C. diff- Morelli- (Morelli)
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
What is the BIGGEST risk factor for C.diff?
antibiotic use
What abx have the HIGHEST risk of causing C.diff?
CLINDAMYCIN
3rd gen cephalosporins
fluoroquinolones
lower risk: SMX/TRM, tetracyclines, aminoglycosides
What’s another class of drugs, not abx, that have been associated with C.diff?
PPIs
Recurrent CDI generally occurs within __ weeks of initial treatment.
8
What is the clinical presentation of C.diff? in severe cases?
nearly always limited to the colon
symptoms range from asymptomatic—> life-threatening
diarrheal illness
in severe cases—> ileus, TOXIC megacolon, pseudomembranous colitis
What 2 toxins are produced by C.diff that are responsible for inflammation, fluid, and mucosal damage? Which is MORE potent?
Toxin A and B
Toxin B—> 1000 times more potent
For diagnosing CDI, who do we test?
a. asymptomatic
b. symptomatic
c. both
b

What LAB tests can diagnose CDI?
Nucleic Acid Amplification Tests (NAAT)
Enzyme immunoassay (EIA) for C. dif glutamate dehydrogenase
Enzyme immunoassay (EIA) for C. dif toxins A and B
anaerobic culture
Differentiate the following:
NAAT
EIA for GDH
EIA for Toxins A and B
anaerobic culture
(IDK HOW IMPORTANT!!!!!!!!)
NAAT
highly sensitive
not capable of differentiating asymptomatic carriers
EIA for GDH
not capable of differentiating toxic from nontoxic strains
useful initial screening step
EIA for Toxins A and B
used with GDH and NAAT
Anaerobic culture
too slow for clinical use
not capable of differentiating toxic from nontoxic strains
What are the infection Control Measures for CDI?
HAND HYGIENE
soap and water
CONTACT precautions
gloves AND gown must be worn when entering room
use cleaning agents Cl- or sporicidal
What are the severity classifications of CDI?
Classification | Clinical Presentation |
Non-severe | |
Severe | |
Fulminant |
MUST KNOW THIS—> MUST KNOW THIS !!!!!!!!!!!!!
Classification | Clinical Presentation |
Non-severe | WBC ≤ 15,000 cells/ml AND SCr <1.5 mg/dL |
Severe | WBC > 15,000 cells/ml OR SCr ≥ 1.5 mg/dL |
Fulminant |
|

WHAT IS THE 1st LINE TREATMENT FOR CDI?
FIDAXOMICIN
VANCOMYCIN PO
WHAT is the treatment for CDI based on severity?
(sadly, MUST KNOW, said in lecture, “spend most of your time on this”)
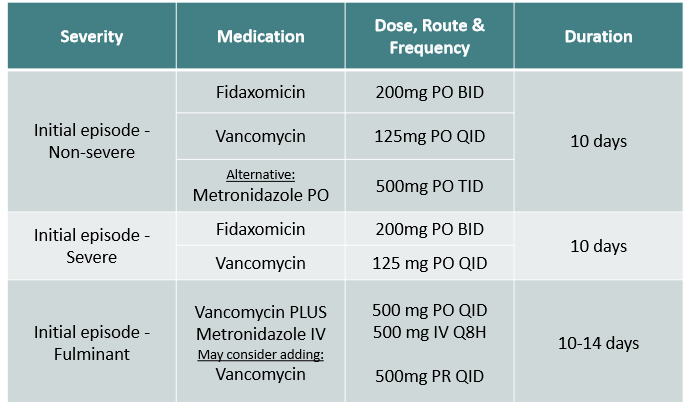
initial episode non-severe
initial episode severe
initial episode fulminant
initial episode non-severe
Fidaxomicin 200mg PO BID, 10 days
Vancomycin 125mg PO QID, 10 days
Alternative: Metronidazole 500mg PO TID, 10 days
initial episode severe
Fidaxomicin 200mg PO BID, 10 days
Vancomycin 125mg PO QID, 10 days
initial episode fulminant
Vancomycin + Metronidazole IV ± Vancomycin PR (rectum)
Vancomycin 500mg PO QID, 10-14 days
Metronidazole 500mg IV q8h, 10-14 days
Vancomycin 500mg PR QID, 10-14 days
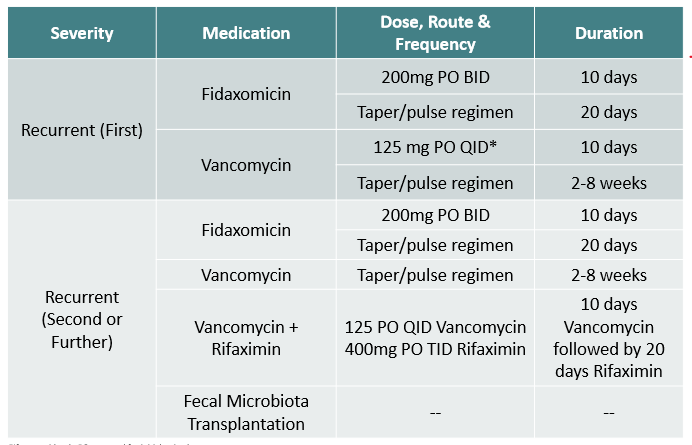
What is the treatment for CDI for recurrent severity?
i wouldn’t memorize —> in lecture said “know all different options, just don’t do what you previously did”
Disadvantage of Fidaxomicin?
Expensive!!!
Vancomycin is the DOC in what?
fulminant CDI
pregnancy
True or False: IV vancomycin is effective against C. dif?
false
What are some alternative options for CDI? (only used in select circumstances)
metronidazole
rifaximin
fecal microbiota transplant
Live biotherapeutic products
surgery

When is Metronidazole used PO v. IV?
ALTERNATIVE OPTION
PO= non-severe infections
IV= used in combo with PO vancomycin for fulminant infections

What is Fecal Microbiota Transplant (FMT)? When is it considered?
transfer of fecal material from healthy donor to the infected individual to restore microbiome
considered after at least 2 recurrences or refractory CDI
What are 2 live biotherapeutic products (LBPs) used as alternative options for CDI? (only in recurrent CDI, so $$)
Rebyota and Vowst
Is Bezlotoxumab indicated for treatment of CDI?
NO!!!—> removed from the market janurary 2025
was indicated to reduce recurrence of CDI in pts. 18 or older who are receiving antibacterial drug tx of CDI, and are at high risk of recurrence
AGAIN… REMOVED FROM THE MARKET
What product is associated with decreased CDI recurrences and can be used for prevention?
PROBIOTICS!!!—> S. boulardii
___________ is an OTC product that contains S. boulardii.
Florastor
“I was just discharged from the hospital and am finishing up medications for C. diff. Should I go back to my doctor to have my stool retested?”
How would you respond to this?
once diagnosed—> no value in retesting stool
pt. continues to shed toxin
Should pts. with C.diff take anti-peristaltic agents like Loperamide or Diphenoxylate and atropine to help decreases diarrhea?
NO!!!!!!!!!!!!!! AVOIDDDDDDDDD