M8/9-VERTEBRAL FRACTURES AND SKULL
1/18
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
19 Terms
C1 FRACTURE
DESC: usually sustains compression-type fractures. A comminuted or burst fracture is referred to as a Jefferson fracture.
ETI: The mechanism of injury is vertical compression: for example, diving into a pool or being pushed into the boards during hockey.
TREAT: treated with cervical traction.
COMP: Neurological deficit is a possible complication
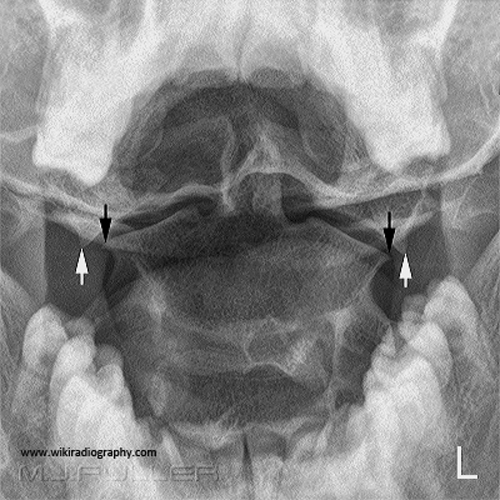
C2
DESC: There is a potential for dislocation. The most common injury site is the base of the odontoid
ETI: severe flexion or extension forces are applied to the neck. For example, in a motor vehicle accident
TREAT: cervical traction to help stabilize the fracture. Alternately, a screw could be surgically inserted if indicated.
COMP: First, there is a greater chance of non-union of the dens because of the limited blood supply to the area. Second, the patient could become quadriplegic or develop other neurological problems.

HANGMAN’S FRACTURE
DESC: vertebral body separates from the neural arch, with or without dislocation. The odontoid remains attached to the body.
ETI: A common mechanism of injury is a force applied to the head while the neck is in extension
TREAT: A halo vest may be used, depending on the fracture. For more severe fractures, surgical intervention may be required.
COMP: Neurological problems can develop if this type is left untreated.

FACET LOCKS
DESC: can be either a unilateral (25% or more) lock or a bilateral (50%) facet lock
ETI: Unilateral=flexion with rotation, bilateral=flexion with severe distraction
TREAT: Facet locks are treated with closed reduction with cervical traction.
COMP: Bilateral more unstable

CLAY SHOVELLERS
DESC: avulsion fracture of the spinous process of the lower cervical spine or upper thoracic spine
ETI: Sudden contraction of the muscles when shovelling snow or dirt when gardening
TREAT: Stable fracture so rest for 3-4 weeks is recommended.
COMP: No complications unless there are multiple fractures.

TRAUMATIC SPINE FRATURE
DESC: usually associated skeletal injuries, A fracture resulting from Seatbelt Syndrome is called a Chance Fracture, where there is a horizontal splitting of the spine and neural arch
ETI: The mechanisms of injury for thoracic and lumbar vertebrae are varied. There are flexion/distraction forces similar to the mechanisms of injury for cervical vertebrae
TREAT: The patient is fitted with a brace after bony healing has started. If there is no healing, or the distraction is too severe then surgical intervention will be required.
COMP: Distraction injuries are associated with serious lower abdominal structure injuries

OSTEOPOROSIS PATHOLOGICAL FRACTURES
DESC: decreased bone mineral density and bone mass. The most common areas are the spine, hip and wrist, although it can usually be seen in all bones.
ETI: Bone loss occurs faster than new bone growth resulting in an overall decrease of the bone matrix
TREAT: sometimes treated with kyphoplasty or vertebroplasty
COMP: ongoing pain from the bone disintegrating, and loss of height.

PATHALOGICAL FRACTURES
DESC: fracture which results from a disease process
ETI: bony matrix is weakened because of disease and can fracture with or without minor trauma to the bone
TREAT: treated with reduction and stabilization of the fracture. Depending on the severity of the fracture, treatment can be with a brace or surgical.
COMP: can result in the inability to bear body weight above the fracture.

INTERVERTEBRAL DISC INJURIES
DESC: due to rupture or herniation of the disc and can vary in the degrees of damage
ETI: Compressive or distraction actions are the mechanisms of injury
TREAT: Conservative treatments are usually the first line of defense, such as rest and anti-inflammatories. If there is no relief, then steroids are used. Surgery is the last option
COMP: Increasing pain, decreased mobility, increased nerve compression with bowel and bladder dysfunction are possible complications.

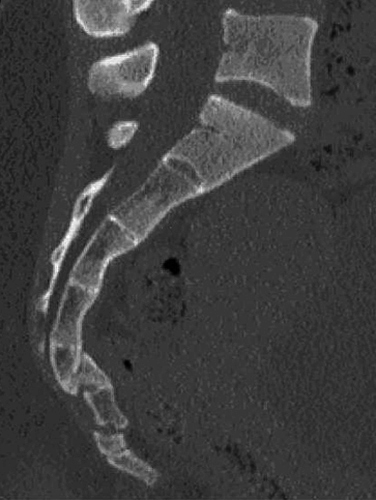
SACRUM AND COCCYX FRACTURE
DESC: They are usually linear fractures
ETI: The mechanism of injury is usually a direct blow to the area, as in a fall
TREAT: Rest or surgical
COMP: ongoing pain and deformed bones.
SKULL FRACTURES
DESC: Either linear or depressed
ETI: Linear is low impact blunt trauma, depressed is direct blow
TREAT: depends on the type of fracture.
COMP: Swelling of the brain, damage to the brain and associated areas which the brain controls.

CEREBRAL CONTUSIONS
DESC: micro-haemorrhages of blood vessels in the brain due to trauma and usually occur in coup and contrecoup injuries.
ETI: brain collides with the sharp edges of bone in the skull which results in bruised tissue.
TREAT: Close monitoring is sometimes necessary.
COMP: There could be a chance of increased swelling and a rise in intracranial pressure
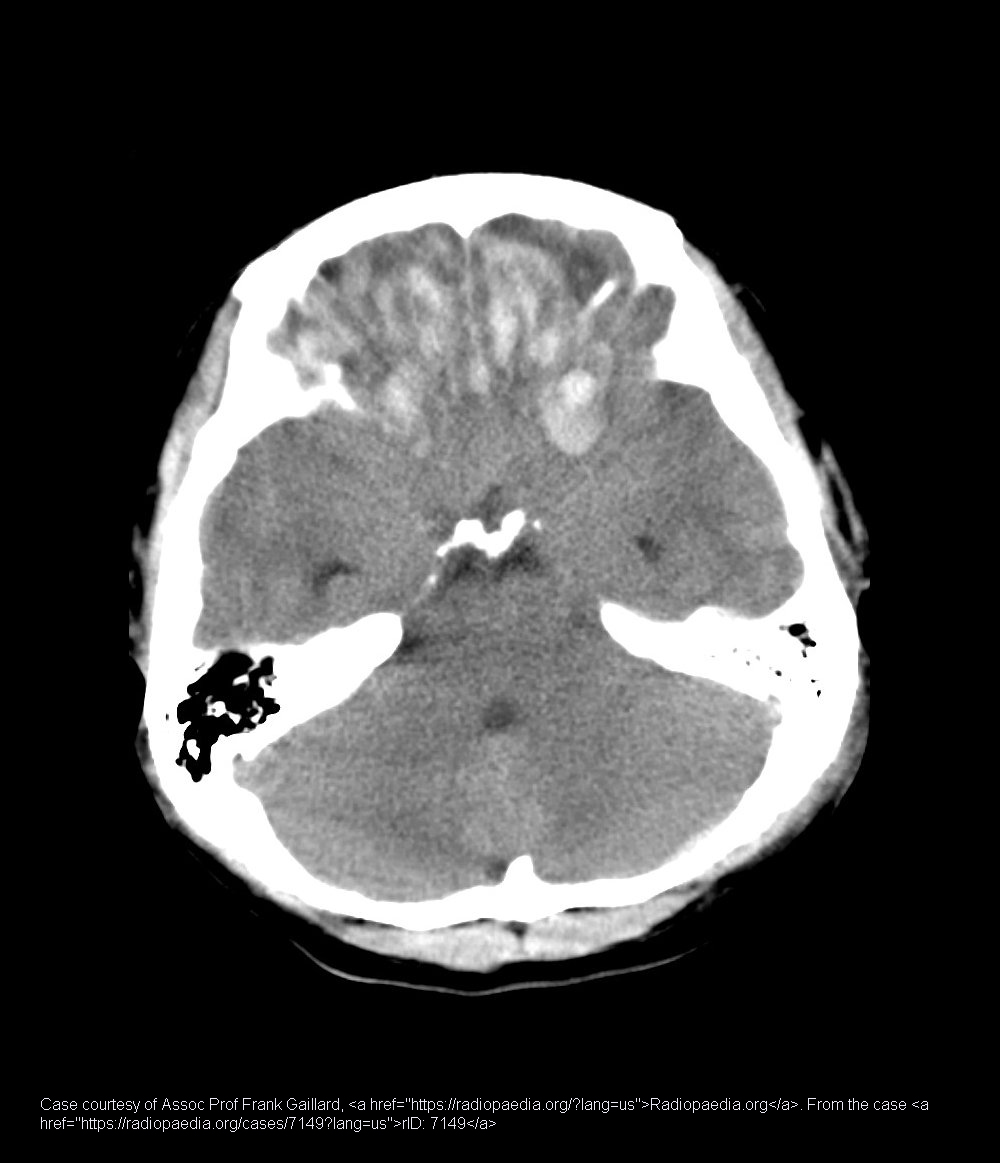
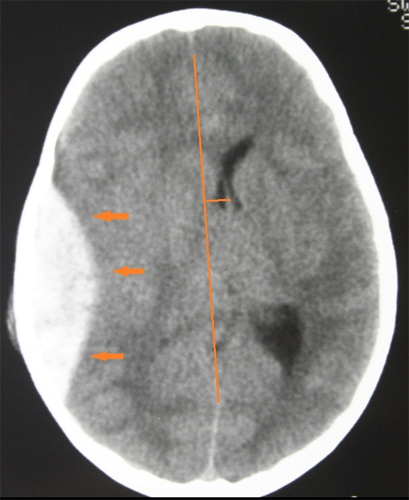
CEREBRAL HEMORRHAGES
DESC: bleeding within the brain which can result from pathological conditions, major trauma to the head,
ETI: mechanism of injury is damage to blood vessels during rapid acceleration and deceleration of the head
TREAT: Medical or surgical intervention may be required to stop the bleeding.
COMP: Paralysis, morbidity if the bleeding is not stopped in time.
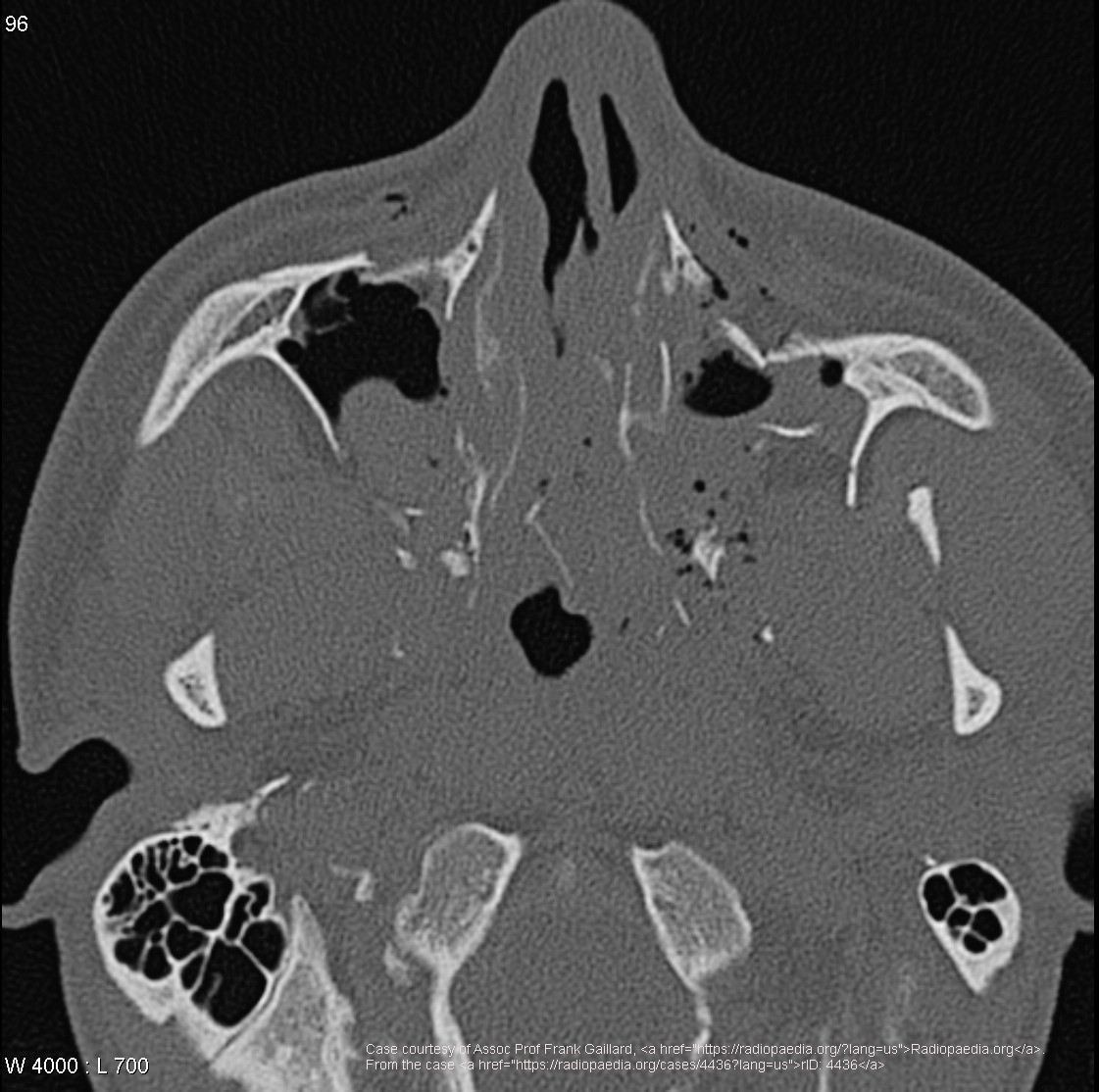
MAXILLA FRACTURE
DESC: can cause entrapment of the optical nerve tissue within the fracture, which can prevent upward motion of the eye
ETI: direct force to the area, which can result in a “blow out” fracture of the inferior orbital rim.
TREAT: Surgical repair is required.
COMP: Loss of teeth, infection, malocclusion, nonunion, malunion, lacrimal system obstruction, infraorbital nerve anesthesia, diplopia.
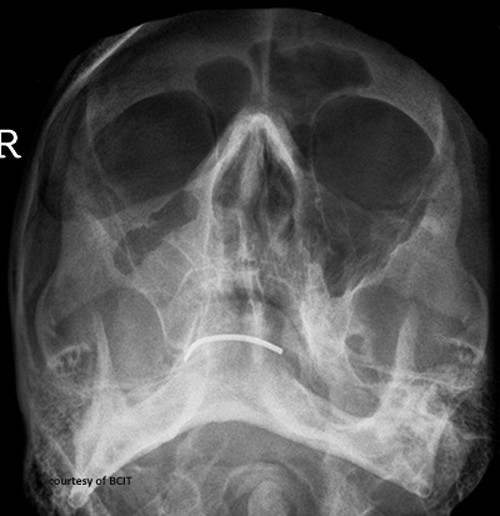
ZYGOMATIC ARCH FRACTURE
DESC: fragile and prone to injuries which are usually depression fractures.
ETI: direct trauma to the area
TREAT: Surgical plating is required for depressed fractures.
COMP: Lengthening of the midface, and lacrimal system obstruction.

LEFORT FRACTURE
DESC: These types of fractures are fractures of the midface. Part or all of the midface separates from the skull base. Usually they are in combination and associated with other facial fractures.
ETI: Direct trauma to the fac
TREAT: Surgical intervention to stabilize the fracture. Usually a multidisciplinary team will be involved
COMP: Mal union, malocclusion, sinusitis, facial nerve paralysis.
TRIPOD FRACTURE
DESC: separates the zygoma from it's attachments.
ETI: Blunt force trauma to the malar eminences.
TREAT: Surgical intervention.
COMP: Impingement of the temporalis muscle causing difficulty chewing, nerve pain. Disfigurement.

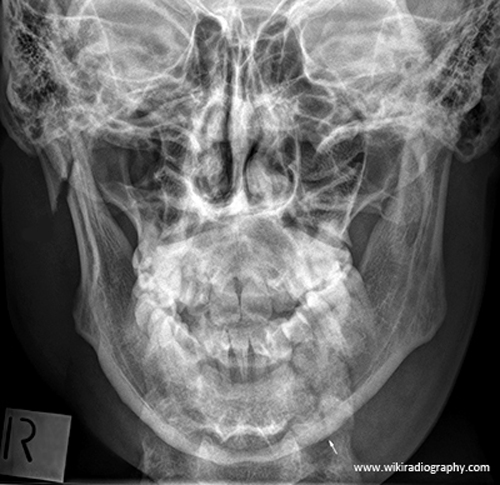
MANDIBLE FRACTURES
DESC: susceptible to contrecoup fractures.
ETI: usually a direct trauma
TREAT: not affected by muscles do not require immobilization. However, unstable fractures may cause airway obstruction due to loss of tongue control
COMP: Fracture fragments often displace due to the movement of facial muscles and can cause further damage.
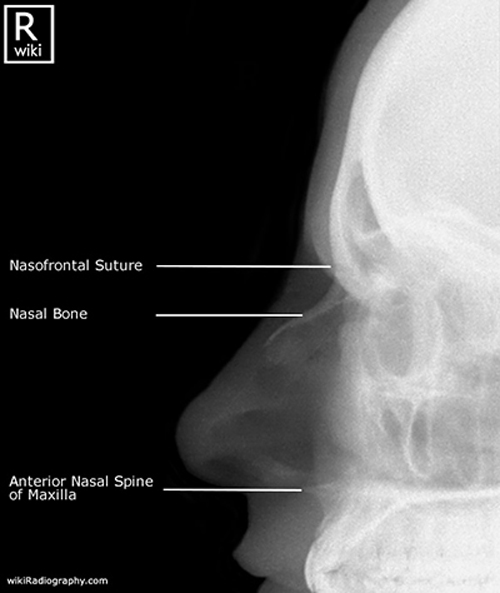
NASAL BONE FRACTURE
DESC: most common of all facial bone fractures. Even a minor impact can cause a fracture
ETI: The mechanism of injury is a direct force
TREAT: Usually, no treatment needed.
COMP: Deviated septum which can impair breathing.