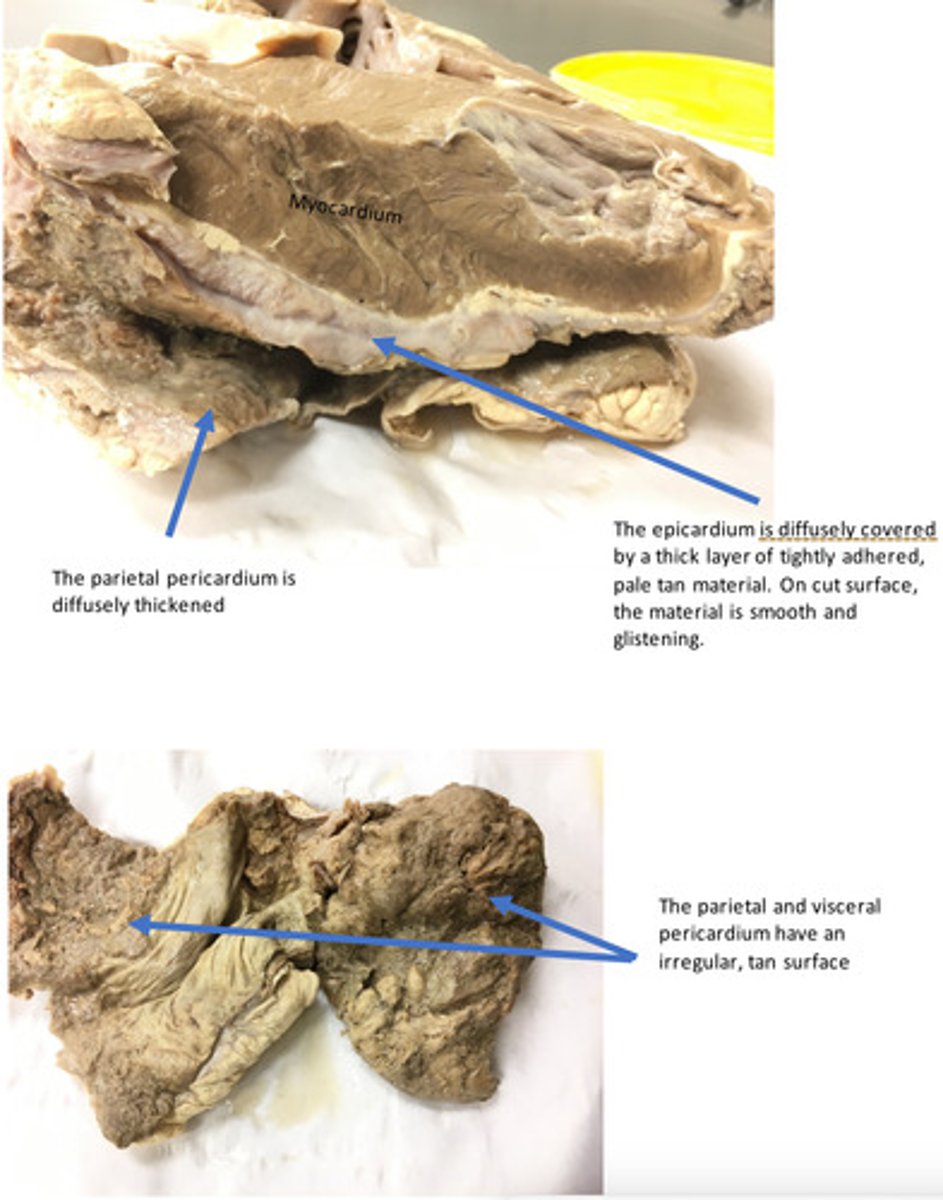
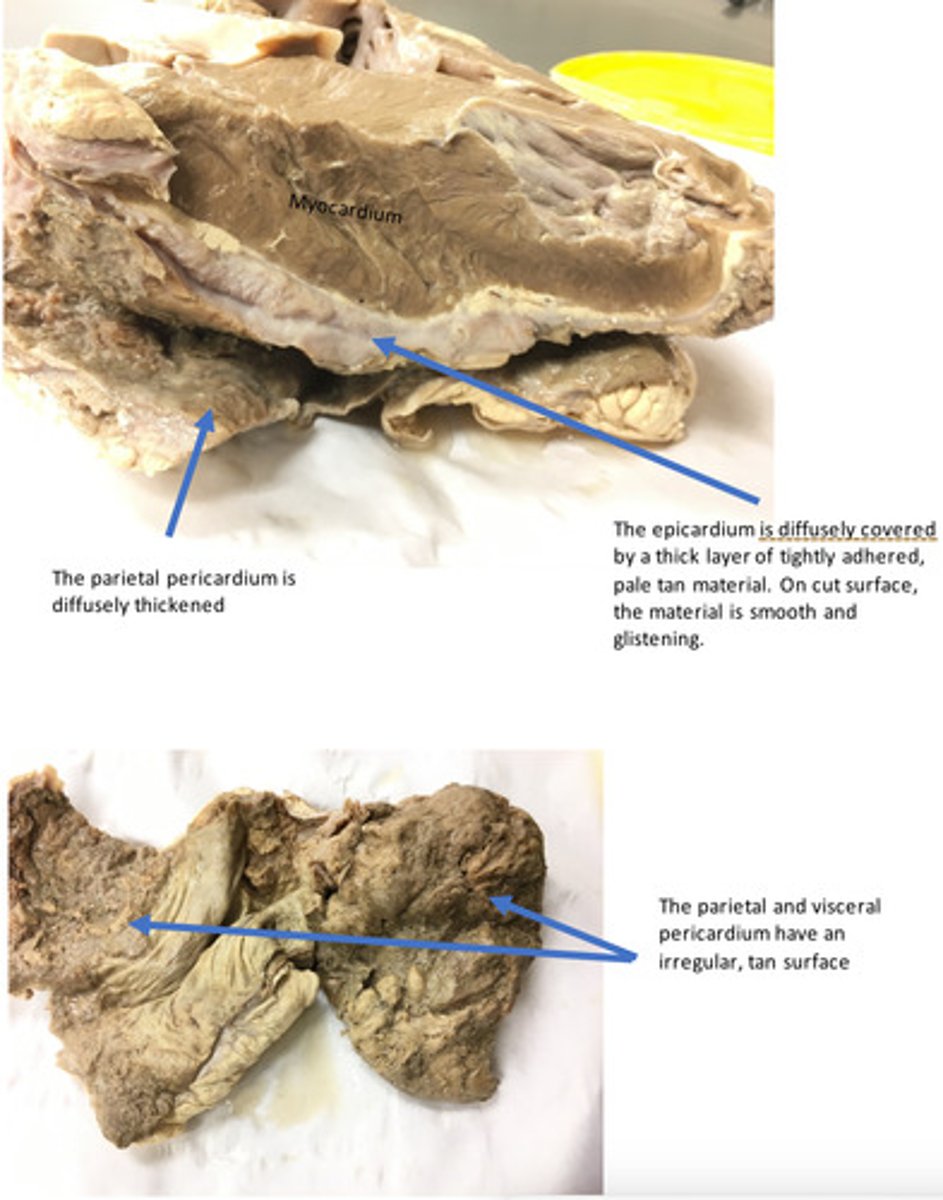
Heart, epicardium and pericardium: Severe, chronic-active, diffuse, epicarditis and pericarditis (hardware disease/ traumatic reticulopericarditis) (there is FIBRIN and FIBROUS connective tissue - acute and chronic findings.
Provide morphological diagnosis
Heart, epicardium and pericardium: Severe, chronic-active, diffuse, epicarditis and pericarditis (hardware disease/ traumatic reticulopericarditis) (there is FIBRIN and FIBROUS connective tissue - acute and chronic findings.
Provide morphological diagnosis
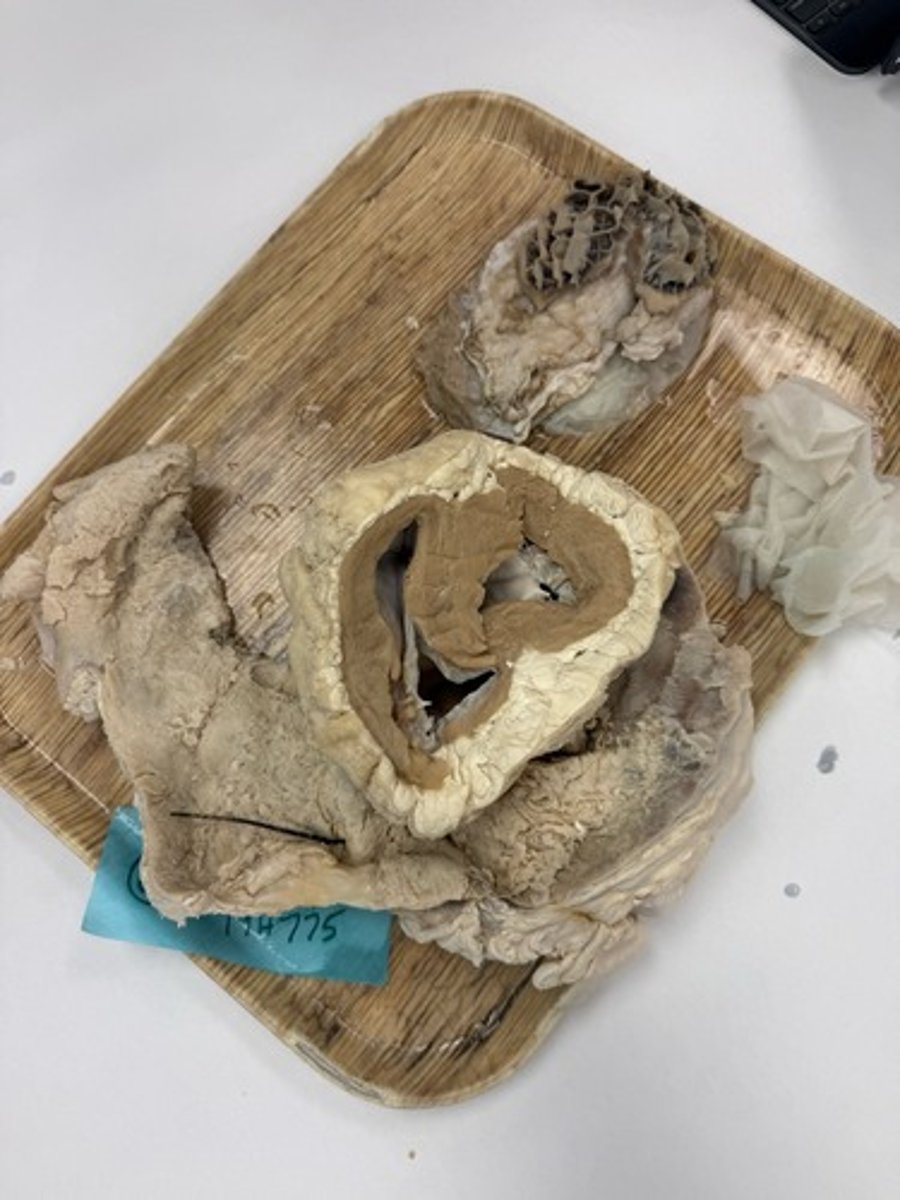
The presence of purulent fluid indicates that neutrophils are still being actively recruited to the site, which means the inciting cause is likely ongoing. This is common in the case of "hardware disease" or traumatic reticulopericarditis. Ventral pitting edema is likely due to progressive right heart failure. Because the right ventricular muscle mass is smaller, the pressure from the pericardial fluid affects the right side of the heart before the left. Decreased output causes expansion of the venous capacitance vessels-increased hydrostatic pressure.
At the time of necropsy, there was purulent fluid contained within the pericardial space. What is the significance of the clinical finding of purulent fluid in conjunction with the gross lesions you described?
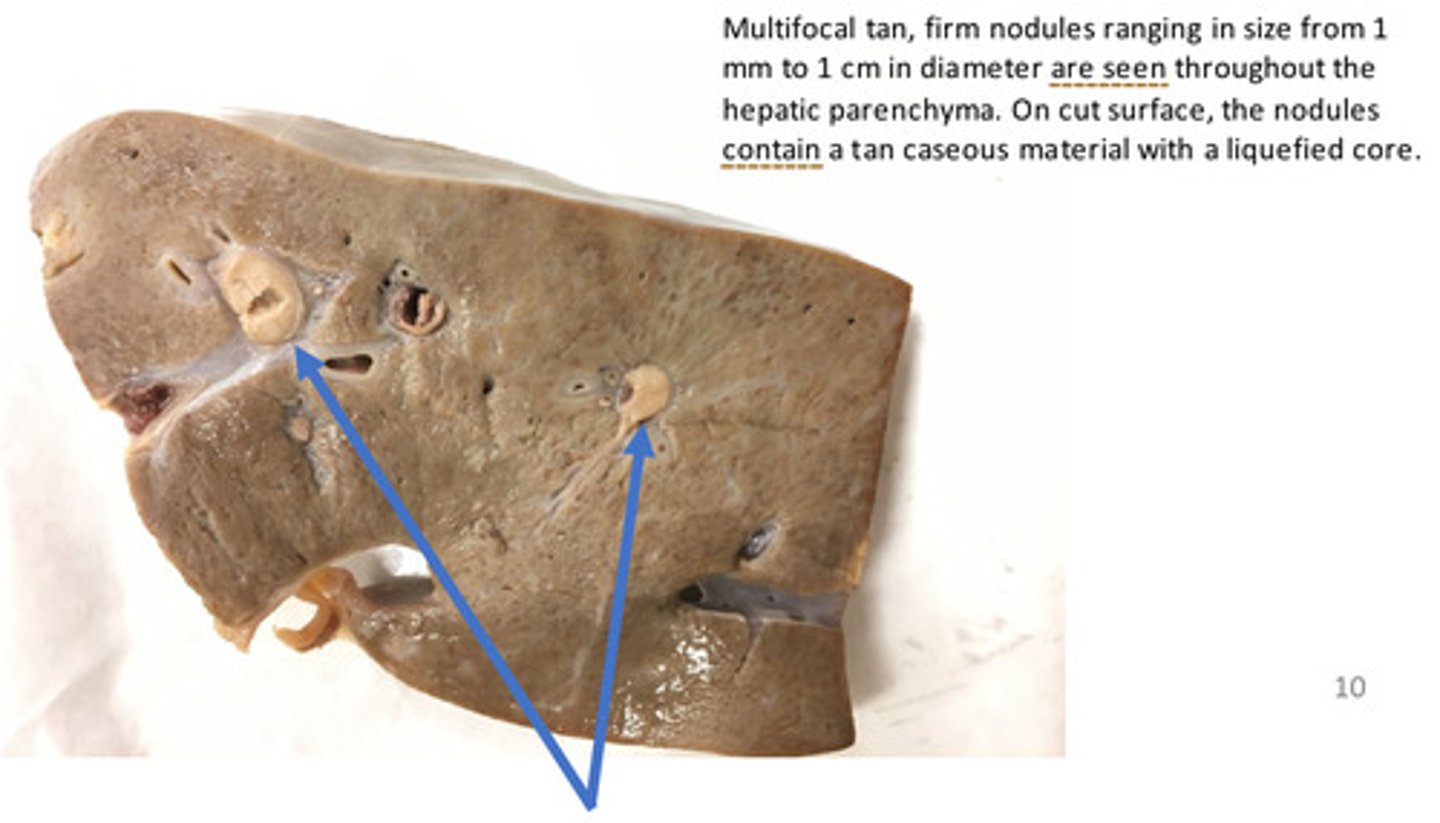
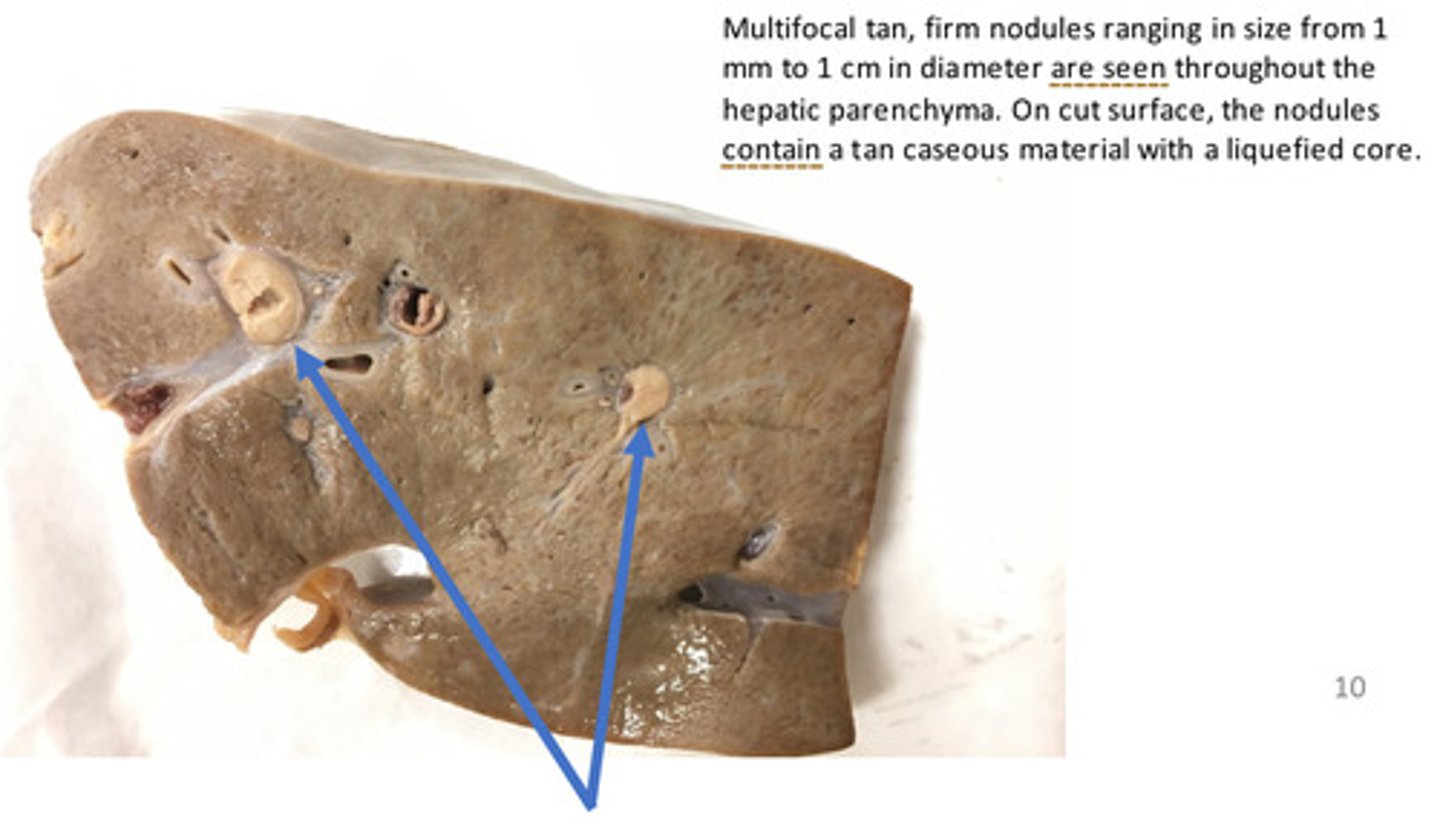
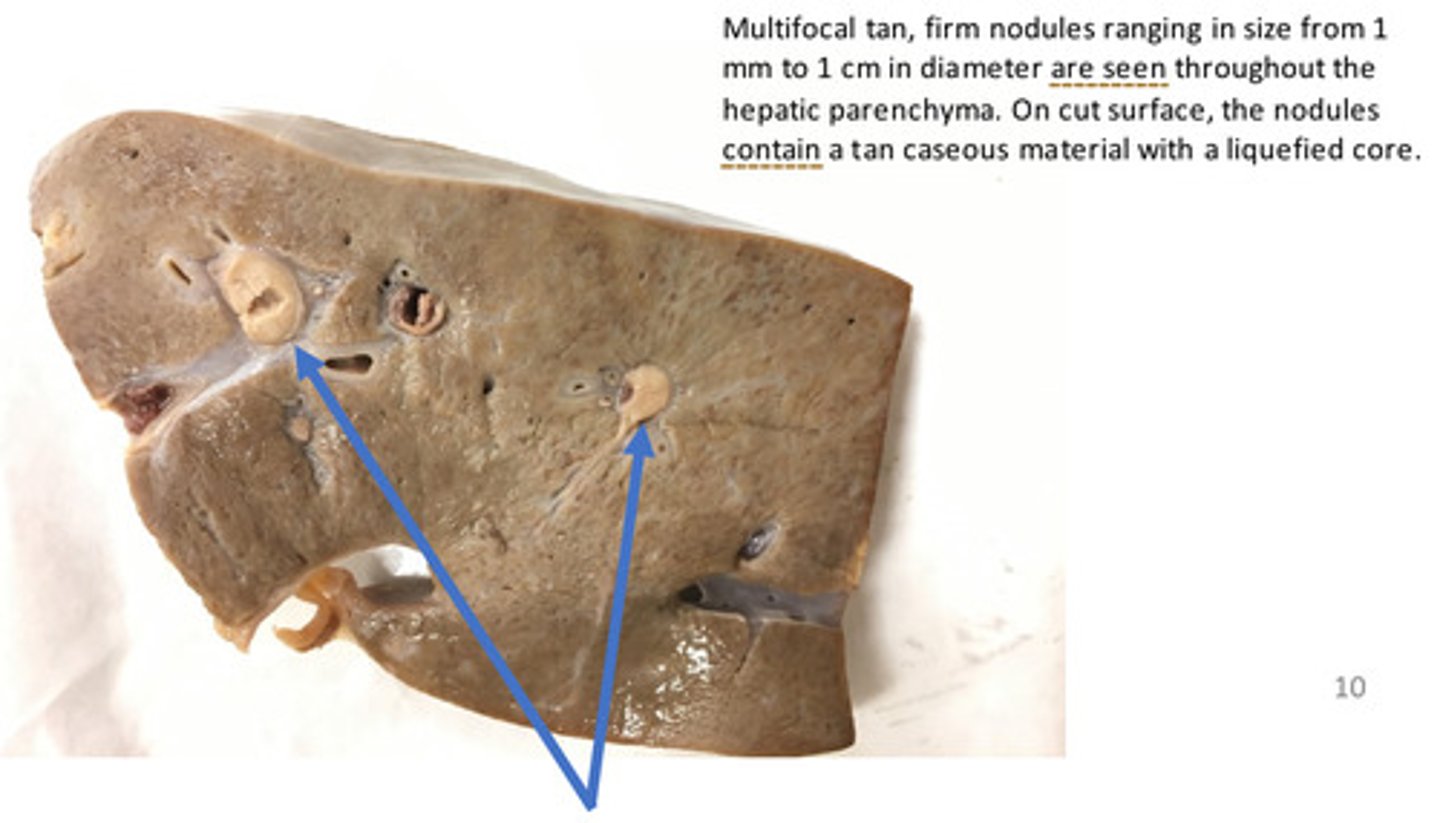
Liver: Severe, chronic, multifocal, hepatic abscesses
Provide morphological diagnosis
Liver: Severe, chronic, multifocal, hepatic abscesses
Provide morphological diagnosis
Liver: Severe, chronic, multifocal, hepatic abscesses
Provide morphological diagnosis
Cyst
Hematoma
Hyperplasia
Abscess
Neoplasia
Granuloma
Seroma
What are potential differentials for a nodule?
Rumenitis can be common occurrence in feedlot cattle. Rumenitis is usually the result of rapid intraruminal fermentation of dietary carbohydrates with subsequent production of lactic acid, which increases the acidity of the ruminal fluid. The acidic environment causes damage to the ruminal epithelium. Necrosis or ulceration of the ruminal epithelium allows bacteria such as Fusobacterium necrophorum to enter the portal blood stream and travel to the liver where they establish infectious foci or abscesses.
3. Provide a potential pathogenesis or cause for these hepatic abscesses in a feedlot steer.
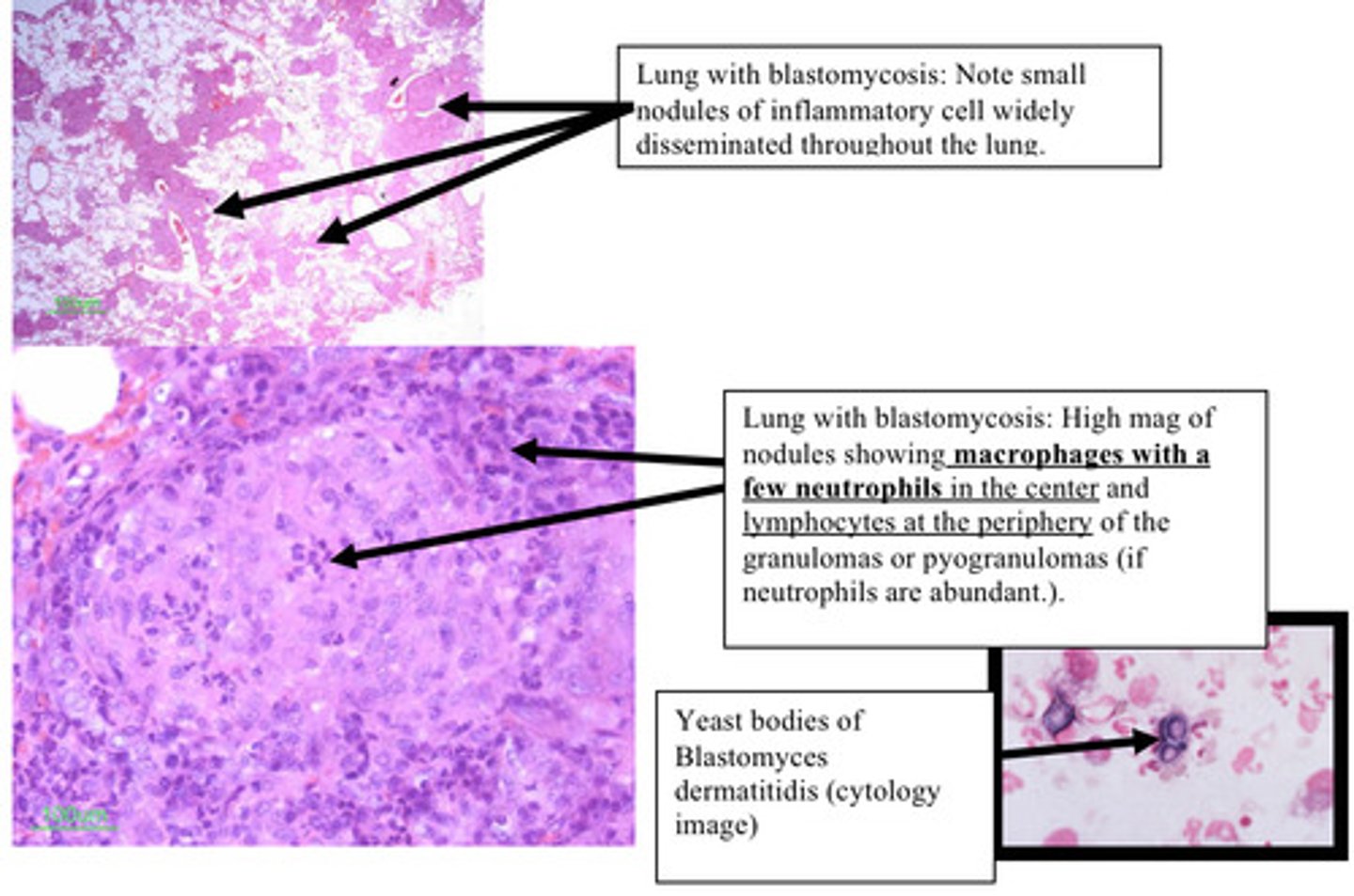
Lung: Chronic, multifocal, severe (pyo)granulomatous pneumonia (with fungal yeast bodies)
Provide morphological diagnosis - this is from a lung
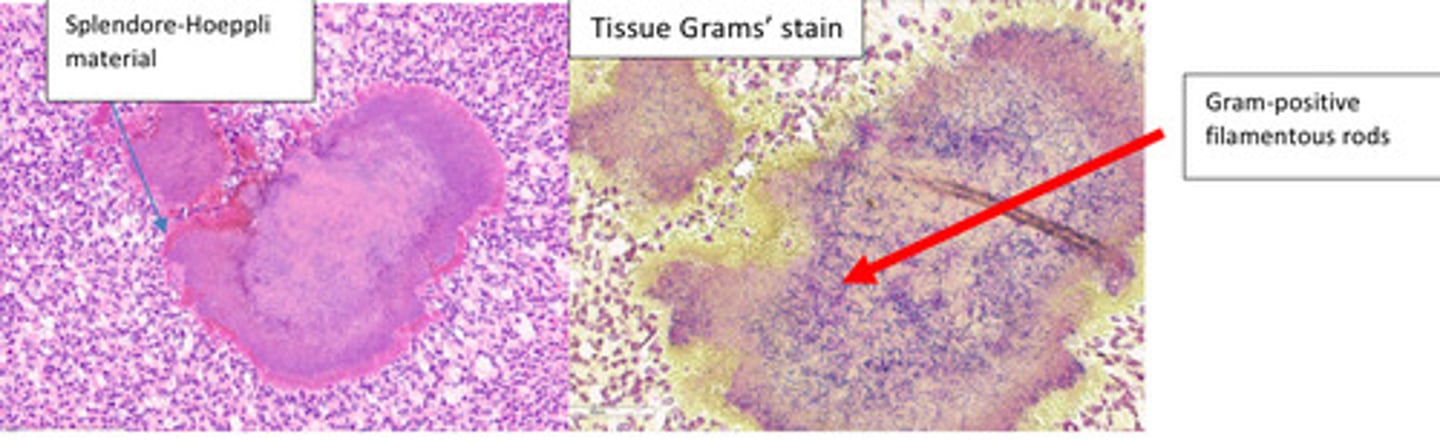
Subcutaneous mass: Severe, Chronic, focal, pyogranulomatous panniculitis and dermatitis with intralesional Gram-positive filamentous bacteria
Provide a morphological diagnosis