14. Learning and Memory
1/33
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
34 Terms
What is Learning
change in behavior as a result of experience (or practice or study!)
– Can be acquisition of information, behavior pattern or ability
What is Memory?
ability to recall or recognize
based on previous experiences, implies
mental representation or memory trace
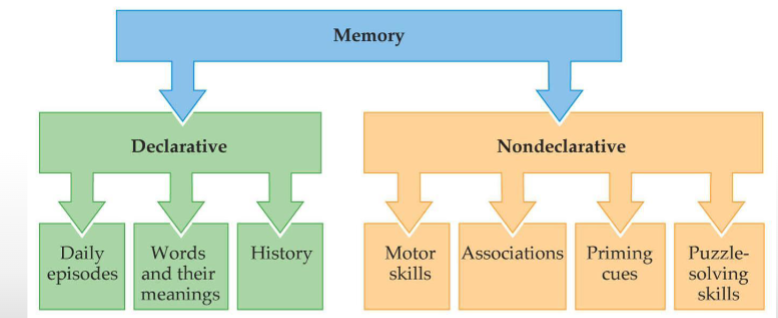
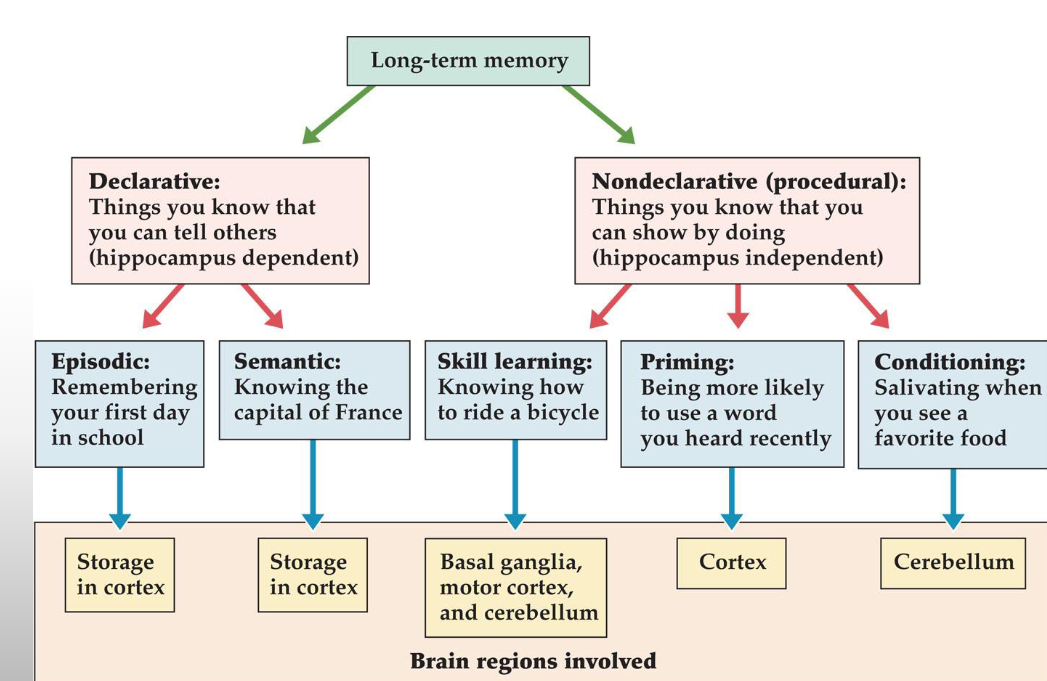
What are the two categories of memory and what do they encompass?
Declarative:
Things you know that you can tell others.
Non-declarative = procedural: Things you know that you can show by doing
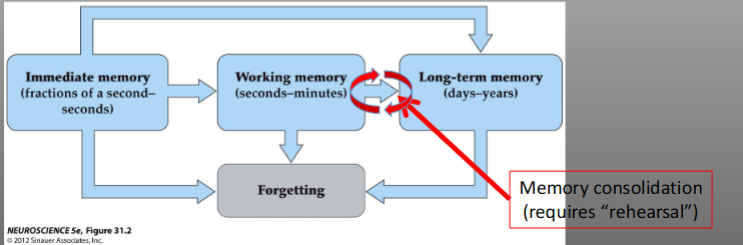
What are the temporal categories of memory?
Immediate memory - ability to hold ongoing experiences in mind for fractions of a second.
Working memory (short-term memory) - hold information in mind for seconds to minutes to achieve a goal, requires attention
Hunting for objects
Remembering a phone number until you can write it down
Long-term memory - retaining information for days, weeks, life
Retaining information of particular importance (for your exam)
Retaining salient (significant) events, skills etc
What is Amnesia?
partial or total loss of memory
– Retrograde: deficit in recalling previous information
– Anterograde: deficit in learning new information
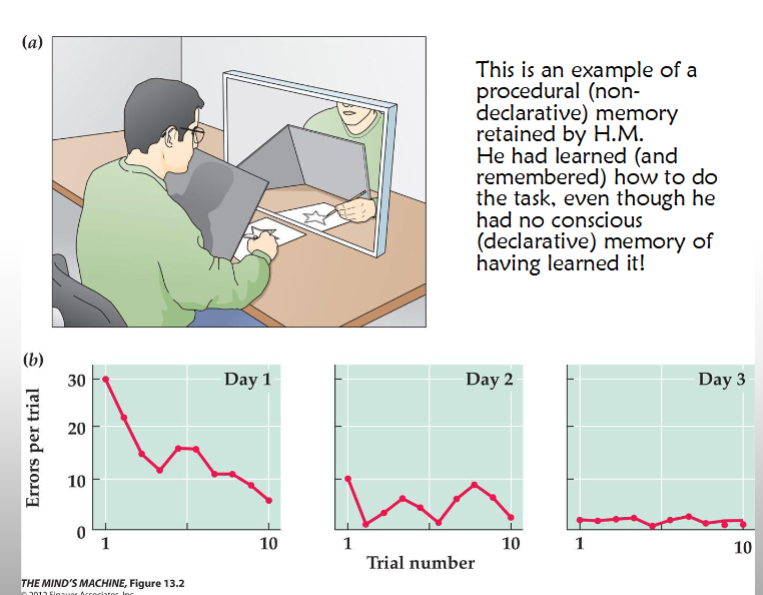
Explicit Memory Storage: Patient H.M.
• Bilateral temporal lobectomy at age 27 (1953)
• All of the ;hippocampus and some surrounding areas removed
• After: normal IQ, thinking, perception, reasoning, motivation
• Profound anterograde amnesia
• Was unaware of the surgery taking place, still reported the date as 1953, each day had to be reintroduced to doctors, etc.
• Older memories (from pre-surgery life) remained intact – so memory storage not
affected!
• Retained ability to form new implicit memories (procedural learning)
What is Korsakoff’s Syndrome?
• Caused by a thiamine (vitamin B1) deficiency due to prolonged intake of large quantities of alcohol
• Characterized by both retrograde and anterograde amnesia; however patients are generally indifferent to suggestions they have a memory problem
•Most patients show atrophy/decreased activity in the frontal lobe of the cerebral cortex (as well as parts of the thalamus and hypothalamus)
What are the two subtypes of declarative memory?
• Semantic memory—generalized declarative memory
• Episodic memory—detailed autobiographical memory
Patient K.C. cannot retrieve _____ memory due to
accidental damage to the ____
K.C.s _____ damage accounts for his ____
amnesia, but not for the loss of his ______ memory
Brain-imaging studies show that semantic and episodic
memories are processed and stored in _____ locations
Patient K.C. cannot retrieve personal memory due to
accidental damage to the cortex
K.C.s hippocampal damage accounts for his anterograde
amnesia, but not for the loss of his autobiographical
memory
Brain-imaging studies show that semantic and episodic
memories are processed and stored in different locations
Episodic memory: patient KC
• Traumatic brain injury resulting from a motorcycle accident
• Cognitive abilities normal, short-term memory intact
• Can recall facts about himself but has NO memory of any
events that included him: episodic amnesia
• Often associated with damage to the frontal lobe of the
cerebral cortex
Implicit Memory Storage: Patient J.K.
Suffered from Parkinson’s disease
• Dysfunction of the basal ganglia
• Demonstrated disruptions in motor tasks or types of memory that seemed implicit (things we do every day without thinking about them, like turning on a light switch)
• Perfectly intact episodic and declarative memory
• Thus, storage must be in different places!
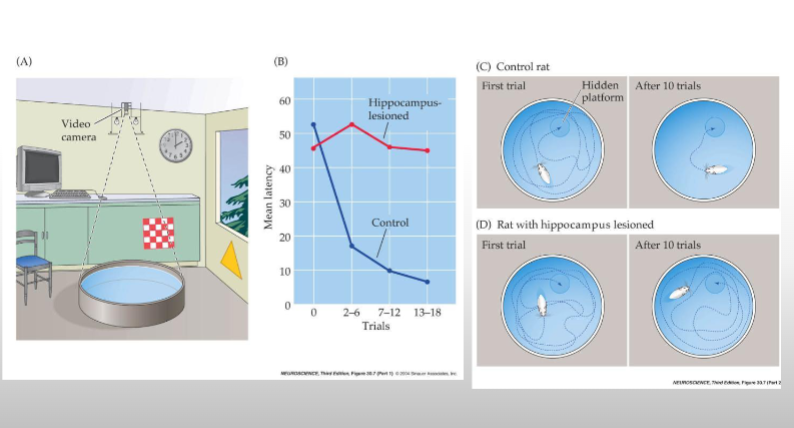
What are hippocampal place cells?
• Hippocampal neurons that increase firing rates when the mouse walks/runs
through a specific point in a previously learned maze
• Each new maze/circumstance leads to a new neural representation of space
• Spatial representations and sequences of activity are thought to be learned in
hippocampal circuits
• Involves synaptic strengthening at CA1-CA3 synapses

Hippocampus and spatial memory
Role of Synapses in Learning and Memory
Learning
– Relatively permanent change in behavior that results
from experience
– Mediated by structural changes in synapses
• Neuroplasticity
– The nervous system’s potential for neurophysical or
neurochemical change that enhances its adaptability to
environmental change and its ability to compensate for
injury
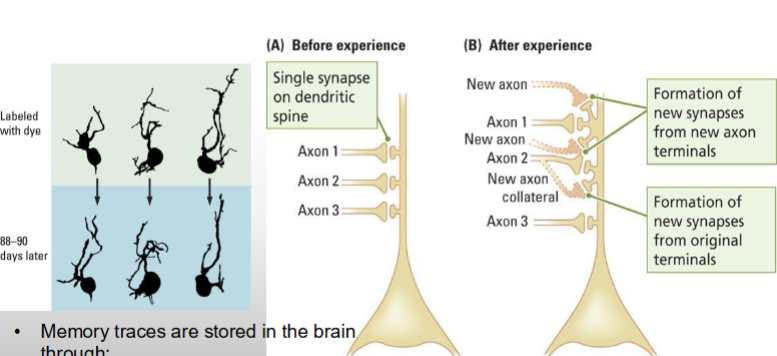
How are memories stored in the brain? Changes at the level of the neuron
Changes in existing circuitry
see pic
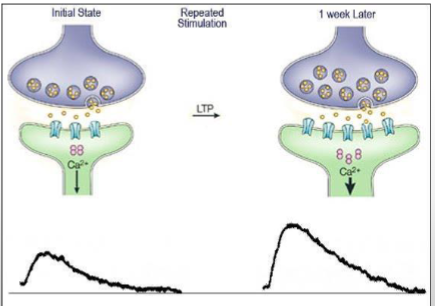
How are memories stored in the brain?
Changes at the level of the neuron
• Memory traces are stored in the brain through:
– Changes in structure or number of synapses
– Changes in synaptic strength: LTP
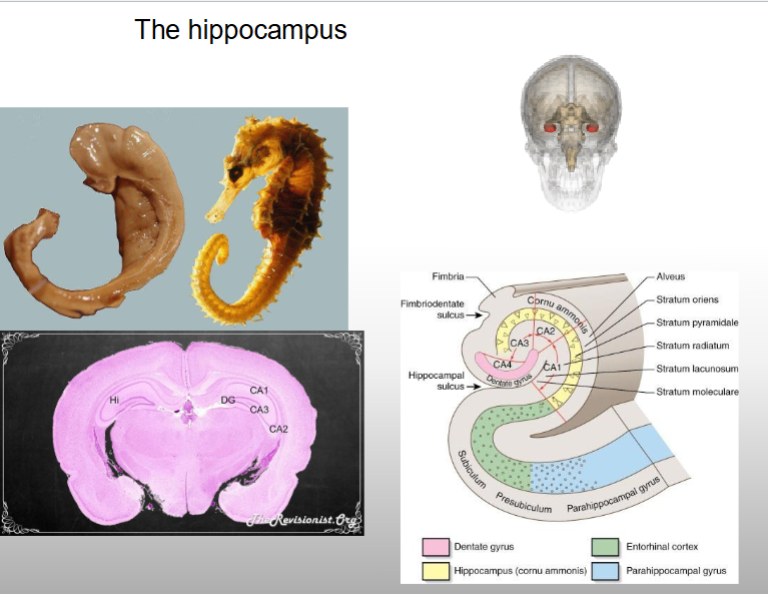
What is the hippocampus?
Region of brain involved with memory formation.
What is long term potentiation?
– Changes in synaptic
strength
– Long-lasting, activity-
dependent synaptic
enhancement (Bliss
and Lomo, 1973)
— Increased strength of connections over time
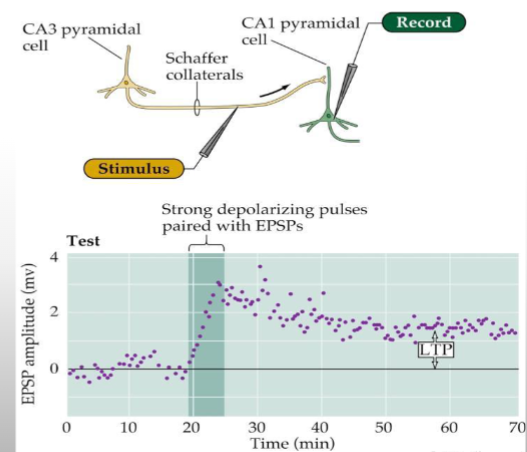
Explain hippocampal LTP
• Stimulate Schaffer collaterals, record CA1 neurons
– Low frequency pulse (1 Hz) evokes excitatory postsynaptic potentials (EPSPs)
– After high-frequency stimulation (>100 Hz), response is potentiated
• High-frequency stimulation induces 100-200% increase in EPSP amplitude that
persists
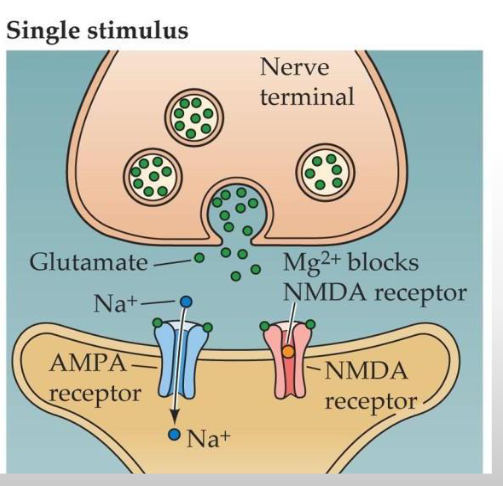
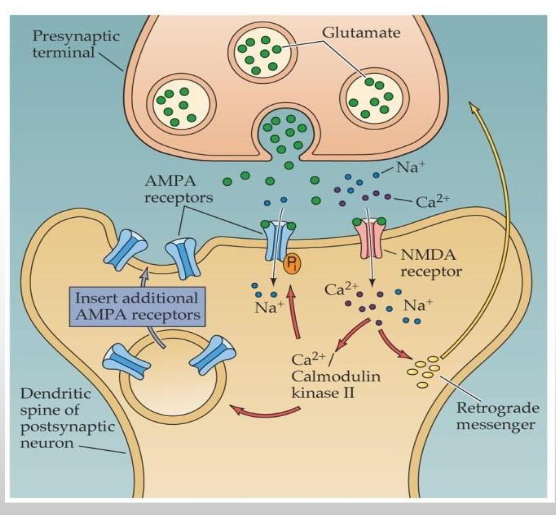
What us the mechanism behind LTP, for a single stimulus?
• Stimulation releases
glutamate into synaptic
cleft
• Binds with glutamate
receptors on CA1
dendrites
– AMPA → depolarizes
membrane through NA+
influx
– NMDA → normally
blocked (magnesium)
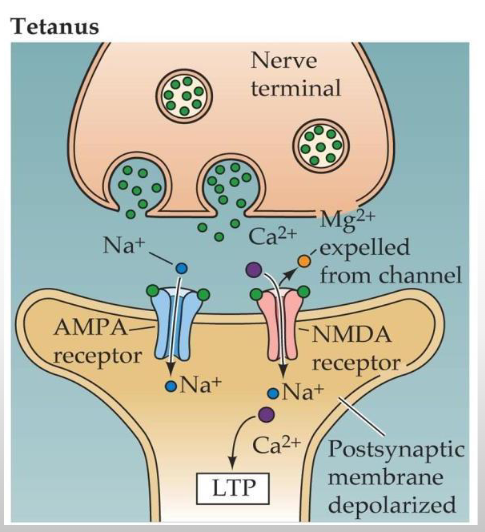
What us the mechanism behind LTP, for tetanus?
• Depolarization to -35 mV
results in magnesium
being expelled from
NMDA receptor
• Glutamate acting on
NMDA receptors opens
Na+/Ca2+ channel
• Ca2+ triggers cascade of
events resulting in LTP
After Glutamate opens Na+/Ca2+ channel, what happens in the post-synaptic dendritic spine?
• Ca2+ activates protein kinases (e.g., PKA, MAPK, CaMKII)
– synthesis of proteins and insertion of new AMPA receptors
Evidence for LTP as a memory mechanism
• Induced within seconds
• Long-lasting (days+)
• Labile consolidation period (sensitive to
disruption)
• Induced at physiological frequencies
• Correlates with maze learning
• Drugs that block learning block LTP
• Enriched environments promote learning and
LTP
What is Long-term depression? LTD
• Long-lasting reduction in synaptic efficacy
• Small increase in Ca2+ activates protein phosphatases
(dephosphorylate proteins)
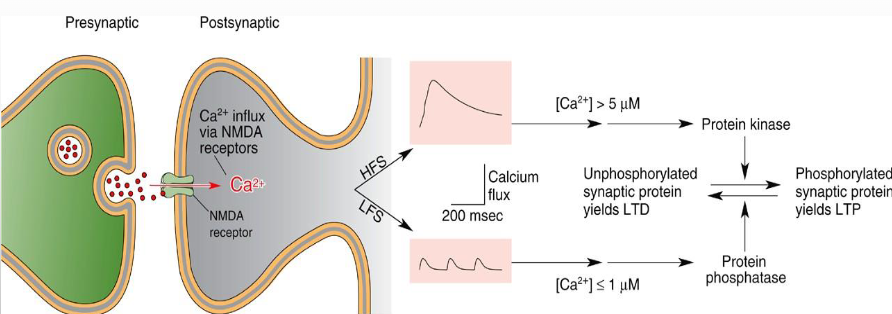
Relationship between LTP and LTD
• May be responsible for sculpting
nervous system to respond to
environment
• LTP strengthens synapses
critical for performance
• LTD weakens synapses that
interfere with performance
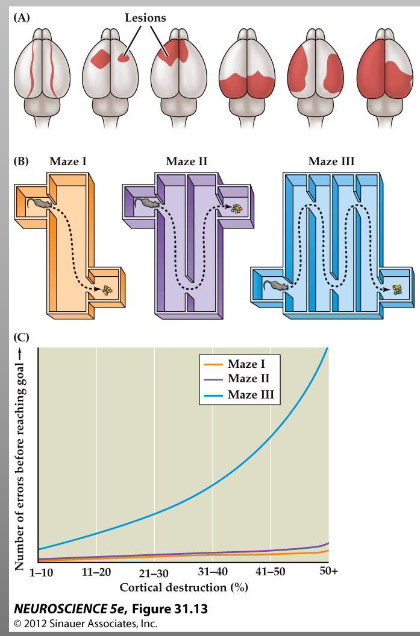
What are memory storage sites?
• Karl Lashley and the “mass
action principle”
• Degradation of learning
and memory depends on
the amount (not the
type) of cortex destroyed
Subtypes of Declarative and nondeclarative memory
What is Alzheimer’s Disease?
• A disease of old age.
• Alzheimer’s is a devastating neurodegenerative disease
which effects 1 in 10 people over the age of 65. Incidence
increases to 47% for people over 85.
• It is extremely costly to our society, and much effort is
being expended to find a cure or better treatments.
• Usually affects people over 65, but rare, aggressive forms
of Alzheimer’s affect people as early as 40’s
• Progresses slowly 3-18 years, average 8 years
• Death results not from the disease, but from a secondary
illness such as pneumonia
• Characterized by dementia
What is Dementia? (Senility)
• Dementia is a progressive decline in mental function, memory
and intellectual skills.
• Defined as memory impairment plus one or more of the
following:
• Aphasia (language problems)
• Apraxia (complex movement problems)
• Agnosia (problem identifying objects)
• Problems with executive functioning (making everyday decisions)
• Dementia is age related - almost never under 45
Is Dementia a normal part of aging?
No
• Used to be thought of as a normal part of aging. We now
know that it is caused by disease processes
• 70% due to Alzheimer’s disease
• 15% due to strokes (vascular dementia)
• 15% due to other neurological diseases
Clinically Diagnosis of Alzheimer’s Disease is typically very ____
accurate
• Thorough evaluation of symptoms
• Assessment of patient's health
– tests for memory and thinking skills
– input from family members
– physical health
– brain imaging scans
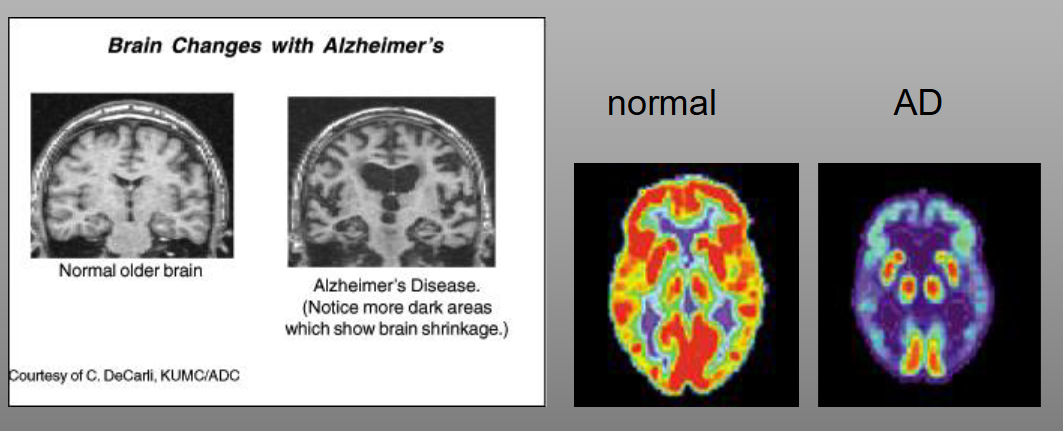
• MRI for structural changes
• PET for functional changes
MRI and PET scans show loss of cortices, enlarged
ventricles, and reduced metabolic activity
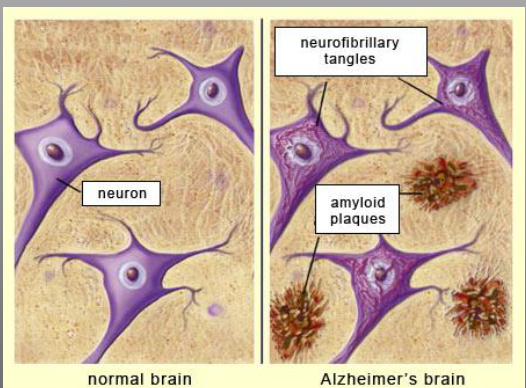
What are plaques and tangles, related to Alzheimer’s Disease?
Senile plaques
• Extracellular
• β-amyloid is a protein component of the plaques
• Also found in healthy brains, but in Alzheimer’s patients it exists as a molecular
fragment of a large protein found in the normal brain
Tangles (neurofibrillary tangles)
• Intracellular
• Bundles of filaments arranged in a helix - derived from normal structures in neurons
• Usually formed in large neurons in the brain
• Linked to an abnormal accumulation of the protein tau
• Tau is a normal brain protein, but people with AD have noticeably elevated levels
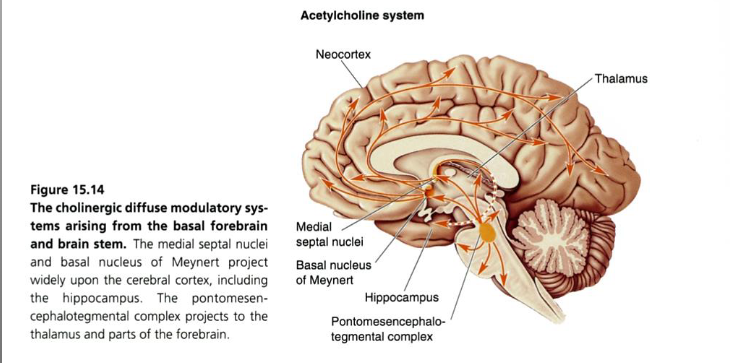
Pathology of Alzheimer’s Disease
Neuronal cell loss and changes in neuronal
morphology
Specific loss of ACh-containing neurons
• nucleus basalis (also called basal nucleus of
Meynert)
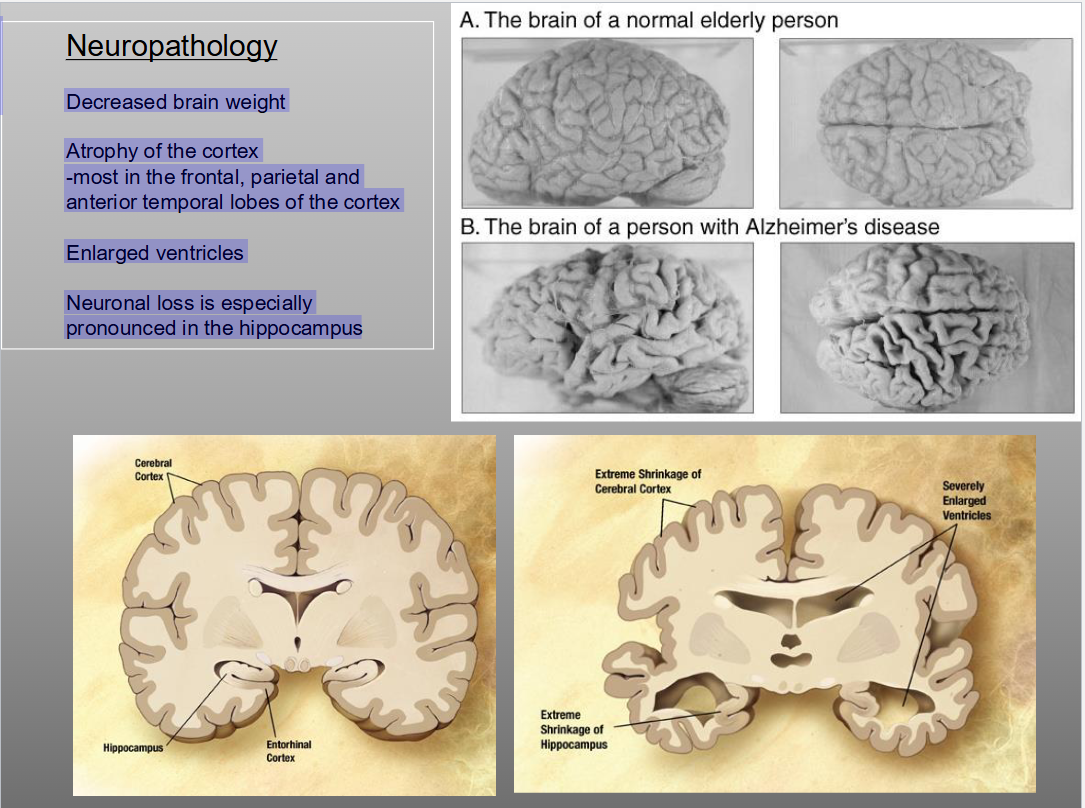
What is the Neuropathology of Alzheimers
Decreased brain weight
Atrophy of the cortex
-most in the frontal, parietal and
anterior temporal lobes of the cortex
Enlarged ventricles
Neuronal loss is especially
pronounced in the hippocampus
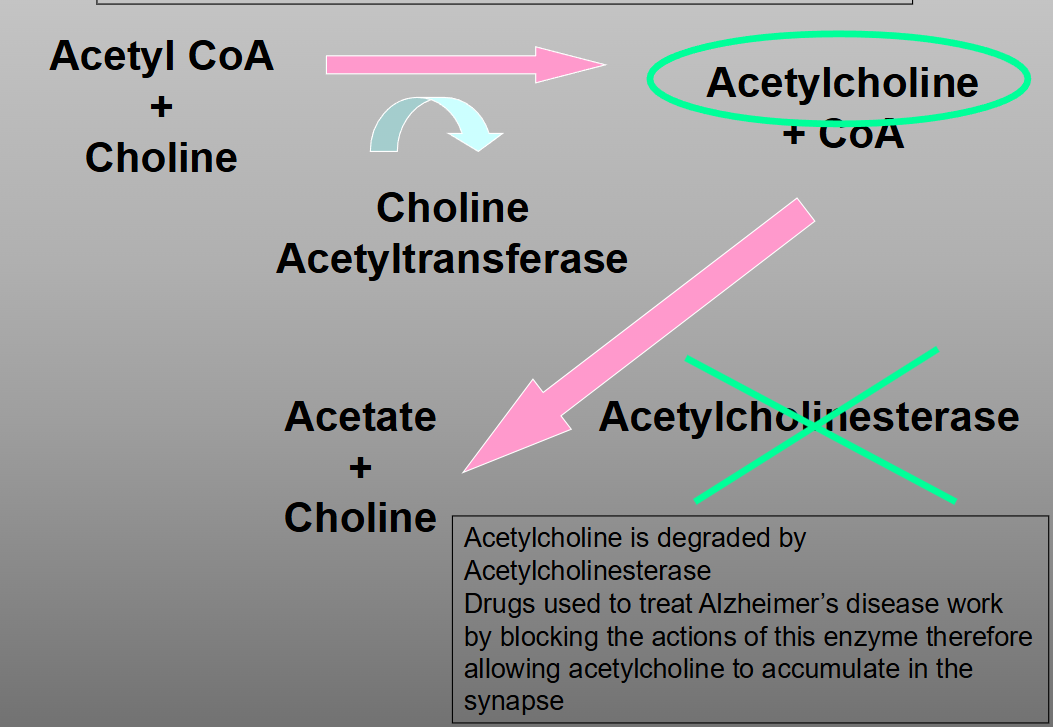
What is the pharmacological treatment for Alzheimer’s Disease?
• What would be the best strategy to counteract AD?
• Try to compensate for the loss of cholinergic
neurons.
• Primary method:
• inhibit the degradation of ACh