M3-UPPER EXTREMITIES
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
19 Terms
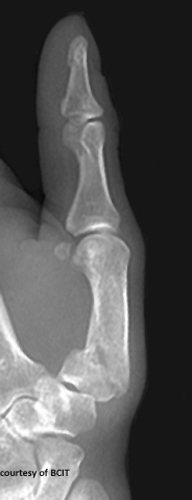
BASEBALL/MALLET FINGER
DESC: a dorsal intra-articular avulsion fracture at the base of the distal phalanx. The injured fingers look deformed and have soft tissue swelling associated with them
ETI: The mechanism of injury (MOI) is a forcible flexion of an extended finger.
TREAT: Most injuries of this type can be treated non-surgically, with a splint to immobilize the fracture.
COMP: Deformity of the bone if not treated. Decreased range of movement of the finger.

BOXER’S FRACTURE
DESC: fracture that occurs at the neck of the 5th metacarpal, sometimes the 4th metacarpal is affected.
ETI: The mechanism of injury (MOI) is an impact with a closed fist.
TREAT: Surgical interventions with “K-wires” are common. Depending on the fracture, immobilization with a cast can be used.
COMP: Bone deformity resulting in a rotational deformity of the phalanx.

BENNETT’S FRACTURE
DESC: oblique intra-articular fracture of the base of the first metacarpal.
ETI: The mechanism of injury (MOI) can be a direct impact along the long axis and hyperextension or abduction of the thumb or axial force applied directly to the metacarpal as in a fist fight.
TREAT: Reduction and fixation. Pins or K-wires are usually used.
COMP: Decreased range of motion of the joint with pain and early onset of arthritis.
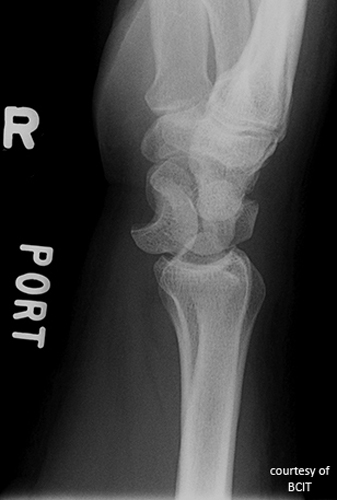
LUNATE DISLOCATION
DESC: loss of articulation with both the capitate and the radius, a spilled "teacup" effect
ETI: The mechanism of injury for lunate dislocations is forceful dorsiflexion of the wrist, for example on a FOOSH.
TREAT: Reduction and immobilization is required. Surgical intervention is often needed to stabilize the carpal bones to promote healing.
COMP: Arthritis and instability of the wrist
SCAPHOID FRACTURE
DESC: Swelling and tenderness are common to the ‘snuff box’ area (base of the first metacarpal). It is the most common carpal bone to fracture
ETI: The mechanism of injury is a FOOSH (Fall On Out-Stretched Hand) or a direct blow to the area.
TREAT: treated by immobilizing wrist area with a cast
COMP: can take up to 2 years to heal. If not identified early, avascular necrosis

COLLE’S FRACTURE
DESC: This type of fracture of the distal radius is within 3-5 cm from the wrist joint with dorsal displacement of the distal fragment
ETI: The mechanism of injury is a FOOSH (Fall On Out Stretched Hand) with the wrist hyperextended, or in dorsiflexion.
TREAT: Reduction (putting it back into correct alignment and apposition) and immobilization is required
COMP: Complex regional pain syndrome, deformity of the bone with loss of range of motion, weak grip, or nerve compression.

SMITH’S FRACTURE
DESC: The distal radial fragment is displaced anteriorly.
ETI: The mechanism of injury is a force applied to the posterior aspect of the wrist that causes palmar (anterior) displacement of the distal fragment.
TREAT: Reduction and immobilization of the fracture.
COMP: A weak grip, ongoing pain, deformity of bone and resulting reduction in the range of motion

GALEAZZI FRACTURE
DESC: type of fracture dislocation. It involves a fracture of the distal one third (or middle third) of the radius along with a dislocation or subluxation of the radioulnar joint.
ETI: Blunt trauma to the arm usually by falling on an outstretched hand with the forearm in pronation
TREAT: Surgical fixation with reduction of fracture and stabilization of radioulnar joint.
COMP: There is an increased risk of compartment syndrome with severe fractures. Nonunion or malunion are also possible complications

MONTEGGIA FRACTURE
DESC: fracture of the ulnar shaft with anterior dislocation of the radial head.
ETI: The mechanism of injury is a fall on outstretched hand with the forearm in pronation.
TREAT: Reduction and immobilization.
COMP: Deformity and angulation of the bone. Non-union of the ulnar shaft. Radioulnar synostosis. Compartment syndrome.

RADIAL HEAD FRACTURE
DESC: difficult to diagnose. Patients usually have pain and swelling at the injury site.
ETI: The mechanism of injury is a Fall On Outstretched Hand
TREAT: Simple fractures are usually splinted or casted. Surgical interventions may be required for severe cases.
COMP: Stiffness and loss of mobility of the joint. Early intervention for range of motion (ROM) is encouraged to avoid these symptoms.

OLECRANON FRACTURE
DESC: the triceps muscle separates the fragment from the ulna
ETI: The mechanism of injury is a fall onto a moderately flexed elbow.
TREAT: Surgical intervention is often required.
COMP: Ongoing pain and loss of full extension of the elbow. Non-union of fragments.

ELBOW DISLOCATION
DESC: usually rupture the capsule and ligaments surrounding the elbow. Associated fractures with posterior elbow dislocations most often involve the coronoid process of the ulna
ETI: The mechanism of injury is a fall onto an extended elbow
TREAT: Reduction and immobilization for 10-14 days. Surgical intervention is necessary for dislocations with associated fractures of the elbow
COMP: Decreased range of motion of the elbow joint. The possibility of recurrent dislocations due to weakened ligaments.

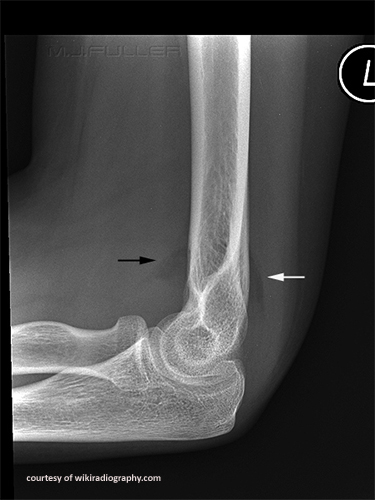
ELBOW JOINT FRACTURE
DESC: The fat pad around a normal elbow joint is not visible. Any trauma to the elbow joint results in a joint effusion which displaces the fat pad.
ETI: The mechanism of the injury is a trauma to the elbow joint.
TREAT: Fracture has to be stabilized.
COMP: all the complications of a fracture can occur.
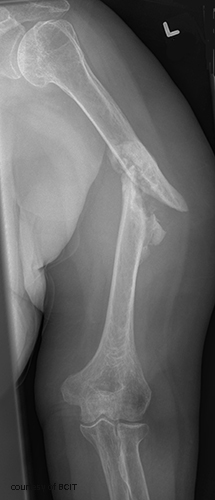
HUMERUS FRACTURE
DESC: There is a high incidence of metastatic involvement leading to pathological fractures
ETI: The mechanism of injury usually is a trauma to the bone by falling or a direct impact as in a motor vehicle accident
TREAT: Reduction and immobilization of the fracture. Surgical intervention may be necessary to stabilize the fragments.
COMP: Deformity
PROXIMAL HUMERUS FRACTURE
DESC: prone to avulsion fractures due to the numerous ligaments and muscles attached to the humeral head
ETI: In the under-twenty age group, epiphyseal separations are the most common injury. In the over-twenty age group, fractures are caused by severe trauma. For those sixty years of age and older, injuries are often due to the presence of osteoporosis.
TREAT: Reduction and immobilization. Surgical intervention may be required if the fracture is severe.
COMP: Arthritis. Recurrent dislocations.
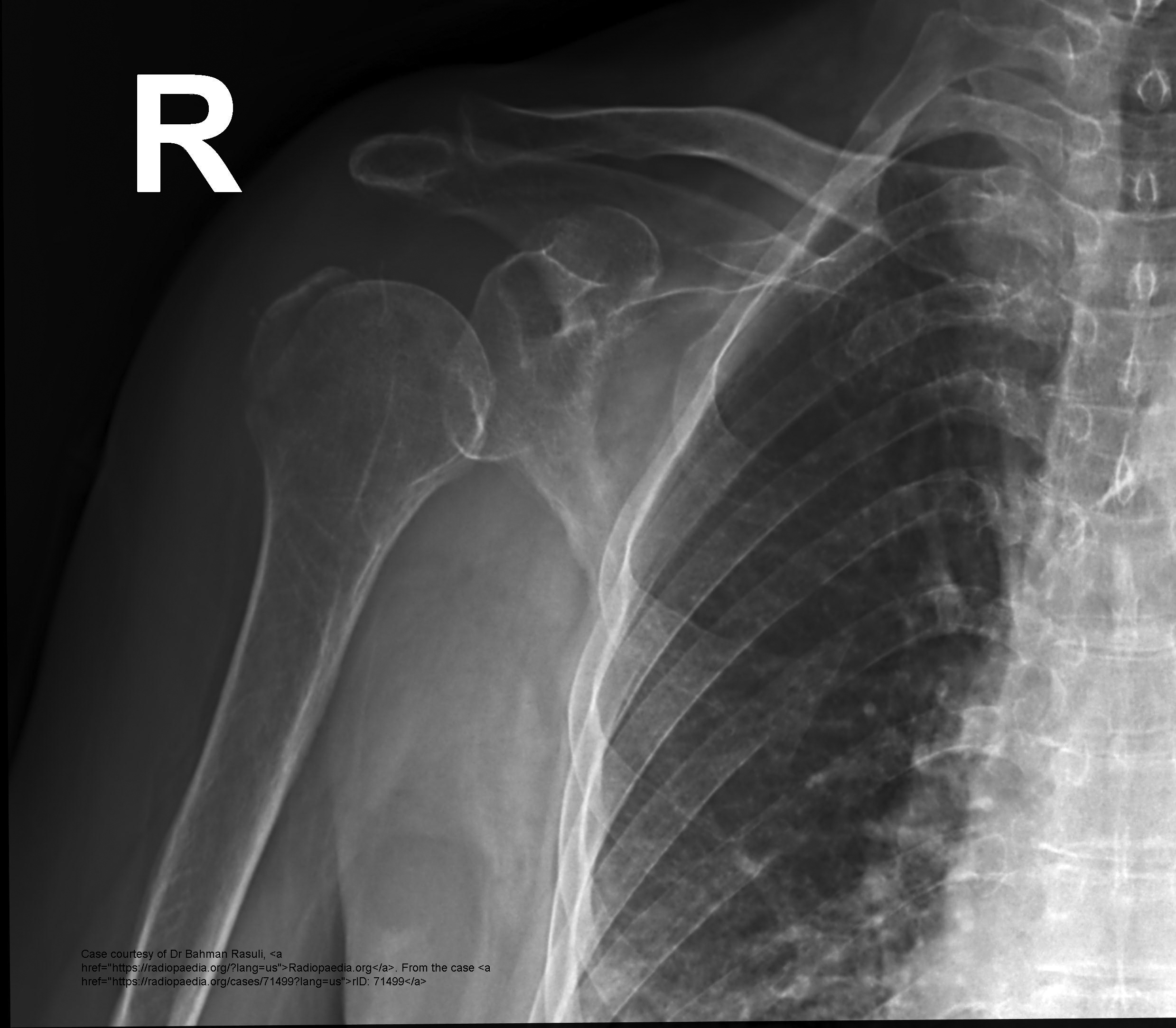
ANTERIOR SHOULDER DISLOCATIONS
DESC: one where the humeral head lies anteriorly to the scapula.
ETI: he mechanism of injury is a force that is applied to the arm when there is an external arm rotation and abduction.
TREAT: Reduction of the injured shoulder.
COMP: Hill Sachs lesion. This lesion occurs when the humeral head sustains a fracture during an anterior dislocation

POSTERIOR SHOULDER DISLOCATION
DESC: rare because of the structure of the shoulder.
ETI: The mechanism of injury is an axial loading of an extended arm with internal rotation.
TREAT: Reduction of the dislocation
COMP: Recurrent posterior subluxation. Hill Sach's lesions.

ACROMIOCLAVICULAR JOINT
DESC: has a complex soft tissue support system. The normal joint space is 3 to 7 mm
ETI: The mechanism of injury usually is a trauma such as a fall onto the shoulder
TREAT: Immobilization of the shoulder with a sling. Surgical intervention may be required for more severe injuries.
COMP: Degenerative changes and arthritis to joint. Ongoing pain with decreased range of movement.

CLAVICLE FRACTURE
DESC: the sternocleidomastoid muscle retracts the medial fragment in a superior direction while the weight of the upper limb pulls the distal fragment in a downward direction
ETI: The mechanism of injury in most cases is a FOOSH.
TREAT: Reduction and immobilization is difficult to maintain due to the pull of the sternocleidomastoid muscles.
COMP: Some malunion is common in clavicular fractures. Healing occurs rapidly.
