Localization of function
1/11
Earn XP
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
12 Terms
What is localisation of function
Localization of function refers to the idea that specific functions or processes in the brain are associated with particular regions or areas. This concept is essential in understanding how different parts of the brain contribute to various cognitive and physical abilities.
What are different types of localisation?
Strict Localization, which means that a specific region of the brain controls a specific function.
Weak Localization, which means that a function is dominantly controlled by a brain area, but other areas contribute.
Holistic Processing, which means that the brain has distributed functions across multiple areas.
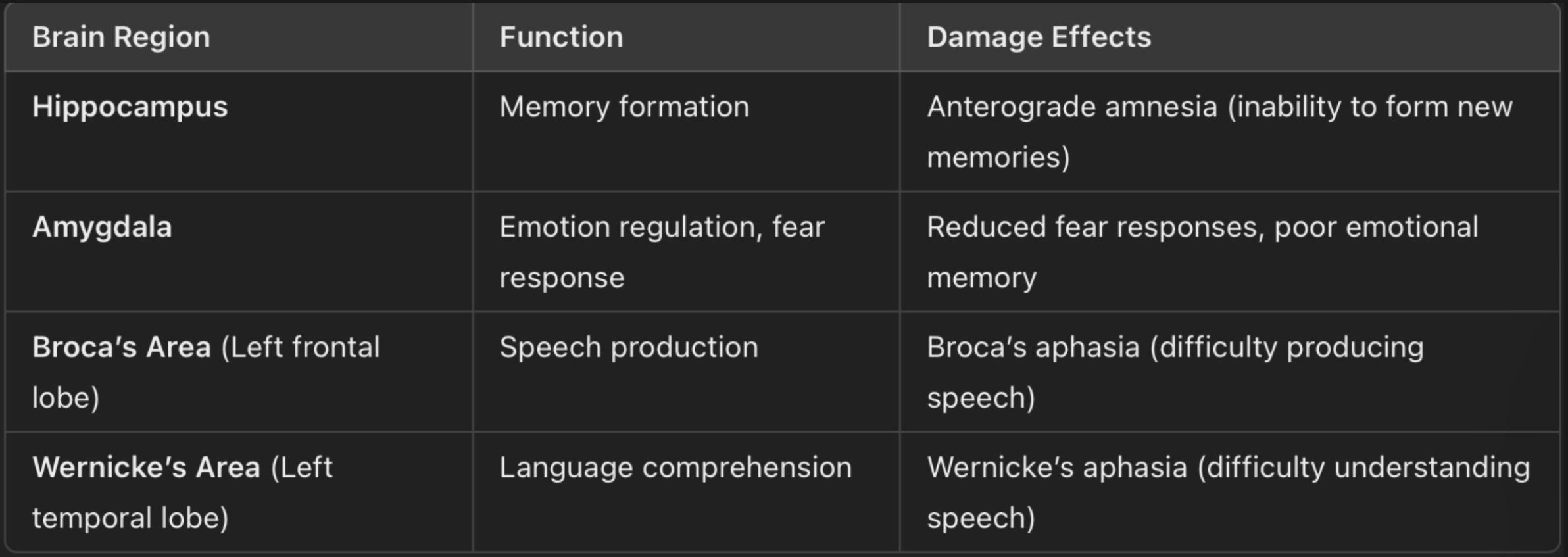
What are key brain areas and their functions?
What studies support Localisation
Maguire et al (2000)
HM (Milner, 1966)
What are the strengths of Localisation?
supported by empirical evidence.
Studies on brain-damaged patients (HM) show a clear link between brain areas and functions.
MRI and fMRI studies (Maguire) confirm brain activity is often concentrated in specific regions.
Understanding localization helps with surgical interventions and stroke rehabilitation.
What are the limitations of Localisation?
Neuroplasticity challenges strict localization.
If localization were absolute, brain damage would result in permanent loss of function. However ,recovery is often possible.
Some functions are more distributed, as memory is not strictly localized.
Hemispheric specialization is not absolute, for example language functions are not exclusive to the left hemisphere (e.g., right hemisphere contributes to tone and emotion in speech)
Tell me about the study of Maguire et al.
When: 2000
Aim: to see whether the brains of London taxi drivers would somehow be different as a result of their knowledge of te city and the many hours that they spend behind the wheel.
Sample: 16 male taxi drivers
Condition: take a “”Knowledge” test and to have their license for more than 1,5 years.
Procedure: they did an MRI scan and the researchers compared it to the MRI of 50 male non taxi drivers, which was taken out of an MRI data base. The data from the MRI was measured using two methods.
VBM (Voxel-based Morphometry) → measure the density of grey matter.
Pixel counting → to calculate the area of the hippocampus.
Results:
Pixel counting revealed that the posterior hippocampi of taxi drivers were significantly larger relative to the control subjects, and the right posterior hippocampi were significantly smaller.
VBM showed that the size of the right posterior hippocampi correlated with the years being a taxi driver.
Conclusion: this demonstrates that the hippocampus may change in response to environmental stimuli.
How do you link this study to the theory?
Extensive navigation experience in London taxi drivers is associated with increased grey matter in the hippocampus, highlighting its role in spatial memory and navigation.
Tell me about the study of HM.
Date: 1966
Aim: to understand the effects of the removal of the hippocampus and the medial temporal lobe on memory foundation.
Sample: 1 participant
HM (Henry Molaison), a male patient who underwent surgery to treat severe epilepsy.
Background:
Suffered a head injury at age 7, leading to severe epilepsy by age 10.
Age 27 → underwent experimental surgery, where they removed parts of the medial temporal lobe, including the hippocampus, on both sides of his brain.
Post-surgery → he suffered from anterograde amnesia (inability to form long term memories)
Procedure: milner conducted a longitudinal case study using method triangulation, including:
Psychometric testing
Direct observation (HM’s behaviour was monitored daily)
Interviews (with HM and his family)
Cognitive testing
Memory recall tests (HM struggled with recalling new information)
Learning tasks
MRI scans (to determine the extent of brain damage.
Results:
Severe anterograde amnesia → he could not form new episodic (event0based) or semantic (general knowledge) memories.
Intact short-term memory → could hold information briefly through rehearsal
Intact procedural memory → learned new motor skills (mirror drawing task), but had no recollection of learning them.
Spatial memory → could form a cognitive map of his new home.
MRI findings → damage was mainly in the hippocampus and the medial temporal lobe, areas responsible for memory consolidation.
Conclusion: the hippocampus is crucial for transferring short-term memory to long-term memory.
How do you link this study to the theory?
Memory is not stored in one specific brain area; rather, different types of memory rely on different brain structures, supporting the holistic processing of localization.
Evaluate Maguire et al.
Quasi experiment → no cause and effect relationship → unable to control IV
Single blind study (researcher did not know whether she was looking at the scan of a taxi driver or a control) → avoid researcher bias
Low ecological validity → MRI scans
Sampling bias → as the sample was only male taxi drivers → difficult to generalize
Sample size → only 16 participants → hard to generalize
Ethically sound → MRI does not cause harm and they all gave consent and had the right to withdraw.
Evaluate HM (Milner).
Longitudinal study → allow researchers to observe change over time
Method triangulation → increase the validity of the studies
High ecological validity → HM was observed in his natural environment
Ethically sound → confidentiality (his name was only used after his death), consent by him and his guardians, protection from harm.
Cannot be generalized → he had a unique brain damage.