MEDS3001 Module 2
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
72 Terms
What proportion of Australia is overweight or obese?
Over 60%
How is BMI calculated and what categorises one as overweight or obese?
BMI = weight/height²
Overweight: BMI of 25 or over
Obese: BMI of 30 or over
What is the heritability of obesity?
~47%
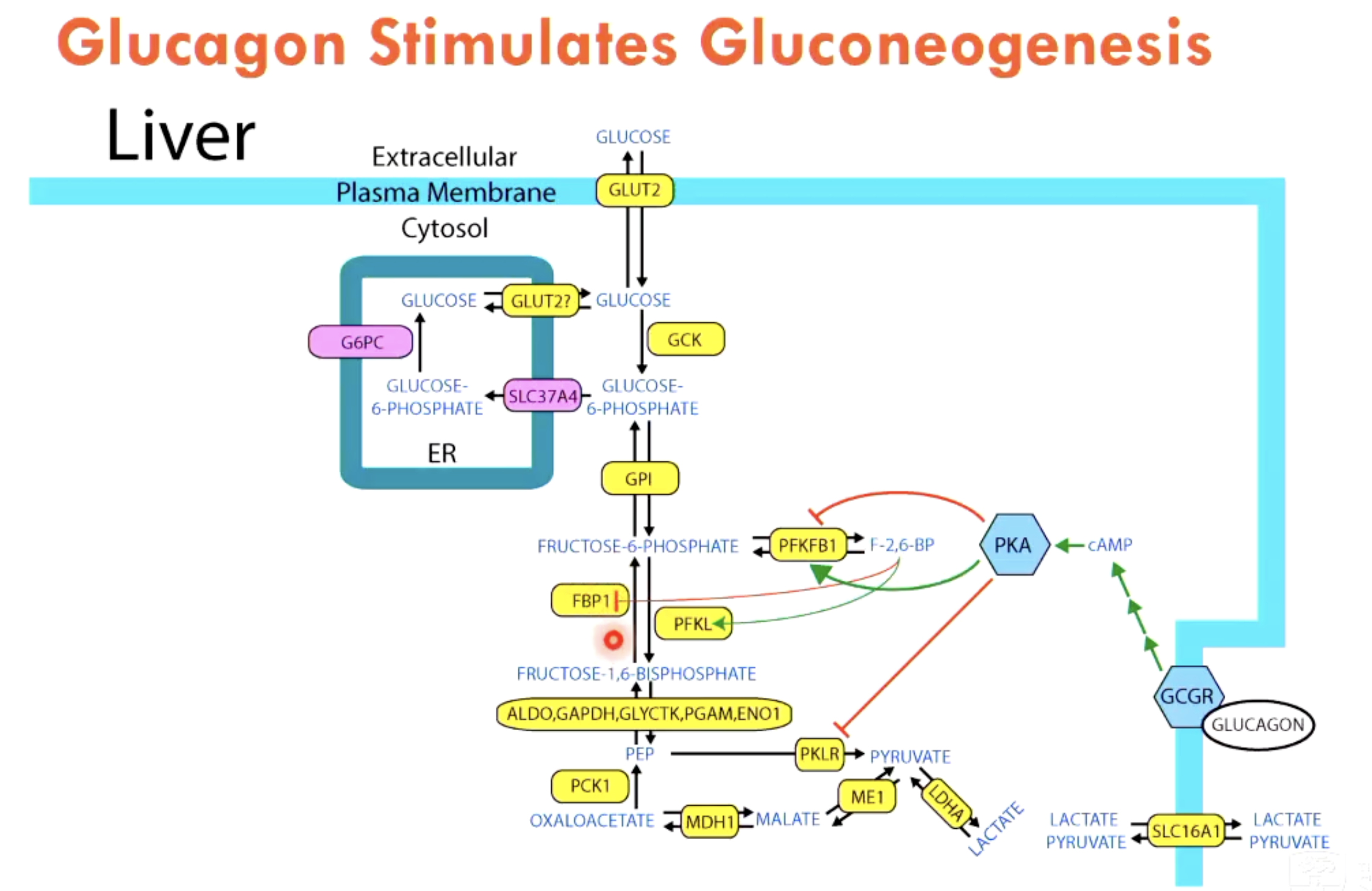
What is gluconeogenesis?
Gluconeogenesis is a metabolic process that creates glucose from non-carbohydrate sources like amino acids, lactate, and glycerol.
It occurs in the liver and kidneys, especially when blood sugar levels are low.
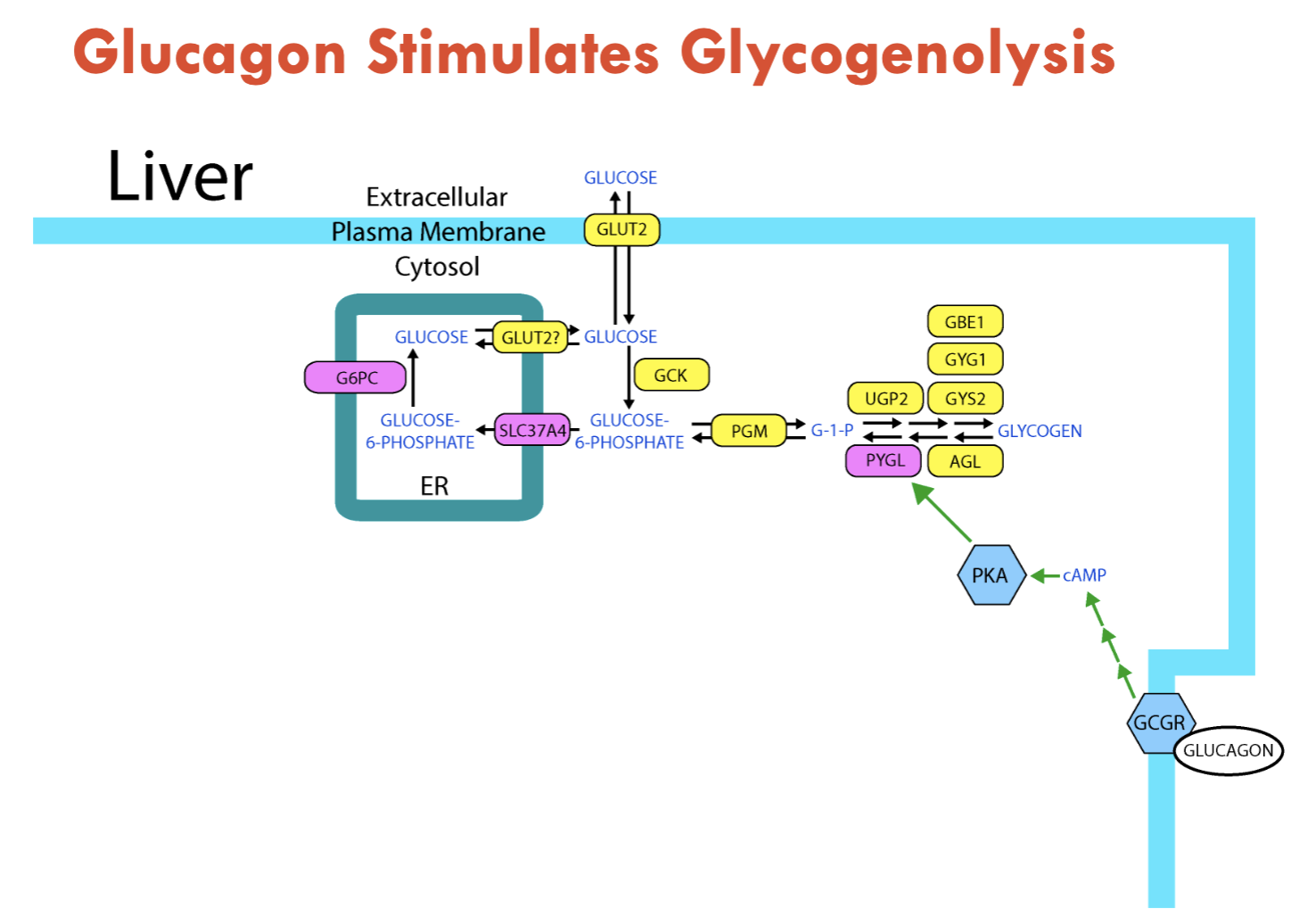
What is the main glucose source for humans in the first 24 hours of starvation?
liver glycogen
undergoes glycogenolysis: breakdown of glycogen to glucose
stimulated by glucagon
What is the main glucose source for humans after the first 24 hours of starvation?
gluconeogenesis
stimulated by glucagon
key substrates: alanine, pyruvate, glutamine, lactate
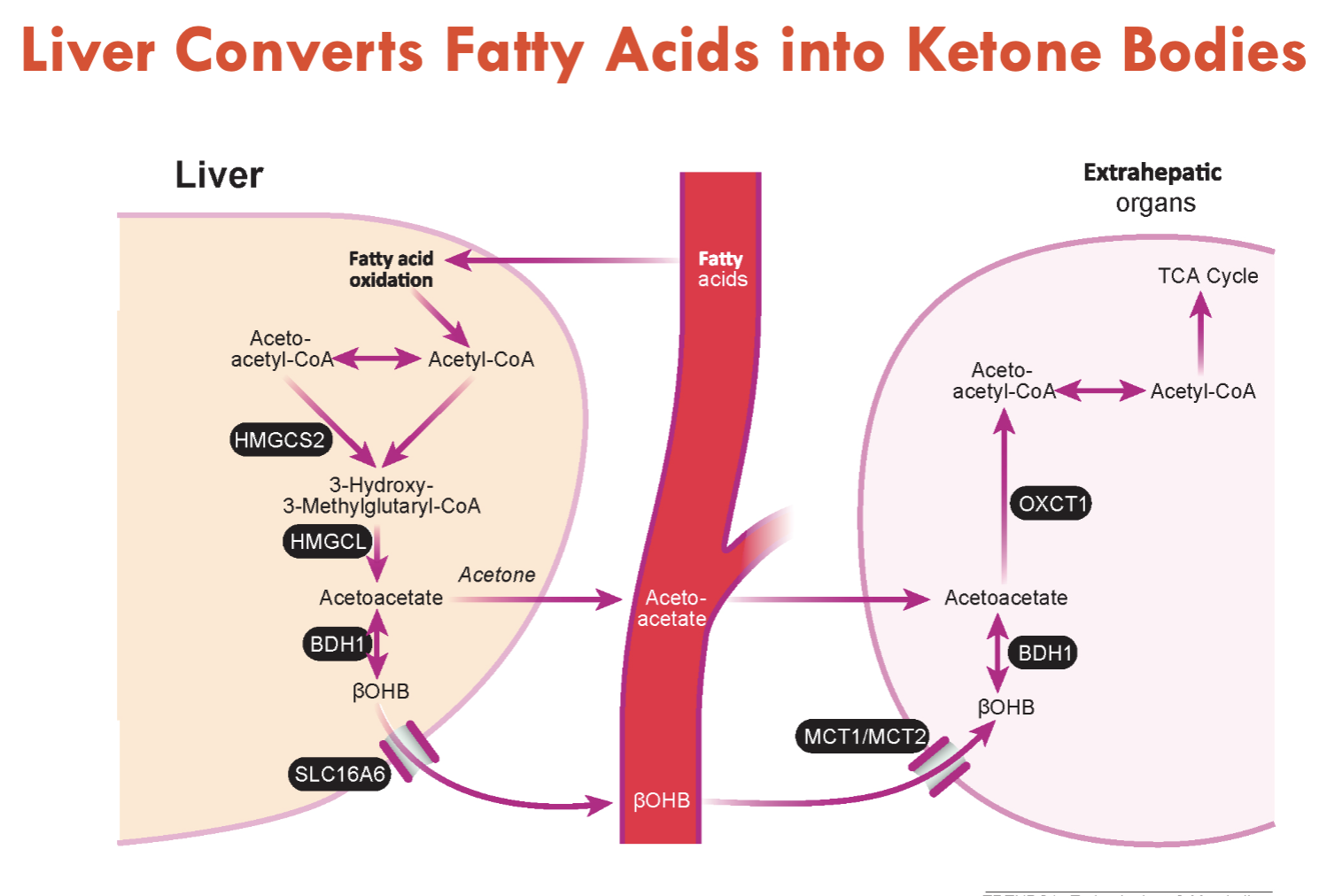
The liver converts fatty acids into…
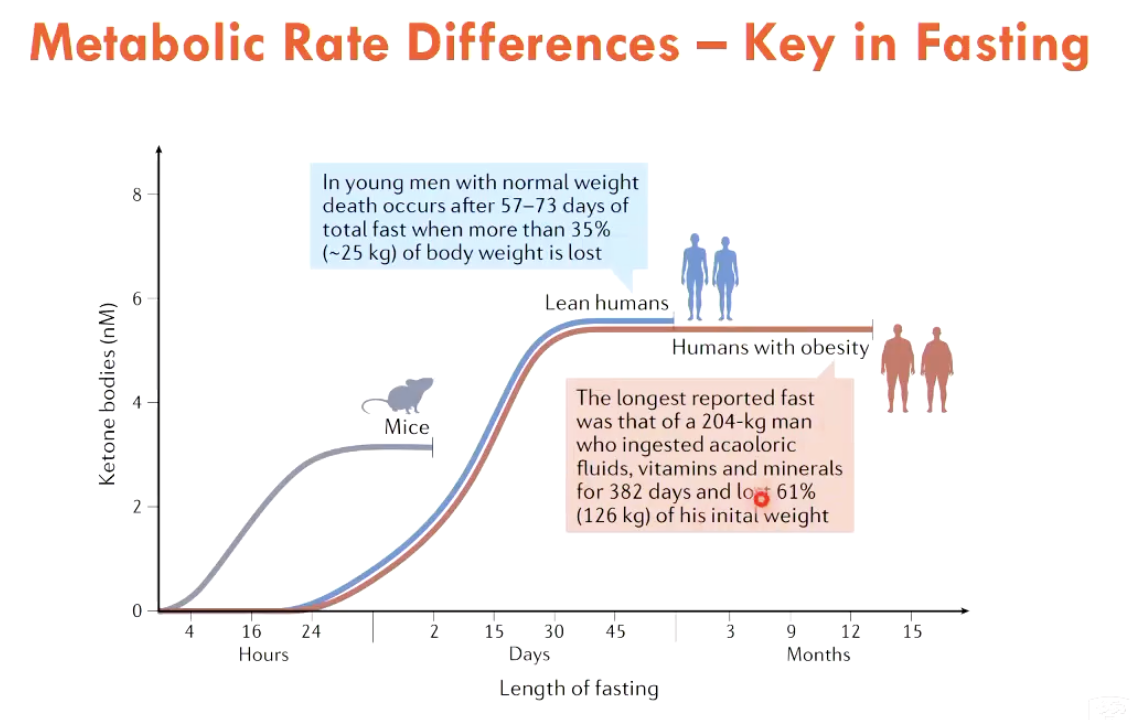
ketone bodies
acetoacetate, acetone, β-hydroxybutyrate (βOHB)
ketone bodies increase dramatically after 48h of fasting
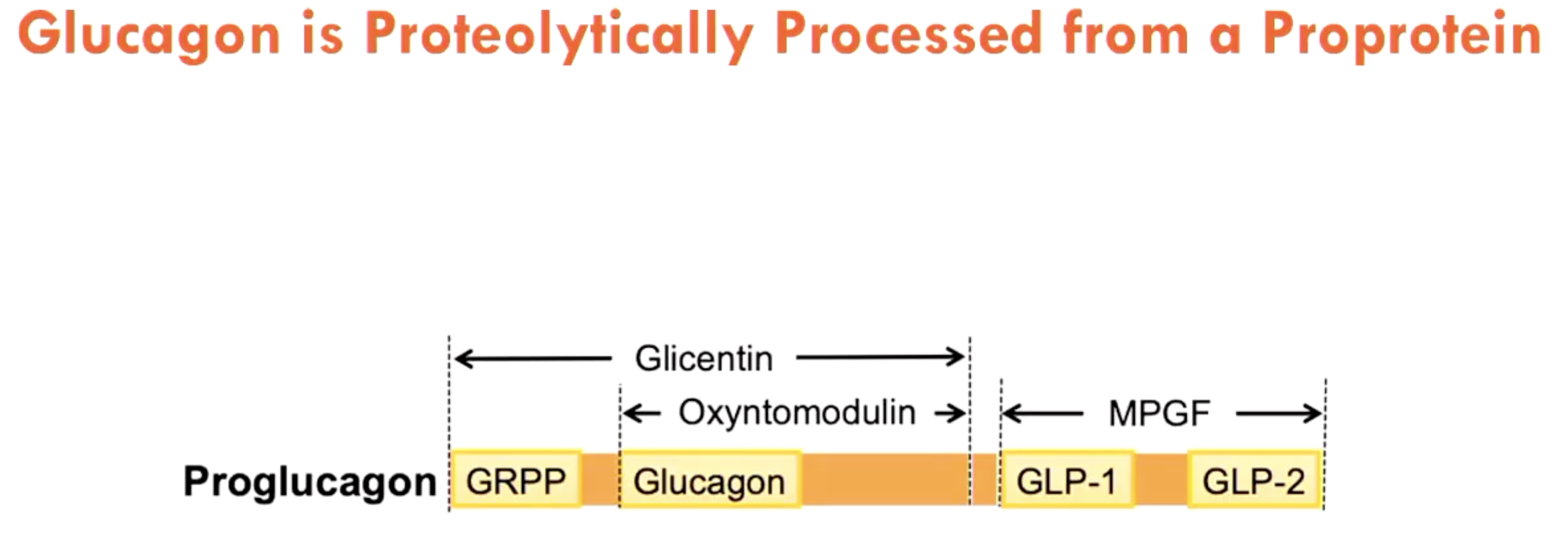
What is the relation between glucagon and proprotein?
Glucagon is proteolytically processed from a proprotein (proglucagon)
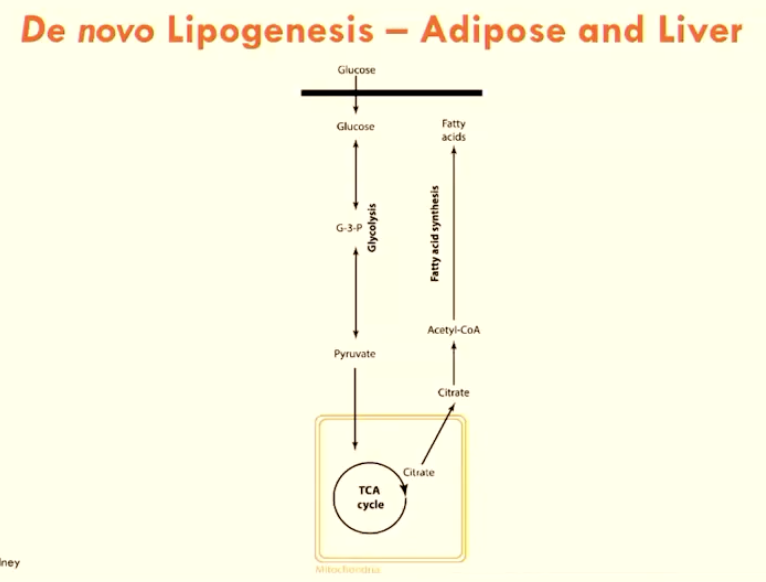
What process uptakes glucose into fatty acids?
De novo lipogenesis:
glucose → G3P → pyruvate (into TCA cycle) → citrate → FAs
can happen in liver and WAT
when FAs are in excess, this will be stored in adipose tissue (WAT)
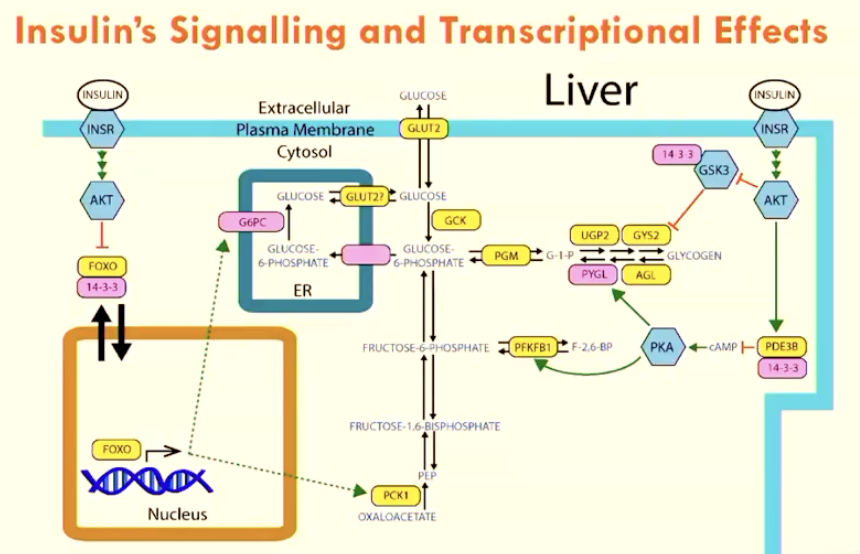
Describe insulin signalling and transcriptional effects
Insulin activates AKT
→ triggers FOXO to go into cytoplasm
OR → activates PDE38
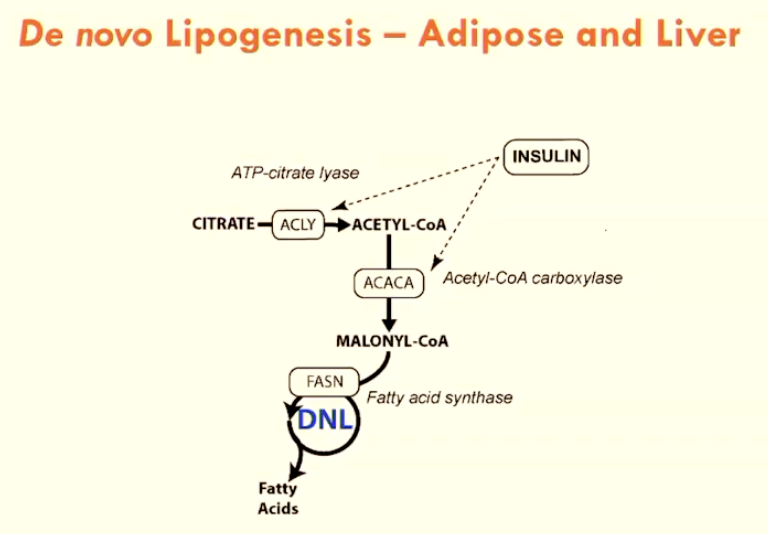
How does insulin regulate de novo lipogenesis?
Insulin directly controls ATP-citrate lyase through a phosphorylation cascade, which is a key enzyme in de novo lipogenesis.
List gut-derived peptide hormones
epithelial layer of small intestine have endocrine cells that release peptide hormones
Increases satiety: GLP-1, OXM, PYY
Increases food intake/appetite: Ghrelin, INSL5
These hormones mostly act on hypothalamus
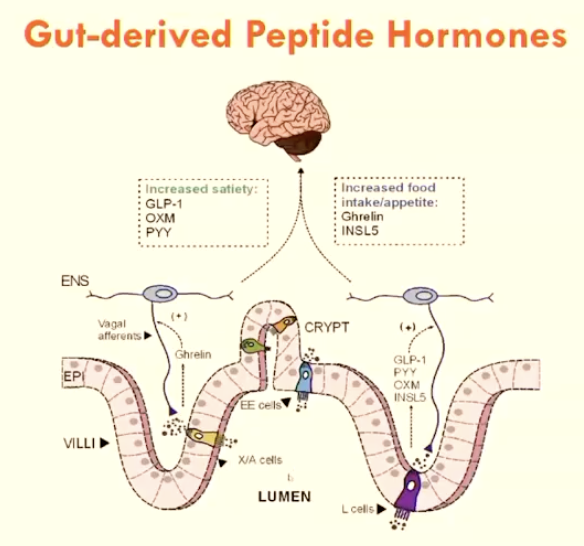
What is the incretin effect?
The phenomenon where oral glucose intake triggers a greater insulin response compared to intravenous glucose, due to the release of gut hormones like GLP-1 (released by L-cells) and GIP (released by K-cells)
these cells are only found in GIT, which would by bypassed intravenously
How is fructose metabolised?
Fructose uses KHK (ketohexokinase) to convert into glucose before undergoing usual glucose metabolism
Note: fructose over-consumption leads to fatty liver disease
Provide some general solutions for obesity (5)
Prevention is better than treatment
Dietary changes to reduce calorie intake
Exercise
Surgery - bariatric (expensive/dangerous?)
Medication (GLP-1 mimetics: expensive, side effects?)
Describe the simple method of implementing calorie restriction
Estimate average energy intake per day
Decrease that energy intake by >2500 kJ per day
Describe the features of a very low energy diet (VLED) (3)
2520 kJ per day
> 80% reduction in energy intake
typically 30% daily energy intake cut
Up to 2.5 kg weight loss per week
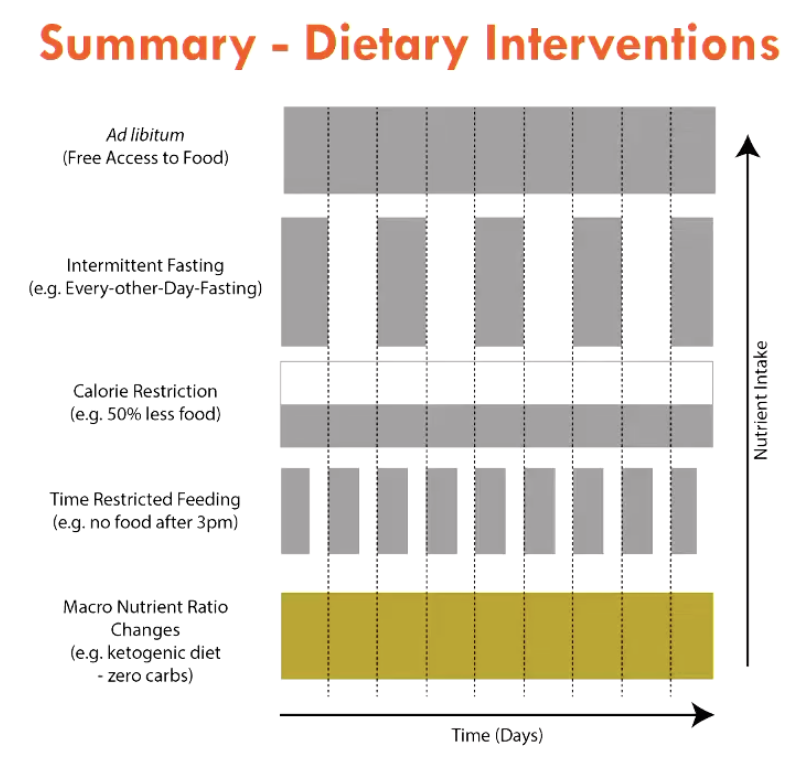
List the 4 main examples of dietary interventions
Calorie Restriction (e.g. 50% less, VLED)
Intermittent Fasting (e.g. Alternative Day Fasting)
Time-Restricted Feeding (e.g. no food after 3pm)
Macronutrient Ratio Change (carb/protein/fat - e.g. ketogenic: no carb diet)
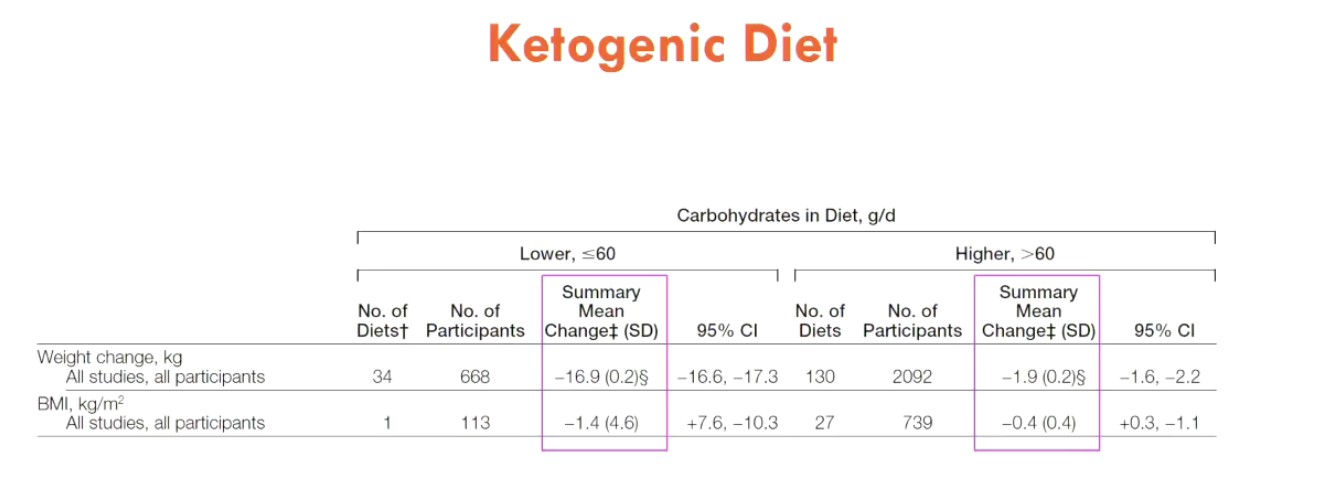
What happens to lipids under a ketogenic diet?
No carbs → no insulin produced → adipose tissue can undergo lipolysis without secretion
usually insulin signalling → AKT → signals for anti-lipolysis
Therefore, ketogenic diet is very effective in humans
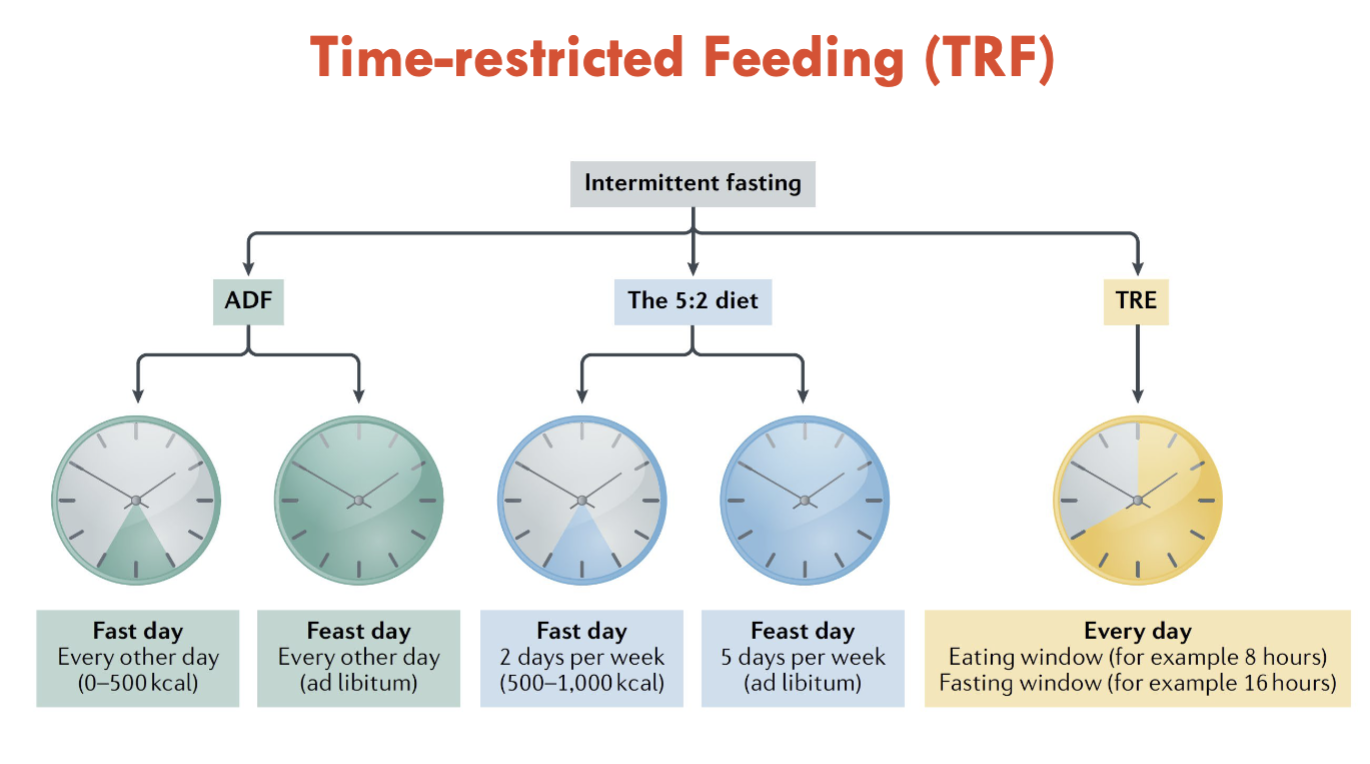
List 3 examples of Intermittent Fasting (IF)
Alternative day fasting (24hr feast, then 24hr fast)
The 5:2 diet (5 day feast day, 2 day fast say)
Time-restricted fasting (8-hour eating, 16-hour fasting)
Note: First 24 hours uses liver glycogen, ketone bodies dramatically increase after 48 hour fasting
What thresholds exist for exercise to intervene with obesity?
Weight loss is achieved with >300 mins aerobic exercise per week
metabolic improvements with >150 mins aerobic exercise per week
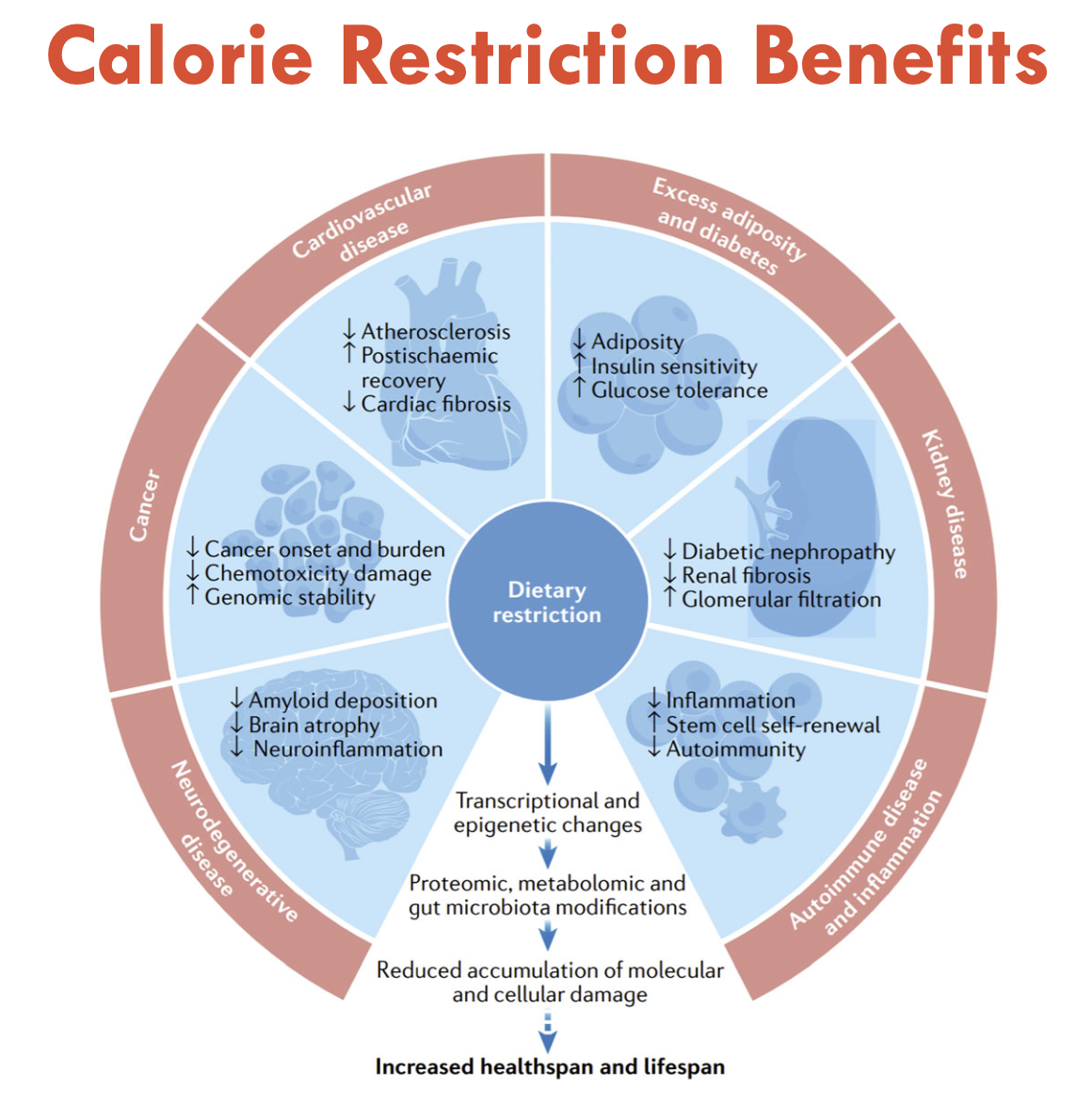
Benefits of Calorie Restriction
Improves:
Neurodegenerative Disease
Autoimmune disease and inflammation
Kidney disease
Excess adiposity and diabetes
CVD
Cancer
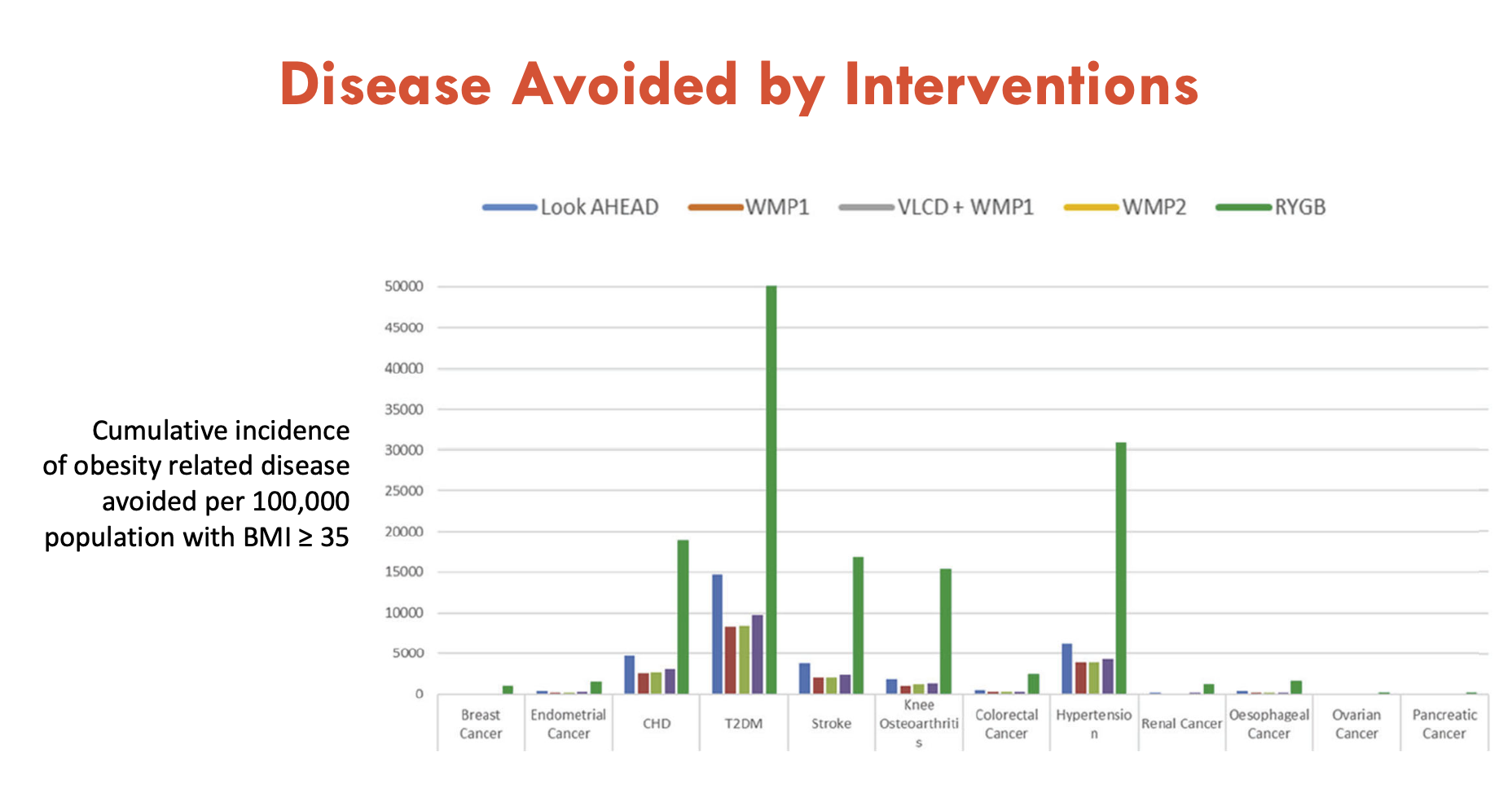
What is the effect of bariatric surgery (RYGB) on disease interventions?
RYGB is the most effective intervention for most diseases
more than weight management plans (WMP1/2) and VLCD
BUT very expensive
What issues exist with VLED studies in humans (2)?
Gender bias: p-values are only significant in females
Hard to conduct in youth: issues in discipline, financial status, peer pressure
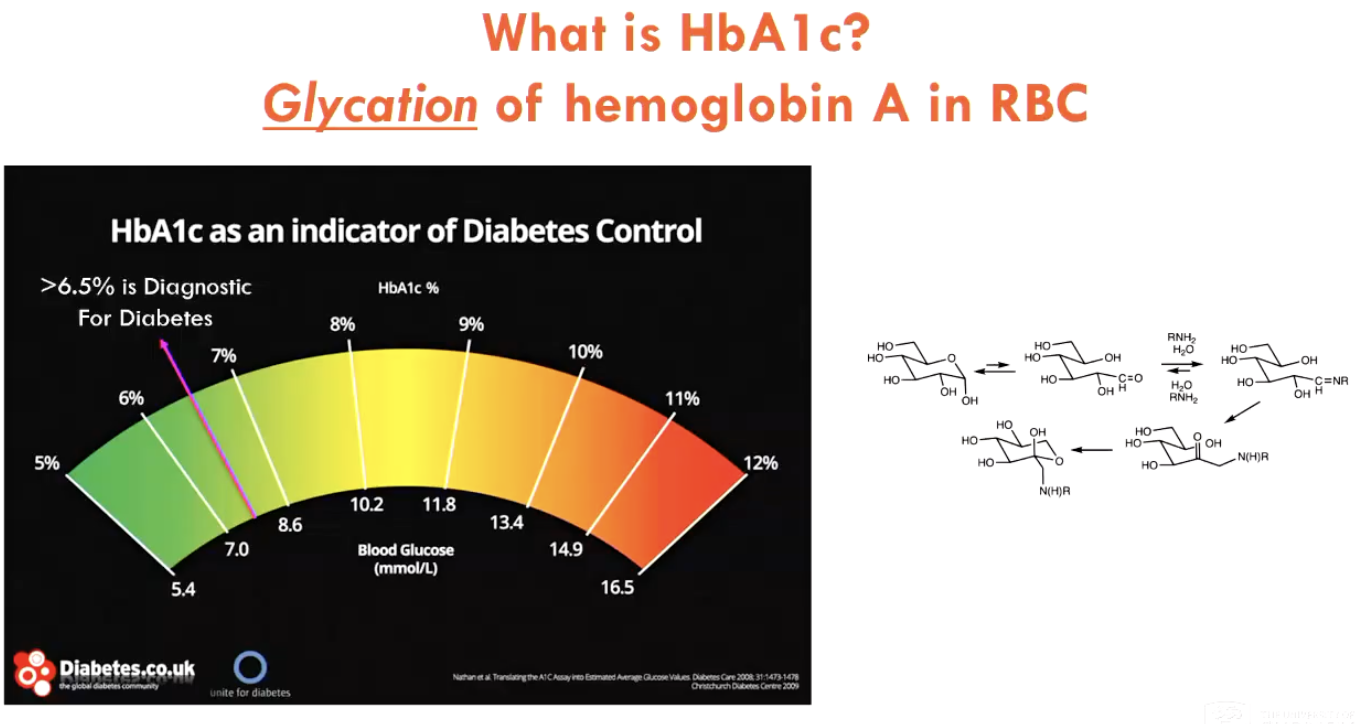
What is HbA1c and what does it indicate?
HbA1c is the glycation of haemoglobin A in RBCs
is a slow process (indicates ~past 3 months), therefore high % represents long-term elevated blood glucose
HbA1c serves as an indicator of diabetes control (>6.5%)
What is the role of leptin in obesity?
Leptin is secreted by adipose tissue at a constant rate
more adipose tissue = more leptin = negative feedback to stop eating
Therefore, in humans and mice with leptin deficiency, they have uncontrolled appetite → higher obesity rates
Injecting synthetic leptin in mice → reduces food intake
BUT injecting leptin doesn’t work in humans
What does calorie restriction do in animals?
Extends lifespan (in mice and monkeys)
What are some limitations of animal studies in food restriction studies (2)?
In the lab, food is always present in the ad libitum groups → unnatural mimicry of environment
instead of representing a control group, perhaps they are overweight due to constant food availability
In the lab, all food is given at one time (e.g. start of day) → long fasting period
creates confusion b/w mechanisms of intermittent fasting OR calorie restriction
IF is usually the mechanism that is required for life extension in animals
Is intermittent fasting effective in humans?
8 weeks IF is effective on insulin sensitivity, even if not trying to lose weight
4 weeks IF (EODF) is also effective on body mass and fat mass (both total and trunk fat mass)
BUT saw lean mass loss (bad bc this is loss in Sk.M and organ mass)
What is the fasting mimicking diet?
a short-term, low-calorie diet designed to mimic the beneficial effects of fasting without complete food restriction
Is time-restricted feeding effective in humans?
After 8 weeks, no significant difference is seen (only 3.2% weight loss)
side effects: fatigue and dry mouth (lack of hydration)
the actual time period used is important (don’t disrupt circadian rhythm)
Is intermittent fasting effective in mice?
Mouse: 2 weeks IF → improved insulin sensitivity, weight same
reduces blood IGF-1, which can reduce cancer risk
adipose repots respond differently to EODF (visceral adipose tissue becomes resistant to lipolysis, while subcutaneous is not affected)
What benefit does fasting mimicking diet have in mice?
extends healthspan
Key difference when fasting (humans vs. animals)
Humans take ~24 hours to achieve fasting state
Animals have higher metabolic rates → achieve fasting state quicker (use up fuel stores quicker)
do animals need to be studied on a different timeline?
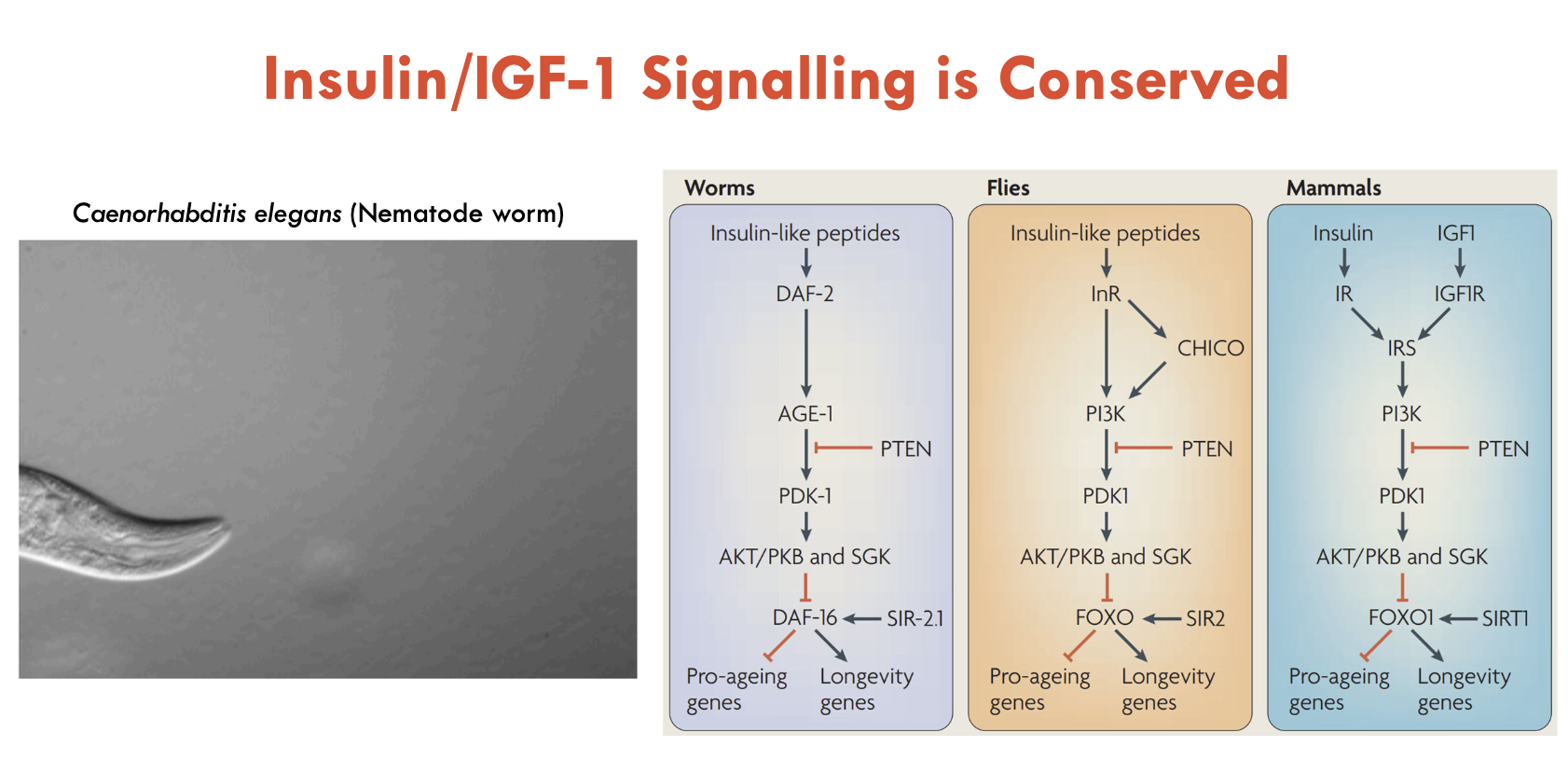
What is the insulin/IGF-1 signalling pathway responsible for?
Responsible for feeding metabolism
Insulin and IGF1 activates AKT (kinase), which phosphorylates FOXO1 (pushes FOXO1 out the nucleus and into cytoplasm → cannot bind to DNA targets)
Insulin/IGF-1 signalling inhibits FOXO1 TFs, which promotes pro-aging genes
Inhibiting insulin/IGF-1 pathway, activates FOXO1, which transcribes longevity genes
genes related to defence (suppress cell proliferation bc of minimal nutrients, also responsible for apoptosis of dysfunctional cells - sounds counterintuitive but LOL)
IGF-1 also controls growth and body size in mammals (dogs)
IGF-1 is pro-growth (more is found in big dogs over small dogs)
Intermittent fasting (EODF) reduces plasma IGF-1 (thought to increase lifespan)
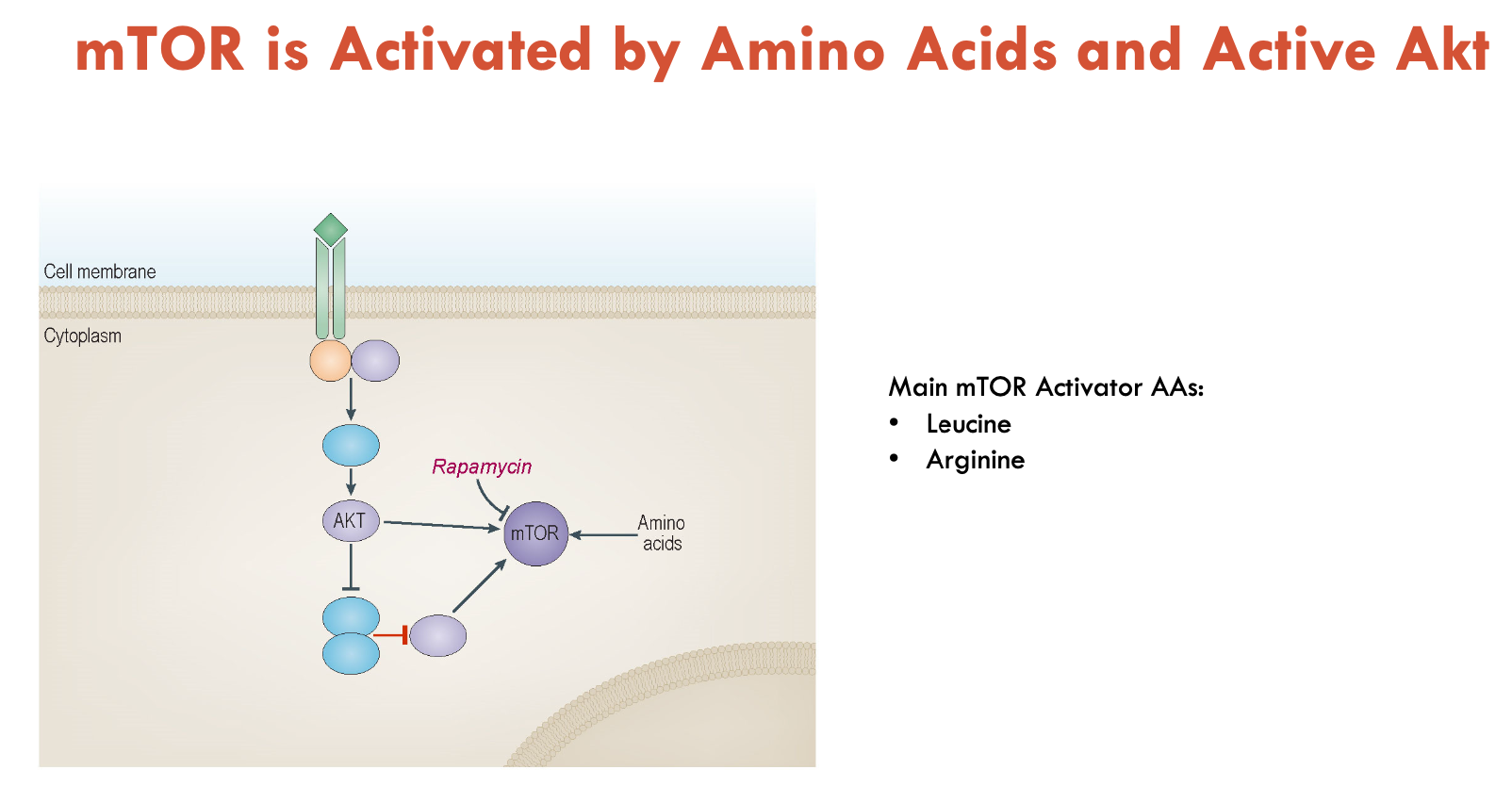
What is mTOR signalling responsible for?
mTOR is activated by sensing intracellular AAs (mainly leucine and arginine) and active AKT (kinase)
regulates protein synthesis
is inhibited by rapamycin (drug)
rapamycin extends life span in mice
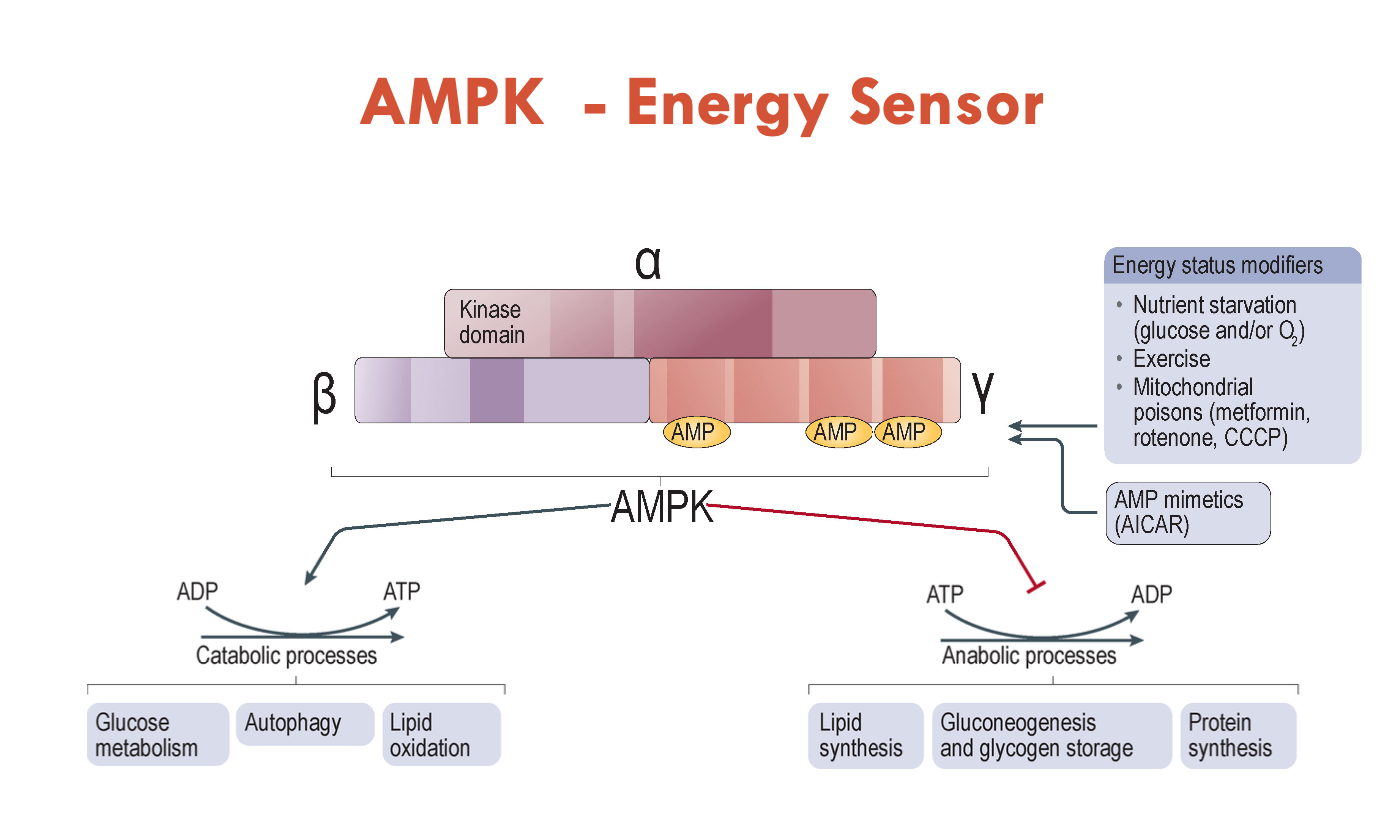
What is AMPK responsible for?
AMPK senses lack of nutrients in the cell
AMPK is made up of 3 proteins: α, β, γ
is activated during low energy levels, which stops processes using up energy (anabolic processes - lipid synthesis, gluconeogenesis and glycogen storage, protein synthesis)
instead, it stimulates processes that will make energy (catabolic processes - glucose metabolism, autophagy, lipid oxidation)
binds to AMP (an indicator of low nutrients bc ATP and ADP have been used up)
stimulated by starvation, exercise, mitochondrial poisons, and AMP mimetics
Metformin activates AMPK and has been approved to treat Type 2 diabetes
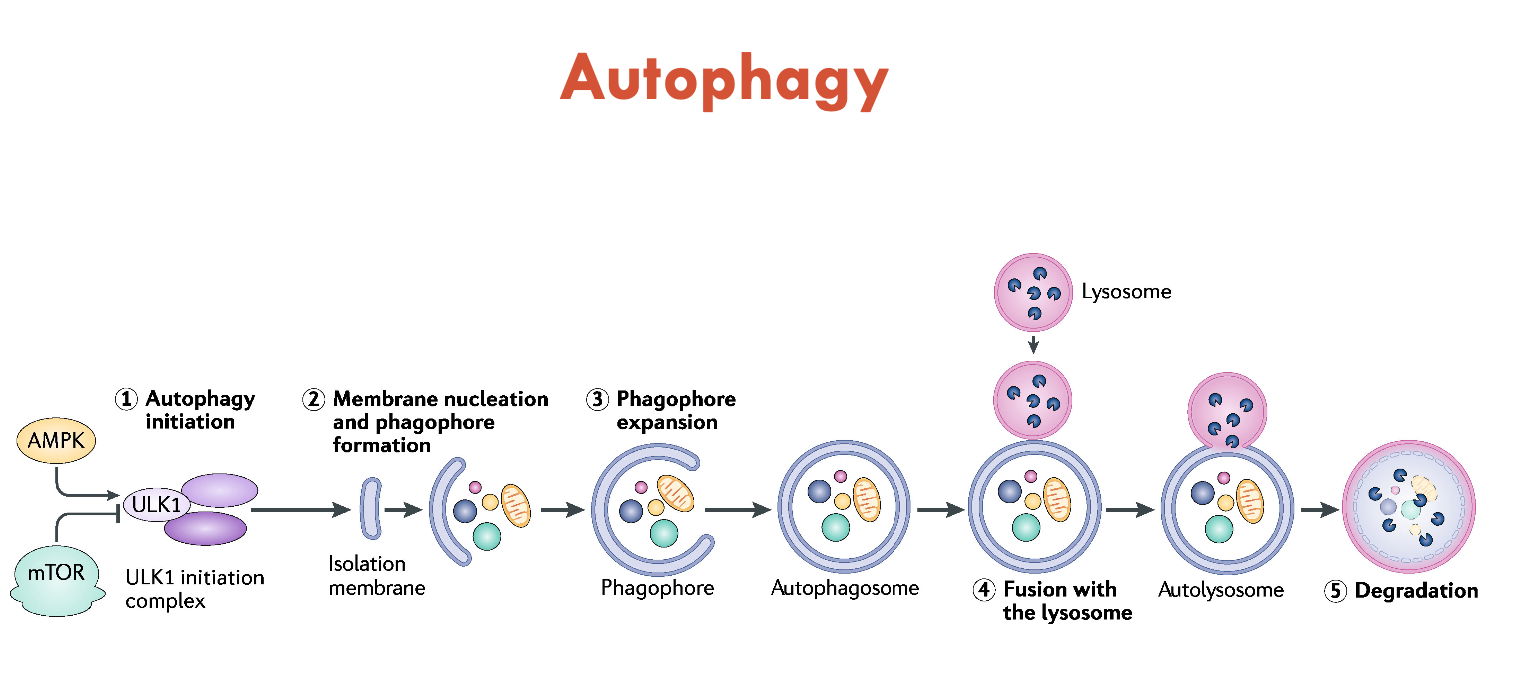
What is autophagy?
Autophagy is a process that occurs in all cells to recycle damaged components (e.g. damaged organelles like mitochondria)
occurs through signalling cascades
AMPK (lack of nutrients) activates autophagy
mTOR (AA availability) inhibits it
When activated, the cell takes a double-layered membrane and engulfs the damaged cellular constituents
then fuses to lysosomes for degradation
Degraded nutrients (AAs, FAs, sugars) are pumped out into the cytoplasm to be recycled
Defects in autophagy can lead to many diseases
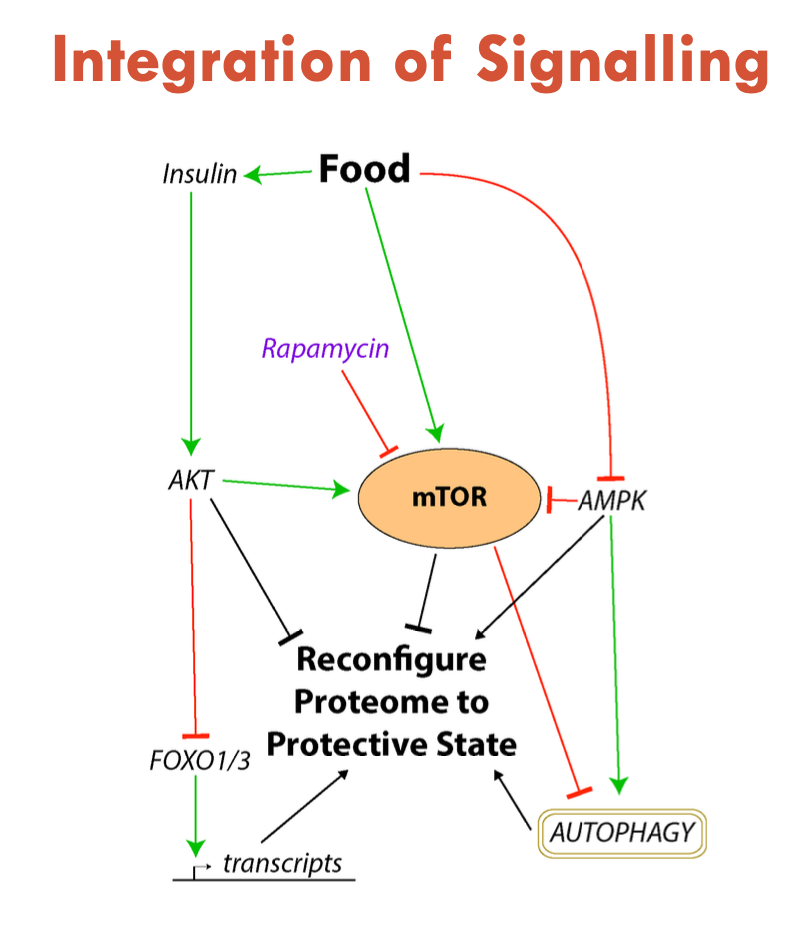
How are nutrient signalling pathways integrated?
Food:
triggers insulin
activates AKT
triggers mTOR
inhibits FOXO1/3
triggers mTOR
inhibits autophagy
inhibits AMPK
ultimately, becomes pro-growth BUT if on all the time, becomes pro-aging
What diets are best for lifespan compared to for reproduction?
High carbohydrate diet is best for lifespan
High protein diet is best for reproduction
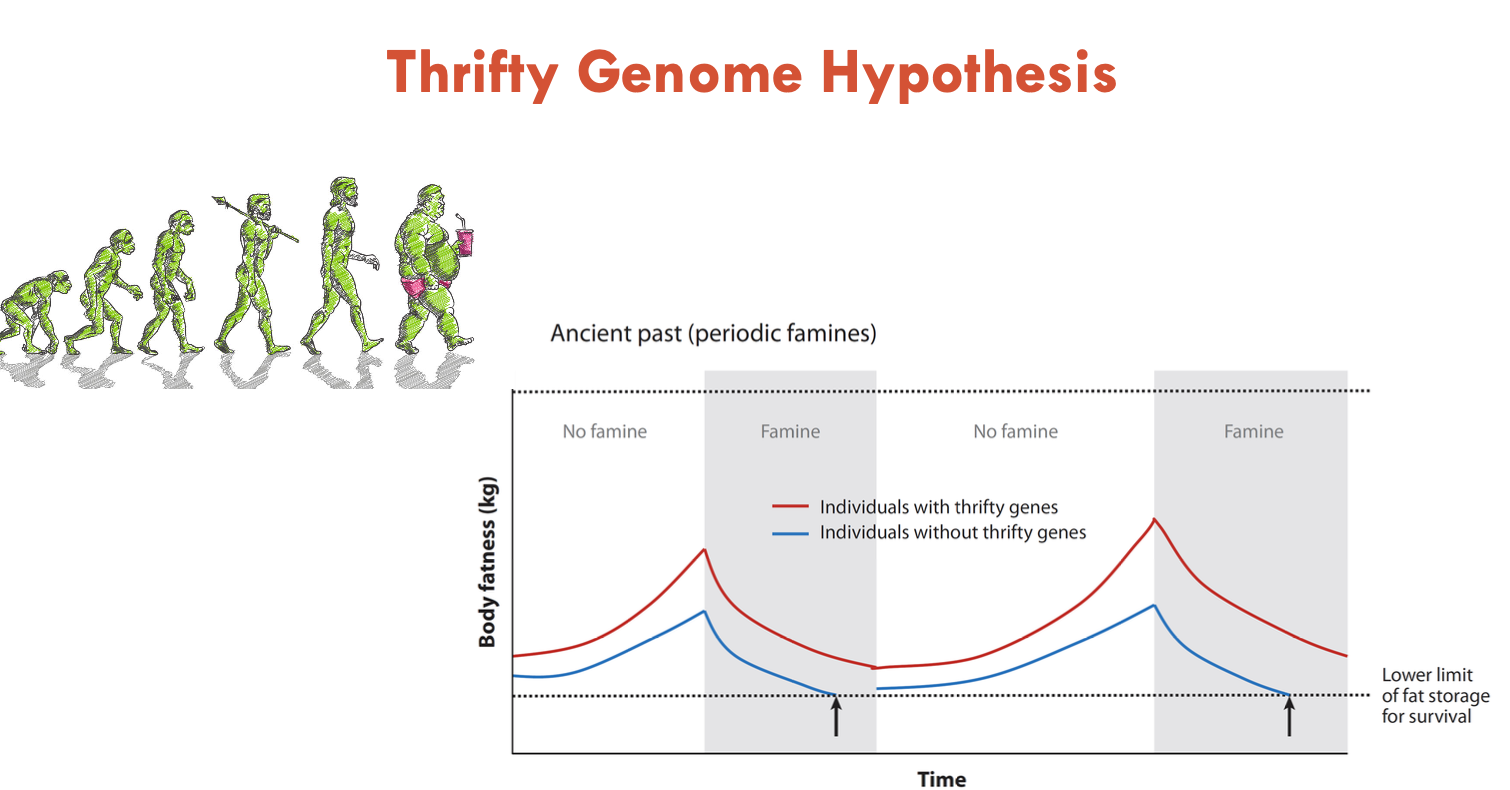
What is the thrifty genome hypothesis?
When food is consumed, we want to store it away for energy
adipose tissue provides the energy to survive starvation
thus, those with thrifty genes who can store more fat mass or extract more nutrients from food can survive longer periods of starvation (prehistoric times)
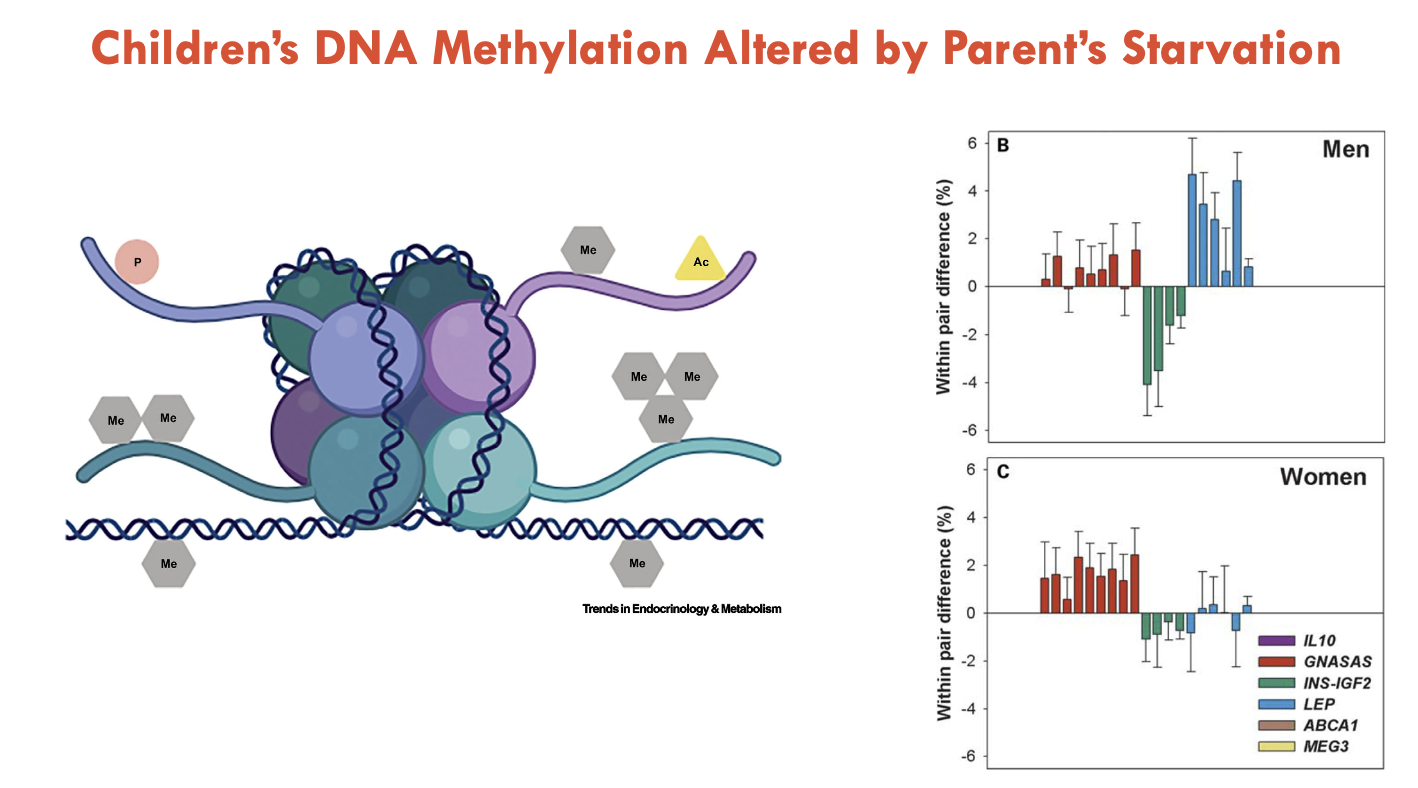
What is the thrifty epigenome hypothesis?
In mothers who were starved, their offspring had a higher risk of obesity and diabetes
demonstrates immediate adaptation to food scarcity
How does this occur?
DNA is wrapped around a histone with histone tails
Histone modifications: on the tails are post-translational modifications that can change gene expression very quickly (can bee through methylation or affect transcription)
DNA methylation: the DNA itself can also be methylated for such a quick modification (affects TFs)
Result: inheritance of starvation resistance
What is the protein leverage hypothesis?
Humans have a daily intake requirement of protein, but modern meals lack protein (protein is exxy) and are instead filled with carbs and fats
therefore, we eat more in search of the protein lacking in meals
How has agriculture affected our nutrient intake?
Transitioning from a hunter-gatherer society to an agriculture-based society, food is become unlimitedly accessible (ab libitum)
we also live more sedentary and settled lifestyles
leads to higher obesity rates
Define proteome
Proteome is the complete set of proteins expressed by an organism
complex and controls phenotype
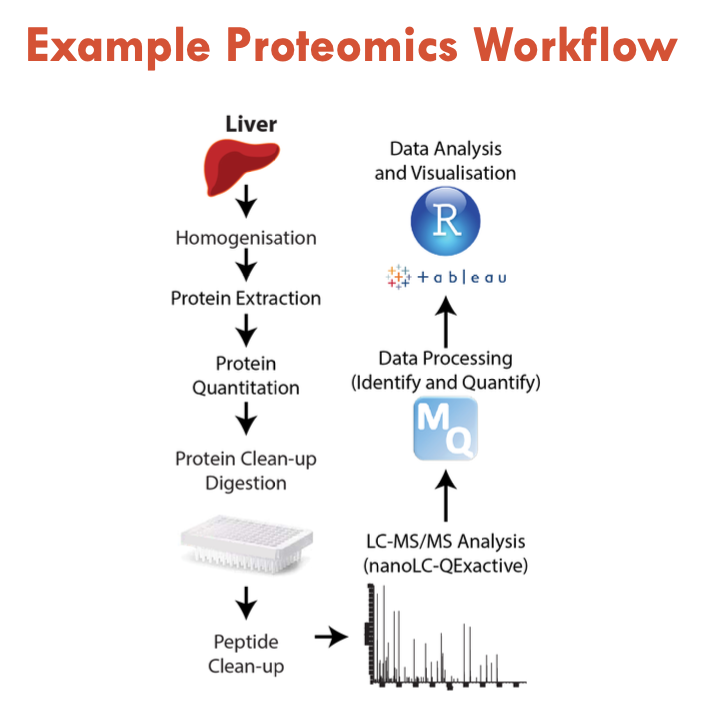
How are proteomes studied?
Proteins tend to be chemically heterogenous
so they are extracted and digested into peptides (often by trypsin)
Protein extraction → protein quantitation (ensure equal amount) → digest protein with trypsin → isolate peptides → LC-MS/MS Analysis → data processing (identify and quantify) → data analysis and visualisation
What steps are involved in mass spectometry?
Often combined with liquid chromatography (molecules bind to liquid-based column separation to determine hydrophobicity)
Overview:
Inlet (liquid chromatography system)
Ion source (in vacuum chamber): makes gas-phase ions (e.g. electrospray ionisation)
Mass Analyser(s) (in vacuum): separates ions by molecules and fragments ions through precise mass measurements and ion collisions
Detector (in vacuum): counts no. of ions for each molecule (an electron multiplier)
Computer: records electrical voltage
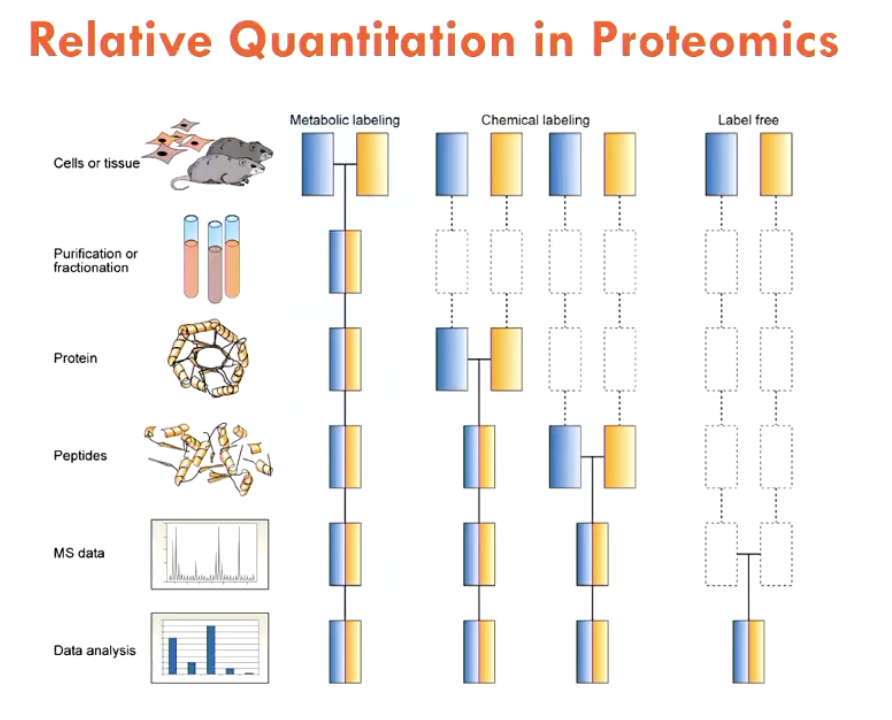
How are samples compared using MS?
Most accurate method: Metabolic labelling
use cells/tissues that are fed with either light (normal form) or heavy (stable isotopes introduced) AAs
establishes different isotope signatures
reduces error (want to introduce samples as early as possible)
Other methods are:
Chemical labelling (can only be introduced to semi-purified samples - aka proteins)
Label-free (no stable isotopes introduced at all, all are light - most errors)
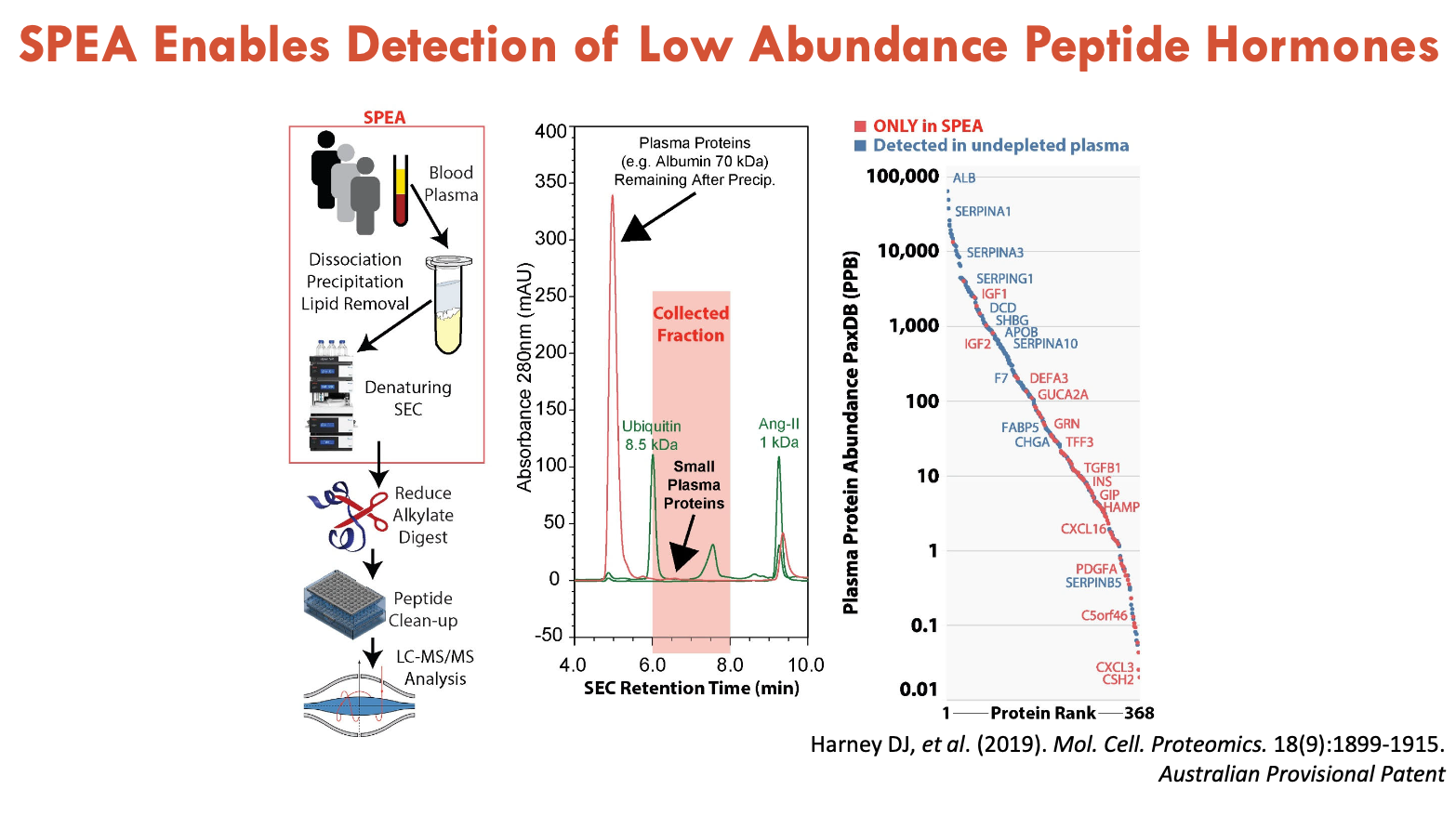
How can blood plasma analysis be used to study human IF?
Plasma proteins have a dynamic range, which presents a problem
instead, focus on the molecular weight of interested proteins
low abundance hormones are mostly low molecular weight
Using small protein enrichment (SPEA) from plasma, it separates proteins by size
enables detection of low abundance peptide hormones
people undergoing IF demonstrated low iron but also had novel peptides
What discovery was made with erusiolin?
Erusiolin antibody staining in the human duodenum (that has enteroendocrine cells secreting GLP-1) revealed that erusiolin increased late after strictly fat consumption
when injecting erusiolin into mice, it lowered food intake
indicates a role in suppressing appetite
Hypothesis: fat regulates erusiolin → regulates nutrient intake (inhibits food intake)
What should be noted about eating behaviours in mice?
They are nocturnal and eat at night
What did proteome analysis reveal of mice undergoing EODF?
Oral glucose tests and DEXA scans were conducted on mice doing EODF; which found that:
liver SERPINA1E (α1-antitrypsin) down 16-fold in response to EODF; SERPINA1E also decreased in mouse EODF plasma
SERPINA1E is a trypsin inhibitor made abundantly by the liver - inhibits proteases in blood
SERPINA1E (α1-antitrypsin) is thought to play a role in regulating LDL/HDL particles
FAoxi was accelerated
EODF caused BHB to be much lower than acutely fasted animals
Beta-hydroxybutyrate (BHB) is the main ketone body that is induced during fasting
What does ACOT2 do in relation to FAoxi?
ACOT2 accelerates FAoxi
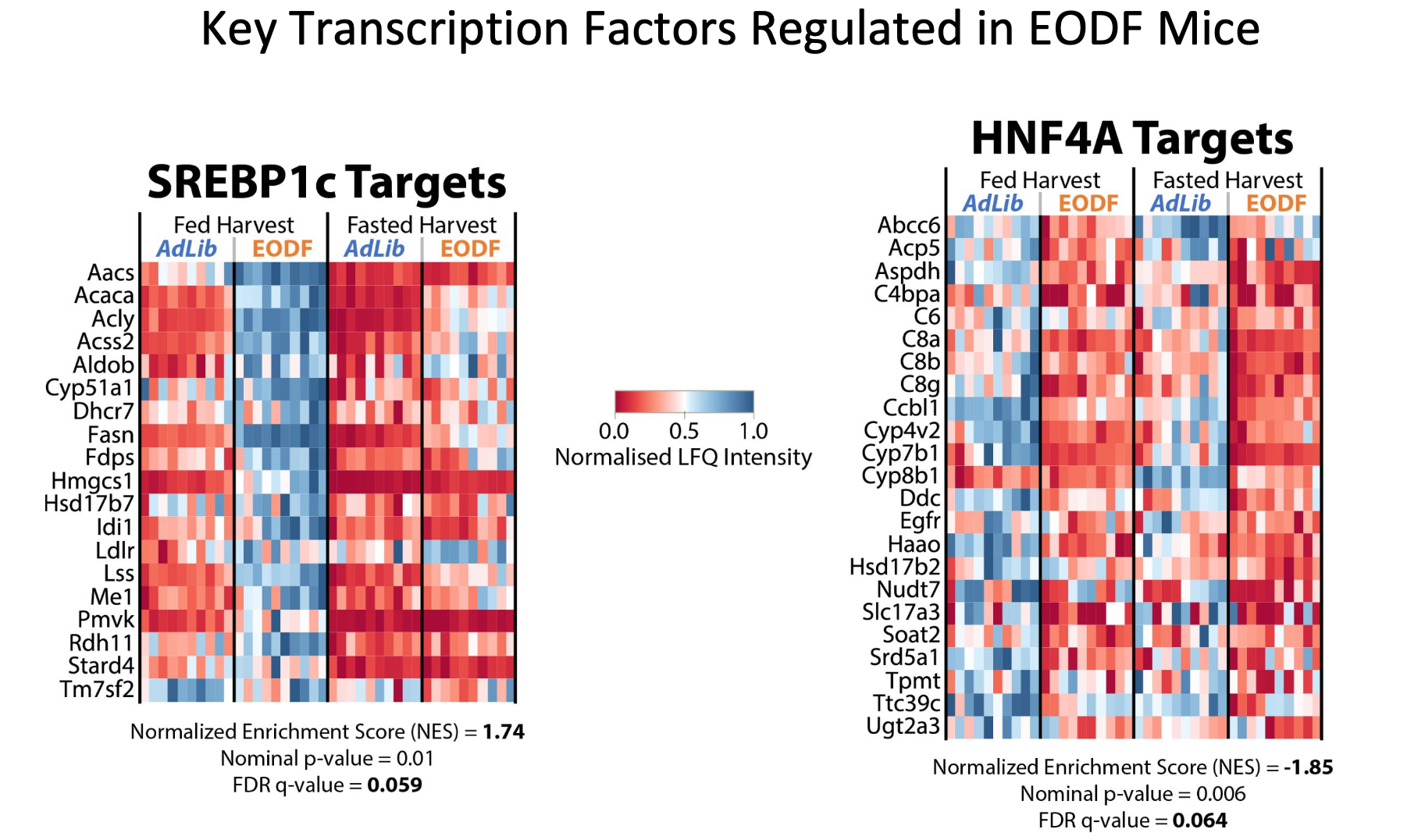
What key TFs are regulated in EODF mice?
SREBP1c and HNF4α are TFs, and their targets are strongly regulated by intermittent fasting.
SREBP1c plays an important role in fat metabolism and FA synthesis (metabolic)
HNF4α regulates a wider array of genes (is downregulated in EODF) - plays a role in specifying the liver differentiation and pancreas differentiation (development)
EOFT alters HNF4α binding to SERPINA1E gene
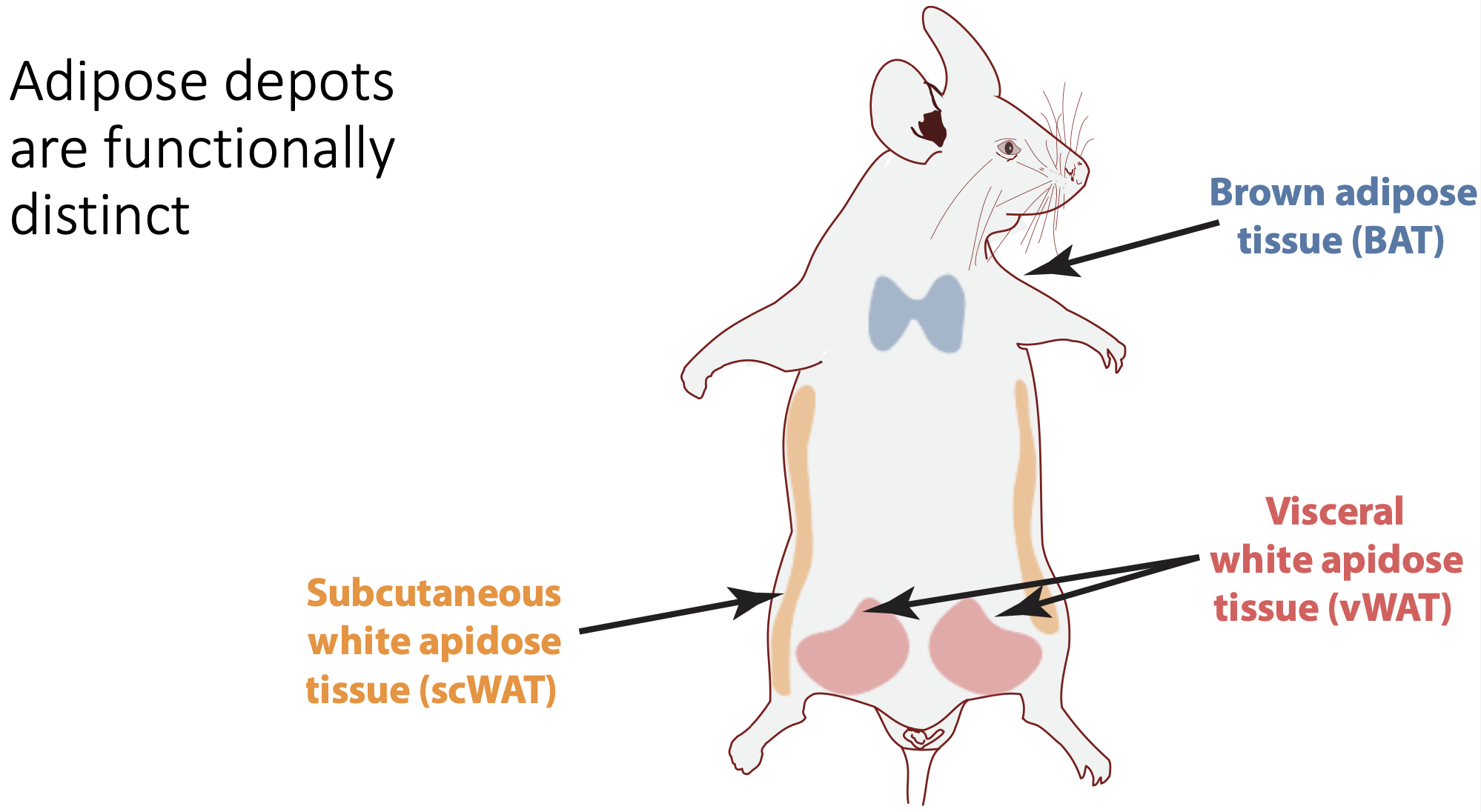
List the 3 types of adipose depots in mice
Brown adipose tissue (BAT) - behind shoulders
Visceral white adipose tissue (vWAT) - near gonads
Subcutaneous white adipose tissue (scWAT)
What was found in proteome analysis on mouse adipose depots during EODF?
Distinct regulations of lipolysis pathways
triggered by binding of Adrenaline/Noradrenaline to ADRB3
ADRB3 (cell receptor) was greatly downregulated in vWAT, but not in scWAT or BAT
therefore, vWAT demonstrates resistance to lipolysis (could be a survival mechanism to retain fat during EODF)
Main finding: EODF reduces the lipolytic potential of vWAT
Describe the sexual dimorphism of the EODF response in mice
Most studies are conducted on male mice, but there are differences between sexes:
Body weight
Fat vs lean mass
However, both sexes are similarly affected by EODF (found on DEXA analysis) in terms of:
oral glucose tolerance test (decrease in AUC → increased sensitivity)
FAs and ketone bodies were both decreased
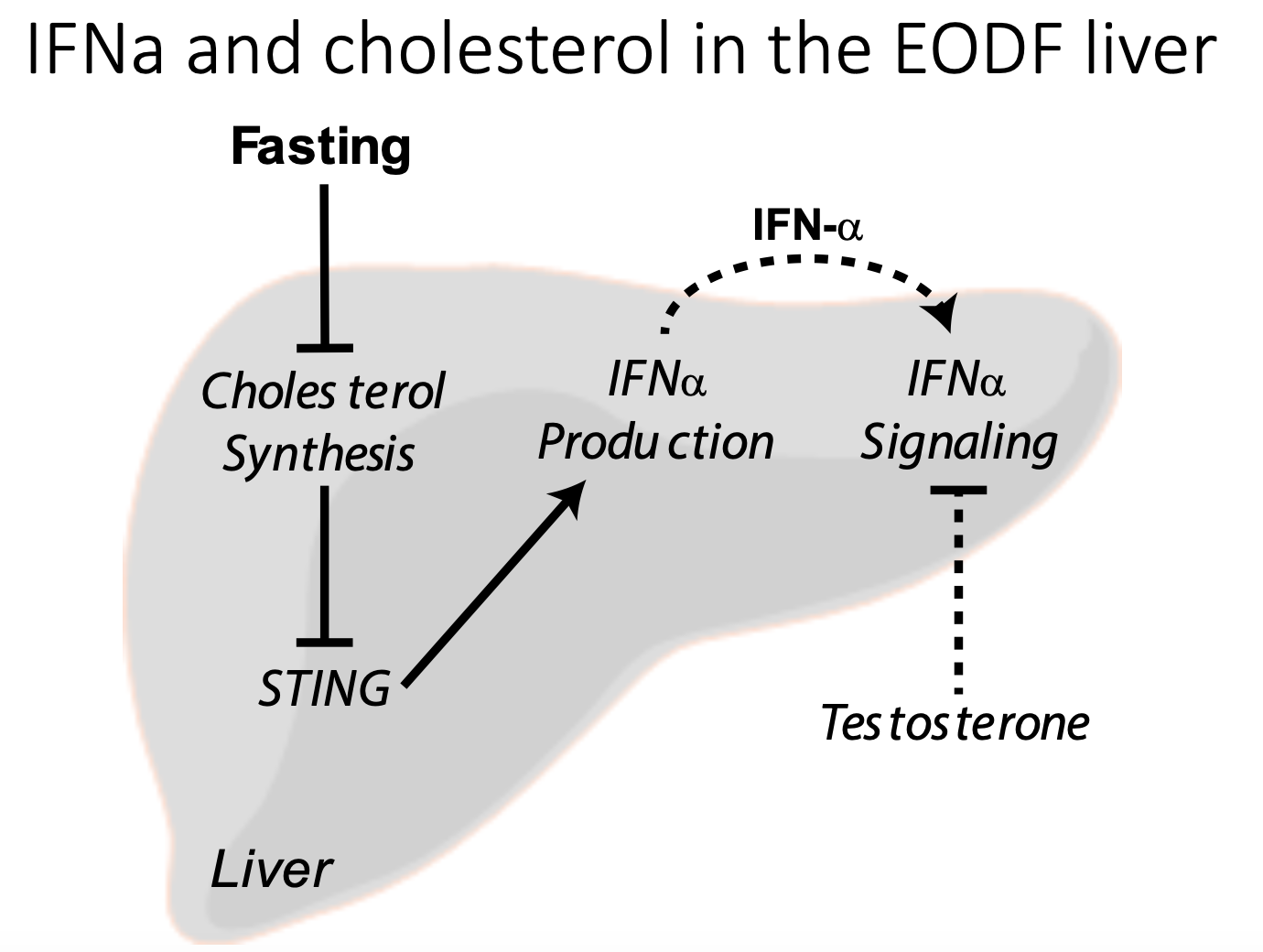
One main difference that was found was:
IFNα (an antiviral cytokine) signalling pathways are increased by EODF in females
may be due to changing cholesterol flux (independent of viral infection) - still a hypothesis
Summarise liver proteomics that can be conducted on EODF mice models
Principal component analysis:
each dot represents a mouse model
placed there based on their entire proteome
Heat map:
shows a normalised abundance of tissues (relative quantification)
Adipocytes are active cells that produce (A - 2), which can people with obesity more susceptible to COVID-19.
Obesity is a state of (B - 2), which (C - consequence), but (D - consequence on COVID testing)
A - adipokines and cytokines
B - chronic and low-grade inflammation
C - alters immune responses
D - has no affect on COVID testing accuracy compared to non-obese
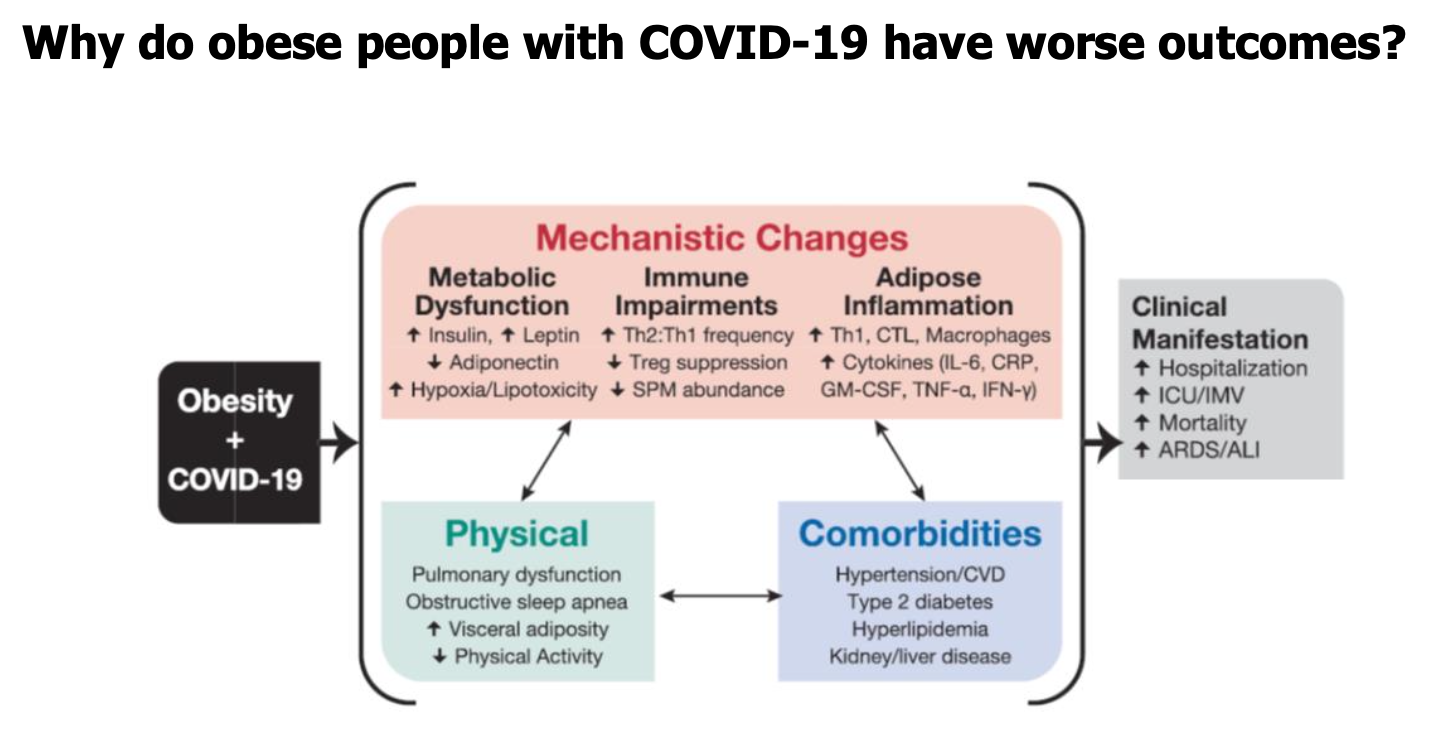
People who are obese have (A - better/worse) outcomes to COVID-19, regarding (B - 3 outcomes).
This could be due to (C - 3 aspects)
A - worse
B - hospital admissions, ICU admissions, and death
C - physical debilitations (e.g. pulmonary dysfunction), comorbidities (e.g. hypertension, CVD, T2D), and mechanistic changes (e.g. metabolic dysfunction, immune impairments, adipose inflammation)
Are people with obesity more infectious with COVID-19?
R0 represents the infectiousness of a singular person
viral load and viral shedding (duration) of COVID-19 is higher in obese than lean people
they take longer to receive a negative test back → are more infectious (should isolate longer)
BUT the data is lacking
Are COVID-19 vaccines as effective in obese people?
Yes, vaccine efficacy is not significantly different in people with or without obesity
What was the impact of COVID-19 on obesity?
There was a slight increase in the average adult weight during the pandemic period of less than 0.5 kg in adults
similarly weight increase was observed in children
Less clinical care was available during COVID-19
obesity treatment was neglected (fewer interventions)
but, virtual care became more common
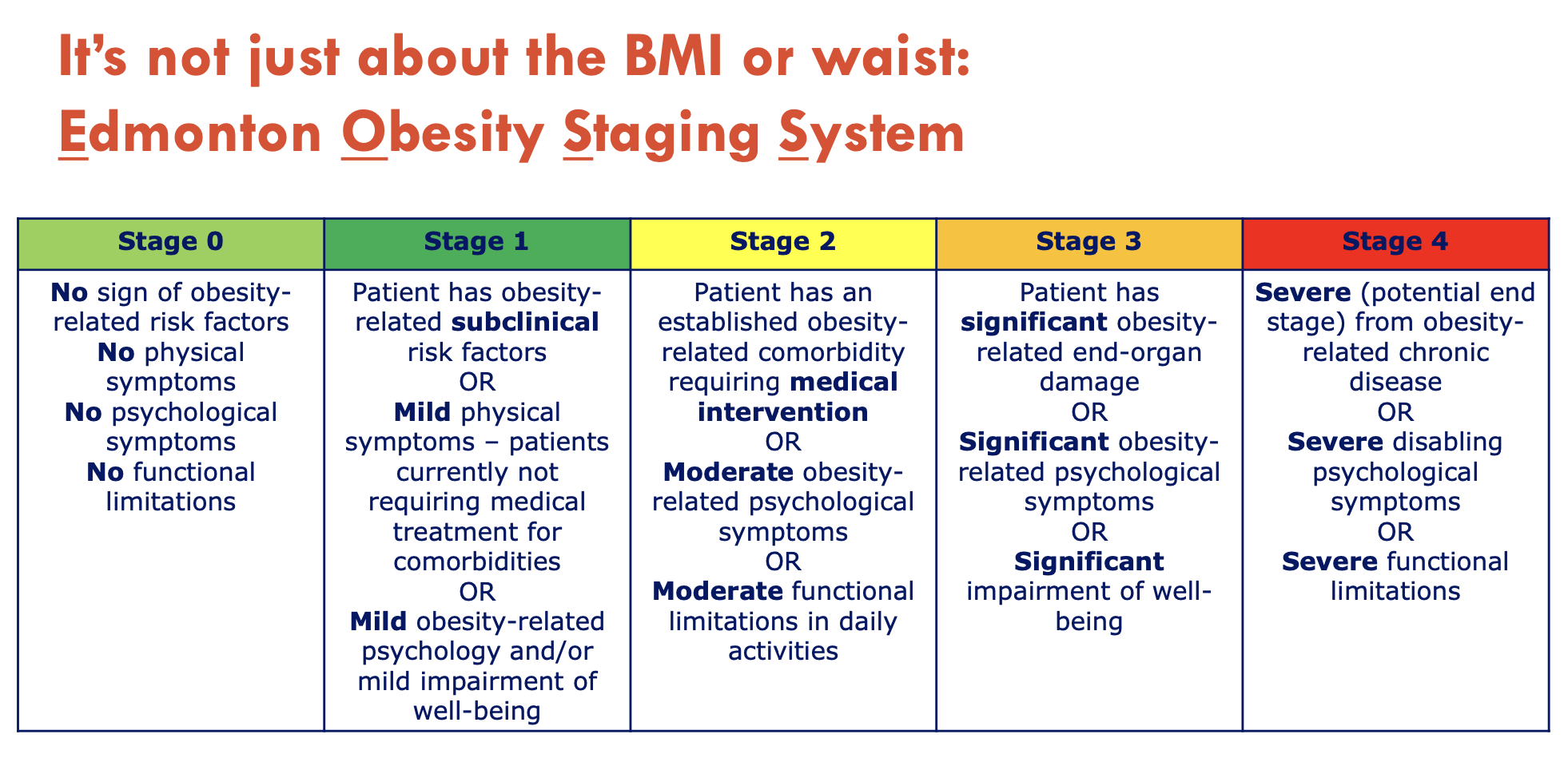
What is the Edmonton Obesity Staging System?
It stages people who have obesity via BMI, but also considers other present diseases - a bettr indicator of mortality
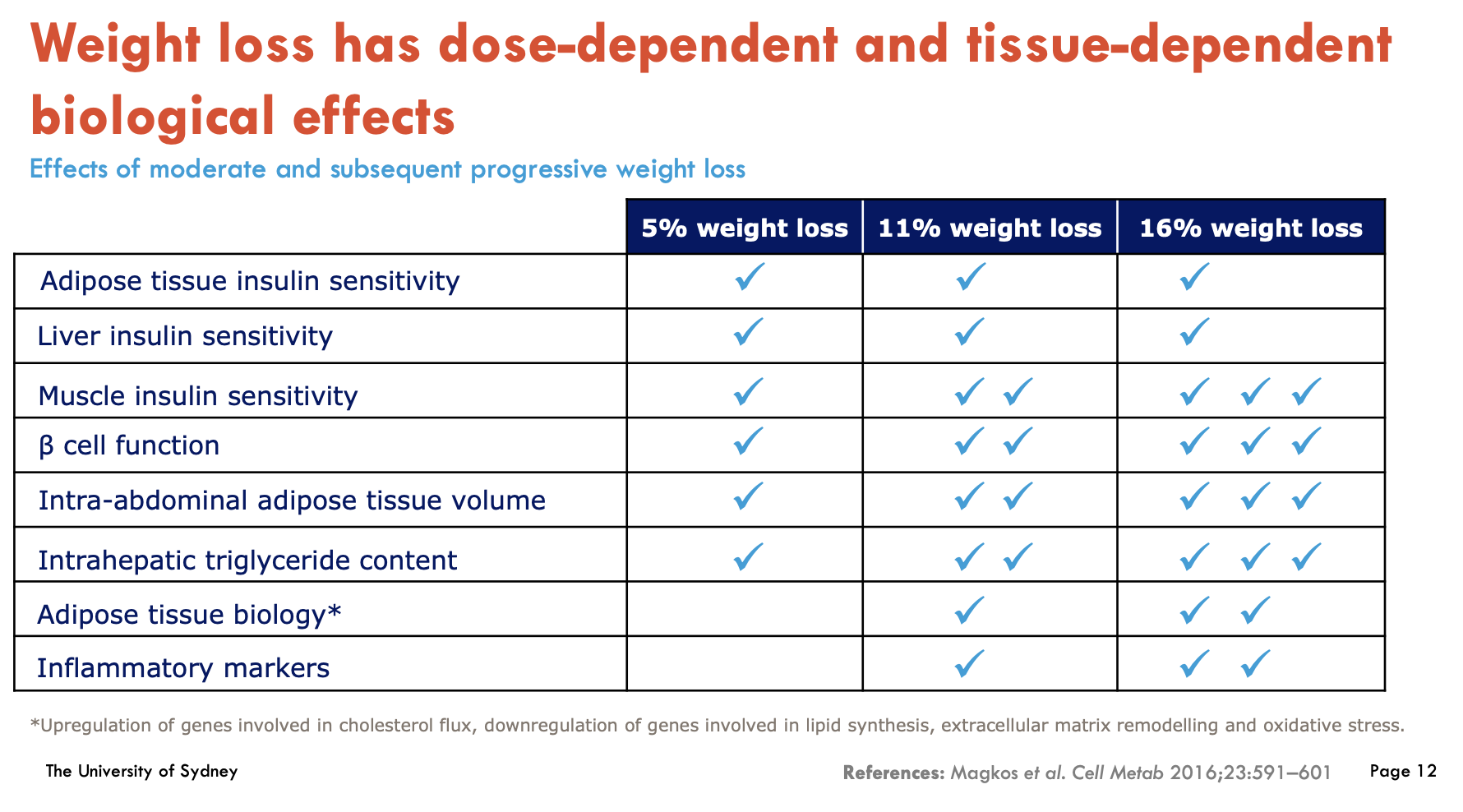
Weight loss produces disproportionately greater loss of (A - 2 tissues), which improved starting at (B - %) weight loss and maximally at (C - %) weight loss. After that, excessive weight loss can lead to remission of (D - condition)
A - Intra-abdominal and liver adipose tissue
B - 5%
C - 16%
D - Type 2 Diabetes
How is pharmacotherapy used to treat obesity?
Pharmacotherapy for obesity targets appetite regulation in the brain
is required for weight loss maintenance
In Australia, only 4 anti-obesity medications are available:
Orlistat: inhibits intestinal lipase to reduce fat absorption
Phentermine: sympathomimetic amine, suppresses appetite
Liraglutide 3.0 mg: GLP-1 analogue, central action to reduce hunger
Naltrexone / Bupropion: anti-addiction therapies, central action to reduce hunger and cravings
What is the safety and tolerability of Orlistat?
oral medication given 3x daily
perceived as a safer option due to its peripheral mechanism of action in the intestinal lumen instead of the brain
unpleasant GIT side effects (oily stools)
rare cases of severe liver injury; potential risk of kidney injury, pancreatitis and renal stones
What is the safety and tolerability of Phentermine?
oral medication given once daily (15/30/40 mg)
cardiovascular side effects: hypertension and tachycardia
dry mouth and headache
CNS side effects: insomnia, restlessness, alters sexual behaviour, hormonal secretion, and mood
What is the safety and tolerability of Liraglutide 3.0?
subcutaneous injection (0.6-3.0 mg once daily)
GIT side effects;
nausea, vomiting, constipation, diarrhoea
gall-bladder-related events
stopping rule if insufficient weight loss after 3 months on max. dose
What is the safety and tolerability of Naltrexone + Bupropion?
oral medication given 2x a day
titrate from 1 to 4 tablets with weekly dose increases
Contradictions: chronic opioid usage, seizure disorder, HT, bipolar disorder, severe hepatic impairment, severe renal impairment
side-effects:
nausea, vomiting, constipation
headache
incomnia
dry mouth
stopping rule if sufficient weight loss after 16 weeks (50% responder rate)
Bariatric surgery is associated with sustained weight loss over (A - duration) and have effects on (B - type of hormones). As a result, people with bariatric surgery experience (C - side effect), which requires combination of (D - action).
A - 15 years
B - incretin hormones
C - nutrient deficiency
D - lifestyle modification
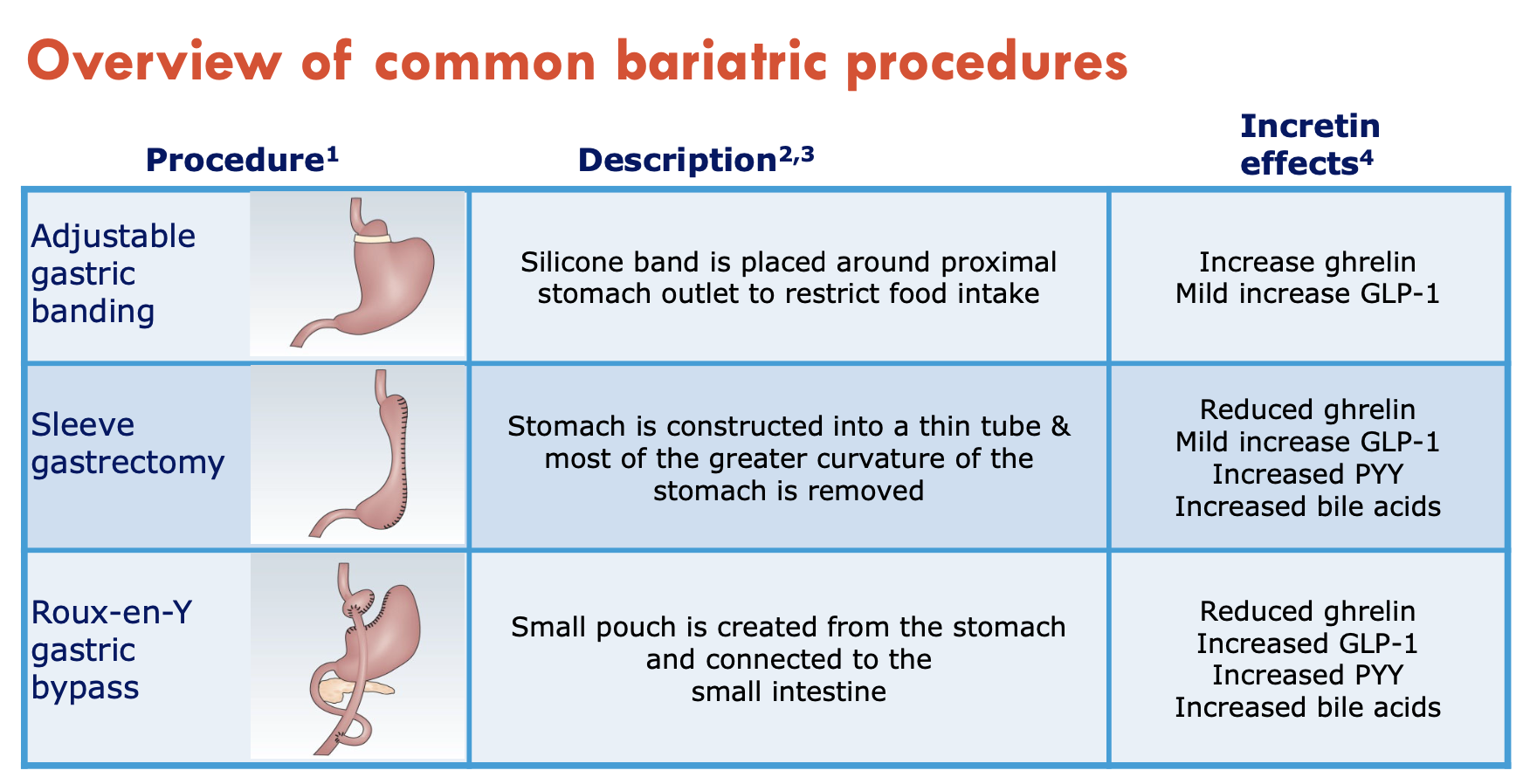
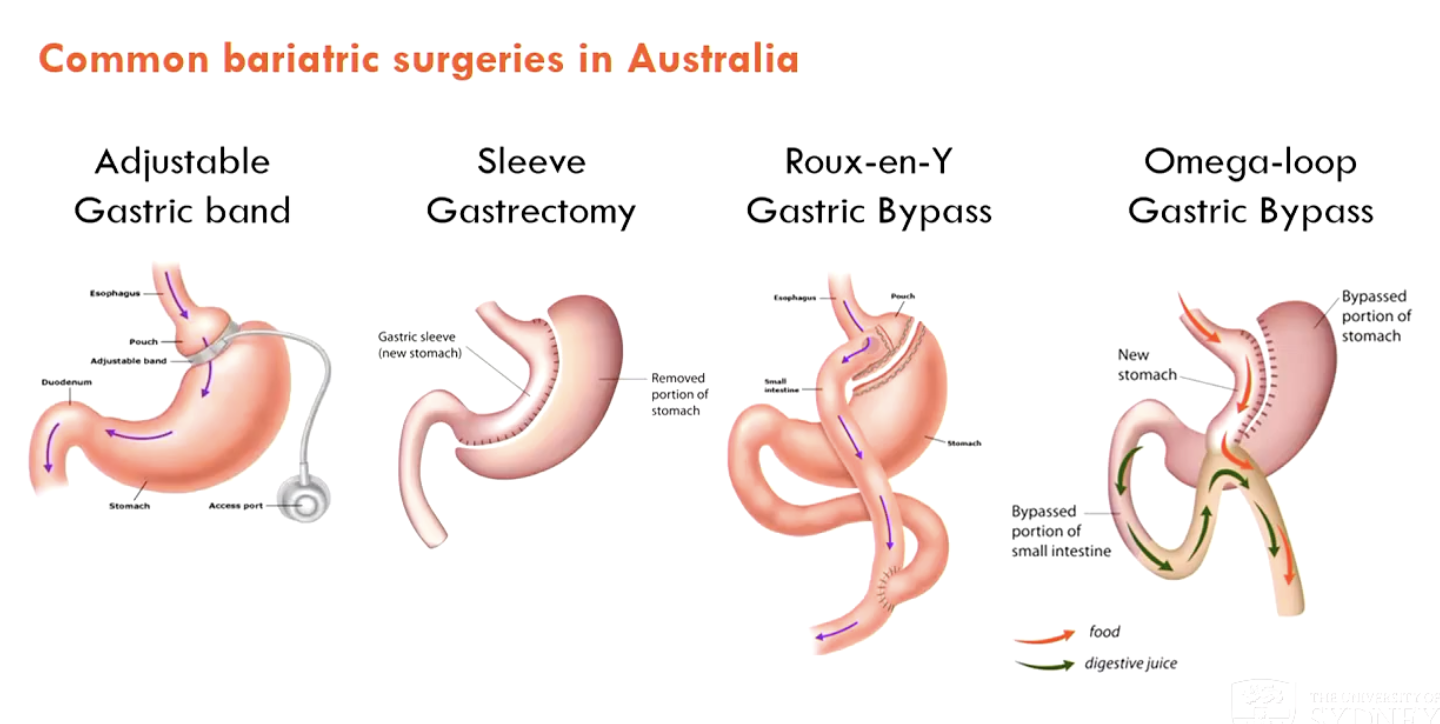
What are the common bariatric surgeries in Australia?
Adjustable gastric band (not preferred)
Sleeve gastrectomy (common in Aus)
Roux-en-Y gastric bypass
Omega-loop gastric bypass