6A: Fluency Disorders
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
38 Terms
Fluency
Effortless flow of speech
Ability to produce speech
with normally long strings of sounds,
at a normally rapid rate,
without pausing or hesitation, and
with a normal amount of effort
Disfluency
Disruption or breakdown in flow of speech
Normal disfluency
Everyone experiences minor interruptions in flow of speech at times
Especially common in young children as they are starting to produce sentences
How do we distinguish “normal” disfluencies from stuttering?
What is stuttering?
An interruption in the flow of speaking characterized by specific types of disfluencies, including:
repetitions of sounds, syllables, and words (e.g., “Look at the b-b-baby,” “Let’s go out-out-out”)
prolongations of consonants when it isn’t for emphasis (e.g., “Ssssssssometimes we stay home”)
blocks (i.e., inaudible or silent fixation or inability to initiate sounds)
Normal Disfluency vs possible stuttering
Possible Stuttering
Repetitions
syllables
individual sounds
Sound prolongations
Sound blocks
Tense pauses
Bursts of speech
Clusters of disfluency
Associated body movements
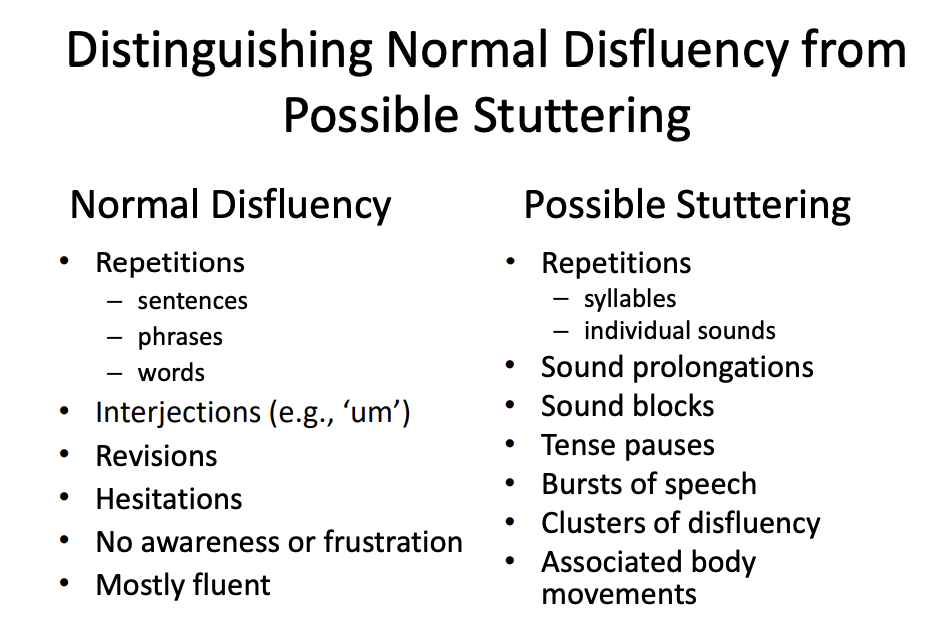
Distinguishing Normal Disfluency from Possible Stuttering
In the first 6 months after onset, groups can look very similar
Strong decline in disfluencies within 1st year in normal disfluency group
More likely to be stuttering if there is a family history of stuttering
strong genetic component to stuttering
Types of fluency disorders
Developmental stuttering
Non-developmental stuttering
Cluttering
Developmental Stuttering: Facts (concepts not numbers)
vast majority of people with fluency disorders
About 1% of the population currently stutter
About 3% of children will stutter during course of development
About 75% of children recover without any formal treatment
More prevalent in boys (3:1)
Typical onset between 2–5 years of age
Developmental Stuttering is…
Heritable
More often in twins and runs in families
Suggests genetic predisposition
Developmental stuttering is…
Variable
within utterances
day-to-day
across situations
Variability…
Decreases:
novel speaking manner (e.g., singing)
while alone, speaking to animals or kids
disruptions in auditory feedback (hearing aid that will play your speech back to you in a delayed form)
Increases:
anticipating stuttering (e.g., waiting to respond)
having to say specific words (e.g., your name, a joke)
talking on the phone
Overt/ Primary Characteristics
Part-word repetition
“mi-milk”, “d-d-d-dog”
Single syllable word repetition
”I…I want that”
Multi-syllabic word repetition
“Lassie…Lassie is a good dog”
Prolongation
“I’m Tiiiiiimy Thompson”
Overt/ Primary Characteristics cont.
Silent/tense pause (block)
“Can I have some….milk?”
Phrase repetition
“I want a…I want a ice cream cone”
Interjection
“He went to the …uh…circus”
Revision or incomplete phrase
“I lost my…Where’s Mommy going?”
Covert/ Secondary behaviours
Bodily Movements/Struggle
Facial grimaces
e.g., blinking eyes, wrinkling forehead, distorting mouth, tongue protrusion
Head movements
e.g., looking away, jerking
Loss of eye contact
Body movements
e.g., limb movement, foot tapping
*Unconscious way of trying to avoid stuttering
Covert/ Secondary behaviours cont.
Psychosocial behaviours
Avoidance
e.g., fillers, pretending to think, avoiding situations and people, appearing shy and quiet
Emotional responses before speaking
e.g., fear of loss of speech control
Emotional responses after stuttering
e.g., embarrassment, shame, anger, frustration
Non-developmental stuttering is either:
Sudden onset of stuttering in previously fluent adult…
Neurogenic
Linked to identifiable neurological event
Psychogenic
In context of psychological disturbance
Neurogenic
Etiology
Neurological damage or disease
e.g., stroke, head injury, neurosurgery, MS, Parkinson’s disease, meningitis
Exposure to toxins
e.g., drugs, poisons
Distinctions from stuttering
Equally disfluent across different speaking situations
Secondary behaviours less common
Negative emotional response less common
Psychogenic stuttering
Etiology
e.g., psychological trauma, anxiety, depression, other psychological disorder
Distinctions from neurogenic stuttering
May be intermittent
Unusual or bizarre speech/language patterns
May respond quickly to behavioural treatment
Cluttering
Fluency disorder of unknown origin characterized by sporadically excessive rate, and incomplete and distorted articulation
Speech characterized by rapid rate, disfluencies, and articulation errors, often accompanied by spoken and written language difficulties. These signs usually occur without the speaker’s awareness or concern
Rare
Cluttering characteristics
Frequent whole word and phrase repetitions
Rapid rate of speech
Irregular rate of speech
Misarticulations
Slurred or deleted phonemes
Substitutions
Distinctions from stuttering
Part-word (sound or syllable) repetitions are infrequent
Secondary behaviours (e.g., tension, struggle, avoidance) not usually present
Lack of awareness of or negative emotional response to the problem
Often more fluent in conditions where person who stutters is less fluent
e.g., under stress, with authority figures, when paying attention to their own speech, when wanting to be fluent
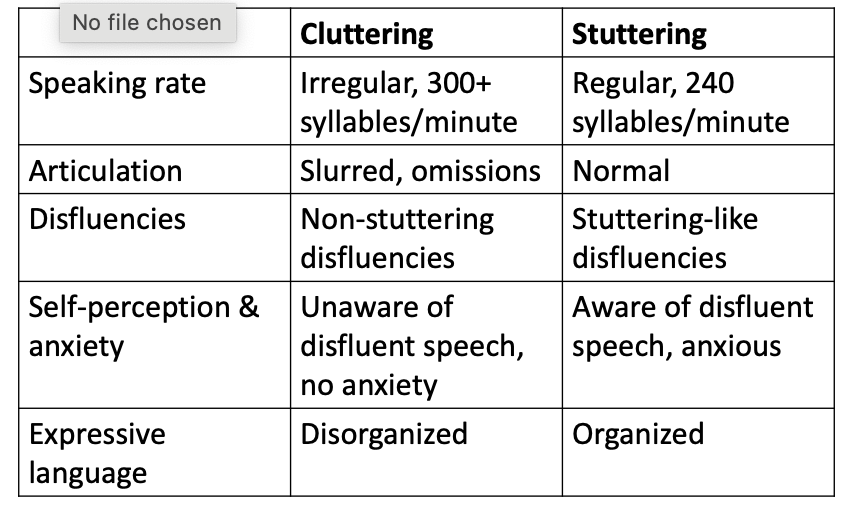
Cluttering vs stuttering
Cluttering:
much faster speech rate
unaware of disfluent speech (no anxiety)
Disorganized
Stuttering Theories
Demands & capacities theory
Intrinsic & extrinsic social demands exceed the child’s capacities for fluent speech
Covert repair theory
Children have a disordered phonological system
Neuropsycholinguistic
Stuttering = disruption in timing of linguistic formulation & speech movement
Likely Causes…
Likely a combination of factors –
genetic predisposition
neurological dysfunction
atypical cerebral organization (over-activation in right hemisphere; under-activation in left)
difficulty with auditory feedback
Environmental stressors
Assessment: Are speech disfluencies present?
Speech sample
Disfluency count (% syllables stuttered)
Normal disfluency count is below 3%, higher than 3% is cause for concern
Type:
mild: easy repetitions
more severe: sound blocks, sound prolongations; body movements
Assessment: What is the nature of the speech disfluencies?
Occurrence of within-word disfluencies
Stuttering severity scales
Occurrence of secondary behaviors
Speaking rate
Examples from communication attitude checklist and stuttering attitudes checklist
*Concepts not specifics
People worry about the way I talk
I don’t talk like other children
Some kids make fun of the way I talk
I let others talk for me
I sometimes feel that my stuttering is my own fault
My teachers should not make me answer questions in class if they think I will stutter when I answer
I feel that it is best if I do not talk about my stuttering with my friends
My stuttering is my biggest problem
Sometimes I feel I should be able to stop my stuttering without help
I think stuttering makes it harder for me to make friends
My stuttering has caused me to make poorer grades in school
Sometimes I think my parents may have caused my stuttering
I doubt if speech therapy can help me a whole lot
Treatment for early stuttering:
Uses indirect methods
changes in environment to stabilize fluency
reinforcing fluent speech
*family involvement
deal with anxiety
e.g., Lidcombe program
Lidcombe program
Clinician-mediated
Parent-implemented
Behavioural treatment
preschoolers
adapted for school age (mild-moderate stuttering)
Goal: no stuttering
Several outcome studies
92% achieve and maintain near zero stuttering up to 7 years post treatment
Treatment for stuttering
Fluency shaping
Stuttering modification
Both use behaviour modification to reduce speech disfluencies
May be used in isolation or in combination
Fluency shaping
Designed to modify all aspects of client’s speaking behavior Robb, 2014
Behavioural modification
“relearning” speech motor movements to produce fluent speech
Goal = stutter-free speech
Fluency Shaping: learn new pattern of speaking
a. Speak at reduced rate
b. Prolong vowel portions of words
c. Use slow and smooth onsets of words
d. Continuous phonation
Fluency shaping
Potential for rapid, dramatic change
Some problems with Fluency Shaping
Abnormal/artificial speaking pattern
Skills may not easily transfer out of therapy context
Attention to speaking pattern ongoing
Stuttering Modification
Designed to address individual moments of stuttering, as opposed to changing entire pattern of speaking behaviour
Clients learn to
stutter more fluently, with less tension
use light articulatory contacts during speaking
reduce situational fears and negative associations with stuttering, feel in control of stuttering
Problems with stuttering modification
Slower observable change
May still have moments of stuttering
Nontraditional treatment approaches
Hypnotherapy
Controversial
Not a ton of evidence to prove this works
Drug Therapy
Some success with dopamine blockers
focus on anxieties associated with stutters
Electronic Devices
Closely resemble hearing aids
Delayed auditory feedback
Cultural considerations
Careful consideration required in the assessment and treatment of fluency disorders among individuals from diverse cultural backgrounds
Use of fluency shaping versus stuttering modification therapy needs to be considered from a cultural perspective
Special considerations for multilingual speakers
Likely to stutter in multiple languages, but more in the less proficient language
Research is needed to support assessment and treatment in this population
How listeners can help
Listen to what the person is saying, not how they are saying it
Maintain natural eye contact
Wait until the person is finished (do NOT finish sentences or fill in words)
Be especially patient on the telephone
Don’t give advice (e.g., slow down, take a breath)
You speak in a slow & relaxed way (modelling).