Laboratory Evaluation of Hemostasis part I
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
Marrow disease thrombocytopenia
Due to:
Drugs(chloramphenicol, sulfa) toxins
Infections: BVD, canine distemper, Parvovirus
Estrogen, bracken fern poisoning
Suspect Thrombocytopenia due to marrow disease?
A. Start off with a blood smear and look for signs of Thrombopoiesis
B. Definitive diagnose via bone marrow aspirate
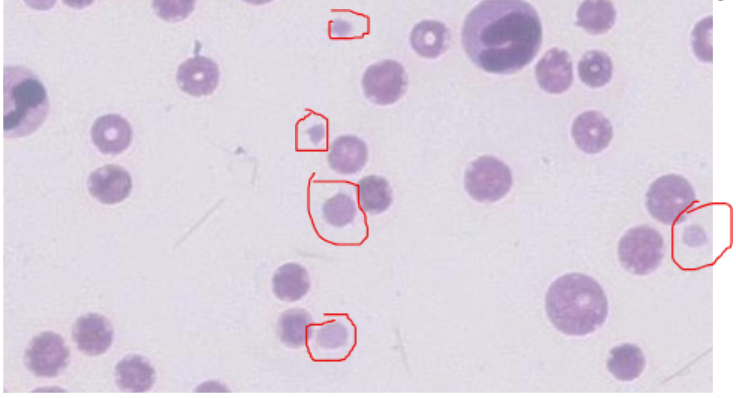
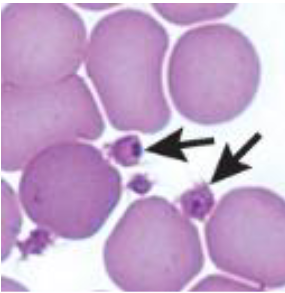
What are signs of Thrombopoiesis?
Large platelets (Large- reactive/immature)
Macrothrombocytopenia is inherited by what dog breeds?
Cavalier
Norfolk terrier
What species is known to clump?
cats
cows
Causes of thrombocytopenia: Abnormal distribution(sequestration)
Spleen enlargement
Liver disease
Causes of thrombocytopenia: Idiopathic or multifactorial
combined decreased production and survival
Causes of thrombocytopenia: decreased survival
Increased destruction
Increased consumption
Causes of thrombocytopenia: decreased production
Inadequate megakaryocyte production
Bone marrow disorders
What answer best matches the image?
Thrombocytopenia
Macrothrombocytopenia is inherited by what species?
cats
What leads to clumping?
Delayed transferring from syringe to tube
Inadequate mixing
Old samples > 5 hrs
The two causes of pseudothrombocytopenia
Large platelets and Platelet clumping
Decreased survival → spleen
increased Destruction
Ab-mediated
Idiopathic
Increased Activation &/or consumption → blood vessels
Vasculitis
DIC(disseminated intravascular coagulation)(intravasc. Consumption)
Endotoxins
Sequestration
Reversible(hypothermia)
or
Irreversible(Endotoxins) pooling in the lungs
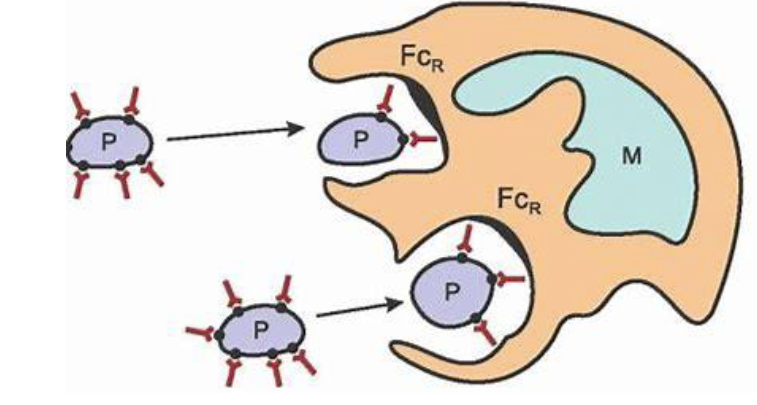
Pathogenesis of Immune-mediated Thrombocytopenia (IMT)
Can be seen with IMHA
Formation of anti-platelet antibodies → Macrophages engulf the antibody-coated platelets→ Thrombocytopenia
Pathogenesis of Immune-mediated Thrombocytopenia diagram
Pathogenesis of consumptive thrombocytopenia
Damage to the endothelium> activation of platelets> platelet aggregation
Platelet activation and aggregation→ consumption and removal from the blood→ Thrombocytopenia
A dog’s CBC results included a mild leukocytosis, mild anemia with schizocytosis, keratocytosis, and thrombocytopenia (100,000/μL; RI 150,000–450,000). The thrombocytopenia was likely due to:
B. Intravascular consumption of platelets
Infectious Canine Cyclic Thrombocytopenia(anaplasmosis)
Pathogenesis: probably immune-mediated destruction or sequestration
Agent: Anaplasma platys
Vector: Ticks
Cyclic aspects: peak parasitemia followed by thrombocytopenia
Agent: Anaplasma platys
Marked thrombocytopenia causes…
hemorrhage
Typically [platelet] < 20,000/μL
Hemorrhage does not typically = Thrombocytopenia
Does blood loss cause thrombocytopenia?
Usually not, Only marked blood loss →mild thrombocytopenia.
(should have concurrent anemia & hypoproteinemia)
Will not spontaneously bleed unless they are less than?
20,000 uL
Thrombocytosis (Primary or secondary)
Definition: [Plt] > appropriate upper reference limit [URL]
1. Increased production or 2. Redistribution
Increased production can be?
clonal/non-clonal
Clonal: Primary(cancer)
Rare* [Hemic neoplasia] / Acute megakaryoblastic leukemia
> 2x URL: If extreme thrombocytosis > 1,000,000/μL Bleeding/Clots (decreased function)
URL
upper reference limit
Non-clonal: Secondary(non-cancerous)
As a reaction to other conditions [Reactive Thrombocytosis]
≤ 2x URL
Increased production (Reactive Thrombocytosis) causes
*Inflammation (infection, immune mediated) IL-6 stimulates Thrombopoietin(Tpo)
*Iron deficiency
*Recovery from thrombocytopenia- Rebound Thrombocytosis
*Post- Splenectomy
2. Redistribution
Exercise
Epinephrine
Summary Hemostasis 3 stages
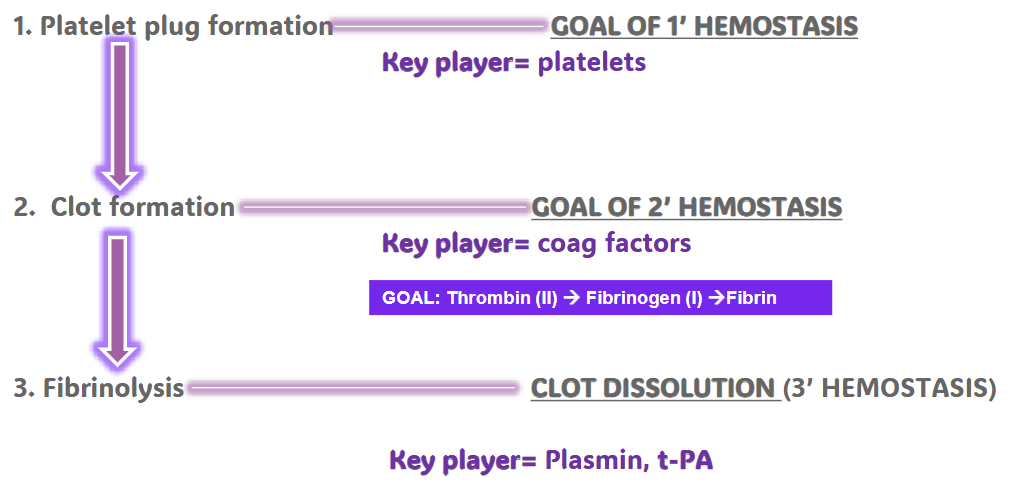
The receptor for vWf (adhesion) is
GPIb
The receptor for fibrinogen (aggregation) is
GpIIb/IIIa
Deficiency in GpIIb/IIIa is
glanzmann thrombasthenia
seen in otterhounds, great pyrenees, and horses
Deficiency of vWB factor
Von Willebrands disease
doberman pinscher
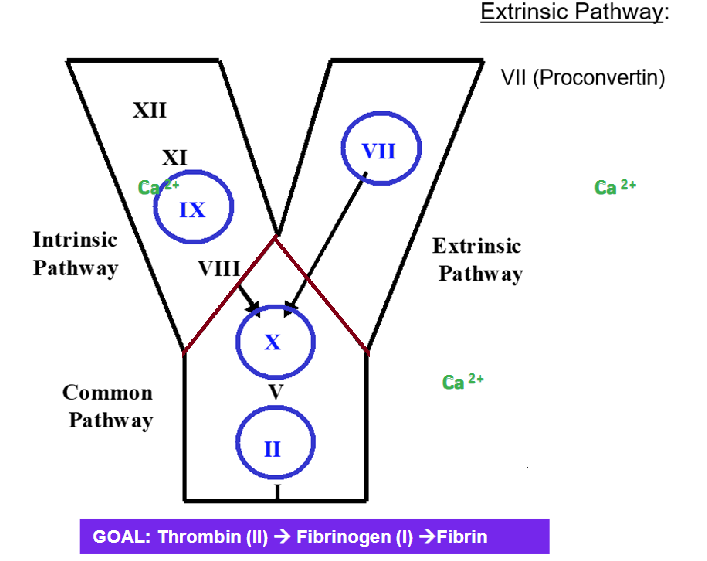
COAGULATION CASCADE simplified
Why is it important to divide 1’ & 2’?
Types of bleeding differ(sometimes you can guess the system affected based on clinical signs)
Lab tests usually evaluate either 1’ or 2’ hemostasis
DDx are different depending on which part of the coagulation cascade is affected
CLINICAL APPROACH Determine:
If the bleeding is the result of a defect or local tissue disease?
If there is a defect, localize it → Narrow DDx list
For primary hemostasis to occur you need…
1) Normal subendothelium [disorders are rare]
2) Adequate #s of platelets
3) Normal platelet function
4) vWf
5) Fibrinogen [ can be 1’/2’][rare]
Any 1’ defect…Your DDx..
1. [Plt] adequate?? → 1) Thrombocytopenia
2. vWF??? → 3. Abnormal plt function(receptor deficiencies)
3. Normal PLT function (receptors!) ???→ 2. vWf deficiency
Big point is for 1’ hemostasis need…
Therefore for 1’ disorders the DDx list would be:
1) Thrombocytopenia → 4 factors
2) vWf deficiency → %
3) Abnormal plt function(receptor deficiencies)
Intrinsic 12,11,9 & 8 Walmart analogy
Why pay $12 when you could pay 11.98
Extrinsic factor 7
Has the shortest half-life
Good screening test

test extrinsic and common
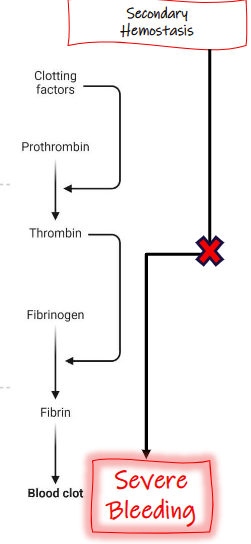
Secondary hemostasis =
Primary hemostasis =
muscosal bleeding
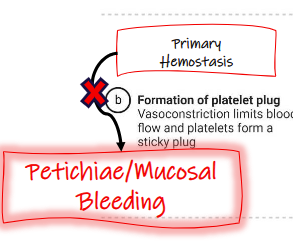
Clinical signs: Primary
Petichiae- Thrombocytopenia/vasculitis(pinpoint hemorrhages)
Mucosal bleeding
Clinical signs: secondary
Large hematomas/SQ bruising- usually but not specific
Cavity bleeding: hemoabdomen, hemothorax, hematerosis
Frank hemorrhage
Clinical signs: non-specific
can be both 1’/2’
Excessive bleeding following surgery/venipuncture
Ecchymoses(paint brush style hemorrhages)
What 3 broad differentials should be considered for 1’ hemostatic disorders?
1) thrombocytopenia
2) vWf deficiency
3) abnormal platelet function
Morphology(microscopy) comments
No platelet clumps at feathered edge/body of smear
[Plt] is inadequate; manual count= 0-1 plt/hpf