3.1 Sexually transmitted bacterial diseases
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
STI
presence of a pathogen (bacteria, virus or parasite) in the body that has been transmitted through sexual contact - the person may be asymptomatic and unaware of the infection
STD
occurs when an STI progresses to cause symptoms, tissue damage or clinical manifestations - not all STIs become STDs, some are cleared by the IS or remain dormant
Divergent disease
when the same pathogen can lead to vastly different clinical consequences across different individuals
asymptomatic carrier
Some individuals harbour infections like Chlamydia trachomatis or Neisseria gonorrhoeae without symptoms, unknowingly transmitting to partners whilst remaining disease free
Localised vs systemic progression
untreated infections may remain localised (urethritis, cervicitis) or ascend to cause severe complications such as pelvic inflammatory disease (PID), leading to infertility, ectopic pregnancy or chronic pelvic pain
Immune response variation
Individual immune responses determine whether an infection is cleared, controlled or progresses to disease - immunocompromised individuals face higher risks of disseminated infection (into the bloodstream)
Co-infections and synergy
Presence of one STI increases susceptibility to others, including HIV, compounding disease severity and transmission risk
Chlamydia info
Bacterial, can be cured, fluid transmission
Gonorrhoea info
Bacterial, can be cured, fluid transmission
Syphilis info
Bacterial, can be cured, fluid and skin to skin transmission
Trichomoniasis info
Protozoa, can be cured, fluid transmission
HSV (Herpes) info
Viral, not curable, can be managed, fluid and skin to skin transmission
HPV (human papillomavirus) info
Viral, not curable, can be managed, fluid and skin to skin transmission
Factors contributing to rising STD cases
Increase substance use, decrease condom use, elevated rates in Native American reservation
chlamydia symptoms
Pain during sex and urination, green/yellow fluid discharge
Chlamydia trachomatis organism
Gram-negative-like (lacks peptidoglycan), obligate intracellular bacteria (lack several metabolic and biosynthetic pathways, depend on host cell for intermediates inc ATP), coccoid or rod shaped, non-motile, 2 forms: small infectious elementary bodies and larger replicating reticulate bodies
Chlamydia habitat/survival
Humans only, genital tract, cervix, urethra. Cannot survive outside host. Oral, vaginal or anal sex, mother → newborn in vaginal birth. No environmental reservoir
Chlamydia epidemiology
Trachoma - worldwide esp in Africa/Asia, inoculated into the eye by contaminated fingers or fomites or through vaginal birth. Genital infections - sexual contact. Respiratory infections - inhalation of infected droplets
Chlamydia genital infection in men
Commonly urethritis, incubation = 7-21 days (more than the 2-5 days for gonorrhoea)
Chlamydia genital infection in women
Typically infects columnar epithelial cells of endocervix, discharge from cervix, urethral syndrome, can develop PID, infertility, ectopic pregnancy
What is PID?
serious infection on women’s reproductive organs, caused by STDs like chlamydia/gonorrhoea, 1/8 women with PID have difficulty getting pregnant
PID symptoms
Pain in lower abdomen, fever, unusual discharge, bad odour from vagina, pain/bleeding during sex, burning urination
PID treatment
if diagnosed early can be treated, cannot undo damage
Lymphogranuloma Venereum (LGV)
3-12 days after chlamydia infection, three stages: small genital blister or ulcer; painful swollen lymph node in the groin; sores heal but left scars.
Neonatal pneumonia
Subacute afebrile (non-fever) pneumonia occurring in infants 4-12 weeks, acquired from mother in vaginal delivery, staccato cough, non-toxic
neonatal pink eye
6-21 days foe chlamydial infection, swelling of infant’s eyelid, conjunctival scarring
Two forms of chlamydia needed for infection/disease
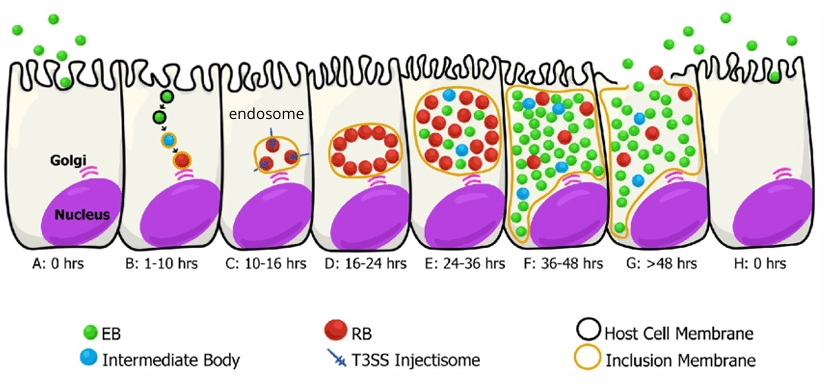
1- infectious, extracellular form - elementary body (EB), 2- non-infectious, metabolically active intracellular - reticulate body (RB)
Chlamydia EB virulence factors
Small and infectious, rigid outer membrane, bind sialic acid receptors on epithelial cells and phagocytes
Chlamydia RB virulence factors
Large replicating form, metabolic, binary fission within the inclusion, reorganises EBs for release/further infection
Chlamydia LPS virulence factors
Endotoxin in outer membrane, triggers inflammatory response, contributes to tissue damage in chronic infections
Chlamydia T3SS virulence factors
Delivers effector proteins into host cells, manipulates host cell signalling pathways, facilitates intracellular survival and replicaiton
Chlamydia SemC protein virulence factors
Secreted by the bacteria during entry, recruits host protein SNX9 to infection site, exploits host cell machinery for bacterial uptake
Chlamydia inclusion membrane virulence factors
Creates protected intracellular niche, prevents fusion with lysosomes, allows nutrient acquisition from HC
Chlamydia evasion of immune response virulence factors
Intracellular location protects from antibodies, inhibits apoptosis to prolong infection, modulates antigen presentation
Chlamydia infection cycle
Image
Neisseria gonorrhoeae overview
sexually transmitted disease most common in young adults, infects genital tract/mouth/anus via vaginal/oral/anal sex, can be passed during vaginal birth
Gonorrhoea organism
Gram negative, diplococci, non-motile, aerobic, nutritionally fastidious (req. blood/hemoglobin), pink/brown colonies, survives few seconds in environment
Gonorrhoea habitat
human only host (repro tract), not normal microflora, sites of exposure, cannot survive well outside eukaryotic host
Gonorrhoea source
contact: unprotected sex, eyes/mouth contact, vaginal birth
Gonorrhoea epidemiology
2nd most common STI amongst 20-30yrs, can occur at any age, 20% risk for men (hetero), 60-80% risk for women (hetero), vaginal birth causing eye infection, cannot be spread on surfaces, most infections are aymptomatic
Gonorrhoea clinical disease women
50% of cases asymptomatic, abdominal pain during sex, vaginal discharge/bleeding
Gonorrhoea clinical disease men
Mainly acute urethritis → infected kidneys, UTI, burning urination, inflammation, swollen testicles, discharge
Gonorrhoea Lipo-oligosaccharide virulence factors
Endotoxin in outer membrane, triggers inflammatory response, undergoes antigenic variation to evade IS
Gonorrhoea Type IV pili (T4P)
mediate attachment to epithelial cells, enable twitching motility, undergo antigenic and phase variation, protect against phagocytosis
Gonorrhoea por protein virulence factors
Channel protein, major outer membrane porin protein, facilitates nutrient stability, provides structural stability, may contribute to immune evasion
Gonorrhoea opacity-associated protein (Opa) virulence factors
Mediates adherence to/invasion of epithelial cells, binds to CD66 receptors on human cells, undergoes phase and antigenic variation, promotes uptake by neutrophils
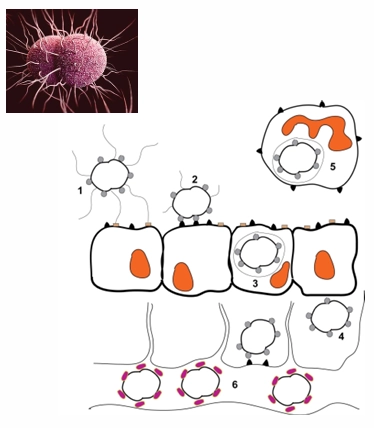
Neisseria gonorrhoeae infection
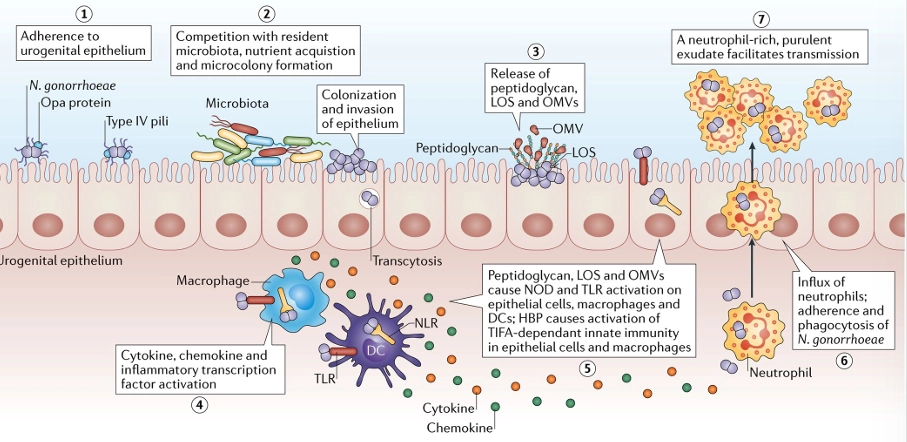
Gonorrhoea T4P + Opa infection
gonococci interact with the mucosal epithelium and neutrophils
pili retract allowing Opa-mediated attachment
after opa attachment, bacteria are engulfed and internalised into mucosal cells
Some cells can transcytose to the basolateral side of the mucosal epithelium
Opa offers immune evasion by multigene phase variation that results in antigenic variation
Following transcytosis, gonococci can enter the bloodstream where LOS renders the bacteria serum resistant
Gonorrhoea Major outer membrane porin (PorB)
As well as being an outer membrane pore, PorB also performs multiple functions contributing to pathogenesis: inducing/inhibiting apoptotic signalling in cells, serum resistance, epithelial cell invasion under low phosphate conditions, can affect generation of reactive oxygen species by innate immune cells
Virulence factors of gonorrhoea
LOS, T4P, Por/PorB, Opa
Treponema palladium (Syphilis) overview
difficult to detect at early stage, penicillin effective antibiotic, first symptom is a small, round sore (chancre), can develop anywhere on body but mainly affects anus/mouth/genitals. Painless sore but highly infectious
T. palladium organism
spirochaete, neither gram pos/neg, endoflagella for motility, obligate human pathogen, aetiological agent of venereal and congenital syphilis
T. palladium habitat/source
Oral cavity, intestines, rumen, genitals (animals/humans). Occurs primarily 15-40yrs, 1 million infants/year born congenital syphilis
syphilis epidemiology
via placenta, kissing, close contact with active lesion, blood transfusion, direct inoculation (clinical setting), sexual contact (vast majority)
Stage 1 syphilis
3-90 days after exposure, painless sore (chancre), anywhere on body, highly infectious, heals 3-6 weeks w/out treatment, bacteria remain in body and progress to stage 2 if not treated
Stage 2 syphilis
4-10 weeks after initial infection, body rash anywhere, common on palms and soles, may be fever, swollen lymph nodes, sore throat, fatigue, symptoms can come/go over several months, highly infectious
Stage 3 syphilis
Occurs if syphilis remains untreated, affects internal organs inc. heart, brain, blood vessels, liver, bones, joints, can cause serious complications like CV problems, neurosyphilis, gummatous lesions, blindness, dementia, death. Not contagious but damage irreversible
T. palladium endoflagella v factors
rotation produces cork-screw movement, hides antigens from host immune system, contained within periplasmic space
T. palladium outer membrane protein v factors
limited immunogenic surface proteins, helps evade immune detection
T. palladium hyaluronidase v factors
facilitates tissue penetration, aids in dissemination throughout the body
T. palladium adhesins v factors
enable attachment to host cells, facilitates colonisation of mucosal surfaces
start of infection - T. palladium
when it penetrates host usually through intact/abraded mucous membrane