Orthodontic Diagnosis (Classification of Malocclusion)
1/76
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
77 Terms
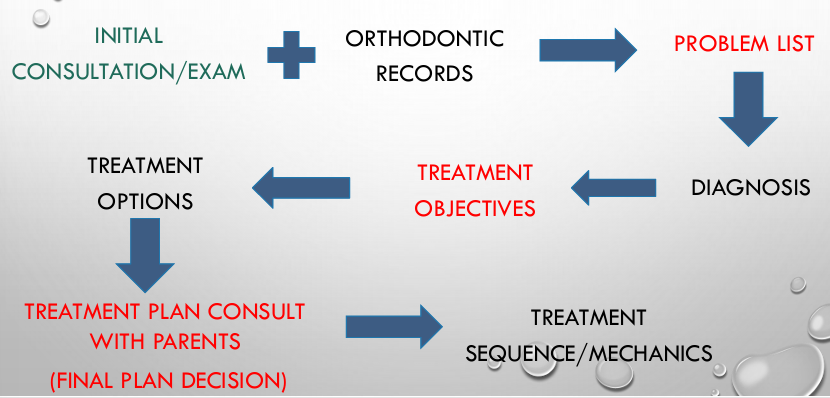
orthodontic diagnostic process
why do we need to classify malocclusion?
-morphological deviations from the norm can be compiled into a problem list which is essential for orthodontic diagnosis and treatment planning
initial consultation/exam- interview with patient/parent/guardian
-important to let patient talk (watch for helicopter parents) → get them to say something so you can assess speech
1) chief complaint- why are they seeking orthodontic treatment
2) medical history- medications, heart conditions, facial skeletal fractures, etc.; not too many conditions are ortho contraindications
3) dental history- history of prior trauma/extractions, previous ortho tx, habits
4) **growth potential- menarche for girls, secondary sexual characteristics for boys
5) behavioral issues- motivations for treatment, psychosocial problems (may need intervention, but emotionally can’t handle it)
6) respiratory assessment- snoring, tired during the day, often diagnose OSA
initial consultation exam- general dental exam
1) oral hygiene- look for presence of plaque, calculus, and gingivitis (hygiene gets harder with ortho appliances)
2) periodontal assessment- recession, gingival defects; very important on adult patients→get these under control first
3) TMJ and occlusion assessment- functional shifts, TMD symptoms, deviation on closing → get these under control first
4) speech and breathing- lisps, tongue thrust upon swallow or speaking, airway obstructions
after an initial assessment, the main questions an orthodontist considers are:
-is the patient ready for orthodontic intervention? (emotionally, too early, too late)
-what type of intervention is necessary at this age/development of dentition
orthodontic records
-standard of care:
-intraoral/extraoral photographs
-diagnostic models/scans
-radiographs
-analysis of all these records will classify our malocclusion and lead us to our diagnosis
standard orthodontic composite
-facial: profile view, frontal (full face) at rest, frontal (full face) with natural smile
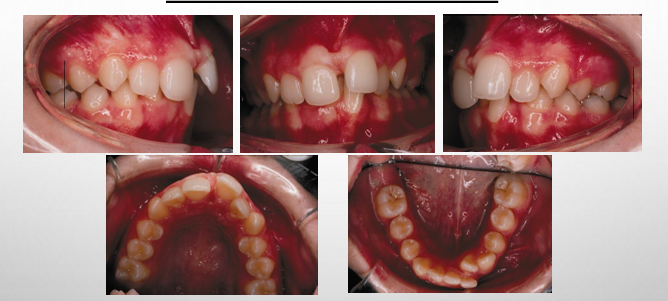
-dental: upper occlusal, lower occlusal, right buccal in occlusion, front occlusion, left buccal in occlusion
model analysis
-has a lot of the same information as the photos with a couple key exceptions:
1) space analysis can be done because the widths of the teeth can be measured
2) the occlusion can be viewed from the lingual as well as the buccal
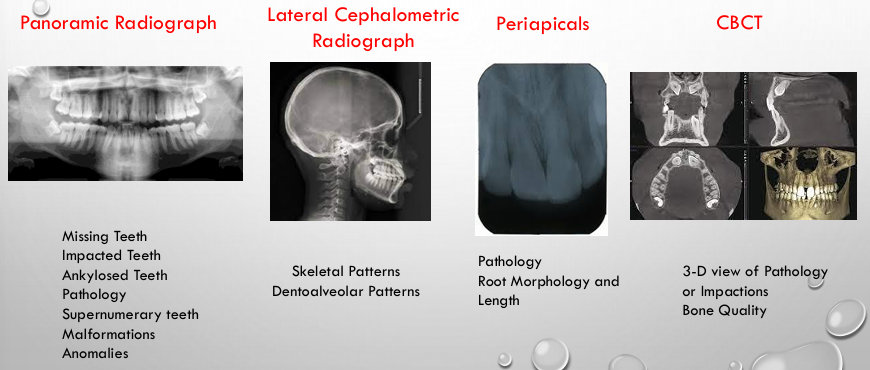
orthodontic records radiographs
-standard of care: pan, lateral ceph
-CBCT, periapicals if indicated (not for all patients)
panoramic radiographic analysis- things to look for
1) pathology
2) root resorption
3) absence of dentition
4) retained primary dentition
5) supernumerary teeth
6) presence of third molars
7) general periodontal assessment
8) condylar shape/resorption
9) root form and parallelism
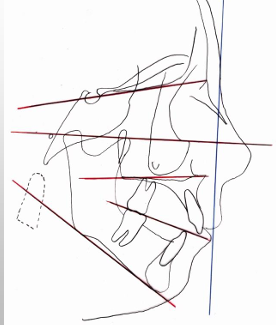
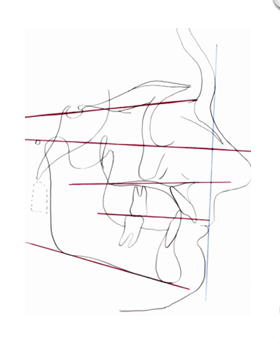
lateral ceph analysis- radiographic analysis
-allows us to see how much of the skeleton is involved in the malocclusion
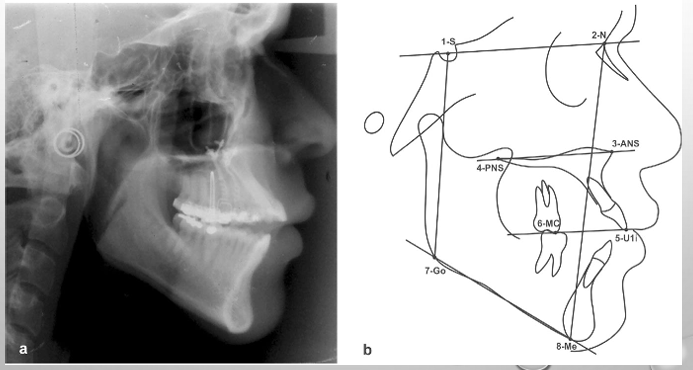
lateral ceph
-used to determine skeletal positions of maxilla and mandible in relation to each other and the cranial base
-used to determine dentoalveolar positions
-used to determine vertical dimensions of maxilla and mandible
diagnosis categories
-facial and profile analysis
-dental analysis
-radiographic analysis
-intraoral exam
orientation planes
-first we need to establish planes of reference in order to identify and communicate which dimension our problem lies
sagittal (A/P) plane
-aka median plane
-an imaginary plane that passes longitudinally through the middle of the head and divides it into right and left halves
-used to describe anterior-posterior relationships

frontal plane
-aka vertical plane
-an imaginary plane that passes longitudinally through the head perpendicular to the sagittal plane dividing the head into front and back
-used to describe superior-inferior relationships
transverse plane
-aka horizontal plane
-an imaginary plane that passes through the head at right angles to the sagittal and frontal planes dividing the head into upper and lower halves
-used to describe right to left relationships
development of a problem list
facial and profile analysis
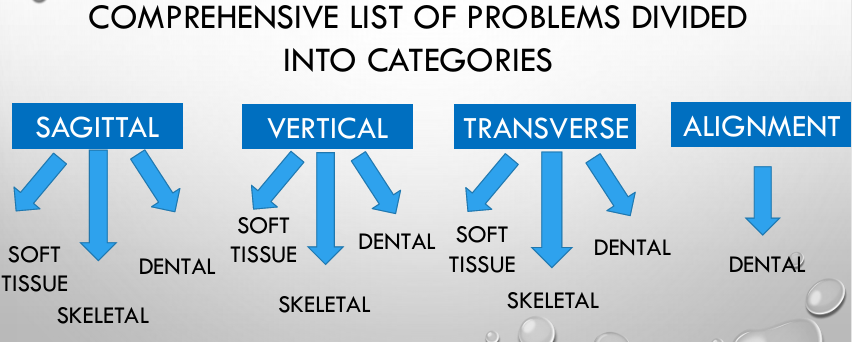
-3 categories to assign dental analysis findings: sagittal (A/P), vertical, transverse
facial profile
-sagittal (A/P plane)- use the profile photo
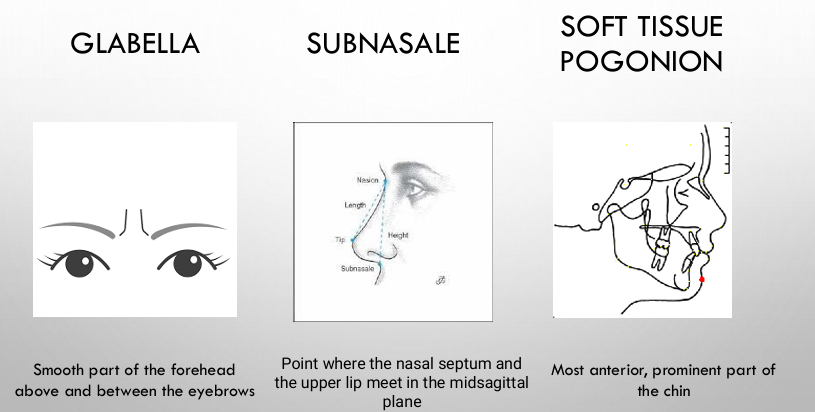
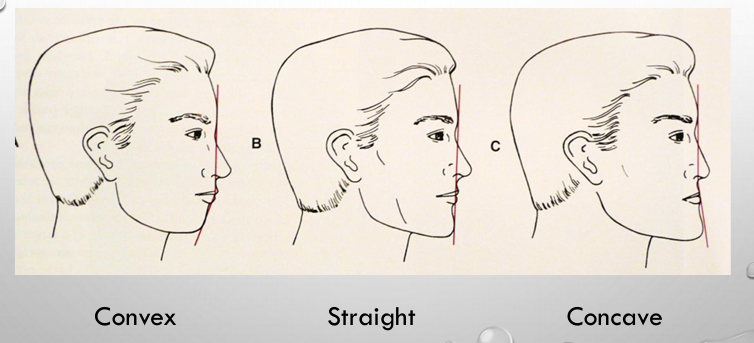
-profile facial view used to evaluate the nose, chin, lips, and facial convexity by drawing a line connecting glabella to subnasale to soft tissue chin
-3 types of facial convexity: convex, straight, concave
-treat to a balanced profile (one type of convexity is not ideal over others!)
facial analysis- profile view
nose descriptions
-large, average, small
-upturned, normal, droopy
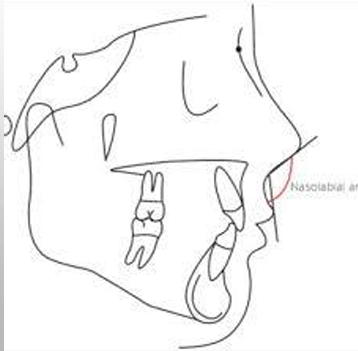
nasolabial angle (NLA)
-angle formed by the upper lip and the nose
-recorded as: normal (90 degrees), acute, obtuse
lip profile
-described as:
-retrusive, normal, or protrusive
-full, average, or thin
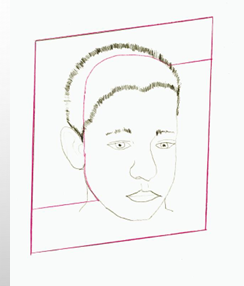
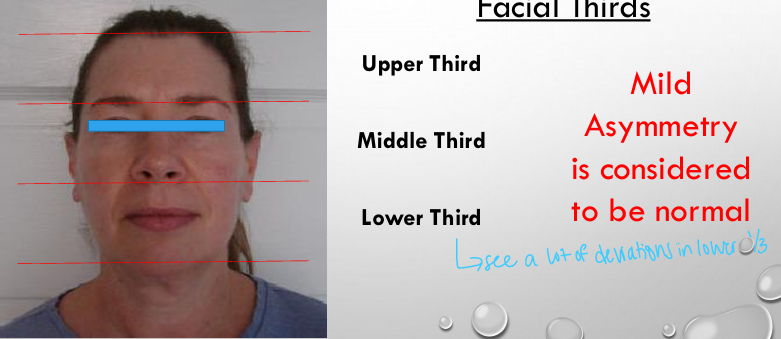
facial analysis- frontal view
-frontal (vertical) plane- use the frontal photos
-assess: facial proportions, lip competence, asymmetries, lip strain
facial analysis- frontal view: facial thirds
lip competence
-ability of the patient to have the lips contacting in the rest position without showing mentalis muscle strain
-lip incompetence: inability of the patient to have the lips contacting in the rest position without showing muscle strain or can’t fully close lips over teeth (have muscle strain when fully closed)

lip/smile lines
-lip line: amount of tooth and/or gingival tissue that is exposed at rest, recorded as percentage of tooth showing
-smile line: amount of tooth and/or gingival tissue exposed upon smiling, recorded as percentage of tooth showing, if there is gingival show, would be 100% of incisal display PLUS the amount of gingival showing in mm
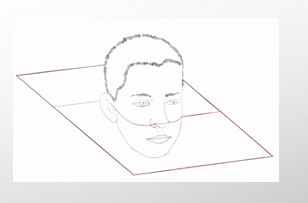
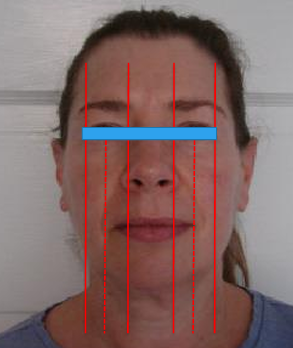
facial analysis- profile view
-transverse plane- use the frontal photos
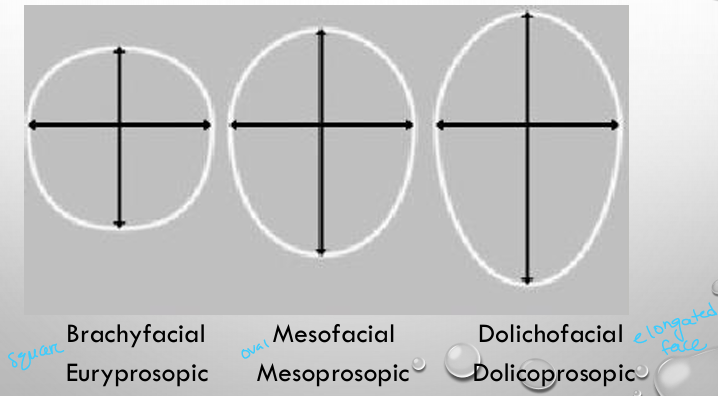
brachycephalic/brachyfacial
-brachycephalic: an individual with a larger than average cranial width and usually presents with a broad, square head shape and low mandibular plane angle
-brachyfacial: an individual characterized by a broad square face with a strong chin, flat lip posture, and a low mandibular plane angle

dolicocephalic/doliofacial
-dolicocephalic: an individual that has a narrower cranial width and usually presents with a long, narrow shape and high mandibular plane angle
-dolicofacial: an individual that has a long, narrow face with a high mandibular plane angle, convex profile, poor chin development, and an anterior-posterior face height imbalance

mesocephalic/mesofacial
-mesocephalic: an individual that falls between the brachycephalic and dolicocephalic types and has an average cranial width
-mesofacial: an individual who has well balanced facial features

transverse facial analysis- facial fifths
-mild asymmetry is considered to be normal
dental (model) analysis
-4 categories to assign dental analysis findings:
1) sagittal (A/P)
2) vertical
3) transverse
4) alignment
intraoral exam- sagittal
-use the buccal photos and diagnostic models
-molar/posterior segment relationship (class I/II/III)
-overjet
-anterior crossbiteA
Angle classification
-classifications based on the relationship of the MB cusp of the maxillary first molar and the buccal groove of the mandibular first molar
-if this molar relationship exists, then the teeth can align into normal occlusion (ideal overbite and overjet in absence of other mal-occlusive anomalies)
-treat to class I
normal occlusion
-MB cusp of the maxillary first molar is aligned with the buccal groove of the mandibular first molar
-there is alignment of the teeth, normal overbite and overjet, and coincident maxillary and mandibular midlines

class I malocclusion
-a normal molar relationship exists but there is crowding, misalignment of the teeth, crossbites, etc.
class II malocclusion
-most common
-a malocclusion where the molar relationship shows the buccal groove of the mandibular first molar distally positioned when in occlusion with the mesiobuccal cusp of the maxillary first molar
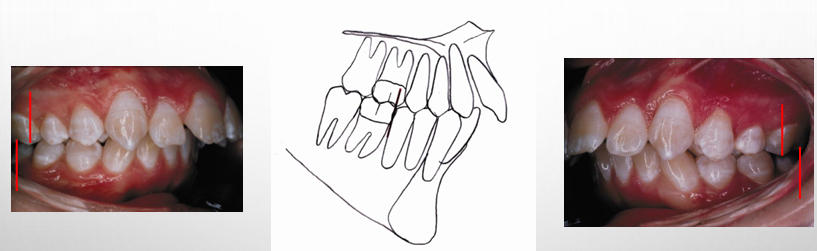
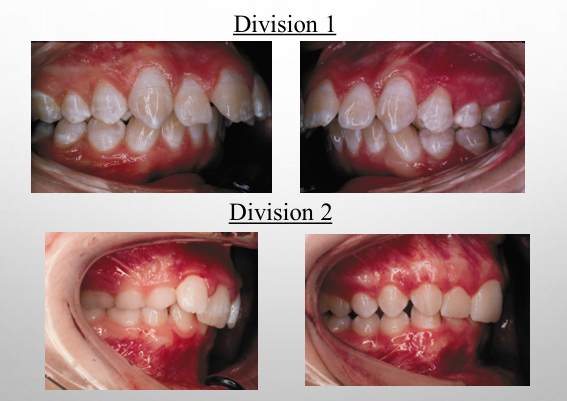
2 divisions of class II malocclusion
-class II division 1: maxillary anterior teeth are proclined and a large overjet is present
-class II division 2: maxillary anterior teeth are retroclined and a deep overbite exists
Class II malocclusion subdivisions
-class II division 1, subdivision RIGHT: maxillary anterior teeth are proclined and a large overjet is present but the class II molar relationship is only present on the right (indicates left is class I occlusion)
-class II division 1, subdivision LEFT: maxillary anterior teeth are proclined and a large overjet is present but the class II molar relationship is only present on the left
-class II division 2, subdivision RIGHT: maxillary anterior teeth are retroclined and a deep overbite exists but the class II molar relationship is only present on the right
-class II division 2, subdivision LEFT: maxillary anterior teeth are retroclined and a deep overbite exists but the class II molar relationship is only present on the left
class III malocclusion
-malocclusoin where the molar relationship shows the buccal groove of the mandibular first molar mesially positioned to the MB cusp of the maxillary first molar when the teeth are in occlusion
anterior tooth postitions- overjet
-everybody has an overjet → can be +, zero, or -
-term used to describe the distance between the labial surfaces of the mandibular incisors and the incisal edge of the maxillary incisors
-recorded in mm
-measured clinically on patient (best), on models or on lateral ceph (ruler is there)
-photos are NOT good to use for overjet
anterior crossbite
-a mal-relation between the maxillary and mandibular teeth when they occlude with the antagonistic tooth in the opposite relation to normal
-anterior crossbites can be single tooth or full anterior crossbite involving all the incisors
-***must specify which teeth are involved
intraoral exam- vertical
-frontal (vertical) plane- use the frontal photos
-overbite
-open bite
-occlusal cants
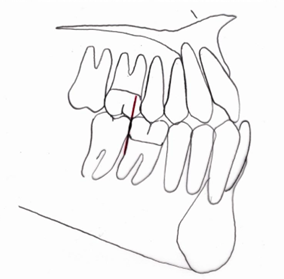
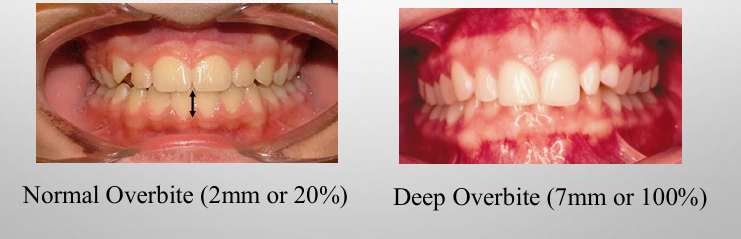
overbite
-the amount of overlap of the mandibular anterior teeth by the maxillary anterior teeth measured perpendicular to the occlusal plane
-recorded in mm or percentage of lower incisor coverage (percentage preferred)
-coverage could be buccally
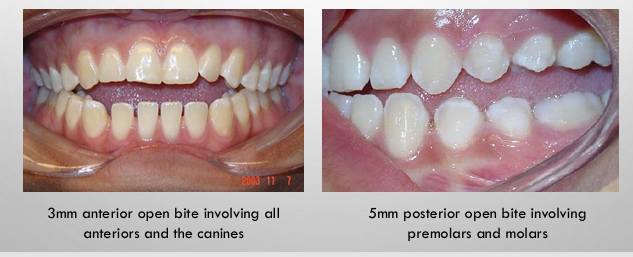
open bite
-present when there is no vertical overlap of the maxillary and mandibular anterior teeth or no contact between the maxillary and mandibular posterior teeth
-recorded as mm between incisal edges of maxillary and mandibular teeth
-can also record as negative overbite (i.e. -5mm overbite)
ankylosis
-fusion between the teeth and the alveolar bone
-ankylosed teeth do not erupt with the vertical growth of the patient and are seen in the infraversion position
intraoral exam- transverse
-transverse plane- use the frontal and buccal photos
-posterior crossbites
-midline analysis: coincidence with each other, coincidence with face
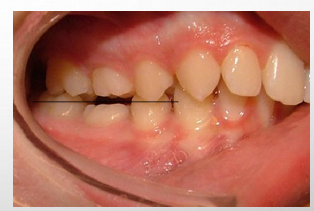
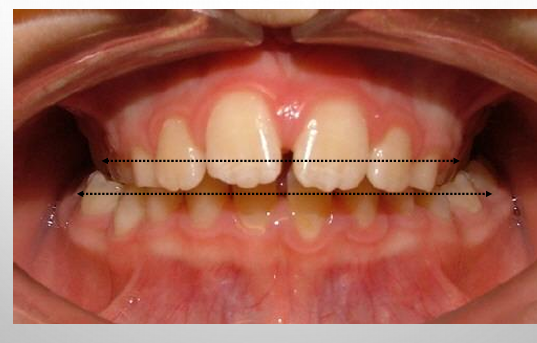
posterior crossbites
-present when posterior teeth occlude in an abnormal buccolingual relation with the antagonistic teeth
-can be result of either malposition of a tooth or teeth, and/or the skeleton
-examining the transverse dimension allows us to evaluate the intermolar and intercanine widths and determine which arch is the offending unit
-posterior crossbites can be unilateral or bilateral
-a functional crossbite results from an occlusal interference that requires the mandible to shift either anteriorly and/or laterally in order to achieve maximum occlusion
descriptive crossbite terms
-buccal crossbite: buccal displacement of the affected posterior tooth or teeth as it relates to the antagonistic posterior tooth or teeth
-lingual crossbite: lingual displacement of the mandibular affected tooth or teeth as it relates to antagonistic tooth or teeth
-palatal crossbite: palatal displacement of the maxillary affected tooth or teeth as it relates to the antagonistic tooth or teeth
-complete crossbite: when all the teeth in one arch are positioned either inside or outside to all the teeth of the opposing arch
-brody bite: complete buccal crossbite (the maxillary posterior teeth are completely buccal to the mandibular posterior teeth)
midline assessments
1) maxillary midline to facial midline
2) intermaxillary midline
3) mandibular midline to facial midline
intermaxillary dental midline
-maxillary dental midline: a line drawn perpendicular to the maxillary occlusal plane through the proximal contacts of the central incisors
-mandibular dental midline: a line drawn perpendicular to the mandibular occlusal plane through the proximal contacts of the central incisors
-if deviation- must say what direction and by how much

facial and dental midlines
-maxillary midline to facial midline: determine if maxillary midline lines up with facial midline
-mandibular midline to facial midline: determine if mandibular midline lines up with facial midline
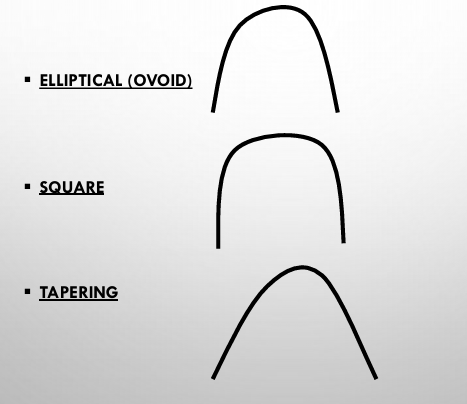
arch form
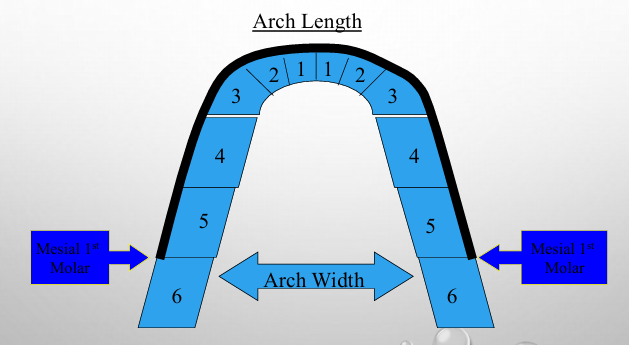
arch forms
intraoral exam- alignment
-crowding
-spacing
-rotations
-diastemas
crowding
-when the available space in the FULL ARCH is less than the space required to align the dentition
-crowding is described as mild, moderate, or severe:
-mild: 1-3mm
-moderate: 4-7mm
-severe: 8+mm
spacing
-when the available space in the FULL ARCH is more than the space required to align the dentition
-spacing described as mild, moderate, or severe:
-mild: 1-3mm
-moderate: 4-7mm
-severe: 8+mm
diastemas
-can be maxillary or mandibular
-if a diastema is present, it should be measured and reported in mm
-midline space
terms used to describe the position of teeth
-mesioversion: tooth in the arch located more mesial than normal
-distoversion: tooth in the arch located more distal than normal
-labioversion: an incisor or canine outside of arch towards the lips
-buccoversion: a posterior tooth outside the arch toward the cheek
-linguoversion: tooth inside the arch form toward the tongue
-infraversion: tooth that has not erupted to the occlusal plane
-supraversion: tooth that has over-erupted
-torsiversion: tooth rotated on its axis
-transversion (transposition): teeth that are in the wrong sequential order
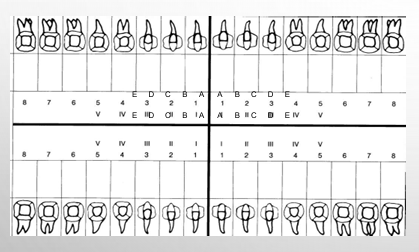
dental status
-use photos and pan
-identify teeth clinically present by circling the number or letter
-identify missing teeth (those not present clinically AND not present in the radiograph) by placing an “X” in the box
-identify impacted teeth by putting an “I” in the box
-identify unerupted teeth by putting a “U” in the box
intraoral soft tissue analysis- periodontal status/oral hygiene
-use photos and pan
-note the following:
-periodontal involvement based on alveolar bone loss on radiograph
-furcations on radiograph
-gingiva: recession, color of gingiva
-oral hygiene: recorded as good, poor, or fair
frenum attachments- maxilla
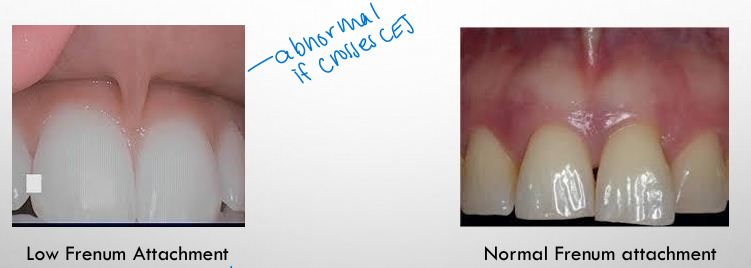
frenum attachments- mandible

radiographic analysis
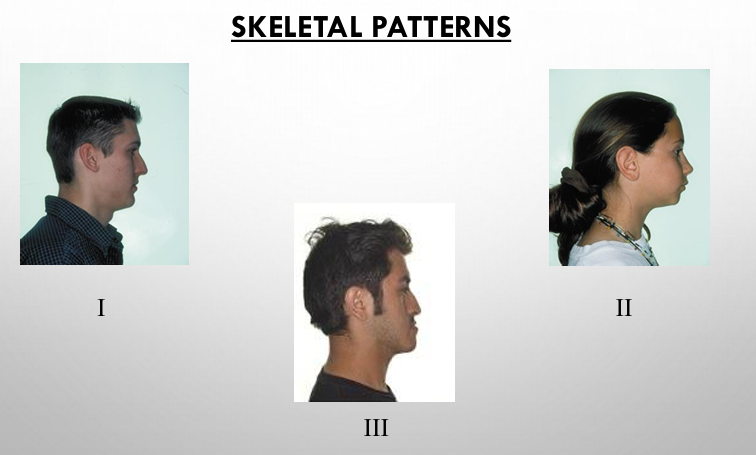
skeletal patterns
-cephalometric analyses reveal the skeletal component of the patient’s malocclusion in relation to cranial base
-can classify patients as: class I/II/III skeletal pattern
-patterns often correspond with the dental molar angle classification but not necessarily all the time- understanding the skeletal pattern is essential for choosing the proper treatment objectives and plan
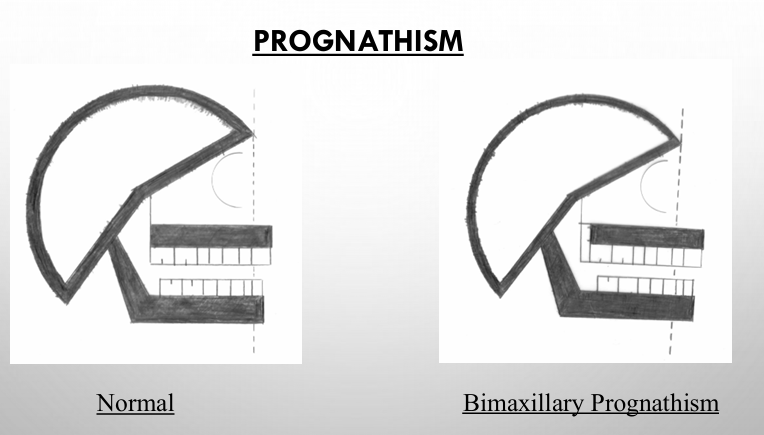
prognathism
-prognathism is a skeletal protrusion
-bimaxillary prognathism (protrusion): present when both jaws protrude forward of the normal facial limits (very convex)
-maxillary prognathism (protrusion): present when the maxilla protrudes forward of the normal limits of the face; usually seen in class II skeletal patterns
-mandibular prognathism (protrusion): when the mandible protrudes forward of the normal limits of the face; seen in class III skeletal patterns
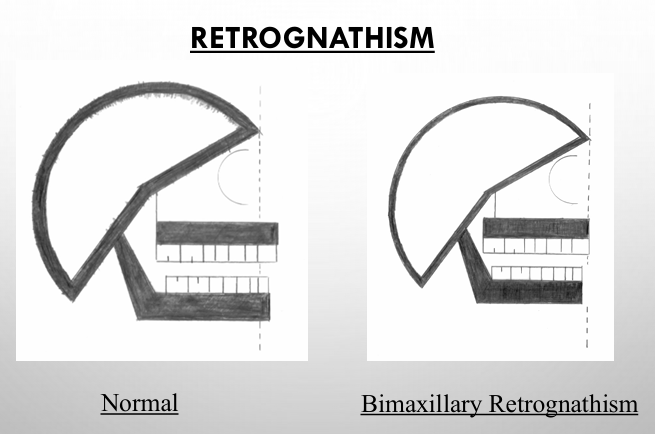
retrognathism
-skeletal retrusion
-bimaxillary retrognathism: present when both jaws are posterior to the normal limits of the face
-maxillary retrognathism: present when the maxilla is posterior to the normal limits of the face; seen in class III skeletal patterns
-mandibular retrognathism: present when the mandible is posterior to the normal limits of the face; seen in class II skeletal patterns
dentoalveolar protrusion
-present when the anterior teeth are anterior to the normal limits of the basal bone
-bimaxillary dentoalveolar protrusion: present when the anterior teeth of both jaws are anterior to the normal limits of the basal bone
-maxillary dentoalveolar protrusion: present when the anterior teeth of the maxilla are anterior to the normal limits of the basal bone
-mandibular dentoalveolar protrusion: present when the anterior teeth of the mandible are anterior to the normal limits of the basal bone

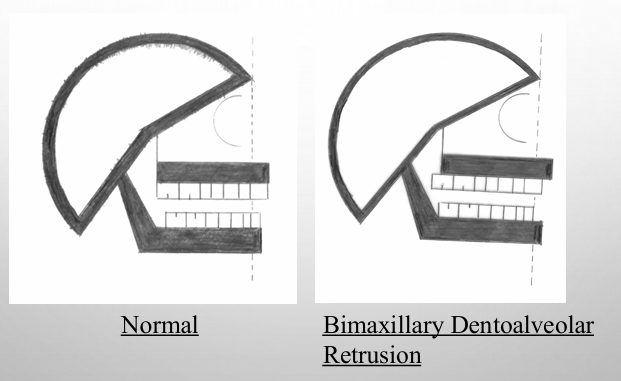
dentoalveolar retrusion
-present when the anterior teeth are posterior to the normal limits of the basal bone
-bimaxillary dentoalveolar retrusion: present when the anterior teeth of both jaws are posterior to the normal limits of the basal bone
-maxillary dentoalveolar retrusion: present when the anterior teeth of the maxilla are posterior to the normal limits of the basal bone
-mandibular dentoalveolar retrusion: present when the anterior teeth of the mandible are posterior to the normal limits of the basal bone
hyperdivergent skeletal pattern
-skeletal pattern that deviates from the norm in that there is an excessive divergence of the skeletal planes (determined by the analysis used)
-characterized by a steep mandibular plane angle, a long anterior lower face height with open bite tendency, lip incompetence, and often associated with class II malocclusion
hypodivergent skeletal pattern
-skeletal pattern in which the skeletal planes are more parallel to each other
-characterized by a low mandibular plane angle, short lower facial height, and is often associated with class II division 2 malocclusions and deep bites
-tend to have a very square face
development of a problem list
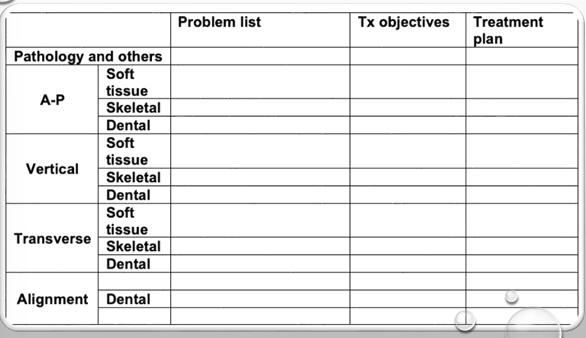
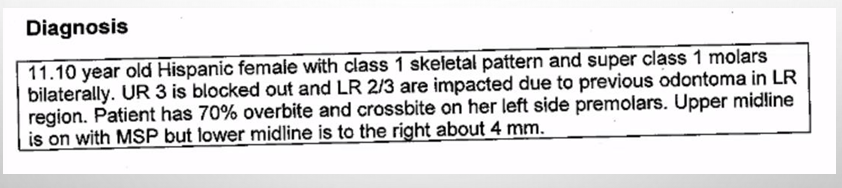
diagnosis rules
-always in paragraph form (no bullet points)
-written as a summary of the problem list (putting the main picture of the patient together)
-always begin with age, sex, and ethnicity of patient in what type of dentition
-summary should paint the picture of the patient that someone can view without the records in front of them
treatment objectives
-state your goals for treatment for ANYTHING that is abnormal → very comprehensive
-examples: a patient is class II and you want to correct to class I, a patient has 9mm overjet and you want to correct to 2mm overjet, a patient is congenitally missing a second premolar and you want to maintain the primary tooth in the final occlusion
-****you must have a treatment objective for every problem you list on your problem list!!!****
treatment plan
-once you have determined your goals, you have to map out a plan to get there
-there will be a plan for the overall treatment and separate plans for the maxilla and mandible
-treatment mechanics and retention plan also included in the treatment plan
-remember: all pts need to have retainers after orthodontic treatment- retention is LIFETIME→ NO EXCEPTION