hollistic health info before finals
1/113
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
114 Terms
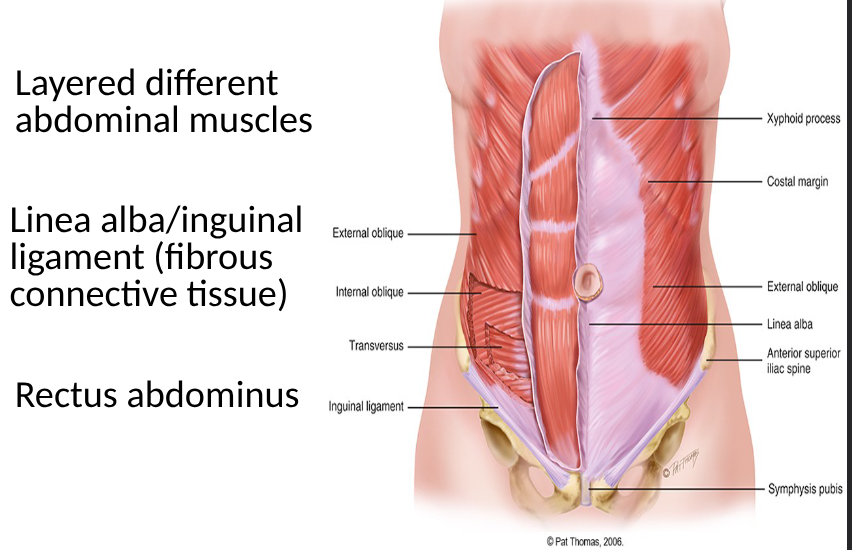
anatomy of muscles in abdomen
internal anatomy of abdomen
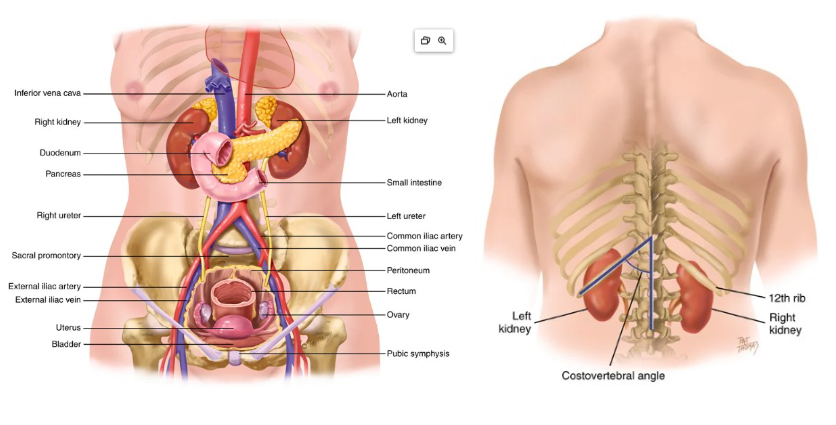
peritoneal organs
abdomen lined with peritoneum (2 layers)
peritoneal cavity contains intraperitoneal organs: stomach, liver, parts of colon
retroperitoneal contains organs outside of peritoneal cavity: kidney, ureters, adrenals, part of colon and pancreas
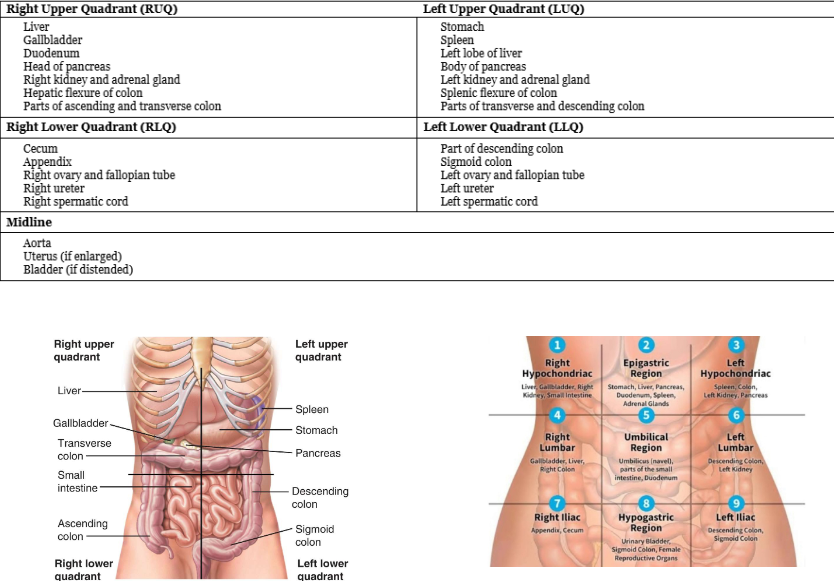
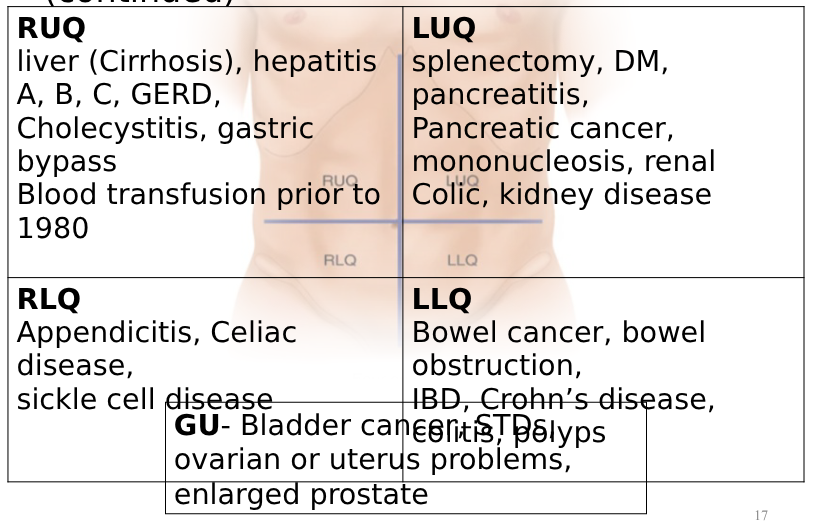
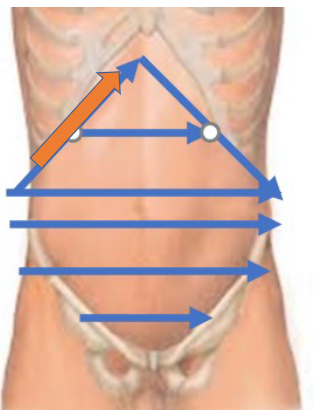
abdominal quadrants and regions
specific questions for abdominal assessment
changes in weight (eating disorder, cancer), bowel movement colour and frequency, vomiting color and frequency, problems with chewing/swallowing (dysphagia), ADLs, Lifestyle
subjective assessment for abdominal assessment
demographic or identifying data, hobbies, work (PPE) - hepatitis, travel hepatitis- hep A
past history in abdominal exam
past surgeries: appendicitis, bowel resection, cholecystectomy, hysterectomy
injuries: trauma, work injury
degrees of family
first degree- individual’s parents, full siblings or children
second degree- grandparents, grandchildren, aunts and uncles, nieces or nephews or half sibilings
third degree- great grandparents, great grandchildren, first cousins
***must be related by blood
relevant family history for abdominal exam
ex- colorectal cancer, GERD, peptic ulcer disease, inflammatory bowel disease- ulcerative colitis, crohn’s disease; anemia/thalassemia, splenomegaly, celiac disease, DM, pancreatic cancer, sickle cell anemia, thyroid disease
medications in abdominal assessment
meds specific to GI or GU, prescription + OTC + vitamins and herbals, narcotics lead to constipation, antacids interact with other meds
malabsorbtion in abdominal assessment
lactose intolerance, food allergies, celiac
DADSPIES for abdomen
diet- water, fibre (bowels), fat (gall bladder), spices (gastro), 24 hr diet recall, special diets like vegetarian, appetite and food intolerances
alcohol- cirrhosis
drugs- hepatitis (sharing needles)
smoking- bladder cancer
physical exam- FIT at 50, last pap test/prostate exam
immunisations- hepatitis and shingles vaccine
excersize
stress
OPQRSTUA for abdominal pain
o- when did it start, gradual or sudden
p- anything make it better or worse? positioning, medications, food?
q- sharp, burning, stabbing, dull
r- located? referred pain?
s- 0-10, ADLs,
t- better or worse at times of day
u- what do u thing is wrong
a- other symptoms
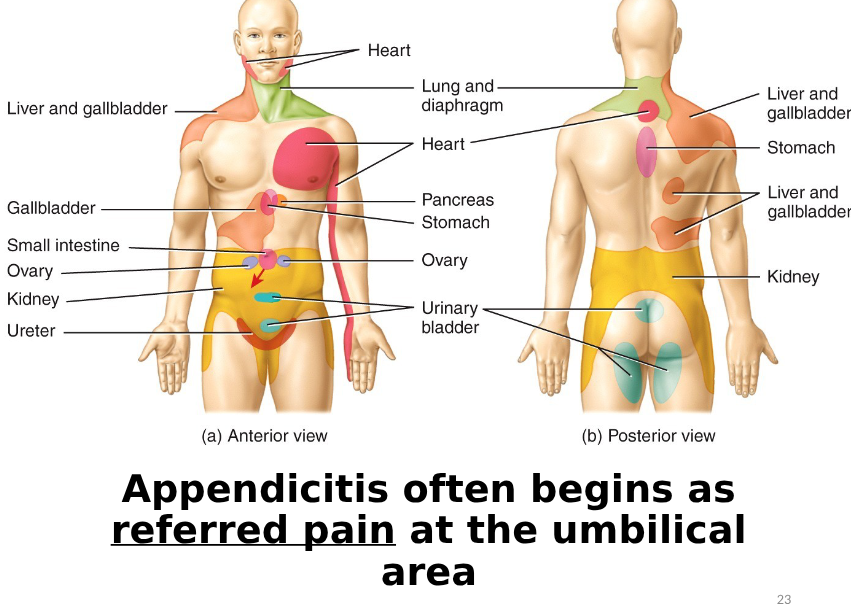
referred pain for abdomen
visceral pain (abdomen)
hollow organs are distended, stretched or contracted forcefully, may be difficult to localise, described as gnawing, burning, cramping or aching, may be associated with sweating, pallor, nausea, vomiting or restlessness
parietal pain (abdomen)
inflammation of the peritoneum, severe and localised over the involved structure, described as steady, aching, sharp esp with movement
referred pain (abdomen)
occurs in more distant sites innervated at approximately the same spinal level as the disordered structure
associated symptoms for GI
nausea, vomiting, indigestion, anorexia, diarrhea, fever, changes to skin colour, changes in weight, dysphagia, painful swallowing (odynophagia), constipation or changes to normal bowel pattern
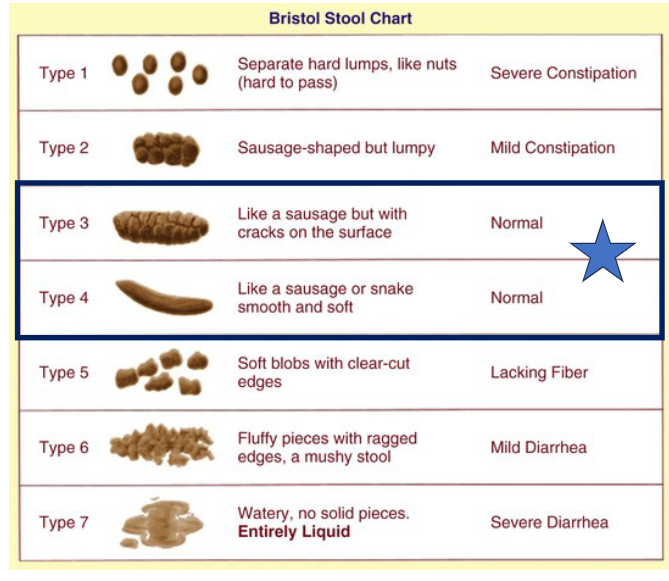
find out what is normal for pt, normal frequency for bowel movements is from 3 times a day to 1 time a week
associated symptoms for GU
hematuria (colour), dysuria, frequency, urgency, change in stream (males- prostate), increased amount of urine with voiding (polyuria), nocturia, urinary incontinence, flank or back pain
urinary incontinence- stress
coughing, sneezing, increased intra abdominal pressure
urinary incontinence- urge
sudden urge and loss of continence with little warning
urinary incontinence- over fliow
continous dribbling or dripping and weaker urinary stream
urinary incontinence- functional
cannot get to the toilet in time due to environmental factors or impaired health
urinary incontinence- total
inability to retain urine, ask also about bowel incontinence
bristol stool chart
ask everyone bowel pattern describe
developmental considerations: pregnancy (abdomen)
morning sickness, heartburn (esophageal reflux), constipation and decreased bowel sounds, smooth muscles relax which results in decreased motility leading to constipation
developmental considerations: older persons (abdomen)
suprapubic fat accumulation in women and abdomnial accumiulation in men, decreased salivation, gastric acid secretion, delayed esophageal emptying (risk of aspiration), more suceptible to dehydration (thirst drive decreased), decreased liver size and increased gallstones, decreased renal function (adverse or toxic drug effects), constipation is a big concern,
developmental considerations: questions to ask older people (abdomen)
help with groceries and meals? lower income and costs for food, constipation concern: gibre, fluids, caffeine intake in previous 24 hrs, bowel patterns, eating difficulties (swallowing and chewing), any meds that affect BMs- laxatives and diuretics
cultural/social considerations (abdomen)
high rates of obesity in women, high prevalence of lactose intolerance, many canadiants have a diagnosis of celiac disease, peptic ulcer disease, IBD, GERD and modifiable risk factors, relationship of hep A and GI illness to socioeconomic factors
preparation for abdominal exam
warm and private, adequate lighting, have pt empty bladder prior, pt lies supine with arms at side and knees bent (to help abdomen relax), drape pt appropriately, gather equipment
specificities to abdominal assessment
painful areas examined last, observe for signs of discomfort, distract patient to avoid tensing, make sure hands are warm
abdominal general survey
distress, upright posture, walking (clutching abdomen), pacing room, eating, crying, grimacing, guarding when you come near, lying flat with knees bent, pale colour
vital signs for abdominal
pain- tachycardia, hypertensive, afebrile, tachypnea
fever- febrile, tachycardia, normotensive, tachypnea
blood loss/shock- tachycardia, hypotensive, afebrile, tachypnea
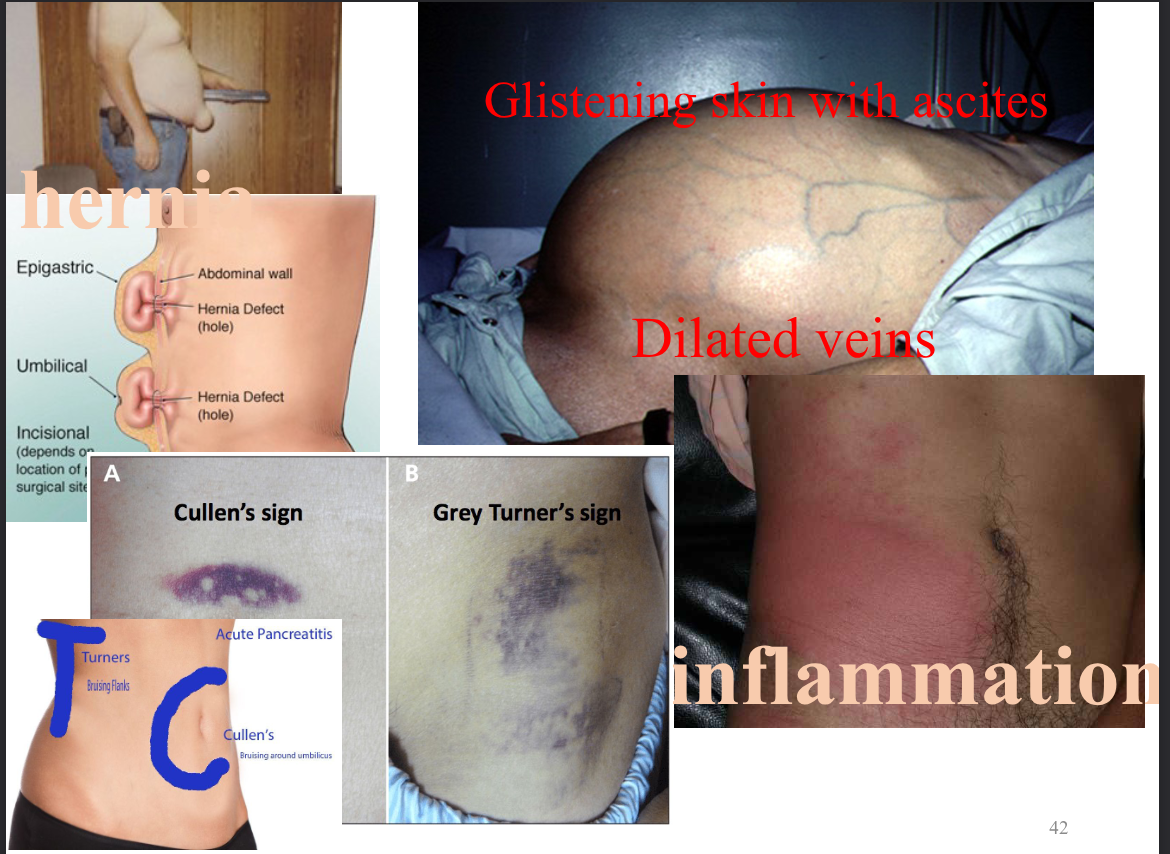
inspection of abdomen
skin: colour and condition, contour and symmetry, umbilicus: inverted or everted, peristaltic waves, pulsation, any visible organs or masses, unexpected findings: scars, striae, veins, umbilical hernia rashes and lesions, deep breath and bear down: hernia or organomegaly, hair distribution
***inspect tangentially with light
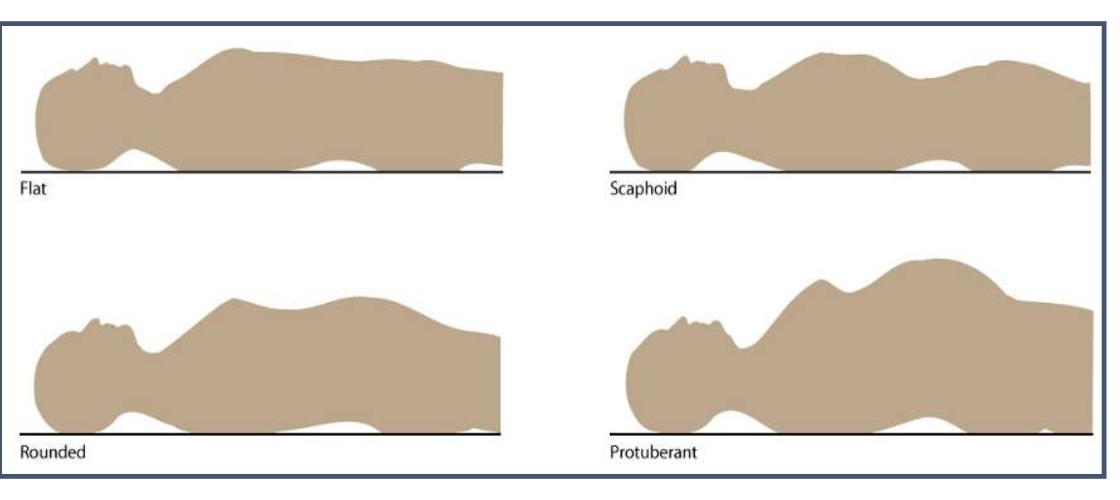
contour of the abdomen
look from above, then stoop lower
abnormalities in abdomen
lipohypertrophy
lump under skin, accumulation of fat, result of many subcutanous inections of insulin- can affect absorbtion and onset, unsightly and mildly painful
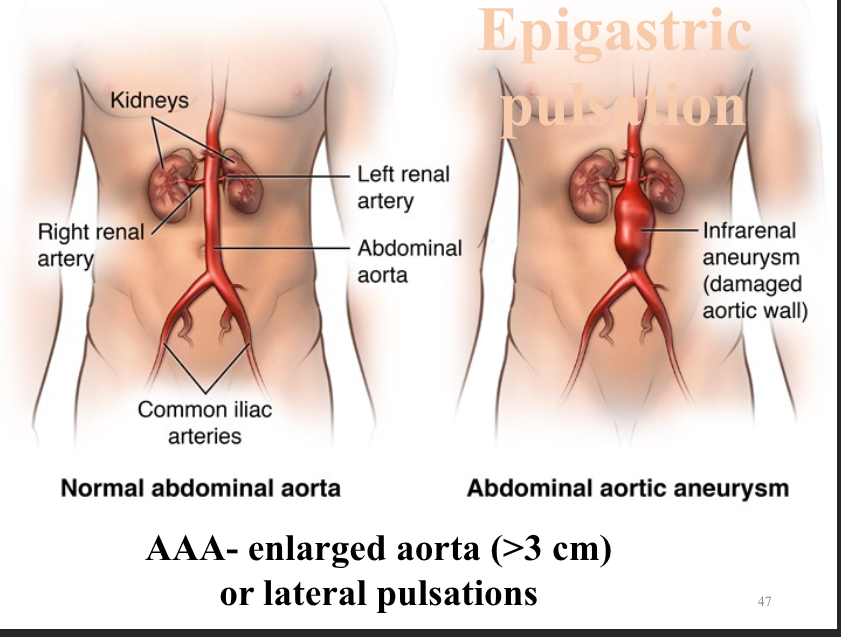
normal abdominal aorta vs abdominal aortic aneurysm
abdominal assessment
inspection, auscultation, percussion, palpation
auscultating abdomen
2 spots per quadrant, start at iliocecal valve (RLQ), bowel sounds: high pitched gurgles or clicks,
borborygmi- air through intestines- stomach growling , 5-30/35 sounds, check for up to 5 minutes to detemine if sounds are absent
hyper active bowel sounds
above partial bowel obstruction, diarrhea, gastroenteritis, early intestinal obstruction
hypoactive bowel sounds
constipation, ileus and peritonitis, decreased or nonexistent below point of obstruction
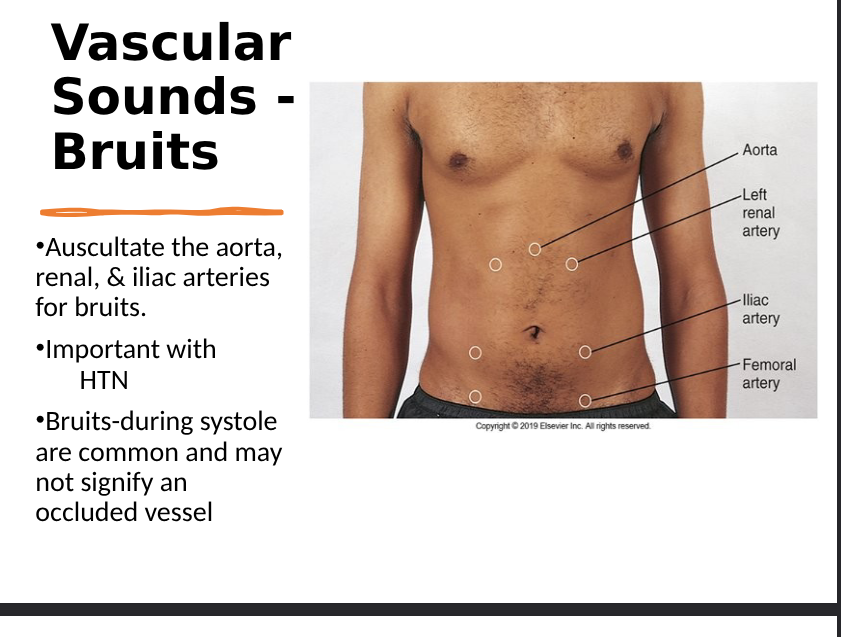
vascular abdominal sounds
use firmer pressure and use bell,
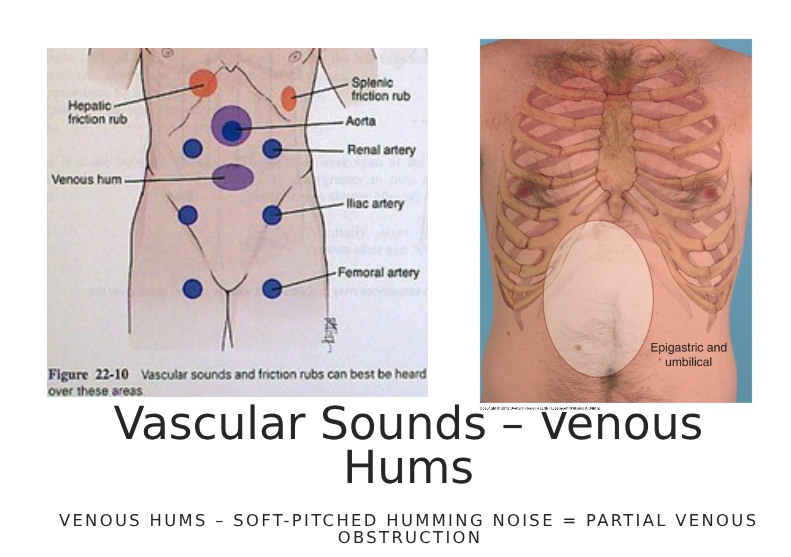
bruit, venous hums,
friction rub- grating sounds that increase with inspiration, liver tumor, spleen infarction, peritoneal inflammation
vascular sounds- bruits
bruit- swishing sounds (turbulent blood flow), constriction of vessel, in hepatic area can indicate liver cancer or hepatitis, during systole are common and may not signify an occluded vessel
vascular sounds- venous hums
venous hums- soft pitched hum, partial obstruction vessel- reduced flow to organ
percussion of abdomen
determines organ size and tenderness, detects fluid, air and masses, percuss mid axilla to mid axilla along costal margins down to supra pubic, normally most of the abdomen is tympanic
tympanic sounds
LUQ (gastric bubble), most of abdomen, gas dullness can be due to feces (stool)
dullness sounds
over organs, masses, or fluid (ascites, GI obstruction, pregnant uterus, ovarian tumor)
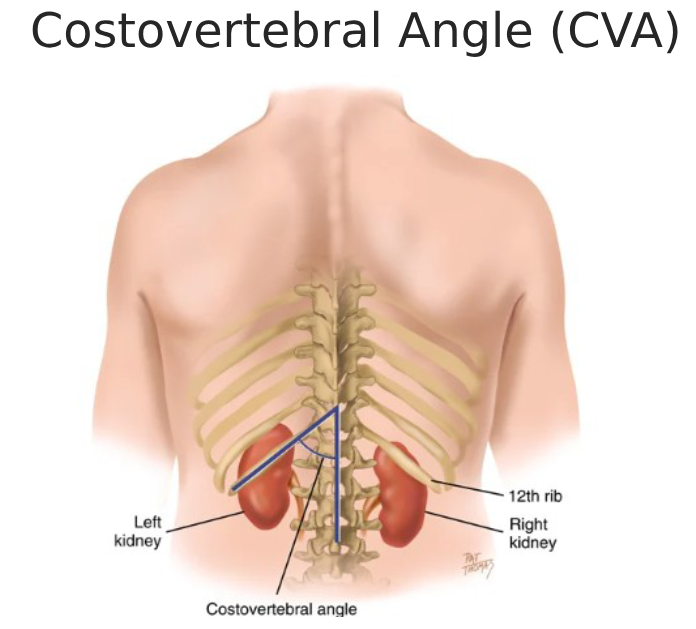
percuss Kidney at costovertebral angle (CVA)
blunt percussion: costovertebral anlge, fingertip pressure is enough, pt will feel a perceptable but PAINLESS thud
percuss liver (enlargement)
percuss along costal margin, should go beyond costal margin, enlarged liver will be dull, liver normally found at 5-7 intercostal space, start RMCL at 3rd ics over lung tissue, then percuss downward towards liver to check for resonance to dullness, then start at rt MCL and umbilical area and percuss upward for tympany tp dullness, should be 6-12 cm
percuss spleen (enlargement)
costal margin- percuss LMCL along costal margin left mid axilla line, should remain tympanic
truabe’s space- triangle shaped area at 6th rib-costal margin and mid axillary line, normally tympanic but dull with splenomegaly
castell sign- percuss lowest ics on left anterior axillary line-tympanic, pt takes deep breath and holds (should be tympanic), dull if enlarged
percuss bladder at distension (full)
percuss from umbilicus to symphisis pubis, full bladder will be dull- determine height
palpation of abdomen
light palpation over all 4 quadrants, tenderness normal in adults near xiphoid process, over cecum or over sigmoid colon
light vs deep palpation
light- 1-2 cm in gentle rotating motion, identify superficial organs/masses/areas of tenderness
deep- bimanual (one hand over other), 3-4 cm, assess organs masses or tenderness
palpating inguinal lymph nodes
using pads of fingers, non tender and slightly palpable, not usually done
palpating aorta in abdomen
use opposing thumb and finger, palpate aortic pulsation in upper abdomen slightly left of midline, in adults is approx 2.5 cm wide
palpate liver (enlargement)
palpation: pt holds breath, push up under costal margin, normal to feel edge of liver as diaphragm pushes it down during inspiration
hooking: pt holds breath, hook fingers under costal margin, normal to feel edge of liver as diaphragm pushes down during inspiration
scratch test- scratch gets louder as nearing liver edge (location of liver)
palpating spleen enlargements
pt holds breath, push up under costal enlargement (right side), must be enlarged 3x normal size to be felt
rebound tendernes (blumberg’s sign)
assess all pts, suggests peritoneal inflammation (appendicitis, peritonitis), insert hand at 90 degree angle slowly and deeply- life up quickly, pain will be increased with removal of hand with peritooneal inflammation, then do away from area of pain (different quadrant)
Pain in RLQ tests
psoas signs
obturator test
rovsing’s sign
(inflammation- appendicitis, ovaria, diverticulitis)
Psoas sign
pt is supine with right lef pushed towards head, nurse pushes down on right thigh pushing towards pts head as pt tries to hold leg up, pain in RLQ is psoas sign
obturator test
pt supine with r light up flexing knee and hip at 90 degrees, nurse holds knee and angle and rotates leg internally and externally, pain in RLQ will give positive obturator sign,
rovsing’s sign
nurse presses in LLQ and pt reports pain in RLQ
RUQ complaint- Murphy’s sign
patient supine, support hand underposterior lower ribs, ask pt to take deep breath and hold, nurse pushes up under costal margin, positive- pt attempts to stop inspiratory effort, tenderness alone is NOT a positive, inflammation- possible cholecystitis/liver involvement
Ascites assessment (fluid in abdomen)
protuberant abdomen and bulging flanks indicates fluid it peritoneal cavity, ascites: cirrhosis/liver tumor, blood in abdomen, ascites is detectable after 500mL accumulated, asses for: shifting dullness, fluid wave
shifting dullness (ascites)
Percuss MCL to MAL (tympanic to dull), turn to right side and repeat with percussion, dullness: shift with free fluid
fluid wave (ascites)
hand midline abdomen- pressure will help to stop wave through fat, hands on both sides of abdomen: tap on one side and palpate the other- fluid wave pushed to opposite side means free fluid, positive sign indicates 1.5L of fluid present
superficial abdominal reflex
stroke tongue depressor or handle of reflex hammer 4 quadrants towards umbilicus one at a time, normal is when muscles contract- umbilicus moves towards stimuli, absent in pts with upper and lower motor neuron diseases (ALS)
health promotion for liver
safe sex, do not share items with bodily fluids, ensure safe tattooing practices, use clean needles, drink alcohol in moderation, avoid mixing alcohol with medications, do not use illegal drugs, eat only boiled or thoroughly cooked foods when travelling,***a cirrhotic liver can shrink downn to a fraction of its normal size and function
review hepatitis make slides if needed
bowel obstruction
history of prev abdominal surgery with adhesions, vomiting, distended abdomen after 2nd day, radiograph shows air filled lopps or smal bowel with air fluid levels, hyperactive bowel sounds earlier then hypo or absent sounds, dehydration and loss of electrolytes, accumulation of fluid and gas in bowel above the obstruction, colicky pain from strong peristalsis above obstruction, fever, pressure from excess fluid and gas, hypovolemic shock
colon cancer
use fecal immunochemical test, average risk: 50-74 yrs old with no first degree, after age 50 get FIT every 2 years, increased risk- family history of colerectal cancer, age 50 with colonoscopy every 5 years or 10 years
stool tests
c&s, occult blood (FOBT), ova and parasites
radiologic procedures
x-ray, barium swallows or enemas, IVPs, CT, MRI
rectum
12 cm long, distal portion of large intestine, from sigmoid colon (3rd sacral vertebrae) to anal canal, above anal canal- recutm dilates and turns posteriorly
anal canal
outlet of GI tract, 3.8cm long, lined with modified skin with no hair or sebaceous glands, merges with rectal mucosa at anorectal junction, canal slants forward towards umbilicus
rectal suppository
insert 4cm into anus against wall of rectum, pt should lay flat for 5 minutes, ask abt discomfort and evaluate relief of symptoms
enema
solution promotes peristalsis and defecation, volume breaks up fecal mass, stretches rectal wall and initiates defecation reflex, used to treat constipation, administer meds or empty bowels
types: tap water, normal saline, low volume hypertonic saline, soapspuds solution, oil retension
each of them exter a different osmotic effect to move fluids btwn colon and interstitial spaces beyond intestinal wall, children and infants only receive saline
should not be used regularly
evaluation: stool evacuated, discomfort diminished, inspect fecal return
stop or slow enema if: severe cramping, bleeding, pain, vagal nerve stimulation (light headedness), pt is unable to hold solution
nasogastric tube
provides food and meds, used for feeding sor giving person extra calories, used to suction out stomach contents (OD, bowel obstruction)
measure: earlobe to nose tip, earlobe to xiphpid process
tips: pull back if feeling resistance, once past posterior nasopharynx- have pt swallow, pull back tube for signs of distress, assess placement by withdrawing stomach contents, injecting air or submerging in water
contraindications: nasal bleeding, obstruction, facial trauma, basal skill fracture
MSK assessment consists of
muscles, bones, joints (cartilage, ligaments and tendons)
subjective msk assessment
demographics: (occupation and hobbies)- potential for injuries? are they staying active?, living alone- risk for falls
pt history: fractures, polio, muscle injuries/disorders, parathyroid disorders, menopause, bone infections (osteomyelitis), surgeries and hospitalisations
family history: osteoporesis, bone cancer, rheumatoid arthritis, osteoarthritis, muscular disorders
allergies: food intolerances (lactose), environment and medications
MSK subjective- medications
medications: steroids (inhibits calcium absorption), calcium, phosphorus and magnesium (bone growth + remodeling), vitamins A C D (calcium absorption) K B12 (bone growth + remodeling), anti inflammatory (delay bone healing and calcification), muscle relaxants (injury risk), contraceptives (impair bone density), HT (in menopause can treat osteoporosis), complementary substances like chondroitn and glucosamine (for joint health)
dadspies for bones
d- calcium/vit D
a- alcohol increases parathyroid hormone which causes calcium loss
d- drugs
s- smoking lowers bone density
p- physical (bone mineral density (BMD) check)
i- immunisations
e- physical activity? sedentary lifestyle
s- stress financial, income decreases can lead to obesity and inactivity
diet and excersize (MSK)
weight bearing activities- walking or moderate weightlifting to build and retain bone mass
agins- calcium absorption is high (60%) in infants and young children, decreases to 15-20% in adulthood, increased during pregnancy, decreases with age
OPQRSTUA (varies by complaint)
o- acute (less than 4 weeks) vs chronic
p- rest? medication? ice? weather (worse when cold and damp- arthritis)
q- describe feeling (burning- nerve, aching, dull, deep- bone, cramping, sore- muscle)
r- region and radiation (muscle- myalgia, bone joint- arthralgia), localised (mono vs polyarticular)
s- scale from 1-10, issues with ADLs
t- worse at times (worse in morning- rheumatoid, worse after rest or end of day- arthritis) chronic vs intermittent
u- what do they think it is
a- associated symptoms (nerve impairment- weakness, numbness, tingling, arthritis- stiffness or limited motion, inflammed/infection- swelling and warmth, fever, chills, injury- deformity, bruising, swelling, cancer- weight loss, anorexia
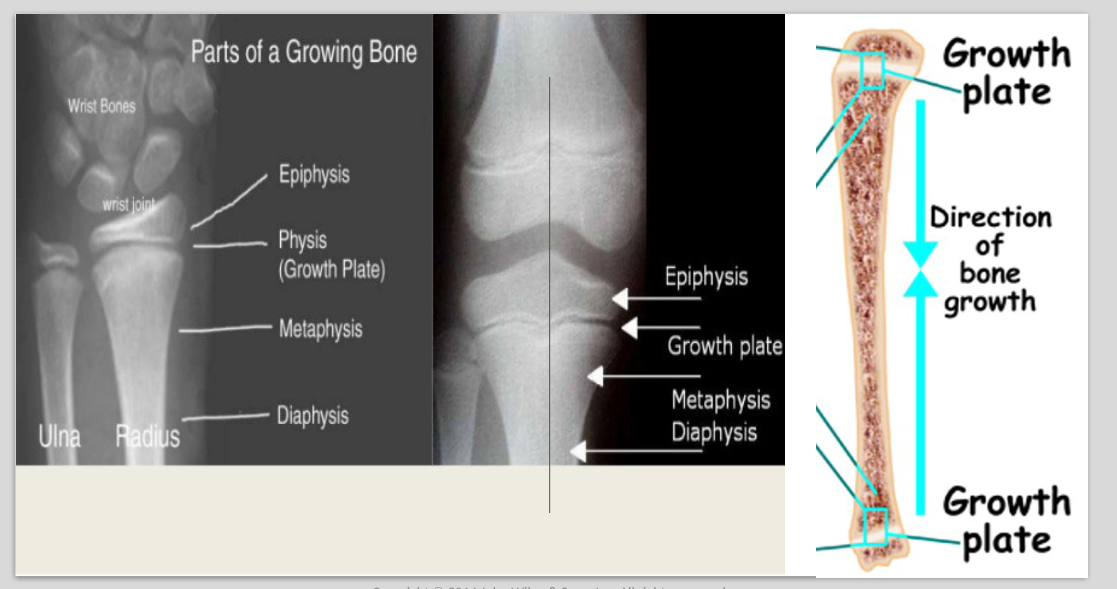
growing bone
finish bone growth at 18 in females and 21 in males (epiphyseal plates close, cells stop dividing, the plate fades and the epiphyseal line remains) salter (growth plate) fractures may alter growth
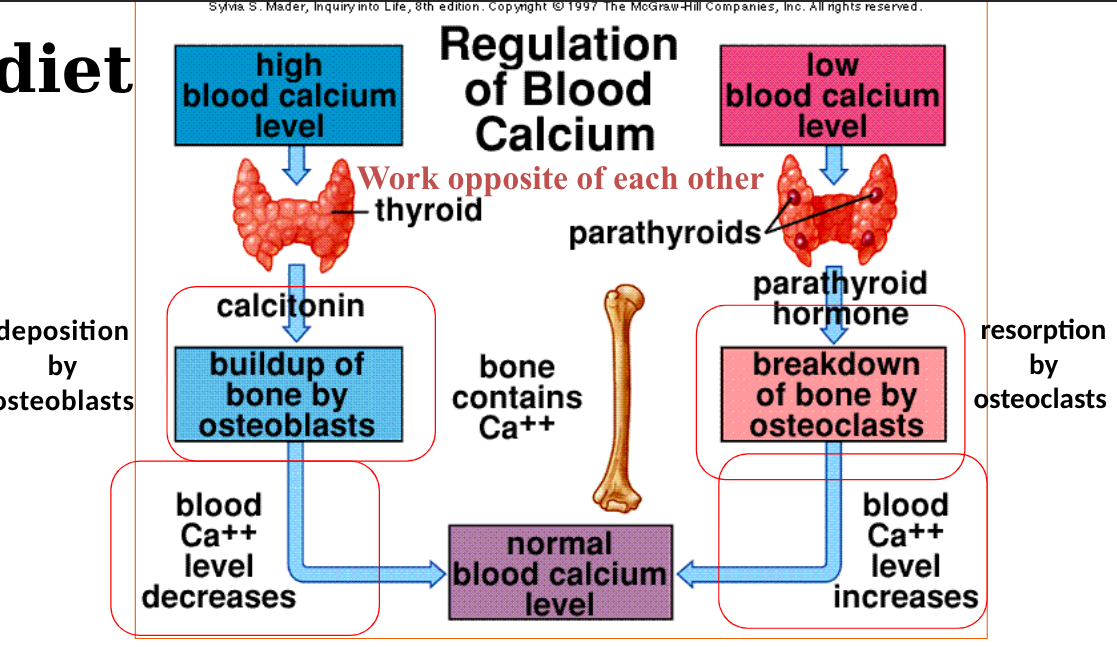
changes to bone with age
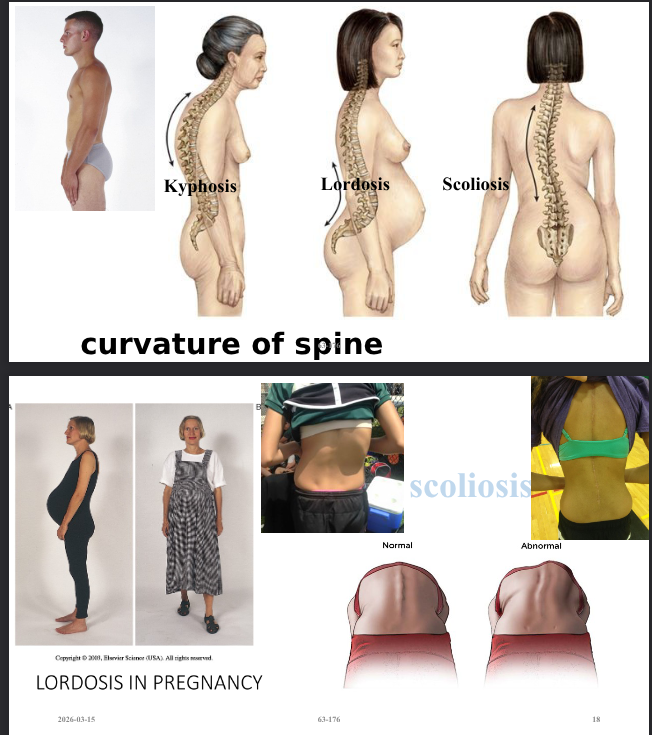
loss of bone mass- reapsorbtion more rapid that deposition (porous - weakened bones is called osteoporosis), britte bones, results in changes in posture, height and fractures, exagerated thoracic spine (kyphosis)
changes to bone with gender
females- small bone frames, rapid loss 5-7 yrs after menopause, female bones are smaller and have higher incidence of osteoporosis in females
males- slower loss, larger and stronger bones
risks to bones
genetic background- shape of bone, melanin- vit D synthesis
hormonal factors, physical activity and calcium intake
diet affecting bones
changes to spine shape
general survey for MSK
posture- sitting/standing erect, assess for symmetry in shoulders, scapulae, iliac crests, posterior superior iliac spines and gluteal folds
gait (walk across room if possible)- do they need device, smooth, balanced, continous, arms swing in opposition to legs, base is 5-10 cm, rises from sitting with ease
balance- walk on tip toes and heels, walk in heel to toe fashion, backwards, hop on one foot (ataxia- irregular, uncoordinated movements or losing balance, cerebellar disorder like parkinsons, MS, bran tumour, inner ear condition or medications)
do we do vital signs for MSK?
YES
INSPECTION of MSK
symmetry, erythema, atrophy, deformity, swelling (SEADS acronym)
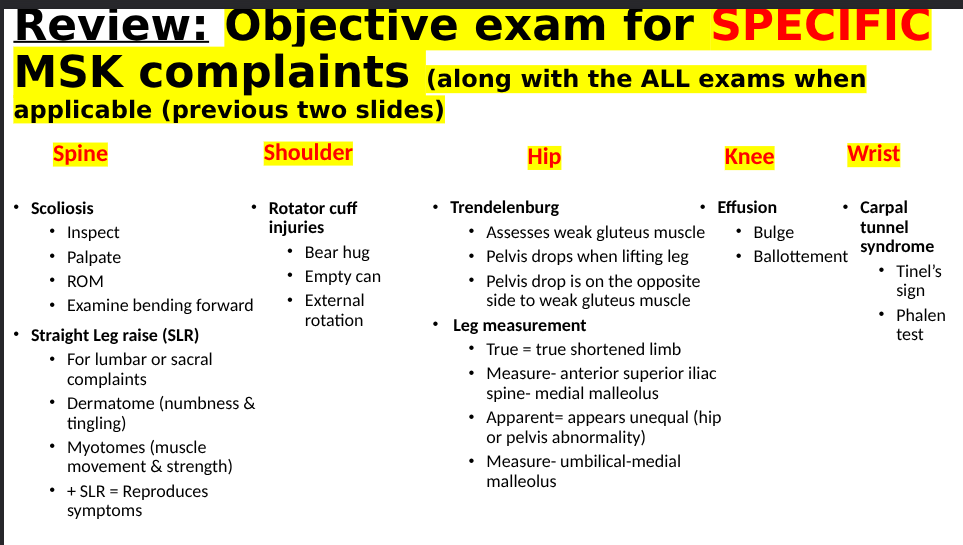
review slide for general objective MSK complaints
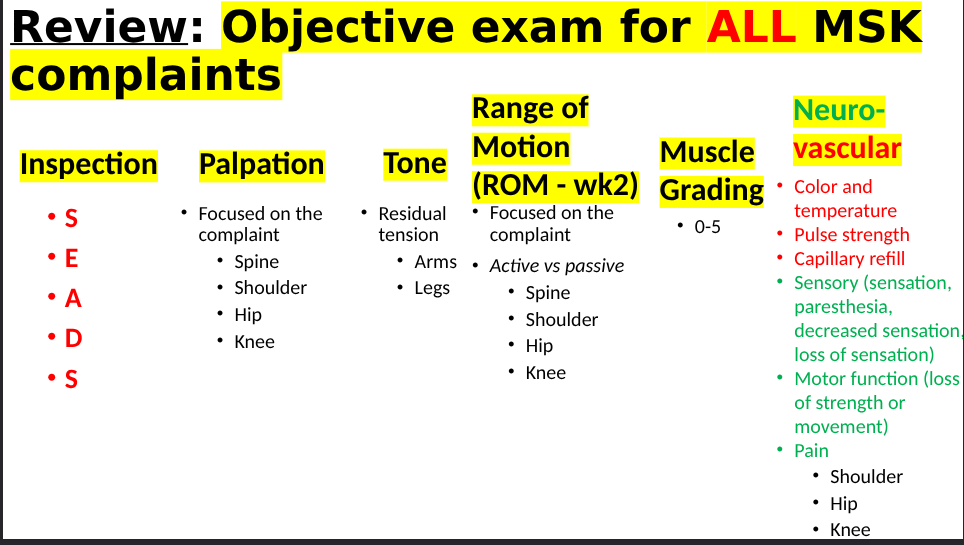
review slide for specific MSK complaints