Geriatrics Baker PP
1/122
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
123 Terms
Geriatric stats
>65 increased by 300% over last 50 yrs
U.S. will have 73 million people > 65 years of age by 2030; 83 million. by 2050
•The geriatric population is becoming more racially & ethnically diverse
•Older adults/elderly= 65 years and older
•Elderly are accessing surgical services at a higher rate than any other age group
Periop risk
Elderly have increased risk periop complications
gradual organ decline
chronological age does not equal function status
Frailty= increased vulnerability to adverse outcomes
•Elderly adults prone to progressive decline of baseline functions
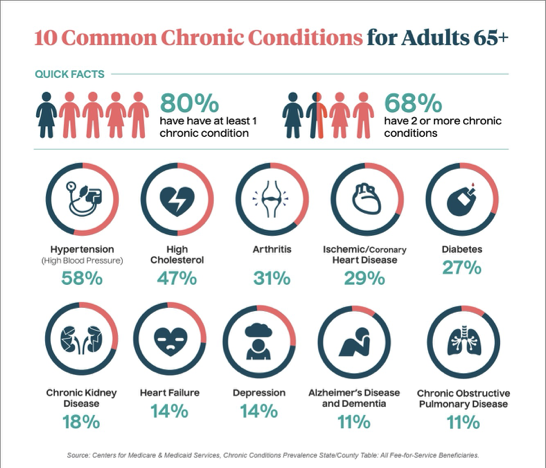
•Increases in age related co-morbidities
•Increased ASA classifications
•Increased morbidity & mortality in post op period
A& P changes affect anesthetic management when
Peak physiological at 30
Most common post op complications
cardiac, pulmonary and neurological
factors that affect complication risk are
reduced reserve capacity, functional decline & comorbidities.
ASSESSMENT CATEGORY | SCREENING TOOLS |
COGNITION | MINI-COG 3 ITEM RECALL & CLOCK DRAW |
DECISION MAKING CAPACITY | LEGALLY RELEVENT CRITERION: 1)understanding 2)appreciation 3)reasoning 4) choice |
DEPRESSION | PATIENT HEALTH QUESTIONNAIRE-2 (PHQ-2) |
RISK FOR DELERIUM | REVIEW: cognitive diseases, metabolic disturbances, functional impairments, polypharmacy |
ALCOHOL & SUBSTANCE ABUSE | MODIFIED CAGE |
CARDIAC | ACC/AHA ALGORITHM & METS |
PULMONARY | REVIEW RISK FACTORS & TESTS (PFTs) |
FRAILTY | WEIGHT LOSS, WEAKNESS, EXHAUSTION |
FUNCTIONAL STATUS | TUGT: TIMED UP & GO TO measures the time to get up from chair and walk a measured distance |
NUTRITIONAL STATUS | BMI SERUM ALBUMIN |
MEDICATIONS | PRESCRIBED & OTC |
OTHER | DNR & ADVANCED DIRECTIVES |
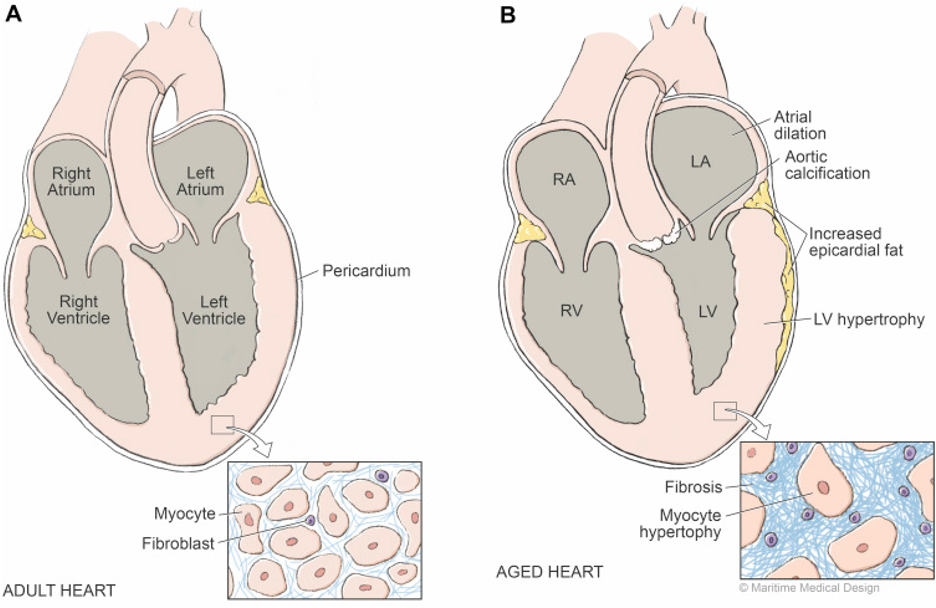
CV system
•Heart & vascular system is less compliant
•Widening pulse pressure: ↑ SBP with ↓ in DSP
•Increased afterload
•Increased SBP: decrease in arterial elasticity
•Ventricular thickening/hypertrophy & slower myocardial relaxation = late diastolic filling & diastolic dysfunction
•Prolonged ejection time
•Atrial contraction becomes very important to maintain adequate ventricular filling
Conduction system and arrhythmias
•Calcification of heart’s conducting system & loss of sinoatrial node cells= Atrial Fib, SSS, 1AVB, 2AVB & arrhythmias
•Valve calcifications, Mitral and Aortic stenosis & regurgitation→ prolongs EF time
ANS
Increased circulating catecholamines but have diminished end organ adrenergic responsiveness (down regulation of receptors)
•Results in a decreased ability to increase HR in response to hypotension, hypovolemia and hypoxia
•Prolonged circulation times = faster inhalation induction but slower induction time with intravenous agents
What increases in CV system in Geriatrics
•LV wall thickness/ hypertrophy
•Afterload and LV wall tension
•Cardiac workload d/t ↓arterial compliance
•SBP
•Peripheral vascular resistance
•Circulation time: reduced pumping action → decreased CO
•Dysrhythmias: fibrosis in conduction system & loss of SA node cells
•Vagal tone: ↓ in sensitivity of adrenergic receptors = ↓ HR
•SV: heart does not atrophy w/age.
•When the heart is stressed, demands for ↑ in CO met with modest increases in HR, then ↑ in LVEDP, then greater SV
What decreases in CV system in Geriatrcs
•Cardiac reserves manifested as exaggerated drops in BP
•CO: due to aging process and ↑ in afterload
•CI: response to ↓ requirements for perfusion & metabolism RT age related skeletal muscle atrophy and loss of tissue mass in organs with high metabolic rates
•Resting HR: due to ↑ in vagal tone & normal loss of one beat/min >50 years
•LV compliance: stiffer myocardial fibers & replace fibers w/non muscle connective tissue
•Blood volume by 25%
•Perfusion to vital organs
•Chronotropic & Inotropic responses: ↓ adrenergic receptor quality → decreased target organ response
•Baroreceptor function: decreased sensitivity of stretch receptors
•Adrenergic sensitivity: quality of receptors ↓ with age
HTN
•Hypertension ↑ risk for post-op complications, risk doubles for every 20mmHg SBP & 10 mmHg DBP
•Decreased vein compliance→ decreased venous return and reduced atrial filling
•Decreased baroreceptor sensitively in aortic arch & carotid sinuses in response to BP changes → hypotension
•Changes in the heart’s regulation of Calcium→ myocardium must generate force over a longer period after excitation which prolongs the systolic phase of the cardiac cycle
CO & SV
Reduced conduction velocity & decreased venous blood flow —> decreases CO and SV
Increased BP is RT increased PVR and decreased arterial elasticity increase myocardial workload
Decreased cardiac reserve affects response to anesthesia
CV
•Myocardium has ↓ sensitivity to Beta- adrenergic activity = ↓ HR & lower cardiac dilation at end diastole & systole
•Not as able to adjust to the stresses of anesthesia & surgery due to decreased cardiac reserve
The aging heart- morphological changes
progressive loss of elasticity of large arteries
Generalized LVH
Fibrotic changes and diminished elsastricy of heart muscle (reduced myocaridal compliance)
Reduced compliance of LVEF
CO maintained by increased EDV
The aging heart- functional effects
Increased SBP
Increased afterload for LV
Increased LVEDV
Volume sensitive and volume intolerant CV system
Inability to optimally response to stress (cannot significantly increase LVEF)
Increased SV
The aging heart both changes
elderly pts may not maintain BP when challenged with minor hypovolemia or added CV stressees
Sympathetic blockage from neuraxial anesthesia may l/t hypotension in hypovolemia
Age related CV changes- RV
Reduces systolic & diastolic function
Age related changes in LV
LVH
Dependence on atrial contribution
Age related impaire dcontractility and relaxation
Age related changes vascualr strucutres
Increased arterial stiffness
Systolic HTN
Age related changes CO
Preserved resting CO
Preserved EF
Age related changes in physiology
Blunted baroreceptor reflex
Decreased adrenergic responsiveness
Age related changes in response to stress
Dereased reliance on HR
Increased CO due to increased SV
Age related changes myocardial hypertrophy
Mechanism: Apoptotic cells not replaced are l/t compensatory hypertrophy of existing cells; reflected waves during late systole create strain on myocardium l/t hypertrophy
Consequences: Increased ventricular stiffness, prolonged contraction and delayed relaxation
Anesthetic implications: failure to maintain preload l.t decrease CO; excessive volume more easily increases filling pressure to CHF levels, dependent on NSR and low-normal HR
Age related changes- myocardial stiffening
Mechanism: Increased interstitial fibrosis, amyloid deposition
Consequence: Ventricular filling dependent on atrial pressure
Age related changes- Reduced LV relaxation
Mechanism: Impaired calcium homeostasis; reduced beta receptor responsiveness, early reflected wave
Consequences: Diastolic dysfunction
Age related changes- Reduced beta receptor responsiveness
Mechanism: Diminished coupling of beta receptor to intracellular adenylate cyclase activity, decreased density of beta receptors
Consequences: Increased circulating catecholamines; limited increase in HR and contractility in response to endogenous and exogenous catecholamines; impaired baroreflex control of BP
Anesthetic implications: Hypotension from anesthetic blunting of sympathetic tone, altered reactivity to vasoactive drugs; increased dependence on Frank-Starling mechanism to maintain CO; labile BP, more hypotension
Age related changes- Conduction system abnormalities
Mechanism: Apoptosis, fibrosis, fatty infiltration, and calcification of pacemaker and His-bundle cells
Consequence: Conduction block, sick sinus syndrome, atrial fibrillation, decreased contribution of atrial contraction to diastolic volume
Anesthetic Implications: Severe bradycardia with potent opioids, decreased CO from decrease in end-diastolic volume
Age related changes- Stiff arteries
Mechanism: Loss of elastin, increased collagen, glycosylation cross linking of collagen
Consequences: Systolic hypertension Arrival of reflected pressure wave during end-ejection leads to myocardial hypertrophy and impaired diastolic relaxation
Anesthetic implications: Labile BP; diastolic dysfunction, sensitive to volume status
Age related changes- Stiff veins
Mechanism: Loss of elastin, increased collagen, glycosylation cross linking of collagen
Consequences: Decreased buffering of changes in blood volume impairs ability to maintain atrial pressure
Anesthetic Implications: Changes in blood volume cause exaggerated changes in cardiac filling
Major risk factors
•Significant exercise intolerance
•Angina
•History of M.I. within the past 6 months
•Arrythmias
•Acute coronary syndrome
•Decompensated CHF
•Valvular disease
Cardiac assessment
•Based on the American College of Cardiology/AHA
•Cardiovascular disease is the most common concomitant illness in the older adult
•CV disease is the primary cause for preoperative and postoperative risk
•Most frequently associated co-existing diseases
Risk stratification tools
METS
Periop cardiac risk calculator
Most frequently associates co-exisitng disease 4
•HTN, HLD
•CAD
•CHF
•MI & cardiac arrest post surgery
Leading cause of death in post op
•MI most common cardiac complication & leading cause of death in post op period
Preexisting HF
•Patient with pre-existing heart failure has double the risk of developing post-op complications
Anesthesia implications: Cardiac 4
Adjustments needed due to reduced cardiac reserve
Increased sensitivity to fluid shifts and blood loss
Careful management of intraoperative hemodynamics (20% of baseline)
Individualized anesthetic plans for elderly patients
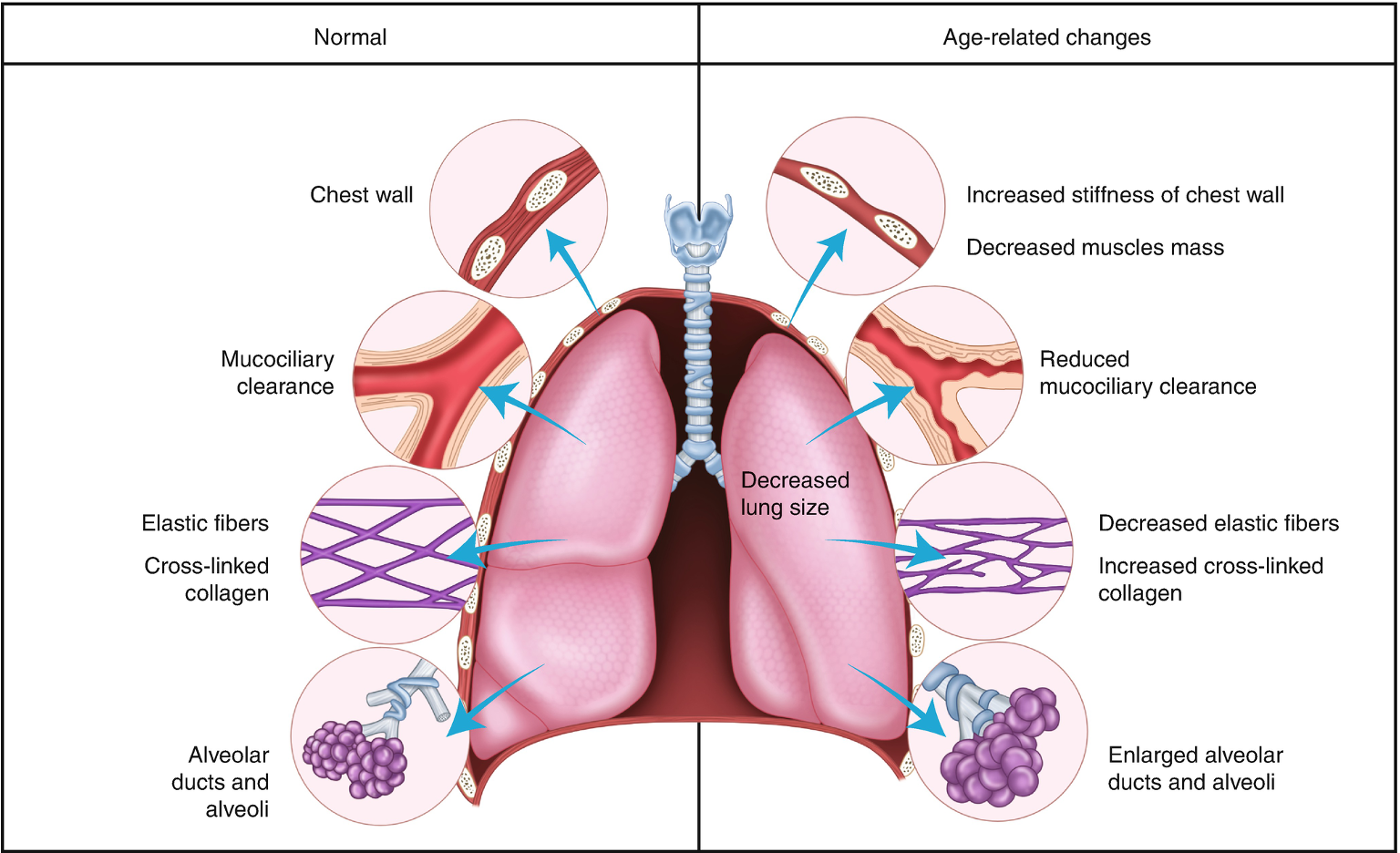
Structural changes that decrease chest wall compliance
•Calcifications of chest wall, intervertebral & intercostal joints
decreased intercostal muscle mass
•Diaphragm is flattened, ↓ in intervertebral disc size & spinal lordosis will further decreases chest wall compliance
Pulmonary parencyhma changes
loss of elastic tissue recoil of the lung bronchioles, alveoli & alveolar ducts l/t Reduced functional alveolar surface area for gas exchange
Imapired V/Q matchhing incrases physiological shunt
•Small airway diameter (Premature closing of the airways) raises closing volume

LUNG COMPLIANCE vs ELASTANCE
opposite to each other
COMPLIANCE (how easy is it to fill the lung)
•A measure of distensibility àchange in vol/change in pressure
•The stretch of the lung, depends on elasticity & surface tension
•The higher the compliance, the easier it is to stretch, doesn’t return to original shape or volume
•Increases as elastance decreases
ELASTANCE(recoil- think elastic band)
•A measure of elastic recoil à change in pressure/change in volume
•Response to a mechanical load
•Decreases as compliance increases
•Wants to return to its original shape or volume when stretch is released
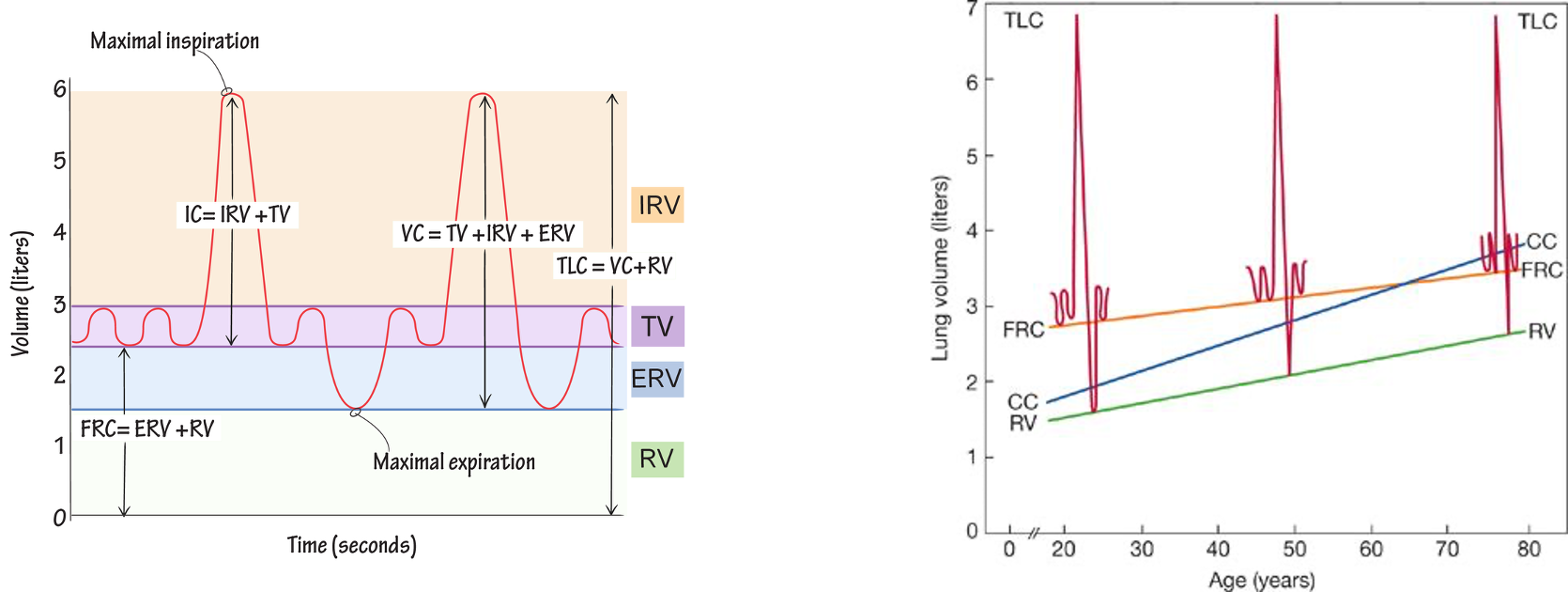
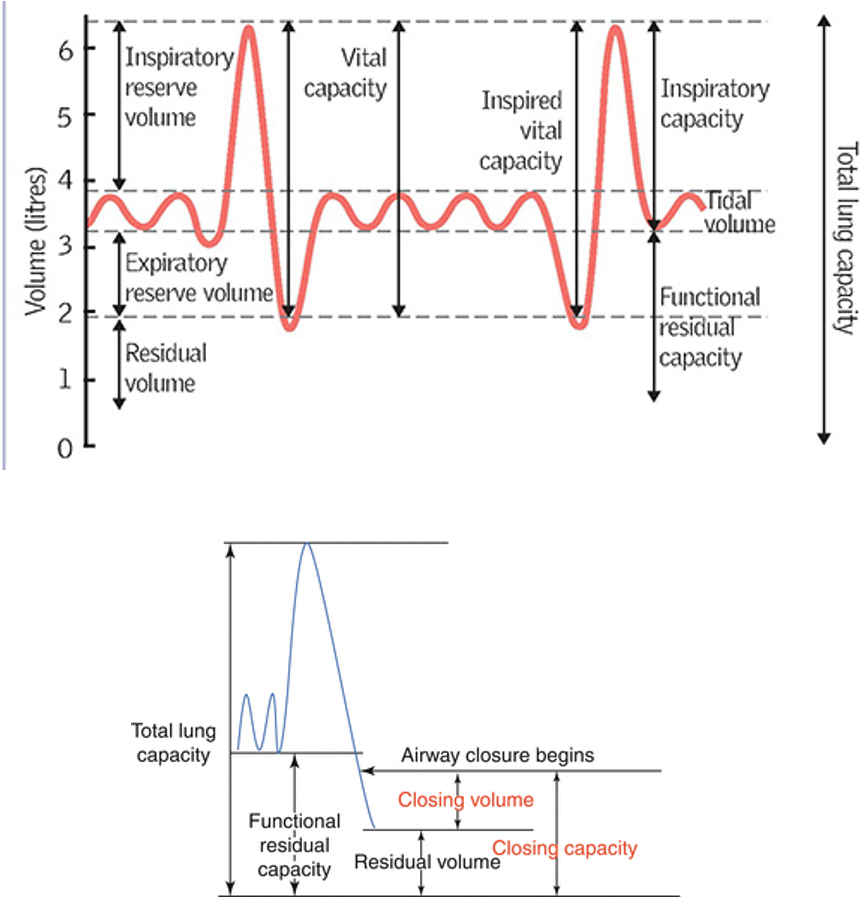
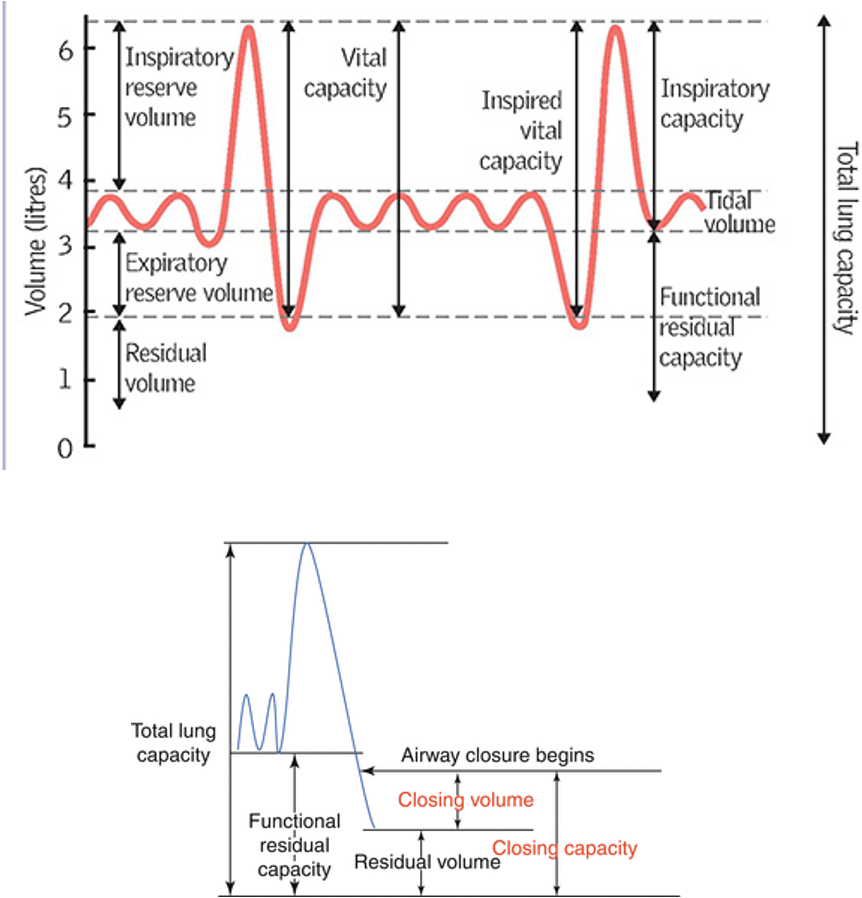
Lung volumes
Lung compliance
•An ↑ in lung compliance impairs V/Q matching, ↑physiological shunt, and ↓ O2 exchange at alveolar level
•Elastic recoil is necessary for maintaining small airway diameter
•Increased lung compliance à small airway diameter decreases and closing volumes are increased
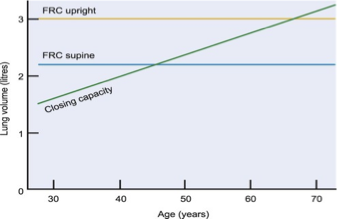
•Closing Volume is the lung volume towards the end of a forced expiration.
•Closing Capacity is the lung volume at which small airway closure in the dependent lung begins
•CC= CV + RV
•Closing volume (CV) > FRC at age 65 in sitting position
• Pa O2 declines d/t premature closing of small airways &
•decrease in alveolar surface area
•CC > FRC at age 45 in supine position
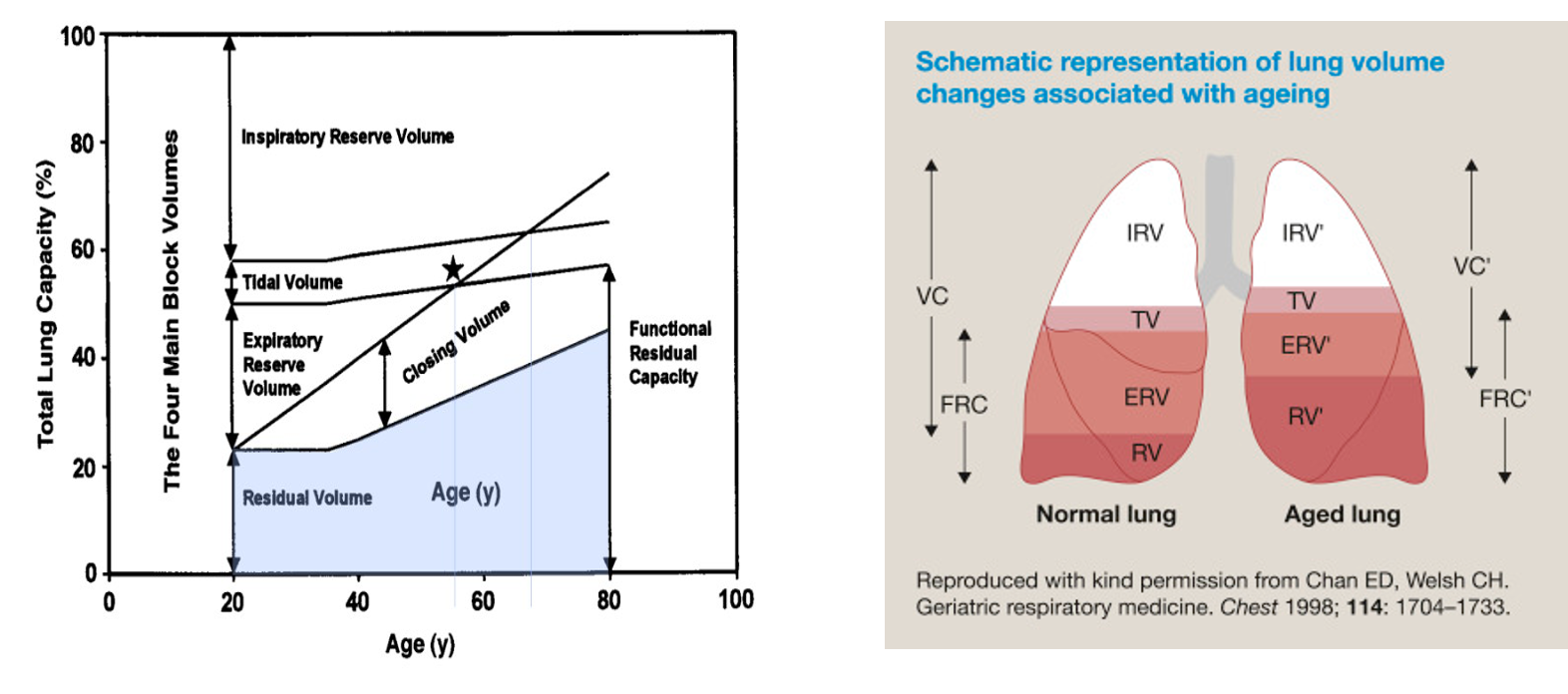
Lung volume changes
Lung changes INCREASED
•Stimulation needed for vocal cord closure & epiglottis function
•Airway obstruction: decreases sensitivity to clear secretions and food—> decreases laryngeal reflexes
•Risk of aspiration: ability to cough is decreased
•Pulmonary complications: aspiration pneumonia
•Physiological dead space: alveolar septae are broken downà decrease in total alveolar areaà increased anatomic and physiologic dead space= increases shunting and dead spacing
•WOB: skeletal calcification & increased airway resistance (may be harder to extubate post op)
•Hypoxia: ↓ elasticity of lung tissueà decreased efficiency of air exchange
•30% of alveolar wall tissue is lost—> decreased elastic recoil & parenchymal traction, which maintains airway patency—> increased RV, CV & FRC
•Closing vol & closing capacity: airway collapse & distribution of TV to area of lung less perfused à decreased PaO2
•Alveolar compliance: loss of connective tissue
•Respiratory depression w/opioids
Lung changes DECREASED
•Elastin fibers
•Tissue elasticity: muscle replaced with adipose & less-elastic components
•Lung recoil: chest wall is less compliant; lung cannot fully expand or recoil
•Ability to cough
•Chest wall compliance: cartilage and connective tissue are stiff, kyphosis, ribs & sternum are moving upward & more anterior
•VC, ERV, IRV: due to increases in residual lung volumes
•Alveolar surface area
•Response to hypoxia & hypercapnia
•Protective reflexes of airway are blunted
•Cervical spine & TMJ mobility: challenging airways
•Ease of mask ventilation: often edentulous
Changes in oxygenation DECREASED
•VC, IRV & ERV
FVC and FEV1 decline RT airway collapse
Changes in oxygenation INCREASED
•FRC, RV, CV & CC
•CLOSING VOLUME = volume in lung at end forced expiration
•CLOSING CAPACITY = volume in lung when airway closure begins
EXAM RV
IS MUCH MORE INCREASED
Airway and protective reflex changes- peiriop
periop resp complication
airway obstruction risk
Reduced laryngeal and pharyngeal support/tone
Increased riks of resp failure
CPAP postop for at risk patients
Aspiration risk
Decreased coughing and swallowing reflexes
Postop pulm complications risk factors
age
smoking
chronic lung disease
fraility
type/ druation of srugery
anesthesi amethod
pain control
Strategies to reduce postop pulm complications
Smoking cessation 8 weeks preop
inspiratory muscle training and IS
medical optimization of COPD and asthma
Anesthetic implications pulmonary
Reduced respiratory reserve
minimize opioids to reduce resp depression risk
Optimize ventilation strategies to prevent atelectasis and hypoxia
PEEP/ recruitment manuevers but careful with barotrauma
Renal function structural changes
•Progressive atrophy of kidney parenchymal (functional) tissues
•Deterioration of renal vascular structures
•Decreased RBF by 25-50%
•Decrease in renal mass
Renal functional changes
•Decrease in GFR —>decreased drug clearance, impairment of diluting portion of the nephron l/t fluid overload
•Renin, ADH & Aldosterone response is decreased—> impaired sodium concentration
•May develop hyperkalemia or hypokalemia
•H+ ion excretion & Na+ concentration are decreased &à impaired ability to respond to changes in electrolyte concentrations, intravascular volume & free water
•Kidneys do not respond to nonrenal loss of H2O & Na+ → dehydration
Renal function labs
•Serum creatinine=unchanged (if the kidney is functioning) because of decreased creatinine production from declining skeletal mass.
•Creatinine clearance is the best indicator of drug clearance
Renal fluid and electrolyte imbalances
•Elderly patient w/renal impairment is at increased risk for
Fluid overload due to impaired nephron functioon
Electrolyte imbalances→ cardiac arrhythmias(K+)
Dehydration risk= decreases response to Na and water loss
Renal drug metabolism
Accumulation of metabolites & drugs that are normally excreted by kidney
Decreased drug elimination → prolongs effects of anesthetic drugs
increases risk of toxicity
Renal anesthetic implications
monitor fluid balance to prevent overload
adjust anesthetic dose based on renal clearance
monitor electrolytes closely to prevent arrhythmias
consider alternative meds with lower renal clearance (Cistracurium)
Hepatic function structural changes
•Decreased blood flow to the liver RT decrease in mass by 20-40%
functional hepatic reserve declines
Hepatic functional changes
Decreased protein binding (decreased albumin, decreased plasma cholinesterase)
•Decreased drug metabolism (phase 1 and 2) & prolonged half-life of drugs
•Function is usually well preserved in the healthy older adult
•Coexisting diseases (hepatitis, drug induced liver injury, cirrhosis) & lifestyle habits (smoking, ETOH, poor nutrition) affect liver function more than the physiologic aging liver
Hepatic function phases of drug metabolism
Phase 1:
oxidation, reduction and hydrolysis: primarily mediated by cytochrome P450
Declines in phase 1 metabolism with age
Phase 2:
conjugation reactions, sulfonic acid and acetylation
drug metabolism is not affected by age
Anesthetic implications- hepatic
assess liver function pre op
adjustment hepatic metabolized drugs
monitor AE in elderly pts
Hepatic function labs
•Serum albumin decreases
Binds acidic drugs (benzos & opioids)
•Alpha 1- acid glycoprotein (AAG) is increased
Binds basic drugs (local anesthetics)
•May have adverse effects if person is malnourished
Pancreas
•Decline in number & function of islet beta cells →decreased insulin secretion
•Insulin resistance occurs peripherally l/t increased hepatic production of glucose & impaired breakdown fats & proteins
•Impaired breakdown of fats & proteins make the elderly glucose intolerant or diabetic → may play a role in brain aging (impaired cognition & Alzheimer’s disease
•Diabetes is a major risk factor for CV disease → increases risk of stroke, MI, ketoacidosis and infection
•As a CRNA, know the type of diabetes, diabetes control (Hgb A1c),length of disease and complications of the disease
Body composition
•Decreased BMR d/t decreased physical activity, decreased testosterone & growth hormone levels
•Decreased Skeletal muscle mass & strength (50% of skeletal mass by age 80) → decrease in functional decline & independence
•Significant loss body protein & carrier proteins (albumin & AAG)
•Body fat increases; distributes more in the viscera, subQ abdomen, intramuscular and intrahepatic areas
TBW
•Decreased dermal & epidermal skin thickness d/t loss of collagen and elastin
•Decrease in total body water
•BV decreases by 20-30% by age 75 → hypotension/ difficulty compensating for positional changes
this is importance because is affects drug distribution and metabolism
increased fat storage if fat soluble drugs
reduced water volume effects of water soluble drugs
Thermoregulation
•Impaired due to decreased hypothalamus function
increased risk of hypothermia
reduced peripheral vasoconstriction
•IA inhibit the temperature regulating centers in the hypothalamus
•Hypothermia is more pronounced and lasts longer
•Lower BMR, high SBA mass & less effective peripheral vasoconstriction in response to cold
Effects of hypothermia 4
•Hypothermia slows anesthesia elimination—> longer recovery
•Impairs coagulation & immune function
•Blunts the ventilatory response to CO2
•Shivering increases O2 consumption by 400% l/t hypoxia, acidosis & increased cardiac demand
Prevent heat loss 4
thermal mattress
forced air warmer
cover pts with blanket
maintain environment temp
warm devices for fluids or blood
CNS
•Progressive loss of neurons, decrease in neurotransmitter activity & decreased brain volume (most prominent in the cerebral cortex in the frontal lobe)
Decreased CSF
•Decreased nerve conduction velocity
•Decreased number of myelinated nerve fibers
•GA affects brain function, neuronal membranes, receptors, neurotransmitters, cerebral blood flow & metabolism
•BIS monitor to guide depth of anesthesia
•This results in changes in mood, memory & muscle function
CNS Drug sensitively
increased drug sensitivy due to receptor downregulation
More permeable BBB which also contributes to increased sensitivity to medications
•Elderly experience an exaggerated response to CNS depressant drugs such as GA, hypnotics, opioids and benzos
most frequent neuro complication RT anesthetic
most common is post op delirium or cognitive dysfunction
prevent post op delierum
•Pre-existing dementia or Alzheimer’s
•Avoid benzos and decrease induction drugs by 50%
decrease lenght of surgery
Neuraxial aneshtesia
•Decreased intervertebral disc height
•Narrowing of the intervertebral foramina & subarachnoid space
•Decreased space between the spinous processes, calcifications & lordosis result in difficulties with spinal & epidural placement
•The dura may be more permeable to LA’s → more advanced spread of LA
•Impaired baroreceptor response l/t severe hypotension, which may not respond to adrenergic stimulation (neo/ epehdrine)(↓ end organ response)
•Test dose of epi in your epidural may be less reliable.
•Decrease the dose you use in spinals & epidurals
Nervous sytem INCREASED
•CSF’s specific gravity
•Cerebral cortex neuron loss
•SAB duration of action
•Sensory block with SAB
•Epidural volume and cephalad spread
Nervous System DECREASED 6
•CBF
•Gray matter
•Nerve conduction
•LA & GA dosage
•Epidural DOA
•CSF volume
Post op delirium
•Cognitive ability should be assessed prior to surgery (baseline)
•Most frequently occurring neurological complication
•Postop cognitive dysfunction results in memory deficits, difficulty concentrating, impaired comprehension, changes in motor function
•Goal is to prevent, maintain oxygenation, and CPP
•Versed only if highly agitated or harm to themselves or others
8 Risk factors for post op delirium
•Lower educational level
•High ETOH intake or abuse
•Age >65 years
•Preexisting mild cognitive impairment
•High ASA status
•CVA history
•Longer surgery & anesthesia
•Interop cerebral hypoperfusion
Periop goals
•Maintenance of independence post operatively
•Speedy recovery
•Avoidance of functional decline
PharmacoKINETIC Changes – Changes to the drug
Volume of Distribution (Vd)
Increased Vd for lipophilic drugs
Benzodiazepines, propofol
Decreased Vd for hydrophilic drugs
NDMR
Metabolism Changes
Hepatic: (Ph 1) decreased, Ph 2 preserved
Decreased blood flow affects clearance
Excretion Changes
Renal: Decreased GFR, blood flow, tubular function prolong half-life (opioids)
PharmacoDYNAMIC Changes – effect on the body 3
Altered receptor sensitivity and signal transduction
Increased sensitivity to CNS depressants
Decreased responsiveness to Beta-adrenergic agonists and antagonists
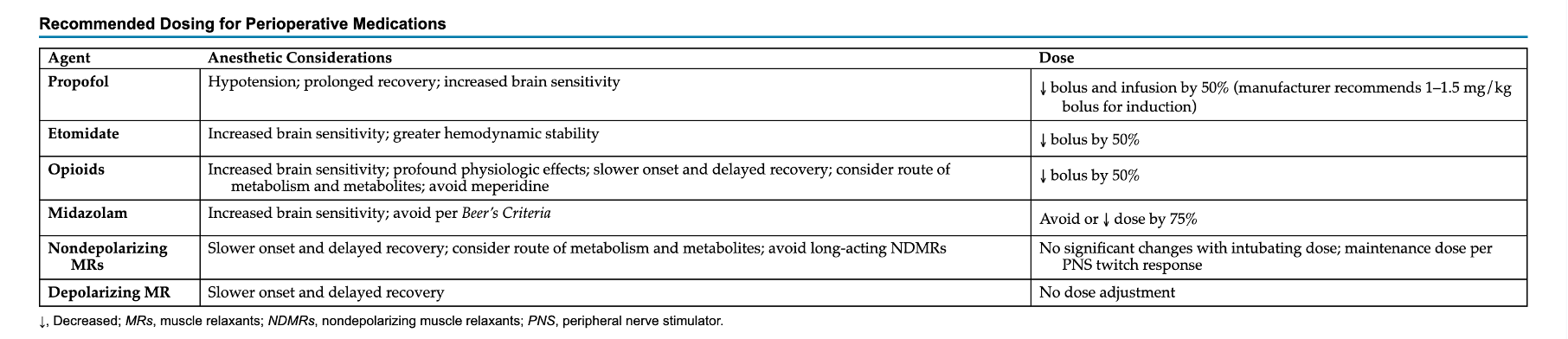
Anesthesia drug implications 5
Increased sensitivity to IV anesthesia (start low, titrate slow)
Prolonged neuromuscular blockade
Higher risk of postoperative delirium (POD) and cognitive dysfunction (POCD)
Individualized drug dosing
Close monitoring (BIS) - short acting, titratable agents
Might not need full MAC of gas
Valley 13- Geriatrics
Physiological changes occurs in geriatric pt
A. Decreased lung compliance
B. decreased chest wall compliance
C. decreased RV
D. Decreased CC
B. decreased chest wall compliance
Geriatric CV changes occur EXCEPT
A. elevated afterload
B. LVH
C. elevated SBP
D. increased arterial elastiticy
D. increased arterial elastiticy
As renal function declines, all decrease EXCEPT
A. BUN
B. Crt production
C. Ability to excrete drugs
D. ability to handle diurectics
A. BUN
Principle pharmacodynamic change A/W aging is
A. arthritis
B. pulmonary changes
C. Lipid solubility
D. reduced anesthetic requirements
D. reduced anesthetic requirements
onset in elderly determined mainly by
A. alveolar ventilation
B. lipid solubility
C. increased circ time
D. decreased circ time
C. increased circ time
age men have prolong effect with anectine but aged women don’t. why
A. lipid solubility
B. water solubility
C. lower plasma cholinesterase concentration
D. fewer motor end plates
C. lower plasma cholinesterase concentration
Mac appropriate for 65 yr old person receiving DES
A. 10
B. 9
C. 8
D. 4
D. 4
which joint is most vulnerable in position
A. hip/leg
B. knee
C. arms/ brachial plexus
D. neck
D. neck
onset of MR is prolonged RT
A. increased CO
B. low muscle blood flow
C. decreased kidney clearance
D. decreased hepatic function
B. low muscle blood flow
10 What drug would have prolonged actin in geriatrics
A. fat soluble drugs
B. water soluble drugs
C. both fat and water soluble drugs
D. no difference
A. fat soluble drugs
All increase pulmonary complications in elderly undergoing surgery EXCEPT
A. type of surgery
B. duration of surgery
C. fat content (obesity)
D. age >70 yrs
A. type of surgery
12 short term increase in CO in elderly is due to all EXCEPT
A. increased HR
B. increased LVEDV
C. larger SV
D. decreased preload
D. decreased preload
13 What best describes des in elderly pt
A. uptake is slower
B. build up first in brain
C. works slower due to bradycarida
D. very blood soluble
B. build up first in brain