Looks like no one added any tags here yet for you.
Peripheral Nerves
Connect information to the central nervous system
Efferent
Motor fibers
Afferent
Sensory fibers
Interneurons
Connect neurons within a specific region of the CNS responsible for reflexes
Nodes of Ranvier
Constrictions separating successive segments of myelin
Nerve impulses leap
Farther apart = faster conductions
Traumatic Injury can cause injury due to
Mechanical damages
Thermal damages
Chemical damages
Ischemic damages
Wallerian Degeneration
Axon distal to the injury degenerates due to nerve fiber being cut, crushed, or compressed
Bands of Bunger
Formed by Schwann Cells, guide growth factors
Schwann Cells and Macrophages
Clear the debris to assist with growth
Which degrees of nerve injury are reversible?
1st and 2nd Degree
Which degrees of nerve injury are non-reversible?
3rd/4th and 5th degrees
1st Degree of Reversible of Nerve Injury (Neuropraxia)
Interruption of conduction; short recovery time
Ex: Carpal Tunnel
2nd Degree of Nerve Injury (Axonotmesis)
Loss of continuity of the axon; Wallerian degeneration; Preservations of endo-, peri-, and epineurium
3rd/4th Degree of Nerve Injury (Neurotmesis)
Loss of continuity; Some loss of continuity of epineurium and perineurium; may or may not be disrupted
5th Degree of nerve Injury (Transection)
Severe Neurotmesis; gross loss of continuity
Treatment for Neurapraxia
Observation and education
Treatment for Axonotmesis
Surgical intervention may be required; education
Treatment for Neurotmesis
Loss of nerve trunk → surgical intervention is neccessary
Goal of surgical repair
Tension free and end to end repair
Surgical repair
May be microscopic immediate repair, within 24 hours
Delayed repair 3-5 days
Delayed repair with nerve graft
Autograph
Harvested from the patient’s own body, but from another location:
Medial antebrachial cutaneous nerve (<8 cm)
Sural nerve (up to 30cm)
Posterior interosseous nerve: distal digital nerve (<2cm)
Limitations of Autographs
Requires 2nd surgery site to harvest tissue
Mismatch of donor nerve size
Fascicular inconsistencies
Allograft
Tissue from another individual
Limitations for Allograft
Risk of infection & tumor formation
Immune rejections
Risk of cross contamination
Secondary infection
Limited supply
Xenograft
Graft attained from a member of a specifies other than the recipient
Limitations of Xenograft
Risk of cross-species disease transmission
Requires immuno-suppressive drugs
Risk of infection and tumor-formation
Nerve Conduits
Serves as an artificial means of guiding axonal regrowth for nerve generation
Preserves extra-cellular matrix for mechanical guidance for regenerating axons
Early Vasomotor distal observations of nerve injury
Skin rosy
Late Vasomotor distal observations of nerve injury
Skin mottled or splotchy
Early Sudomotor distal observations of nerve injury
Dry skin
Late Sudomotor distal observations of nerve injury
Dry or overly moist skin
Pilomotor observations
Goose flesh or goosebumps. This is absent for early and late nerve injury
Early Tropic distal observations of nerve injury
Fingernails blemish
Longer & fine hair growth
Skin soft & smooth
Slight atrophy
Later Tropic distal observations of nerve injury
Curved
Longer & fine hair growth
Skin smooth/non-elasticAtrophy at finger pulps (tips)
Test for pain/temp sensory return
Sharp/dull, temp
Test for vibration (30cps) sensory return
Tuning fork (30 cps)
Test for moving touch sensory return
Moving light touch
Test for constant touch sensory return
Semmes Weinstein
Test for vibration (256 cps) sensory return
Tuning fork (250 cps)
Ten Test
Screen for large A-Beta fibers (testing moving fibers)
Touch contra-lateral unaffected digit to identify normal sensation. Touch same area on the involved side and have pt rate the normal sensation compared to contra-lateral side.
Primary goals for direct intervention
Prevent rupture after surgical repair with orthosis fabrication and client education. Control edema and scarring, maintain motion safely. Promote healing
Work on sensory return and desensitization. Work on strengthening avoiding fatigue when MMT is 3/5 or less
Additional treatment consideration
•Hypertrophic scarring
•Decrease pain
•Increase prehension skills
•Increase ADL & work skills
•Instruct patient and family in rehab process.
•Psychological adjustment
•Prevocational & vocational assessment
Acute Phase of Treatment Post-Surgical Nerve
Orthosis to protect nerve repair
Maintain AROM in uninvolved joints
Scar management
Recovery Phase of Treatment Post-Surgical Nerve
Orthosis to maintain webspace to be worn nocturnally
Digit motion combined with wrist motion
NEuromuscular Re-education
Desensitization
Sensory Re-education
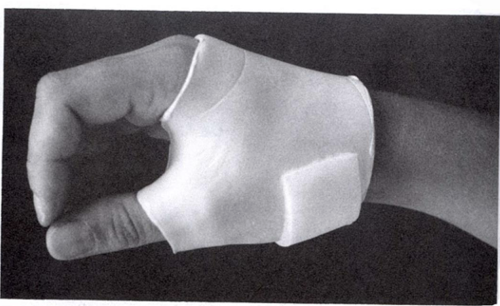
Orthosis Fabrication for Median Nerve
Fabrication of wrist based, and thumb included to maintain webspace orthosis
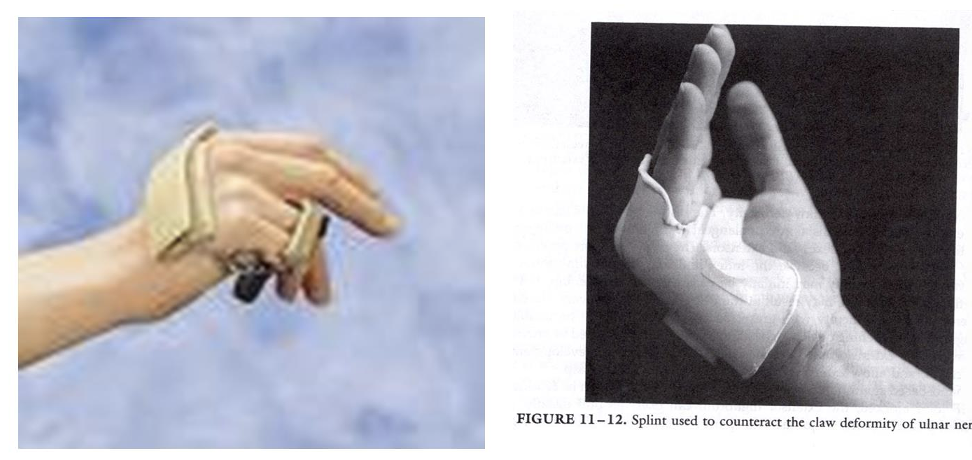
Orthosis Fabrication for Ulnar Nerve
Fabrication of wrist orthosis in neutral and MCP joints of ring and little in 70 deg. flexion
Orthosis Fabrication for Radial Nerve
Depends on location of repair, possibly a resting hand orthosis (unusual)
Length of Acute (Protection) phase of post-surgical repair
0-4 weeks
Sensory Re-Education: Silent Phase (Early)
Return of vibration 30 Hertz and beginning to identify moving touch
Sensory Re-Education: Silent Phase (Early) Activities/Procedures
Imagery
Mirror Box
Laminated cards with verbs to be read throughout the day
Sensory Re-Education: Late Phase
Identifies 250 cps
Nerve is beginning to innervate
Sensory RE-Education: Late Phase Activities/Procedures
Introduce traditional sensory training identifying objects
Rice bins
Textures
Shapes
Tracing items with digits
What kind of activities would you use in the Advanced late Phase of Sensory Re-Education?
Proprioceptive Activities, such as gentle oscillations, light ball toss or scarf juggling
What may occur in early or late phase?
Hypersensitivity
Desensitization Massage Interventions
Self Massage every 2 hours
Grade up: massage with soft brush and progress to electric toothbrush with vibration
Desensitization Texture Interventions
Rub area with textures 4-6 times daily for 3-5 minutes
Textures should be bearable, but uncomfortable
Start soft and grade up as area adapts
Desensitization Immersion Interventions
Immerse area with varying textures within a container
Ex: dry lentils, rice, macaroni, dried beans, etc.
Key exercise for motor retraining Median Nerve Injury
Hold hand so thumb in a palmar opposition position and try to maintain. Try to mimic the perimeter of a jar lid
Key exercise for motor retraining Ulnar Nerve Injury
Finger abduction and adduction. Hand palm down on a flat service abd & adduction of fingers. Use powder on a board to reduce friction
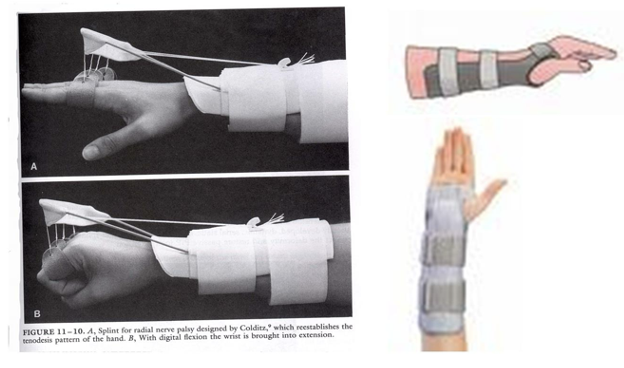
Radial Nerve Injury
Wrist drop
Loss of:
Extension of wrist
Extension of fingers
Thumb abduction
Thumb extension
Supination of forearm (weak)
Splint for radial nerve injury
Focus on wrist extension for functional grasp
Key exercise for motor retraining Radial Nerve Injury
Extension of wrist, fingers and thumb. When retraining, finger intrinsic substitution (lumbricals) can be a problem. Use coban to isolate the extensor digitorum.
Median Nerve Injury
Ape Hand Deformity
Atrophy of Thenar muscles
Splint for Median Nerve Injury
Focus on thumb in functional position
Special tests to use to assess integrity of Median nerve
Phalen’s Test
Tinen’s Test
Ulnar Nerve Injury
Claw Hand
Loss:
Functional grip is weak, loss of power grip
Weakness of wrist flexion
Loss of little and ring finger DIP flexion
Partial loss of Palmar pinch
Weakness of MP adduction and abduction
Difficulty making an O
Functional loss of writing grip
Loss of thumb adduction
Splint for Ulnar Nerve injury
Focus on 4th and 5th digit flexion for increased function
Special test to assess integrity of Ulnar Nerve
Froment’s Sign
Froment’s Sign
When patient attempts to pinch with the thumb and index finger, the long flexor of the thumb is used to substitute for thumb adductor, resulting in flexion of thumb at the IP joint