3336 Week 9: Elbow, Hand, and Finger
1/78
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
79 Terms
elbow joints
humeroulnar joint
humeroradial joint
radioulnar
elbow ROM
flexion 0-140 degs
extension 0-5 degs
pronation 0-90 degs
supination 0-90 degs
scenario: elbow
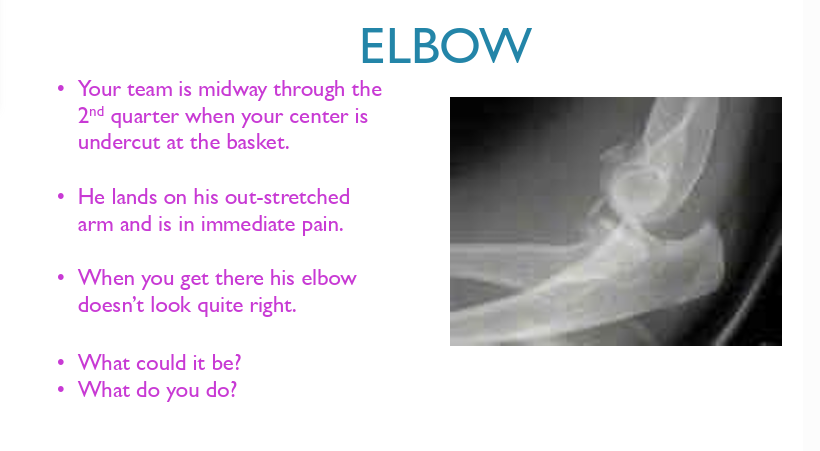
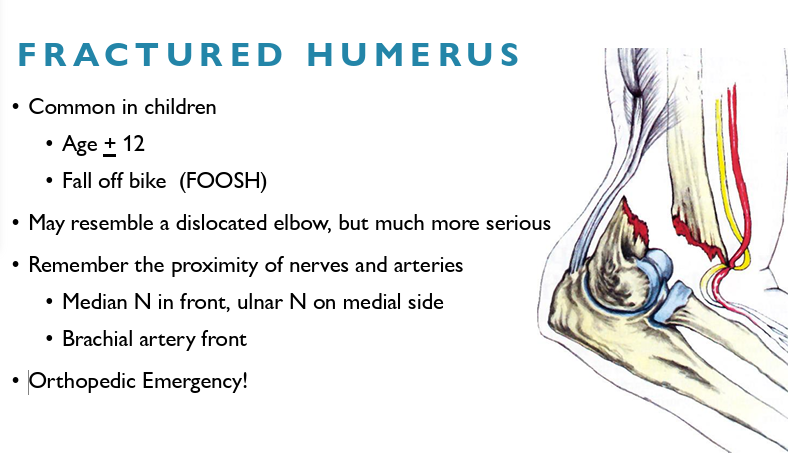
fractured humerus
Common in children age + 12
Fall off bike (FOOSH)
May resemble a dislocated elbow, but much more serious
Remember the proximity of nerves and arteries
Median N in front, ulnar N on medial side
Brachial artery front
Orthopedic Emergency!
supracondylar fracture symptoms
HX of MOI - bike, FOOSH
pain ++
light headed/dizzy
supracondylar fracture signs
may or may not have visible deformity
spasm
swelling
hemorrhage
± neurovascular signs
supracondylar assessment:
palpatiob - start at tip of olecranon and palpate supracondylar ridge of humerus
should be no pain or incontinuity on humerus - if so, could be fracture
if deformity apparent: check radial pulse, median and ulnar n function
beware of shock
in all patients with supracondylar fractures, the extremity should be assessed for:
pulse
skin colour
temperature
capillary refill
elbow dislocations
One of the most serious acute injuries to the elbow
Second most dislocated large joint, after the shoulder
Major complication is neurovascular compromise
Median/ulnar nerve and brachial artery
elbow dislocation MOI
Shoulder abducted with forearm in supination, then forced flexion from extended position, causing it to dislocate posterior laterally
dislocation elbow symptoms and signs
Report of extension to flexion + supination MOI
Severe pain and disability
Bulge behind elbow
May have neurovascular symptoms
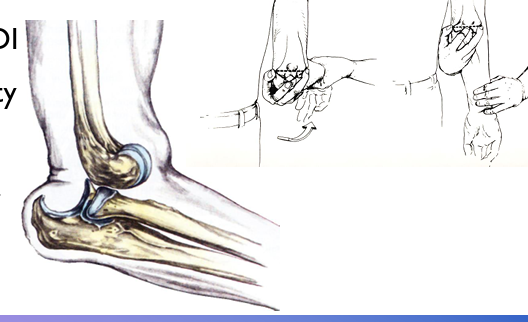
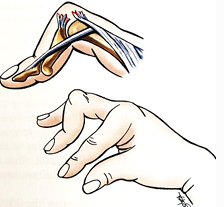
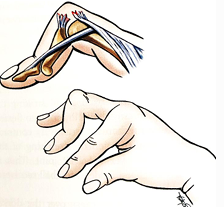
checking for median nerve
innervates gun fingers
if median n intact, the thumb can be rotated and flexed towards the pulp of the index finger (Opp. Pol. mm)

checking for ulnar nerve
innervates tea fingers
If ulnar N. intact it can activate Add. Pol. mm and hold paper between thumb and finger. If injured, thumb flexor mm do the work D.
Intact ulnar N. allows normal finger abd/adduction

management for dislocated elbow
rapid reduction is ecellent pain therapy, but first rule out fracture
if in doubt, LEAVE IT AND ACTIVATE EAP
to reduce: hold elbow at 45, apply gentle longitudinal traction to forearm - do not force!
evaluate pulses/cap refill, median and ulnar n, and strength after reduction
POLICE/PEACE and LOVE
refer to hospital, may need imaging, usually coronoid or radial head fracture with it
most elbow dislocations are stable once reduced and may be treated conservatively
olecranon bursitis
Bursae are closed fluid filled sacs with a synovial lining that facilitates gliding of musculoskeletal structures over one another during motion.
The floor of the olecranon bursa lies on the triceps tendon and olecranon, and the roof is loosely connected to the overlying skin of the elbow
MOI usually fall or repeated rub/blows to elbow
Single trauma
Repeated rub from boards
Student’s elbow

olecranon bursitis symptoms and signs
variable:
point tenderness
swelling
red
warm
fever
management for olecranon bursitis
POLICE/PEACE&LOVE
Use cold compress to decrease swelling
Monitor for infection
Minor trauma and sometimes repetitive microtrauma are enough to allow bacterial invasion of the bursa
Red, hot, increased temperature
Must pad prior to return to sport
elbow: lateral aspect responsible for
supination of forearm
strong wrist extension
mid elbow flexion
lateral elbow: static restraints
Stability in response to varus stress is provided by the lateral collateral ligament complex.
LCL complex runs from lateral epicondyle to annular ligament of the radius
primary static restraints against VARUS loading:
Annular
Radial collateral
Lateral ulnohumeral/ulnar collateral
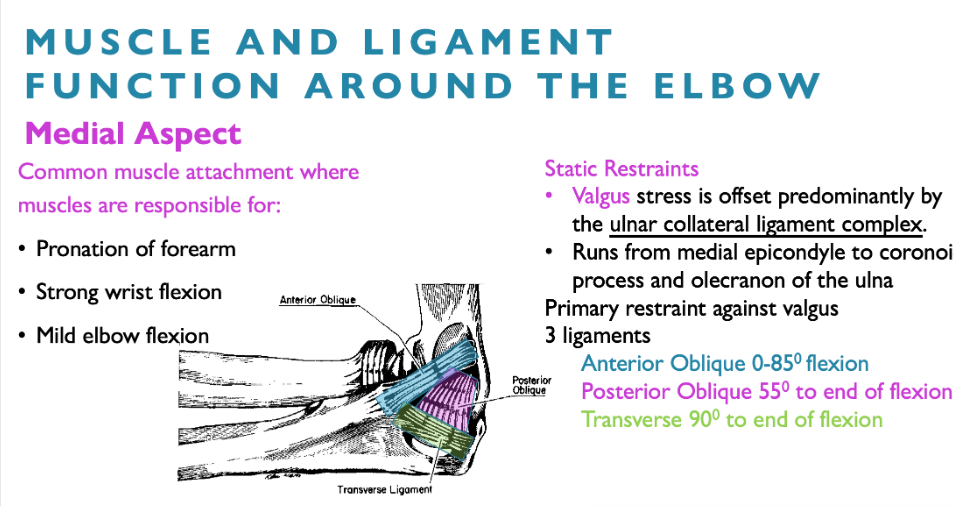
medial aspect of elbow responsible for
pronation of forearm
strong wrist flexion
mild elbow flexion
medial elbow static restraints
valgus stress is offset by ulnar collateral ligament complex
runs from medial epicondyle to coronoid process and olecranon of the ulna
primary restraint against VALGUS loading
anterior oblique 0-85 flexion
posterior oblique 55 to end of flexion
transverse 90 to end of flexion
MCL sprain
Medial (ulnar) collateral ligaments are primary STATIC restraints to valgus stress • The failure capacity of the UCL is approached with pitching.
Typical valgus torque of 64 N · m and a tensile force of 290 N
On average the UCL withstands a valgus torque of 34 N
m and a tensile force of 261 N
Similar to the lateral knee, the muscles provide a large part of support.
MCL MOI
Valgus stress from throwing or falls
Can be result of acute or chronic injury
MCL sprain: acute and chronic
Acute- Hx of fall or hyperextension with valgus Chronic- overload
Throwers with poor mechanics - open up too soon
MCL sprain, signs/symptoms
Pain localized to medial elbow
Chronic: During the late cocking and early acceleration phases of pitching, decreased velocity accuracy or endurance, may not have inflammatory signs
Acute: The player typically recalls a popping sensation along with a specific throw that prompted the on-set of symptoms, early inflammatory signs
Varying instability/laxity on valgus stress at 20-30
Ulnar nerve may be involved- +ve Tinel’s test
management for ACUTE MCL sprain
POLICE and refer to physician
Partial tears- brace and rehab
Gain ROM
Nonoperative management focuses on flexibility and strengthening of the forearm musculature, rotator cuff, and scapular stabilizers
Medial muscle bulk strengthening to aid in support
management for CHRONIC MCL sprain
Rest
Decrease pain and increase ROM (address inflammation if present)
Strengthen medial muscle bulk
Correct throwing errors
Address upper and lower chain issues
lateral epicondylosis: tennis elbow
Associated with activities involving wrist extension against resistance
Racquet sports, carpentry, bricklaying, sewing, knitting, computer work
Usually slow but can be fast onset (itis)
Micro vs. macroscopic injury
medial epicondylosis: golfers elbow
Not as common
(7-10x less)
Seen in golfers (chunk) and tennis players who use top spin on forehand shot
Occurs in medial flexor group
Primarily pronator teres
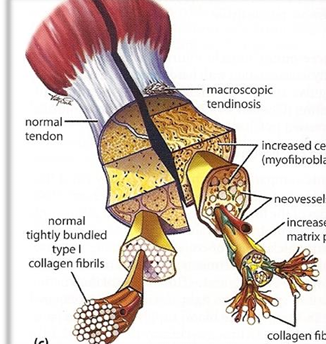
tendinosis review
Stage 1 : NO inflammation associated with pathologic tissue alterations
Stage 2: Alterations characterized by disrupted collagen architecture Fibroblastic and hypervascular response, No inflammatory cells
Stage 3: Tendinosis with tissue structural failure (e.g., microtearing)
Stage 4: Continued failure with fibrosis/calcification
lateral epicondylosis signs and symptoms
pain lateral aspects of elbow, usually ECRB m
Maximal area of tenderness is within 1-2 cm of the epicondyle
Pain before, during and after activity
Pain with squeeze and grasp
Pain reproduced with resisted wrist extension in a pronated and radially deviated wrist (Cozen’s test)
Resisted extension of the middle finger - Ext digitorum or Extensor Carpi ulnaris
medial epicondylosis signs and symptoms
Localized tenderness just below medial epicondyle
Activity makes it worse
Pain with resisted wrist flexion and/or pronation
Pain with passive stretch into wrist extension
Test ulnar nerve as it may become trapped in scar tissue
epicondylosis management
POLICE/PEACE&LOVE if acute
Modification of activity
Limit FITT
Correct technique/ergonomics
Repair Stage
Cryogenics vs. heat
Ice (pain) and cross friction- breaks down disrupted collagen and aligns
Heat will increase blood flow to region
Stretching • Strengthening • Bracing/equipment modification
stretching lateral epicondylosis
Pronate forearm, extend the elbow and flex the wrist (flex the fingers)
stretching medial epicondylosis
Extend the fingers, extend the wrist and extend the elbow
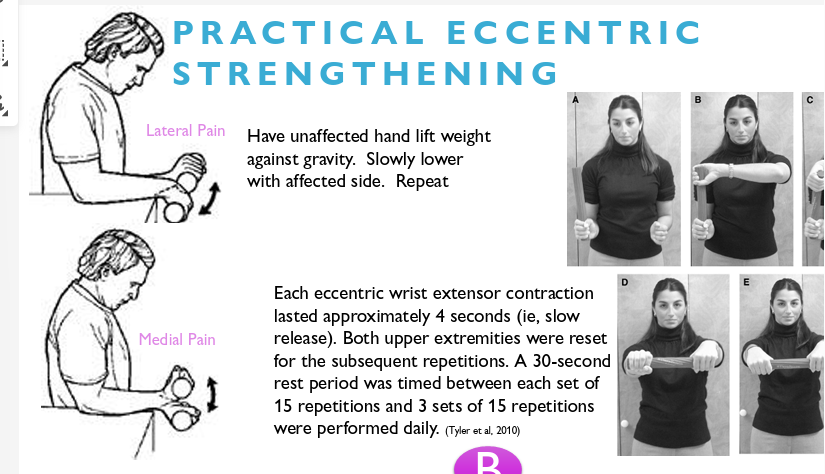
strengthening for tendinosis/epicondylosis
Eccentric training has demonstrated promising results in the management of elbow tendinopathy when added to standard physical therapy treatment
Improvements were greater for the Eccentric Group versus the Standard Treatment Group (percent improvement reported):
Little consensus regarding parameters including: •Painful vs. non-painful • Sets/reps
practical eccentric strengthening for epicondylosis
bracing for lateral epicondylosis
Brace treatment might be useful as initial therapy. Combination therapy has no additional advantage compared to physical therapy, but is superior to brace only for the short term
A counterforce brace provided significant relief (frequency and level of pain) at 2-12 weeks, as well as a significant improvement in overall elbow function at 26 weeks, compared with the placebo brace
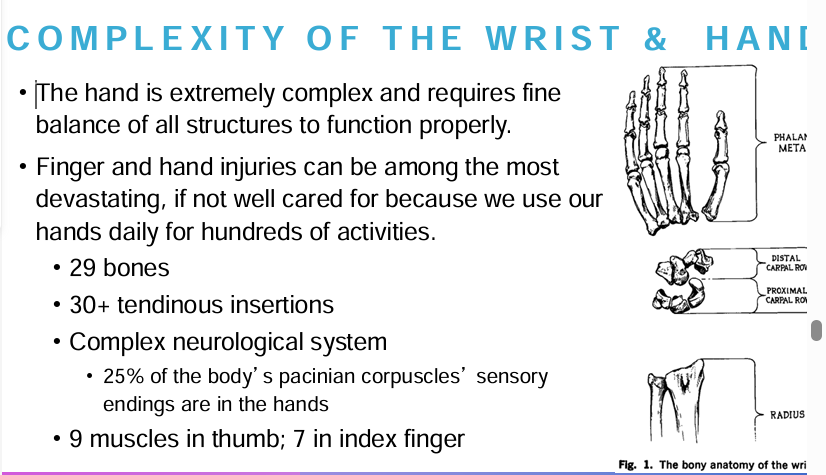
complexity of the wrist and hand
skin of hand: volar surface
Thick
Underlying fascial attachments
Inelastic
Hairless
Ridges for grasping
skin of hand: dorsal surface
Elastic
Mobile
Thinner
Loose
Pliable
Must stretch 1 in. for fingers to close
edema in hand
Frequently accumulates in dorsum.
Can lead to contractures.
Excessive swelling on dorsum can cause hand arches to collapse anteriorly and adduct the thumb.
Finger ROM can be impaired.
Edema causes reduced mobility and function of the hand in short term and in long term if fibrous formations occur
treatment for hand edema
Must reduce early edema, or risk loss of function
Measured by circumferential gauge or string wrapped around finger and track progress
Use of POLICE, compression dressings and other modalities
wrist ROM
Flexion 80
Extension- 70
Ulnar deviation 30
Radial deviation 20
fractured radius: MOI
Most common is the Colles Fracture, which runs through the distal metaphysis of the radius
May fracture the ulna (styloid) MOI- Usually FOOSH, with distal fragment displacing dorsally
Fall on flexed wrist is termed a Smith Fracture (distal fragment displaced palmarly)
fractured radius: signs and symptoms
Pain on radial (thumb) side of forearm
Local tenderness
Dinner fork deformity (reverse in Smiths)
If non-displaced
Pain on percussion
+ swelling
Passive pronation - Bends radius around ulna - If pain- send for imaging
Stabilize with splint and sling transport
fractured scaphoid: MOI and symptoms
Most common carpal fracture
MOI is a fall on an extended wrist
Symptoms- Post traumatic pain on the radial side of the wrist in anatomical snuffbox
signs of fractured scaphoid
Sensitive examination findings include tenderness to palpation in the anatomical snuffbox (direct test), and pain on longitudinal compression of the thumb (indirect test)
Wrist extension with radial deviation is reduced and painful (indirect test)
Confused with wrist sprain/lunate subluxation as often does not show on initial X ray.
fractured scaphoid: management
Surgical management of scaphoid fractures can provide significantly improved return to sport compared to conservative management • (mean 7.9 vs 13.9wks)
Immediate return to sport in a cast should be avoided due to the significant risk of non-union.
scenario

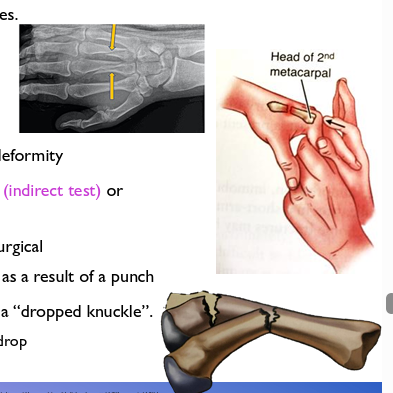
fractured metacarpals: MOI
Hand fractures comprise one-third of all fractures during athletic competition, with metacarpal fractures comprising two-thirds of hand-related injuries.
MOI: Direct blow to the hand or as a result of punching something
metacarpal fractures: symptoms and signs (boxers and bennets fracture)
The athlete generally presents with dorsal hand pain, swelling and deformity
Pain on direct palpation and axial load through fingers/MCP joint (indirect test) or squeeze from side for 2nd and 3rd metacarpals
Bennet’s fracture is an injury to the 1st metacarpal- usually surgical
Boxer’s fracture is most common in 5th, then 4th metacarpal as a result of a punch
Often see flexion deformity of the distal fragment that results in a “dropped knuckle”.
The more proximal the fracture, the greater the knuckle will drop
fractured phalanges MOI
MOI- Shaft fractures of the proximal and middle phalanges can occur in a variety of patterns
Most mid-phalangeal fractures are transverse fractures related to direct blows
Distal phalangeal fractures usually result from crushing injuries
fractured phalanges: symptoms and signs
Pain on axial compression and or circulative compression around the phalanx
4 fingers tend to move as a unit and should maintain longitudinal and rotational alignment
Fractures to middle or proximal phalanx may have deformation due to pull of tendons
Look for overlapping fingers
1st aid for fractured phalanges
Immobilize in wrist splint with gauze pad or roll to produce approximately 30 of flexion and refer for X rays
Buddy taping and/ or protective splint wear in acceptable alignment can allow fast return to play of nondisplaced, non-articular fractures
finger dislocations MOI
May occur at the DIP, PIP or MCP joints
MCP joint dislocations are rare
PIP joint is most common dislocation in the body
MOI: Hyperextension and axial compression
ball hits the end of a finger
finger dislocations: signs and symptoms
DIP and PIP - swollen and painful finger.
DIP dislocations usually occur dorsally and may have an open wound- These individuals often reduce the injury on their own
PIP usually dislocates dorsally with visual deformity
MP joint dislocations often present with the proximal phalanx at 90 to the metacarpal
finger dislocation first aid
Due to probability of entrapping the volar plate, an untrained individual should not attempt reduction
Immobilize in a wrist or finger splint and refer to physician
wrist sprains/instability
Because of the proximity of structures in the wrist, diagnosis of these injuries can be challenging and is often a diagnosis of exclusion
X-rays negative for fracture or dislocation
Pain caused by capsular injury is subjective and varies from patient to patient
Most commonly between the scaphoid and the lunate (Scapholunate ligament- SLL) but may be a number of structures
wrist sprain/instability MOI
FOOSH or direct blow to or twisting of the wrist in combination with an extension moment
Athletes of almost any sport involving violent contact with other players or the ground are prone to this injury on a hyperextended wrist. Cumulative microtraumatic injuries may also result in SLL damage.
wrist sprains/instability symptoms
Pain, tenderness, on dorsum of joint
Increase pain between scaphoid and lunate increases with active or passive extension.
Remember that scaphoid fractures may not show immediately on X-ray

lunate subluxation/dislocations
Lunate Subluxation (wrist sprain)
Axial load with radius compressing lunate in a volar direction
Equally limited flexion and extension
Loss of articulation between radius and lunate is a dislocation
Lunate may move into the carpal tunnel
Tinel’s test over carpal tunnel may be positive
Dorsum of hand is point tender
X ray shows “spilled teacup” sign with dislocation
wrist sprain/instability treatment
ulnar collateral ligament sprain of the first MCP joint
skiers or game keepers thumb (common in skiing, basketball, and football)
MOI: Forced valgus of proximal phalanx of thumb
Symptoms and signs:
Tender and swollen over medial MCP joint
Pain, ecchymosis, and swelling on the ulnar aspect of the thumb MCPJ.
Pain with Valgus stress test and laxity greater than the contralateral side or 20-30 is considered positive.
treatment for game keepers thumb
POLICE/PEACE&LOVE
Tape/brace injuries with firm endpoints.
Those with no endpoint refer to surgeon
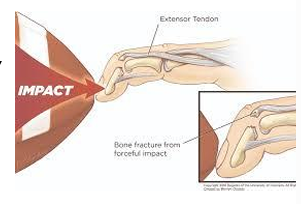
mallet finger
Mallet Finger - AKA Extensor Tendon Avulsion MOI is a blow from an object that hits the tip of the finger and is is commonly seen in softball, basketball, baseball, volleyball, or in receivers in football
Causes an avulsion of the distal extensor tendon
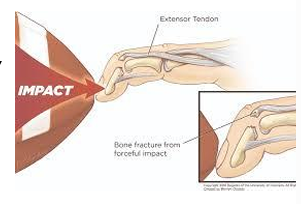
signs and symptoms of mallet finger
+/- Pain at dorsal DIP joint - When the bone is not involved, this lesion can be remarkably painless.
Inability to actively extend DIP with PIP stabilized in full extension
mallet finger treatment
POLICE
Extension splinting of the DIP joint is appropriate for almost all mallet fingers, including those with bony fragments if there is no significant joint subluxation. Must be very diligent with splint wearing
Boutonniere deformity
Boutonniere Deformity- AKA Extensor Digitorum Cummunis Tendon
Result from a disruption of the central slip of the extensor digitorum at its insertion on the base of the middle phalanx
Similar MOI as mallet finger, but at the PIP joint
Blunt trauma over dorsal aspect of PIP or PIP forced into flexion against residence
boutonniere finger symptoms/signs
Patients present with pain on dorsal side of PIP and the inability to extend at joint
The deformity is often absent at initial presentation as the band slowly migrate volarly
This results in PIP joint flexion and hyperextension at the distal interphalangeal (DIP) joint
boutonniere finger treatment
Splint in full extension 6-8 weeks
Rehabilitation goals are to regain full strength and range of motion and avoid a deformity.
jersey finger
Jersey Finger - Flexor Digitorum Profundus (FDP) Rupture
MOI- usually occurs on the ring finger when an athlete grabs an opponent’s jersey
A disruption of the FDP tendon occurs because the DIP joint is actively flexed and then forced into extension.
Either ruptures or avulses tendon
The ring finger is involved in up to 75% of reported cases, but any digit may be injured.

jersey finger signs and symptoms
Pain and point tenderness volar DIP
Can’t flex DIP with MCP and PIP joints stabilized

jersey finger treatment
POLICE- Splint in 30 flexion at PIP and DIP
Significant grip and strength repercussions
Requires surgery within 7-10 days
collateral ligament sprain PIP/DIP
Partial or complete collateral ligament tears are often referred to as "jammed fingers,” MOI
may occur at any interphalangeal joint with an ulnar or radial-directed force.
They occur more often at the PIP joints than at the DIP joints
symptoms and signs for collateral ligament sprain DIP/PIP
Pain at joint, tenderness and swelling.
Rule out fracture via direct (palpation) and indirect (axial load) testing
Test structure by flexing involved joint to 20-30 and apply valgus and/or varus stress.
Compare to finger on contralateral hand

treatment for collateral ligament sprain DIP/PIP
Nonsurgical management of collateral ligament injuries is almost always successful.
Apply a splint or use buddy taping
Athletes may continue to participate in their sport as pain and function allow.