acromegaly, gigantism and dwarfism
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
21 Terms
what hormones have a negative feedback on the release of GH
somatostatin (in the hypothalamus) and insulin like growth factor (in the liver)
excessive secretion of GH usually due to a pituitary somatotroph (cells in anterior pit that produce GH) that happens in adulthood only (40-45yo avg onset), after the epiphyseal closure
acromegaly
what is the onset like for acromegaly
insidious onset w slow progression (dx takes like a year)
acromegaly sx
acral (facial bones/lips/nose/tongue) overgrowth, soft tissue overgrowth, skin thickening
enlarged jaw, hands, and feet (inc glove and shoe size over time)
coarse facial features w big nose and frontal bones
macroglossia (big tongue)
deepening of the voice (enlargement of soft tissues of pharynx and larynx)
hand paresthesias
headaches and visual changes due to pressure from the adenoma
cardiovasc disease (HTN, cardiomyopathy)
type 2 Dm (inc gluconeogenesis and lipolysis)
arthropathies and back pain
single BEST test for acromegaly dx
serum Insulin like growth factor-1
normal serum IGF-1 when screening for acromegaly means what
strong evidence against acromegaly
unequivocal serum IGF-1 when screening for acromegaly or gigantism what can we do next on top of that to confirm
oral glucose tolerance test (measures serum GH before and after)
what is the most specific test to dx acromegaly and gigantism
oral glucose tolerance test (pos= over 1 after 2hrs)
if a pt has high IGF-1 or unequivocable IGF-1 and high GH after oral glucose tolerance test (shows inadequate suppression) whats the last step to dx acromegaly or gigantism
pituitary MRI (see if its extra-pituitary acromegaly or a GH-secreting pituitary adenoma)
whats the surgical tx for acromegaly
endoscopic transphenoidal surgery
if we cant do surgery on the acromegaly pt what meds can we give
somatostatin analog (octreotide, ianreotide), dopamine agonist (cabergoline), competitive GH receptor agonist (pegvisomant)
what are the tx goals for a pt w acromegaly
lower serum IGF-1 and Gh concentrations back to normal (improves sx and soft tissue growth and reverses metabolic abnormalities like T2D but cant reverse bony changes)
GH excess that occurs before the fusion of the epiphyseal growth plates AKA happens in kids
gigantism
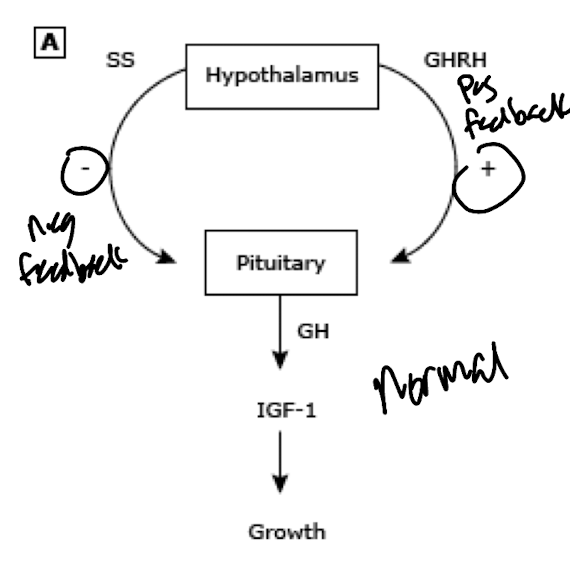
what is the NORMAL pathway for GH release
hypothalamus releases GHRN (pos feedback) and somatostatin (neg feedback) to the anterior pit → GH released → IGF-1 released → grow
what are some causes of gigantism
either too much GHRH in hypothalamus, too much GH in pituitary all on its own, or too little somatostatin (too little neg feed back)
gigantism sx
often around 13 but earlier in girls
big hands and feet
coarsening of the facial features
excessive sweating
progressive macrocephaly
adenomas (associated w amenorrhea in girls and sx of tumor compression in boys)
dramatic linear growth
gigantism surgical tx
endoscopic transphenoidal surgery
gigantism tx if we cant do surgery
dopamine analog (bromocriptine), somatostatin analog (octreotide), competitive GH agonist (Pegvisomant)
what causes dwarfism
growth hormone decifiency
diagnostic tests for dwarfism
serum IGF-1, Xray for bone age, growth hormone provocation
dwarfism tx
recombinant growth hormone (start as young as possible) (very safe and effective, few ADR)
theraputic monitoring every 4-6mo for height velocity, IGF-1 and bone age