5. Investigation and management of convergence and accommodation anomalies
1/42
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
what makes the near triad
convergence
accomodation
pupil miosis
what are the primary causes of convergence insufficiency CI
illness
fatigue
drugs
antidepressants
pregnancy
what are the secondary causes of convergence insufficiency CI
heterophoria
presbyopia
uncorrected rx
accom insufficiency
thyroid eye disease
what are the symptoms of convergence insufficiency CI
headaches
eyestrain
sore eyes
difficulty changing focus
blurred vision caused by XOP breaking down
how would you test convergence insufficiency
NPC
jump convergence
CT- decompensated xop may be present
fusional reserves
convegent FR may be low
VA- low VA at near
stereoacuity- may be low
ocular motility
what are normal NPC values
should be 8cm
ideally 5cm
what is convergence paralysis
The ability to converge closer than infinity is entirely lost
In convergence paresis some ability to converge is retained
what are the causes of convergence paralysis
closed head injury, viral illness, occlusive vascular disease, multiple
sclerosis, encephalitis
what are the symptoms of convergence paralysis
diplopia and blurred vision at distances closer than infinity
what are the signs of convergence paralysis
• XOT at distances closer than infinity
• Accommodation may be normal, reduced or absent
• Pupillary response may be absent for convergence and present for light
• Normal ocular movements
• Absent positive fusion range good negative fusion range
• Examined in exactly same was as CI (NPC, jump convergence, CT)
what is accomodative insufficiency
Inability to obtain or maintain adequate accommodation for comfortable
binocular vision at near
what are the causes of accom insuffieincy
High hypermetropia, illness, drugs, trauma, infection, prolonged fever
what are the symptoms of AI
Blurred vision at near, asthenopia, micropsia
what is accomodative fatigue
Inability to sustain adequate accommodation over time. It is usually due to
repeated or sustained visual effort
what are the causes of accom fat
poor general health, fatigue, psychological, drugs
what are the symptoms of accom fat
Near vision is initially normal, but then reduces over time
may be a near SOP
what is accomodative infacility (inertia)
Inability to adequately change accommodation
what are the causes of accomodative infacility
accommodative spasm, uncorrected hypermetropia, presbyopia,
excessive amounts of close work at too close working distance
what are the symptoms of accomodative infacility
blurred vision when changing fixation from near to distance or
distance to near, both distance and/or near vision may be reduced
what is accomodative paralysis
The ability to accommodate to near objects is entirely lost. No accommodation can be exerted
what are the causes of accomdative paralysis
convergence paralysis
neurological (3rd. nerve pasly, Parinaud's syndrome)
trauma
what are the symptoms of accomodative paralysis
blurred vision for distances closer than infinity
what is convergence/accomodative spasm
Spasm of convergence usually causes spasm of accommodation and miosis
what becomes contracted in convergence (1) and accomodative spasm (2)
1- medial rectus
2- cilary muscle
what are the causes of spasm
uncorrected hypermetropia, intermittent distance XOT, drugs/alcohol,
inflammation, very often of psychogenic origin, trauma, neurologic
(encephalitis, lesion in CNS)
what are the symptoms of spasm
blurred vision, intermittent diplopia, headache, asthenopia
how to use the RAF rule to diagnose what
near point of accom
RAF rule
assessed 3 times to help diagnosing AI and accom fatigue
assessed monocularly and binoculalry to help diagnosing AI and CI
how would you use accom facility test and what does it measure
measures rate of change of accommodation
done binocularly and monocularly
measure cycle per minute (8 is normal)
how would you use accom accuracy to diagnose accomodation anomolies
objetcive test
accom lag measured using dynamic ret (MEM or Nott)
how to manage CI
Treat any pathology
correct any refractive error
cycloplegic refraction should be conducted when appropriate
CI nearly always be treated successfully using orthoptic exercises
secondary CI need to address the primary condition so refer if ocular diseases detected
anti suppression tests
bar reading
dot card
stereograms
base out prism
describe the 2 orthoptic exercises to manage CI
pencil-to-nose
-Patient is asked to look at a pencil at 50cm and maintain single and clear vision while the pen is moved towards the patient's eyes
- Patient reports when the pencil is double and stops
- Try and bring convergence closer by repeating exercise
near-far jump
-Fixation 'jumps' between near and distance targets
-- Prior to 'jumping' to other distance patient should see target clear and single
- The patient should ensure that he/she sees the object clear and single before 'jumping' to the other distance
how would you manage convergence paralysis
-Pathology (if any) treat and/or refer for treatment accordingly
• If early onset refer for ophthalmological examination
• Botulinum toxin
• Occlusion
• Base in prisms
• Surgery
how would you manage accom insufficiency
• Pathology (if any) treat or/or refer for treatment accordingly
• Correct refractive error, particularly hypermetropia (consider cycloplegic
refraction, if appropriate)
• SV for reading, progressive or bifocal
• If patient is not keen on glasses try orthoptic exercises
what 2 tests for managing AI
accom push up
lens flippers
how to manage accomodative fatigue
• Pathology (if any) treat or/or refer for treatment accordingly
• Correct refractive error, particularly hypermetropia (consider cycloplegic
refraction, if appropriate)
• Orthoptic exercises (same as AI)
- Accommodative push-ups
- Lens flippers
how would you manage accom infacility
• Pathology (if any) treat or/or refer for treatment accordingly
• Correct refractive error, particularly hypermetropia (consider cycloplegic
refraction, if appropriate)
• Bifocal for reading with a low add (+1.00) may help
• Orthoptic exercises
- Accommodative push-ups
- Lens flippers
- Near-far jump exercises (ensure patient keeps letters single and
clear)
how would you manage accom paralysis
• Pathology (if any) treat or/or refer for treatment accordingly• Correct refractive error, particularly hypermetropia (consider cycloplegicrefraction, if appropriate)• SV for reading, progressive or bifocal
how would you manage convergence/accom spasm
• Pathology (if any) treat or/or refer for treatment accordingly
• Correct refractive error, particularly hypermetropia (consider cycloplegic
refraction, if appropriate)
• Short period of atropine instillation (with plus lenses to help near work)
• Monocular occlusion
• Botulinum toxin to the medial rectus
• Psychological counselling (given that it is often associated to psychological
conditions)
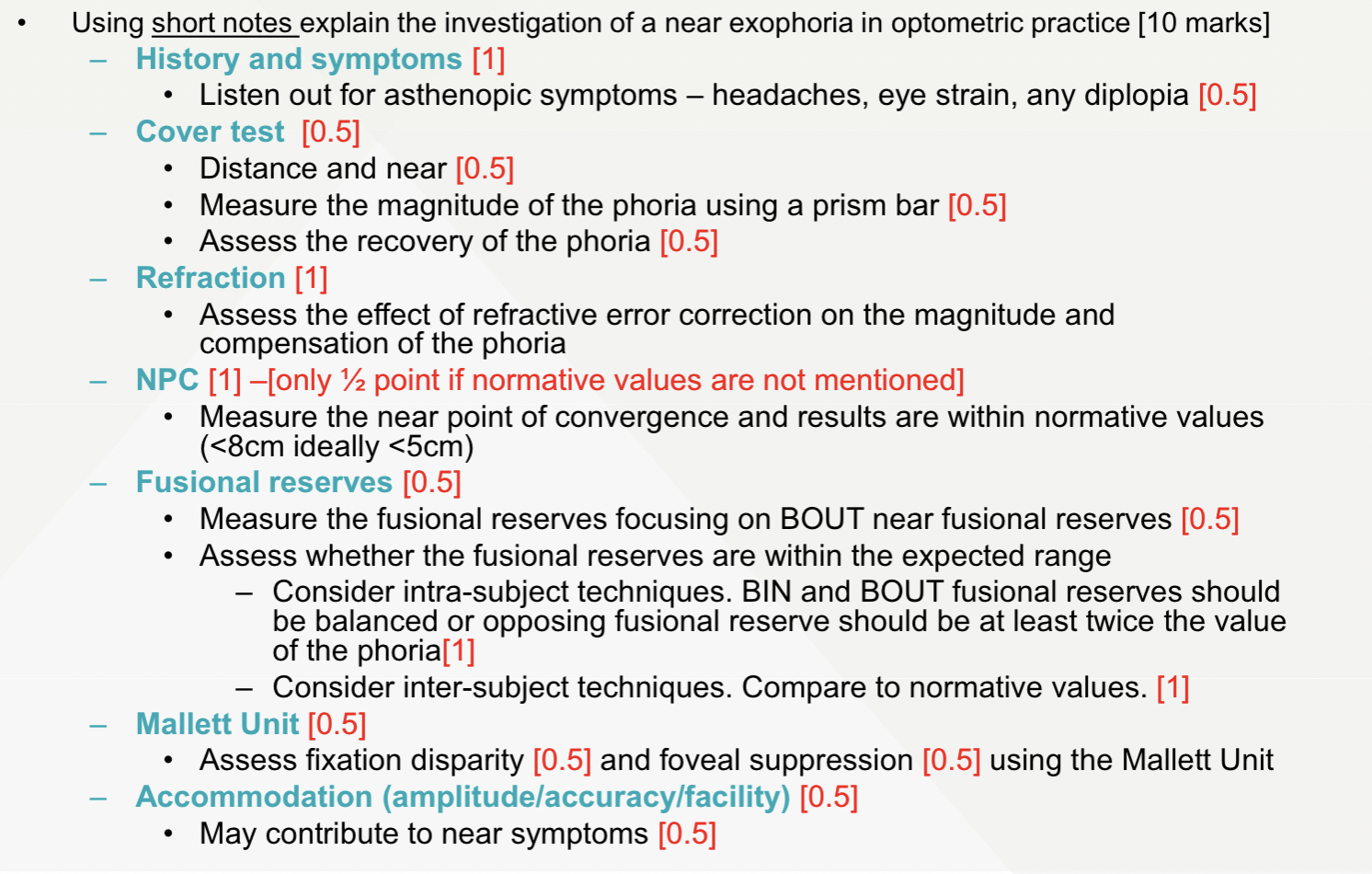
Using short notes explain the investigation of a near exophoria in optometric practice [10 marks]
You perform MEM retinoscopy on a
patient (with the subjective refraction in
place) and find -1.00D RE and LE.
Which is the most likely diagnosis?
1. Accommodative insufficiency
2. Accommodative excess
3. Accommodative lag
4. Accommodative inertia
5. Convergence insufficiency
2
Which one of the following is not a
treatment for a decompensated
heterophoria at near?
1. Fusional reserves training
2. Refractive error modification
3. Prismatic correction
4. Flipper exercises
5. Exercises using stereograms
4
At a working distance of 33 cm you
measure 10Δ XOP for a –2.00DS myope
without their glasses. With the glasses on
you record a 2 Δ SOP. Using this
information what is the AC/A ratio for this
patient?
1. 2:1
2. 4:1
3. 6:1
4. 8:1
5. 10:1
3