anatomy 2 content before finals
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
97 Terms
glomerular filtration rate
amt of filtrate formed by BOTH kidneys per minute, average GFR is 125 mL/min in males and 105 mL/min in females
homeostasis requires kidneys to maintain a relatively constant GFR
high - substance pass too quickly and not reabsorbed
low- nearly all filtrate reabsorbed and some waste not excreted
directly related to pressures that determine net filtration pressure, when system bp rises, net filtration pressure and GFR only increase a little bit
coltrolled by renal autoregulation, neural regulation and hormonal regulation which adjust blood flow into and out of glomeruus and alter glomerular capillary surface available for filtration
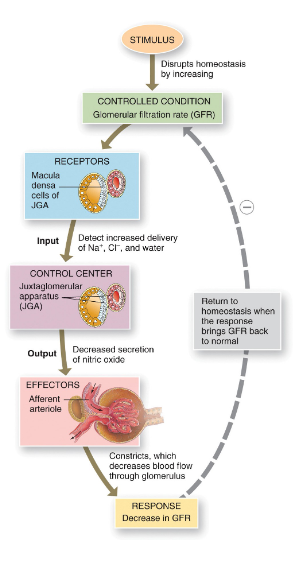
renal autoregulation of GFR
keep stable pressure in kidneys and thus- GFR, intrinsic mechanism with the kidneys consisting of the myogenic mechanism and tubuloglomerular feedback
myogenic mechanism- stretching causes contraction of smooth muscle in wall of afferent arteriole
tubuloglomerular feedback- as macula densa provides feedback to the glomerules
high GFR diminishes reabsorption of Na and Cl
macula densa inhibits release of nitric oxide
afferent arterioles contract
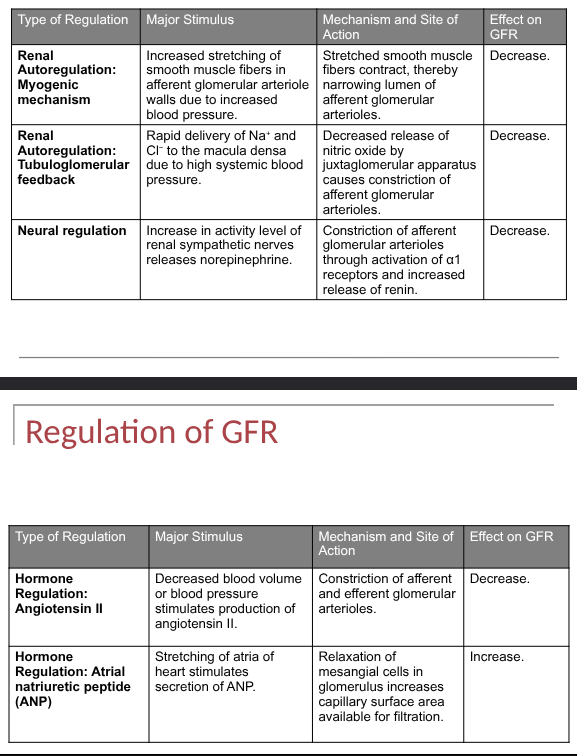
neural regulation of GFR
kidneys supplied by sympathetic fibers, excersize and hemorrage trigger sympathetic stimulation and afferent arterioles constricted so urine output is reduced and blood is available for other organs, ANS fibers release norepinephrine on alpha 1 receptors causing vasoconstriction
hormonal regulation of GFR
through the action of angiotensin ll and atrial natriuretic peptide, ANP increases GFR
ANP secreted in response to stretch of cardiac atria
increased urine formation leads to decreased blood volume and pressure to promote sodium and water loss
angiotensin ll constricts afferent and efferent arterioles- decreasing GFR
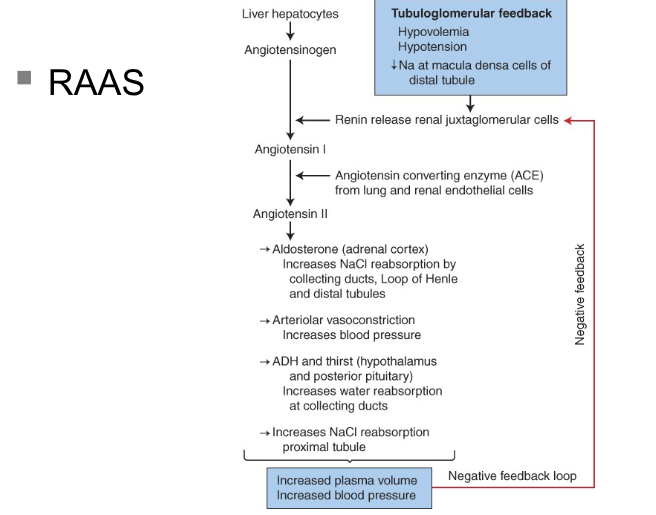
RAAS (renin angiotensin aldosterone system)
increases systemic arterial presssure and increases sodium absorption
renin: enzyme formed and stored in afferent arterioles of the juxtaglomerular apparatus
renin helps for angiotensin 1 (physiologically inactive)
in presence of angiotensin converting enzyme, angiotensin l converted to ll
regulation of GFR summary
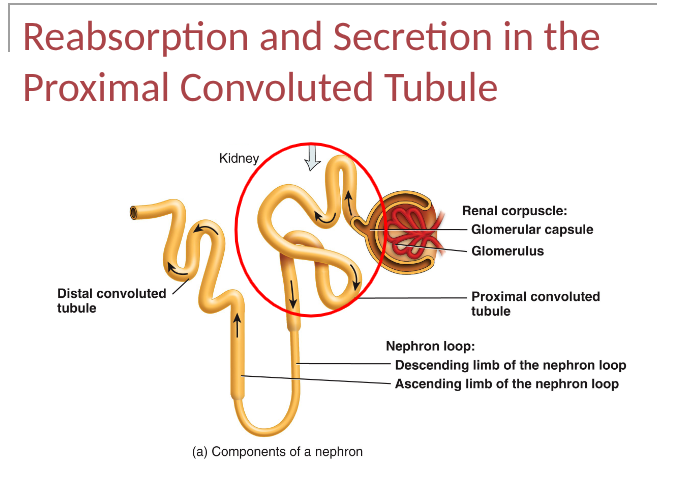
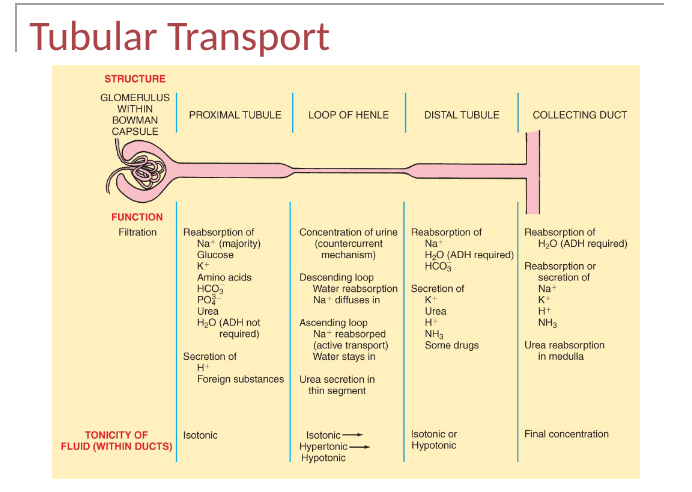
tubular reabsorption and secretion
normal rate of GF is so high that the volume of fluid entering PCT in half an hour is greater than the total plasma volume, much of the filtrate is reabsorbed- esp water, glucose, aa and ions, secretion helps to manage pH and rid the body of toxic and foreign
notes for elena (WHAT WAS NOT ON THE SLIDES)
ex- coffee and tea stimulates reabsorption, 99% of water is reabsorbed
DONT memorise table- will be given, 0 absorbtion of creatinine so it is a good test to see if kidneys are secreting
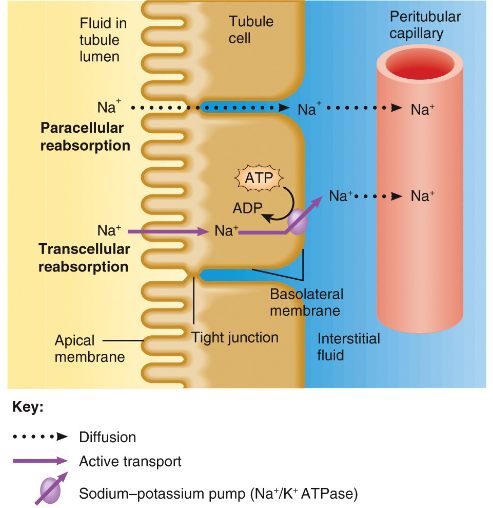
transcellular is an active process (can passively go into cell, need energy to leave)
when all solutes are reabsorbed- high conc of water left which drives water reabsorbtion
tubular reabsorption
returns more of the filered water and many filtered solutes (glucose, aa, ions) to the bloodstream using passive and active transport
tubular secretion
transfer of materials from the blood and tubule cells into tubular fluid, helps control bood pH and helps eliminate other substance from the body
reabsorption routes
substance being reabsorped in the tubule lumen will take one of 2 routes before entering perirtubular capillary
paracellular reabsorption- passive fluid leakage btwn cells
transcellular reabsorption- directly through tubule cells
what causes transport mechanisms
solute reabsorption drives water reabsorption, mechanisms that accomplish Na+ reabsorption in each portion of renal tubule and collecting ducts recover filtered Na+ and also electrolytes, nutrients and water
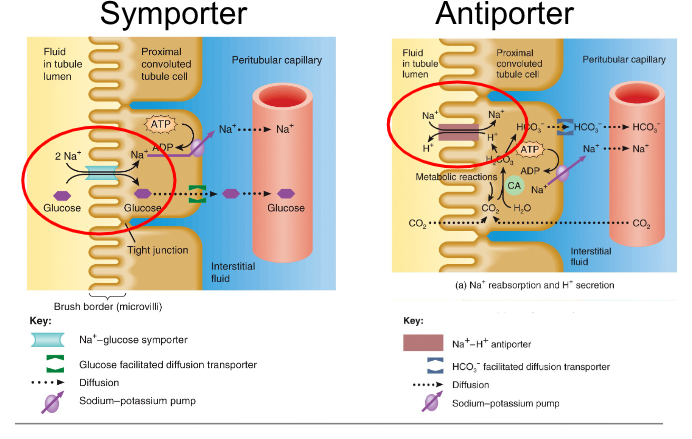
Transport Mechanisms
Primary active transport
uses ATP (Na, K pump)
energy from ATP used to pump substance across membrane
Secondary active transport
driven by ions electrochemical gradient
symporters move substances in same direction
antiporters move substances in opposite directions
water reabsorbtion
renal tubule and collecting duct use osmosis for water reabsorption, abt 90% of filtered water is reabsorbed by kidneys occurs with reabsorption of solutes (obligatory water reabsorption), reabsorption of final water (facultative water reabsorption) based on need and occurs in collecting ducts and regulated by ADH
reabsorption of PCT
majority of solute and water reabsorption, mostly involves Na, reabsorption of Na and other solutes creates osmotic gradient that promotes reabsorption of water by osmosis
Secretion of PCT
ammonia is waste produced by hepatocytes- convert ammonia to urea, both are filtered at glomerulus and secreted by PCT cells into tubules. PCT cells can produce additional NH3 and NH4+ as needed
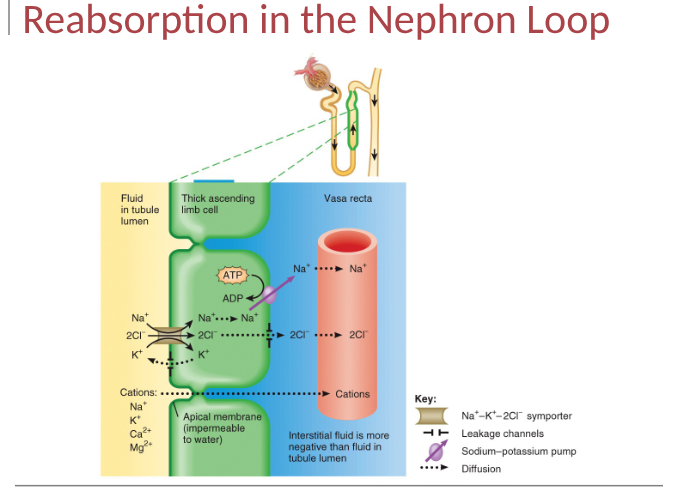
reabsorption in the nephron loop
set stage for independent regulation of both the volume and osmolarity of body fluids, relatively impermeable to water esp in the ascending limb, little obligatory water reabsorption
reabsorption and secretion in the DCT and Collecting Duct
Summarise 37, 38
tubular transport summary
homeostatic regulation of tubular reabsorption and secretion
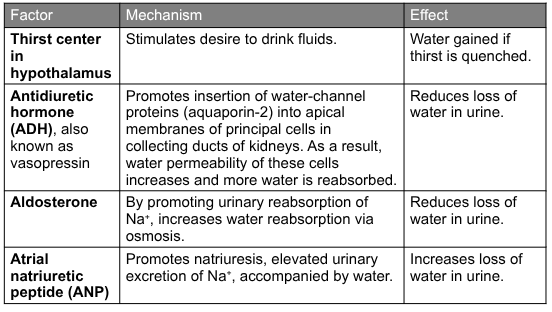
key hormones secreted by renal tubules
RAA- angiotensin ll increases blood volume and pressure, regulated electrolyte reabsorption and secretion along with aldosterone which also increases reabsorption of water in the collecting duct
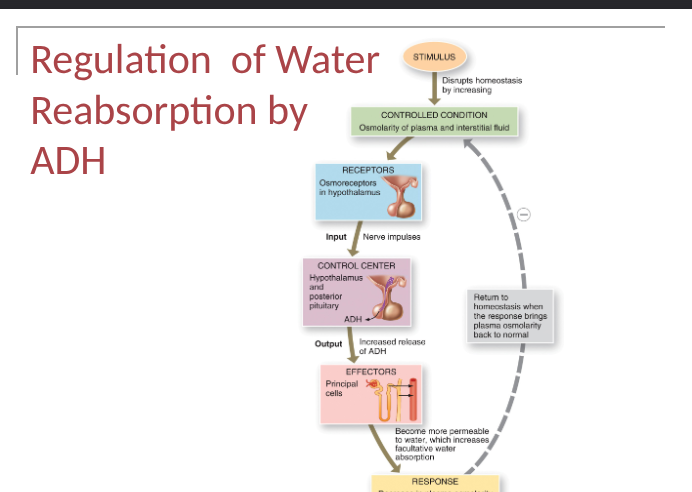
ADH- antidiuretic hormone, regulated facultative water reabsorption by increasing the water permeability of principal cells
ANP- atrial natriuretic peptide, can inhibit both water and electrolyte reabsorption
PTH- parathyroid hormone, promotes calcium reabsorption
Urine production
fluid intake is highly variable, homeostasis requires maintenance of fluid volumes within specific limits, rate at which water is lost depends on ADH- controls water permeability of principal cells in collecting duct (and in last portion of DCT)
high intake of fluid = dilute urine of high volume
low intake of fluid = concentrated urine of low volume
Urine concentration
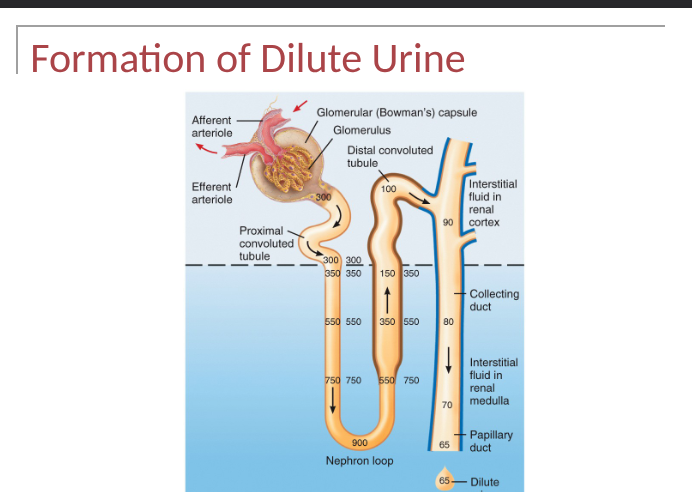
formation of dilute urine
when ADH level is very low, kidneys produce dilute urine and excrete excess water- renal tubules absorb more solutes than water, tubular fluid progressively becomes more dilute as it flows- can be as low as 65-70 mOsm/liter
Thick ascending limb
symporters actively reabsorb Na+, K= and Cl-
low water permeability
solutes leave, water stays in tubule
collecting duct
low water permeability in absence of ADH
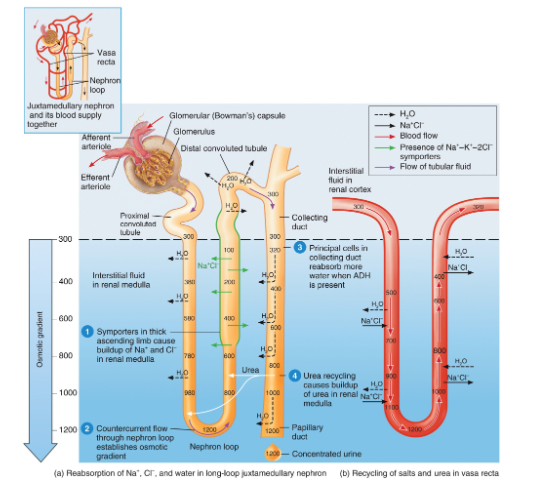
Formation of concentrated urine
when ADH level is high, kidneys secrete concentrated urine to conserve water, large volume of water is reabsorped from tubular fluid into interstitial fluid,
ascending limb cells of nephron loop- establish osmotic gradient in renal medulla
collecting ducts- absorbing more water and urea
urea recycling causing a build up of urea in renal medulla
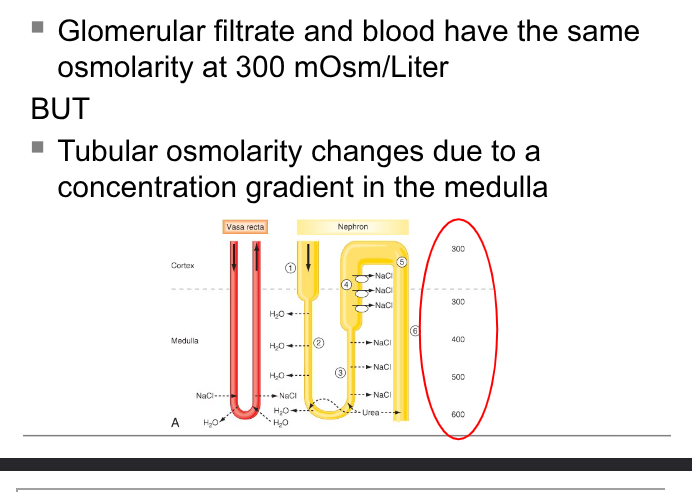
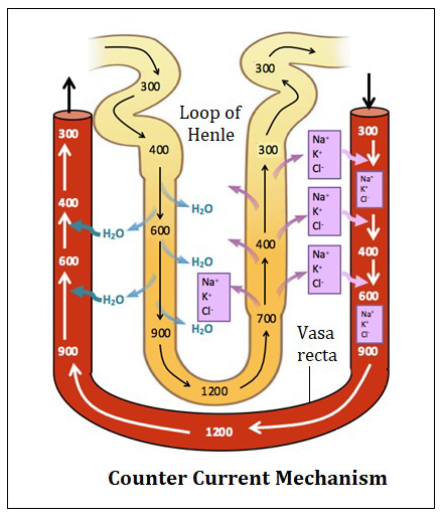
* 2 types of countercurrent mechansims
involves juxtamedullary nephrons with long nephron loops, osmotic gradient created by countercurrent multiplier, colutes pump out of ascending limb but water stays in tubule, medulla osmolarity is increased
in presence of ADH- collecting ducts are very permeable to water- tubular fluid becomes very concentrated
movement of water carries urea to the medulla, contributing to its osmolarity
2 types of countercurrent mechanisms
countercurrent multiplication- progressively increasing osmotic gradient is formed in interstitial fluid of renal medulla as a result of countercurrent flow
countercurrent exchange- solutes and water are passively exchanged btwn blood of vasa recta and interstitial fluid of renal medulla as a result of countercurrent flow
countercurrent exchange
nephron loop and duct cells need nutrients and coygen from blood, capillaries (vasa recta) form loops like those of nephron loops in medulla, solutes and water are passively exchanged btwn blood of vasa recta and interstitial fluid of renal medulla as a result of countercurrent flow
incoming and outgoing blood have similar osmolarity which maintains medulla concentration gradient
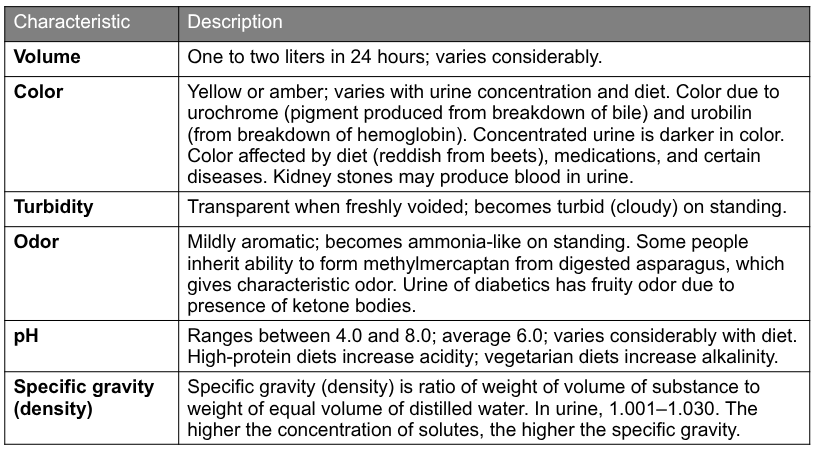
urinalysis
an analysis of the volume and physical, chemical and microscopic properties of urine called urinalysis reveals info abt the body, analysed by hospital/clinic lab or using reagent stripts (dipsticks)
ex- color, odor, pH, etc
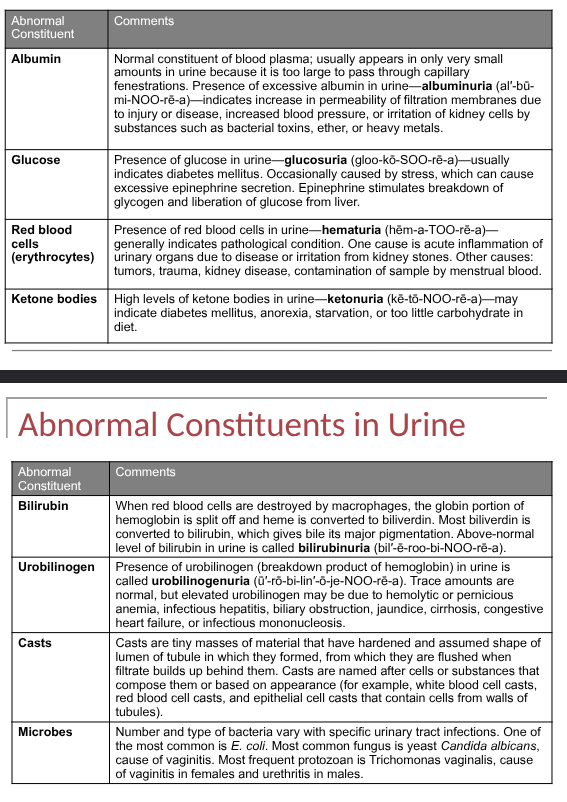
evalutes for presence of abnormalities: albumin, glucose, rbc, ketone bodies, microbes
normal urinalysis findings
abnormal constituents in urine
blood tests providing info abt kidney function
blood urea nitrogen (BUN)
plasma creatine
blood urea nitrogen test
measures blood nitrogen part of the urea resulting from catabolism and deamination of amino acids, when glomerular filtration rate decreases severly (may occur with renal disease or obstruction of uritnary tract) the BUN rises steeply
varies with protein intake and protein catabolism, better indicator for hydration status (increases in dehydration and kidney failure), adult normal range is 8-26 mg/dl (3.6-7.1 mmol/L)
Plasma creatine
normal value (0.5-1.2 mg/dL or 15.3-76.3 umol/L)
value above 1.5 indicates poor renal function, creatinine produced by muscles, most valuble for monitoring progress of chronic (not so much acute) renal disease, measures progressive renal dysfunction
renal plasma clearance
determines how much of a substance can be cleared from the blood by the kidneys during a given unit of time, permits indirect meaure of GFR, tubular secretion, tubular reabsorption and renal blood flow, clearance in INULIN gives the glomerular filtration rate, clearance of para-aminohippuric acid gives rate of renal plasma flow
GFR vs creatinine clearance
GFR- best estimate for the functioning of renal tissue, uses INULIN (fructose polysaccharide)
Creatinine Clearance- estimate of GFR, only one blood sample is required in addition at a 24 hr volume of urine (normal- 120-140 mL/min)
urine transportation and storage
urine drains through papillary ducts into minor calyces which join to become major calyces that unite to form renal pelvis, then drain into the ureters, then bladder then urethra
ureters
each ureter transports urine from a renal pelvis by peristaltic waves, hydrostatic pressure and gravity, ureters are retroperitoneal and consist of a mucosea, muscularis and adventitia
bladder
no anatomical valve at opening or ureter to bladder, when bladder fills it compresses the opening to prevent backflow, bladder is hollow muscular organ posterior to pubic symphysis (700-800 mL capacity)
floor of bladder is a small smooth triangular area called the trigone, ureters enter bladder near posterior points in trigone, the urethra drains bladder from anterior part of trigone
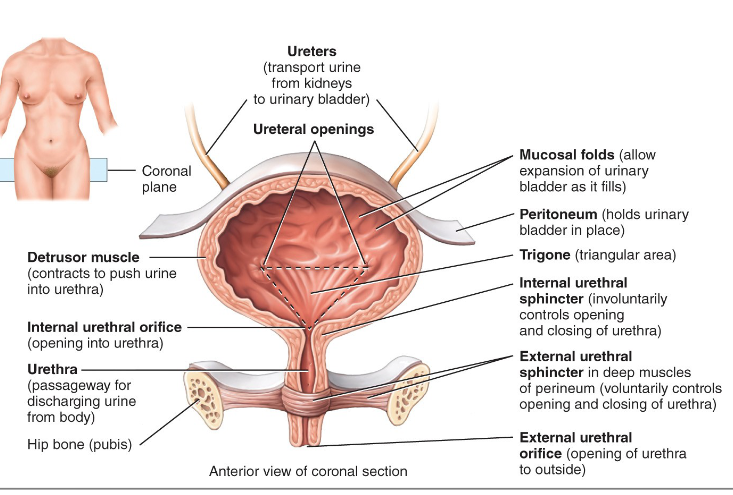
bladder histology
mucosa (mucuosal folds), lamina propria, muscularis (detrusor muscle) and adventitia/serosa)
area around opening of urethra- the circular fibers of the muscularis form the internal urethral sphincter
below the internal sphincter is the external urethral sphincter, which is composed of skeletal (voluntary) muscle
micturition reflex
urine expelled through bladder by act called micturition (urination or voiding), voluntary and involunatary muscle contractions, when volume reaches 200-400mL- strethc receptors in bladder wall transmit impulses to initiate spinal micturition reflex, older children and adults may initiate or inhibit micturition volunarily
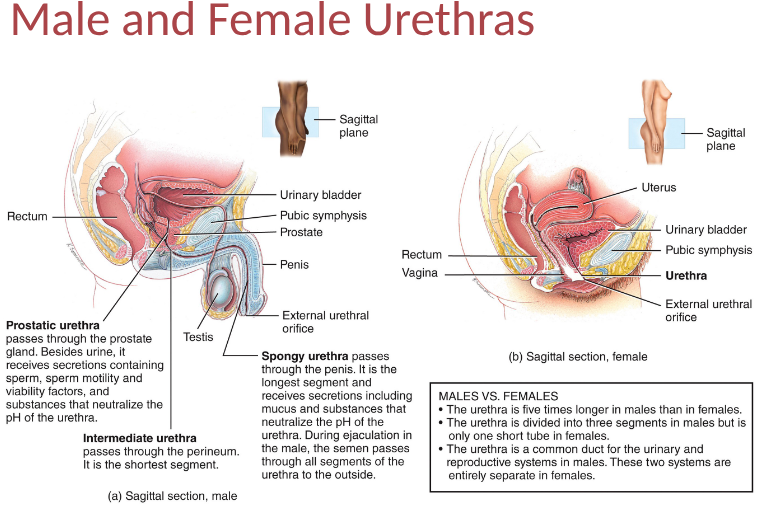
urethra
tube carrying urine from internal urethral orfice to the exterior of body, wall of urethra has 3 coats in females and 2 coats in males, urethra discharges urine as well as duct and ejaculation of semen in males,
waste management in other body systems
buffers- bind H+ to manage acidity
blood- transports waste
liver- metabolic recycling- turns toxic substances less toxic (ammonia and urea)
lungs- CO2, H2O and heat
sweat glands- heat, water, CO2, salts and urea
GI- solid undigested foods, waste, CO2, H2O, salts and heat
aging and urinary system
after 40 effectiveness of kidnyes decreases, kidneys shrink, decrease blood flow to kidneys bc glomerular vessels are damaged or fewer, decrease in filtration, increased bladder symptoms (urgency, frequency, nocturia), decreased elimination of drugs
renal calculi
kidney stones, crystals of calcium oxalate, uric acid, calcium phosphate
glomerular disease
damage to golmerulus and permeability increase: glomerulonephritis (urine contains blood and protein), nephrotic syndrom (urine contains protein)
urinary tract infections
more common in females, painful or burning urination, urgent and frequent urination, low back pain, bed wetting- infections such as urethritis, cystitis, pyelonephritis
renal failure
decrease or cessation of glomerular filtration, acutra renal failure and oliguria/anuria, chronic renal failure, may be caused by low blood volume, decreased cardiac output, kidney stones, contrast dye, NSAIDs, antibiotics, diabetes, liver disease
kidney transplant
kidney from donor to receipent, live or deceased donor, nonfunctioning kidneys left in place
cystoscopy
allow direct examination of urethra, bladder and prostate
body fluids
bodw water + dissolved substances, regulatory mechanisms ensure homeostasis of body fluids since their malfunction may seriously endanger nervous system and organ functioning
body fluid percentages
in adults- 55-60%
infants- 75% (in premature it is higher)
older persons- decreased intracellular fluid
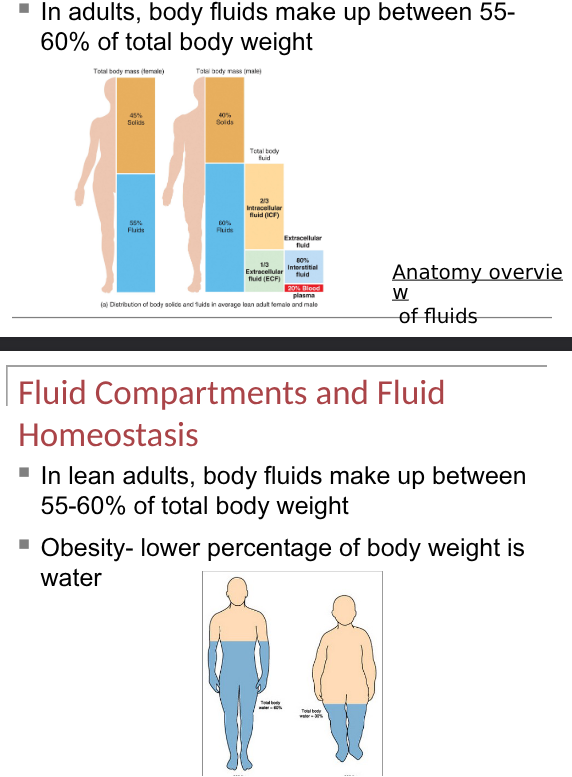
fluid compartments and fluid homeostasis
inside cells (intracellular fluid is called cystol) and outside cells (extracellular fluid is interstitial fliuid (80%) and blood plasma (20%)
selectively permeable membranes seperate fluids
plasma membrane- intracellular fluids from interstitial fluid
blood vessel walls- interstitial fluid from blood plasma
capillary walls- allow exchange of water and solutes btwn blood plasma and interstitial fluid
extracellular fluid
interstitial fluid, intravascular fluid (blood), CSF, pleural, peritoneal, pericardial fluids, sweat, urine, lymph, synovial fluid
fluid balance
means various body compartments contain required amt of water, osmosis is primary way in which water moves in and out of components- determined by solutes, filtratio + reabsorption + diffusion and osmosis allow continous exchange of water and solutes among compartments
solutes in body fluids
mostly electrolytes that dissociate into ions, fluid balance is not just water but also electrolyte balance,
fluid homeostasis
gains water- ingestion and metabolic synthesis
loses water- urination, perspiration, exhalation, feces
osmosis
how water moves btwn intracellular and extracellular fluid compartments
passive transport
occurs when water, solutes and small electrically uncharged molecules move through pores, doesnt require energy, high conc to low conc, osmosis, hydrostatic pressure and diffusion
active transport
larger molecules and molecular complexes, requires energy, moves molecules across concentration gradient, protein mediated, ex- postassium sodium pump
water loss and gain
largest constituent in body, varies from 45-75 percent of body weight depending on age and fat, fluid intake usually equals output so body maintains constant volume
regulation of water gain
metabolic water volume depends mostly on level of aerobic cellular respiration which reflects demand for ATP in body cells, main way to regulate body water balance is by adjusting volume of water intake, when water loss is greater than gain- cause dehydration, stimulation for fluid intake is thirst sensation
thirst sensation
renin angiotensin ll pathway responds to decreased blood volume/pressure and so stimulates the thirst centre in hypothalamus , altered thirst sensation or restricted access to fluids: elderly, infants, confused mental state
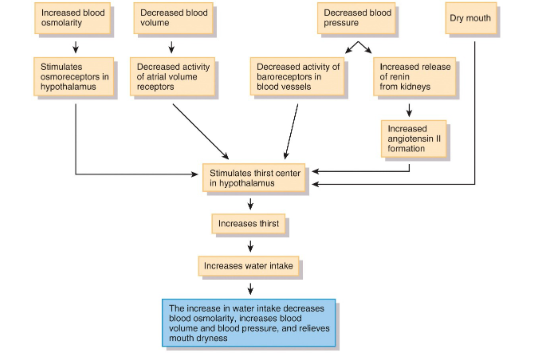
dehydration
decrease in volume and an increase in osmolarity of body fluids, triggers osmoreceptors in hypothalamus, volume receptors in atria, baroreceptors in blood vessels, neurons in mouth that detect dryness
regulation of water and solutes lost
mainly depends on urine, amt of urinary salt loss is main factor for determining body fluid volume, main solutes in extracellular fluids are sodium and chloride (wherever solutes go, water follows)
daily water loss
fluid output adjusted by antidiuretic hormone, atrial natriuretic peptide, angiotensin ll and aldosterone,
control Na and Cl: angiotensin ll, aldosterone, ANP
control water loss: ADH
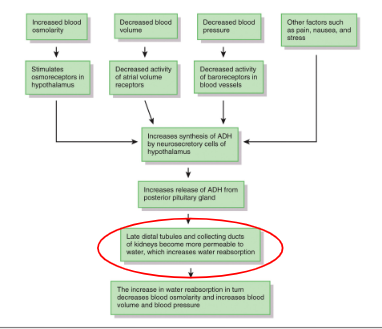
ADH
released when there is an increase in plasma osmolarity or decrease in circulating blood volume, acts on kidney to promote reabsorption of water
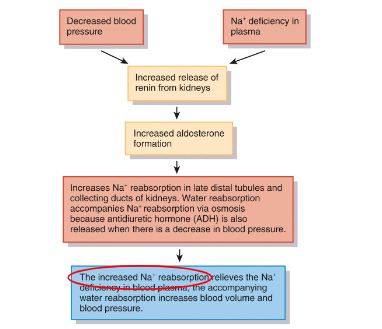
Aldosterone
increased reabsorption of sodium by distal tube of kidney
ANP
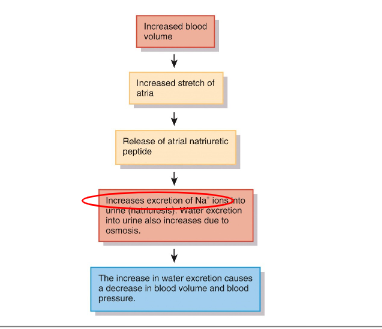
regulation of water and solute loss summary
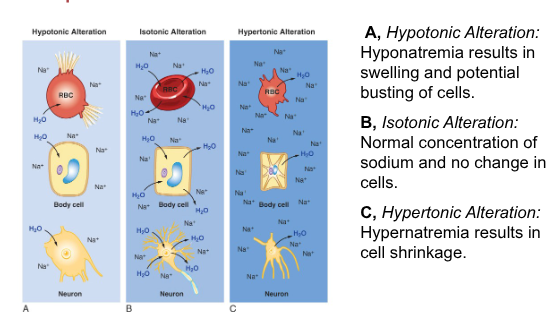
movement of fluids btwn body fluid compartments
fluid imbalance btwn intracellular and interstitial fluids can be caused by a change in their osmolarity, most often a change is due to change in Na+ conc.
when extracellular fluid is isotonic to cells of body- cells dont swell or shrink, however changes in the osmolarity can cause shrinking or swelling of cells
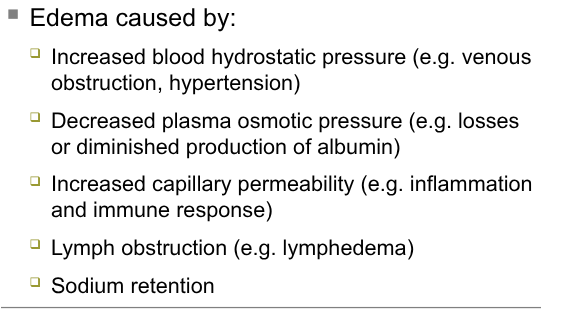
edema
accumulation of fluid in interstitial spaces, increased risk for tissue damage, can be in extremities heart or lungs, dependent edema, putting edema
causes: image
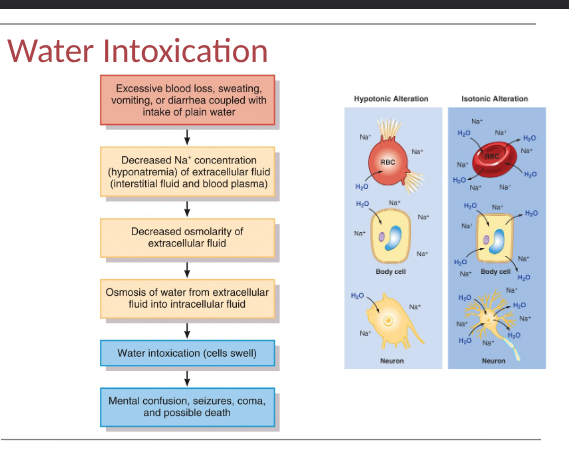
water intoxication
when water is consumed faster than kidneys can excrete, water intoxication can occur- when excess body water causes cells to swell dangerously
enema
introduction of solution into the rectum to draw water and electrolytes into the colon osmotically, increased volume increases peristalsis which evacuated feces, used to treat constipation, repeated use of enemas can increase risk of fluid and electrolyte imbalances
electrolytes in body fluids functions
many of them, so control osmosis of water btwn body compartments
maintain acid base balance for normal cellular activities
carry electrical current which allows production of APs and GPs and controls secretion of some hormones and neurotransmitters
cofactors needed for optimal activity of enzymes
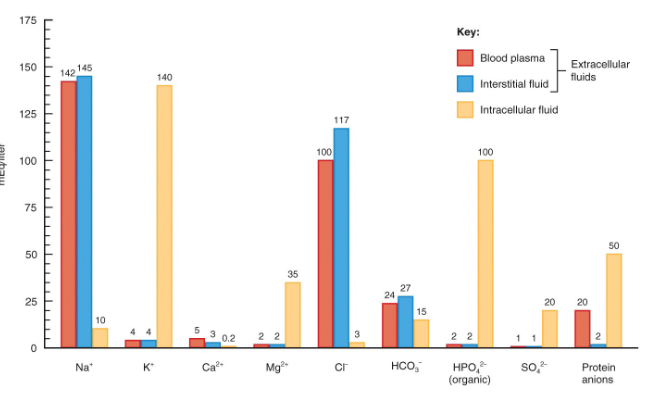
electrolytes in body fluids
dissolved particles in body fluids, electrically charged, ions with opposite charges attract, (mEq/liter), blood plasma, interstitial fluid and intracellular fluids have different conc of elecrolytes and protiens, (blood plasma has many proteins while interstitial fluid has few
know functions of electrolytes
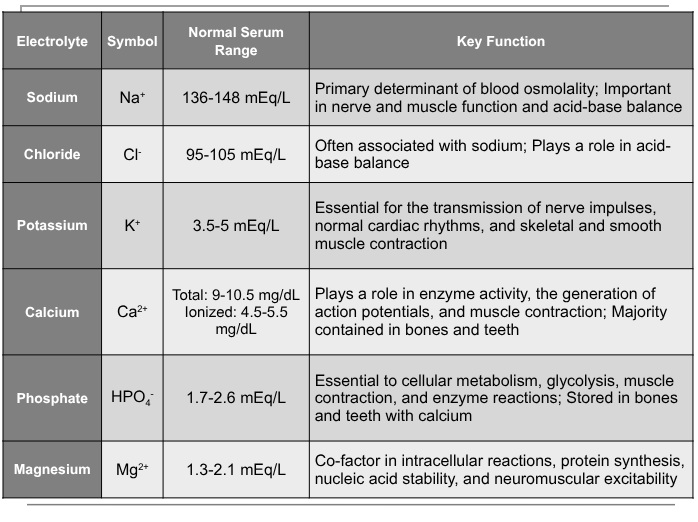
sodium
kidneys excrete most sodium and conserves it during periods of sodium restriction, controlled by ANP and ADH indirectly,
hyponatremia (less than 136 mEq/L)- caused by fluid loss and causes plasma hypoosmolarity and cellular swelling, hypovolemia
symptoms: muscle weakness, dizziness, headahce, hypotension, tachycardia, shock, mental confusion, stupor, coma
hypernatremia (over 148 mEQ/L)- caused by dehydration, excessive sodium and causes water movement from ICF to ECF (intracellular dehydration)
syhmptoms:intense thirst, hypertension, edema, agitation and convulsions