Hip Exam and Interventions
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
What questions should you ask during your history?
Any N/T or symptoms beyond the knee?
Any changes in running/training/exercise routine?
Do symptoms change with lumbar movements?
Any stiffness? If so, when and how long does it last?
Any catching/clicking/snapping?
What is the lower extremity functional scale (LEFS)?
Self-reported measure
Rank difficulty of ADL
Sports subscale available as well
Lower score indicates greater disability
MDC/MCID = 9
What is the flow of the hip exam?
History/subjective/constitutional s/s
Cardio screen
UQ neuro screen
Clinical movement assessment
Screening (lumbar/knee overpressure)
Static postural assessment
AROM/PROM
Strength (MMT)
Palpation
Special tests
What should you do during the lumbar screening?
Seated extension/rotation
Slump test
Repeated motions
Straight leg raise
If your pt has dysfunctional MS flexion on SFMA, what should you check?
Active/passive SLR
Double knees to chest
Prone rock test
If your pt has dysfunctional MS extension on SFMA, what should you check?
Active/passive SLR lumbar locked thorax rotation/extension
Prone on elbow lumbar rotation/extension
FABER
Modified Thomas test
If your pt has dysfunctional MS rotation on SFMA, what should you check?
Seated and prone ER/IR
What are the extra-articular conditions of the hip?
Muscle strain/tear
Stress fracture
Athletic pubalgia
IT band syndrome
Trochanteric bursitis
Piriformis syndrome
Snapping hip
What are the trauma conditions of the hip?
Hip/femur fracture
What are the intra-articular conditions of the hip?
Femoral-acetabular impingement (FAI)
Acetabular labrum tear
Degenerative arthritis (OA)
What are the congenital/pediatric conditions of the hip?
Legg-Calve-Perthes disease
Slipped capital femoral epiphysis
Avascular necrosis of femoral head
What is the common presentation of hip/femur fx?
Over age 60
Hip pain
Can't bear weight
**Trauma
What is important to remember about hip/femur fractures?
Mortality is high (30 day mortality rate 1-12%)
Permanent loss of function (up to 50%)
What are the special tests for hip/femur fx?
Fulcrum test
Patellar-pubic percussion
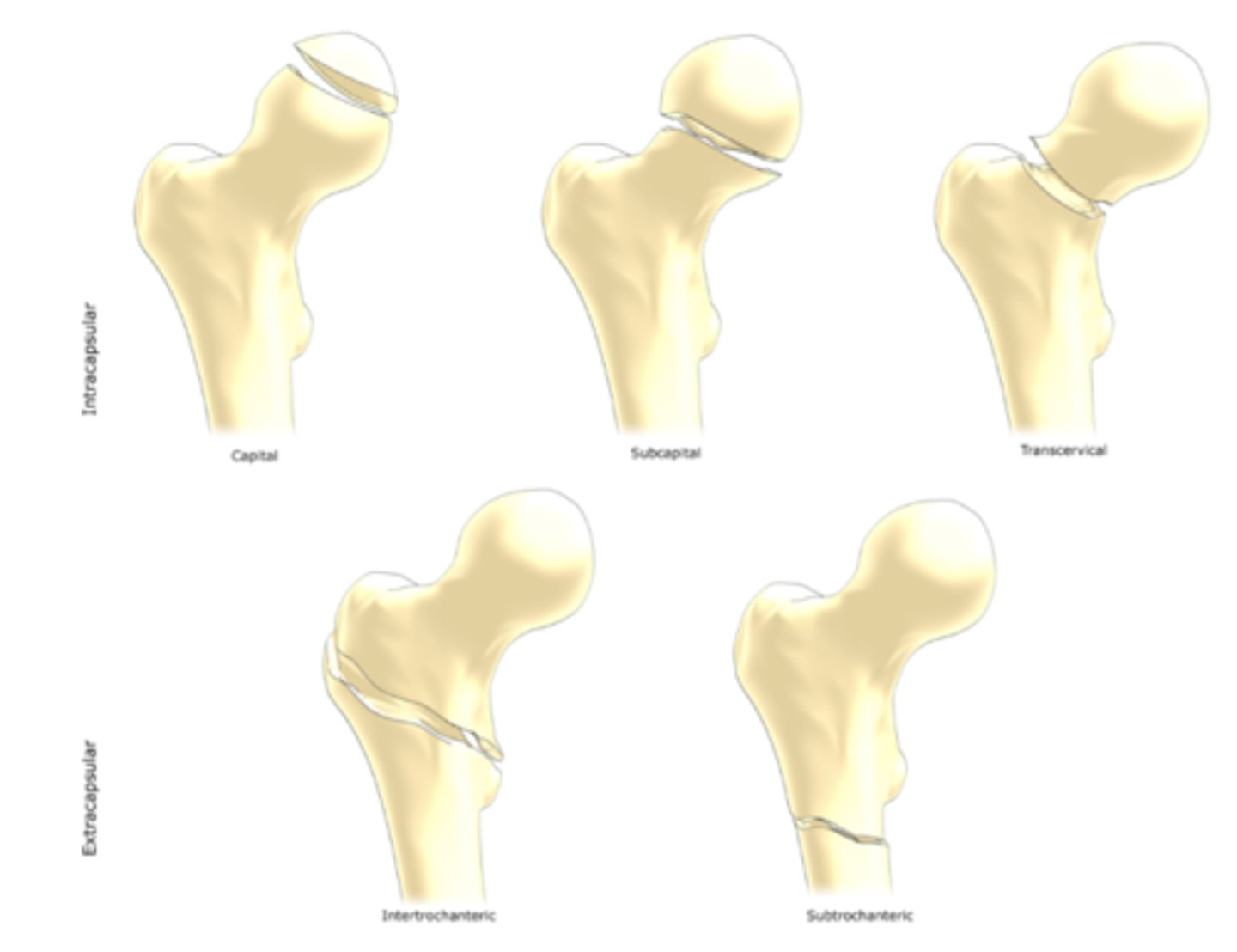
What are the different types of femur fx?
Subcapital neck
Transcervical neck
Intertrochanteric
Subtrochanteric
Fx of greater trochanter
Fx of lesser trochanter
What is the fulcrum test for hip fx?
Pt is seated. PT places arm under painful leg and hand on opposite leg. PT applies a downward force at distal femur on painful side
Positive test = reproduction of pain
What is the patellar-pubic percussion test?
Place stethoscope over pubic bone, tap on patella
**Listening for difference from side to side
What is the presentation of a hamstring strain/tear?
Typically ages 15-45
Due to sudden overload of hamstrings (usually eccentric)
Pain typically in post thigh or buttock
How to clinically diagnose a hamstring strain/tear?
Pain with resisted testing (hip ext, knee flex) and passive SLR; tenderness over hamstring muscle belly
What are the additional special tests for hamstring injury?
Puranen-Orava test
Bent knee stretch test
Modified bent knee stretch test
What is the "take off the shoe test"?
Pretty self explanatory
Ask the pt to take their shoe off the painful side
Positive test = pt reports pain with mvmt
What is a 1st degree hamstring injury?
Pathophys- tearing of only a few muscle or tendon fibers
S/S - Minor swelling and discomfort with no or minimal loss of strength
What is a 2nd degree hamstring injury?
Pathophys - more severe partial tear without complete disruption of of the musculotendinous unit
S/S - clear loss of strength with more discomfort
What is a 3rd degree hamstring injury?
Pathophys -a complete rupture of musculotendinous unit
S/S - total lack of muscle function and commonly associated with massive hematomas
How to diagnose other muscle strains in the hip?
Same concept as hamstring (exam and grading can be applied to other muscles - adductor, quads, etc)
Generally pain with resistance and stretching of involved muscle
What is the adductor squeeze test for muscle strain?
Pt in hook lying. PT places fist between pt's legs. Ask pt to squeeze fist
Positive test = pain and/or weakness
What are additional adductor injury tests?
Hip flexed to 30 degrees, pt resists abduction motion
- can do single or bilateral
Positive test = pain is reproduced
What is the presentation of femoral neck stress fx?
Persistent groin pain that worsens with activity
Usually in endurance athletes/training errors (female athlete triad)
**Pain with ROM, tenderness to greater trochanter
What is the female athlete triad?
Low energy availability (disordered eating), Irregular period (amenorrhea), Low bone density (osteoporosis)
What is the additional test for hip fx?
Heel strike test (no metrics)
What is the presentation of adductor tendinopathy?
Usually point tender and pain localized to pubic tubercle
Commonly associated with twisting the foot planted, repetitive kicking, sudden changes in directions, lateral movements
May have associated pelvic floor weakness (Ask about incontinence)
*sometimes called a sports hernia
What is the description of adductor tendinopathy?
"disruption and/or separation of the more medial common aponeurosis from the pubis, usually with some degree of adductor tendon pathology"
Commonly seen in soccer and hockey players
What is the clinical diagnosis of adductor tendinopathy?
Deep groin/lower abdominal pain
Pain exacerbated with exertion (sprinting, cutting, sit-ups but improves with rest)
TTP pubic ramus
What is the special test for adductor tendinopathy?
Single adductor test
What are the 2 types of snapping hip syndrome?
External = iliotibial band syndrome
Internal = iliopsoas bursitis
What is iliotibial band syndrome?
Gradual onset of lateral hip, thigh or knee pain
May have snapping over greater trochanter
What is the Ober test for IT band syndrome?
Examined leg up, abduct and extend hip until it is in line with the trunk; allow gravity to adduct hip as much as possible
Positive test = if unable to adduct to horizontal position and/or pain
What is tronchanteric bursitis?
May have history of trauma or overuse
Difficulty lying on affected side
What is the clinical diagnosis of trochanteric bursistis?
TTP greater trochanter; pain with active and resisted hip abd or ER
What is the special test for trochanteric bursitis?
Trendenlenburg sign
What is the presentation of ilipsoas bursitis?
Deep snapping sensation (even with walking)
Common in sports with forceful, repetitive hip flex/ext
May reproduce symptoms with active or passive hip flex/ext; painful resisted hip flexion; usually limited hip extension
What is the presentation of piriformis syndrome?
Gradual onset of buttock or posterior thigh pain, mimics radiculopathy (pain will stay above the knee)
May have pain with transitional mvmts (bending, stooping)
What is the FAIR test for piriformis syndrome?
Pt is sidelying on uninvolved side
Involved side is flexed to 90 degrees and maximally adducted before adding passive IR
Positive test = symptoms reproduced
What is the presentation of FAI?
2 types
Can be associated with labral tears
Commonly seen in active individuals
May be due to limited capsular mobility
Where is a pt's pain with FAI?
Groin
C - sign: pt indicates pain over anterolateral hip (deep pain)
What is the FADDIR special test for FAI?
Passive combined flexion, adduction, IR in supine
Positive test = reproduction of groin pain and/or clicking
*can also add axial compression
What are the additional special test for FAI?
Flexion IR test
Internal rotation-flexion-axial compression test
What is the special test for FAI/Labral tear/Intra-articular pathology?
Patrick (FABER) test
Positive test = reproduction of pain, clicking, catching is noted; also quality and quantity of motion
**not great metrics
What is the presentation of an acetabular labrum tear?
Wide age range
Women > men
Groin pain (up to 55%)
No known MOI (74%)
Who is at risk for acetabular labrum tears?
Runners, pro athletes, or rotational sports; gym attendance of 3x/week
How do you diagnose a labrum tear?
FADIR, FADIR + axial compression, Flexion/IR, etc. all have great sensitivity
No tests to confidently rule in
Arthrogram MRI is best option to capture
What is the special test for labrum tear?
Report of clicking in hip (best option)
What special tests can be used to elicit a click?
Fitzgerald test (SN= .98): D1/D2 PNF pattern
McCarthy test: passively go from flexion to extension
What is the presentation of Degenerative arthritis?
Age >60
Reports pain and stiffness in hip that may radiate to the groin
Reports morning stiffness that lasts <1 hour, generally gets better with mvmt
Limited IR in early stages; all ranges limited as OA progresses
What is the Scour test for OA?
Pt in supine, passively flexes the symptomatic hip to 90 degrees and then move the knee toward the opposite shoulder and applies an axial load to the femur
What happens if a pt reports pain in ER, flexion, abduction during Scour test?
Doesn't fulfill criteria but still need to document the test reproduced pain and where the pt felt it
According to the 2017 clinical practice guidelines, what is the hip OA diagnostic criteria?
Pt is over 50 AND:
- moderate anterior or lateral hip pain during WB activities
- morning stiffness less than an hour in duration after waking
- hip IR ROM less than 24 degrees OR IR and hip flexion 15 degrees less than non-painful side
- AND/OR increased hip pain associated with passive hip iR
What is the CPR for OA (2008)?
- Squatting aggravates symptoms
- Lateral pain with hip flexion
- Scour test with adduction causing lateral hip pain or groin pain
- Pain with active hip extension
- Passive IR of 25 degrees or less
**4+ variables = SP .98, LR+ 24.3
**5 variables = SP .98, LR+ 7.3
What are some functional tests for hip OA?
30 second chair stand test
4-square step test
Step test
Timed single leg stance
Berg Balance Scale
Timed up and go
6 minute walk test
Stair measure
How do we differentiate between OA and FAI/labral tear?
Symptoms we expect for FAI or labral tear: clicking, C sign, young, active individuals
- flexion and IR reproduce pain, joint restrictions in 1 plane, ROM limitation in 1 plane
Symptoms for OA: morning stiffness, groin/lateral pain, older
- joint restrictions in multiple planes, ROM loss in multiple planes, pain w WB activities
How to differentiate between OA and trochanteric bursitis?
Bursitis: don't expect joint restrictions, positive Ober test, can't lay on that side
What is the diagnosis of Legg-Calve-Perthes?
Decreased blood flow to the femoral head which leads to avascular necrosis
Roughly 4x more common in males, ages 2-13
Familial link (20-25%)
What is the presentation of Legg-Calve-Perthes?
Insidious onset (1-3 months) of limp; may be accompanied by groin
May have pain during or immediately after activity, but pain-free at rest
May have quad atrophy
Will have limited hip ABduction and IR
Interventions include Petrie casting (4-6 weeks) - prefer this method
What is the diagnosis of Slipped Capital Femoral Epiphysis (SCFE)?
Displacement of the upper femoral epiphysis
Age 8-17 years
Slightly more common in males (60%)
Obesity is a risk factor (95%)
What is the presentation of SCFE?
Most are insidious, but can have trauma
Reports dull, vague, intermittent pain in hip, thigh, knee
Limited and painful IR, leg is typically in ER
Difficulty WB (limp)
Risk for avascular necrosis
How do we differentiate between Legg-Calve-Perthes and SCFE?
LCP:
- pain with activity, better with rest
- younger, usually boys
- No pain with IR
SCFE:
- typically high BMI, boys (a bit older)
- Painful IR, stay in FABER position
What is the diagnosis of avascular necrosis (AVN)?
Anterolateral region of femoral head most commonly affected, may be due to trauma
What is the presentation of AVN?
Dull ache or throbbing usually in groin, may radiate to lateral hip or buttock
Age range varies
May have history of previous fracture, prolonged steroid use, alcoholism, or SCFE
Pain w/ROM, but especially extension (<15 degrees)
Antalgic gait/difficulty WB
What is the summary of hip exam?
- Several hip diagnoses exist but they look very similar
- The tests to differentiate between diagnoses aren't great, so we rely heavily on subjective and demographic info