Lecture 2 TOD and PM changes/ Courts and expert witness
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
Observations/measurements
Livor mortis (lividity)
Rigor mortis (rigidity)
Algor mortis (body temperature/cooling)
Degree of decomposition
Insect activity
Chemical changes in the vitreous humor
Gastric contents
Scene investigation clues
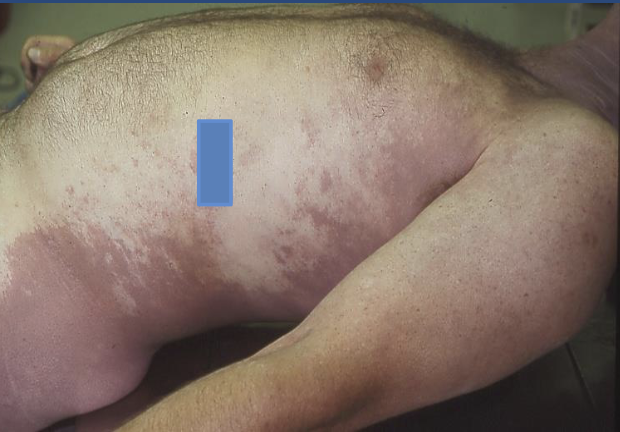
Livor Mortis (lividity)
Postmortem hypostasis
Accumulation of blood
in small vessels
Dependent on gravity
Can be misinterpreted
as bruising
Reddish-purple
(dependent on body
pigmentation)
Blanched areas =
pressure from position
or clothing
Evident within ½ to 2
hrs after death
Maximal at 8 – 12 hrs
“fixed lividity” – test by
applying pressure
Has the body been
moved?
Darkest in areas most
gravitationally
dependent (ie, lower)
• Pale (blanched) areas
where body pressed
against surface or
object
• Difficult to assess in
darkly pigmented
individuals
• Early (blanchable) – can
shift if body is
moved/turned
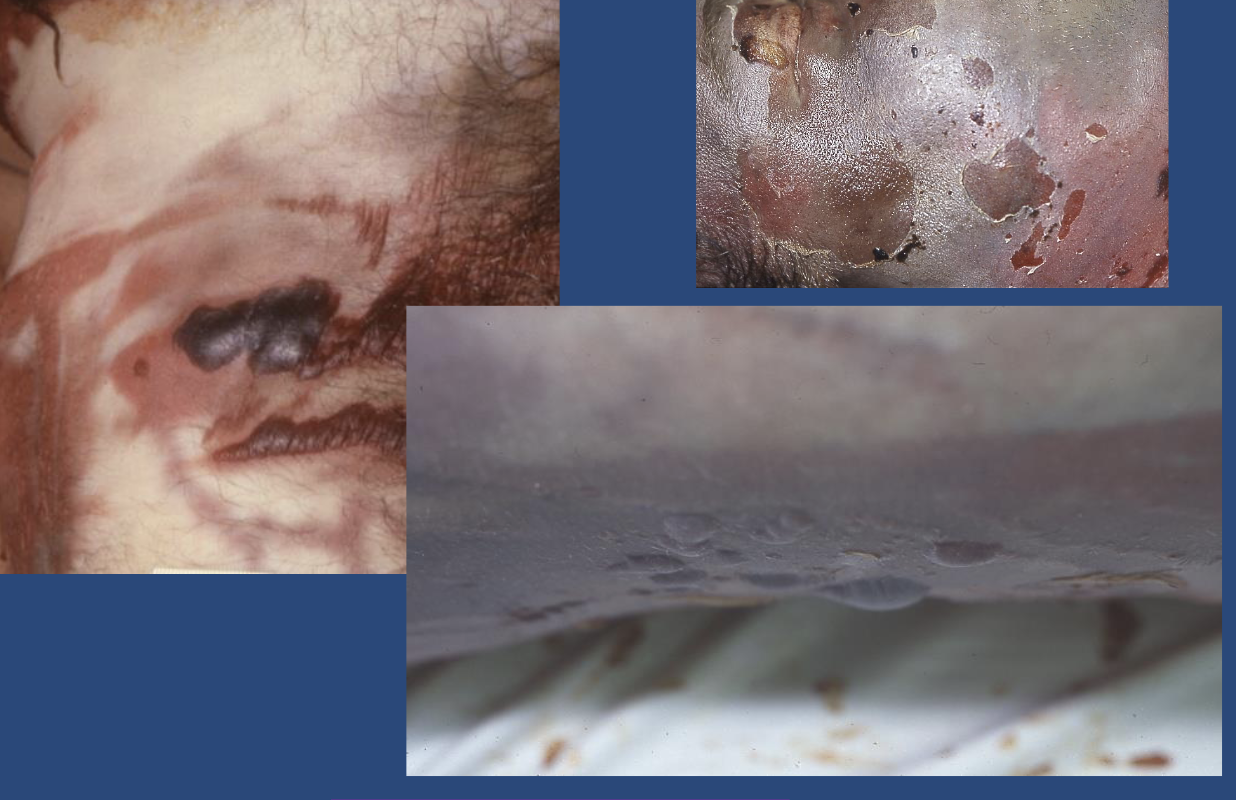
• Advanced (fixed) – can
develop pinpoint
hemorrhages (Tardieu
spots)
• May show in internal
organs as well
(posterior more
congested with blood)

Tardieu spots
First described in
hanging deaths
Increased dependency
(pressure)
Usually petechiae
(minute or pinpoint in
size)
Purpura (patches)
More common in
asphyxial or slow deaths
The three C’s
Cherry-pink lividity
‘C’ARBON
MONOXIDE
‘C’YANIDE
‘C’OLD
ENVIRONMENT

Rigor Mortis (rigidity)
Stiffening of the
body after death
(the”stiff”)
Disappearance of
ATP from the muscle
cells
Actin and myosin
filaments become
complexed
Remains until
decomposition
2 – 4 hrs = noticable
6 – 12 hrs = full
First evident in small
muscles (i.e. jaw)
12-12-12 hr rule in
“normal” conditions
Has the body been
moved?
Rigor Mortis: exceptions to the rule
Rapid onset with violent muscular exertion (as
seizures, exercise, drowning)
Can form and leave swiftly with elevated body
temperature (sepsis, hyperthermia)
Can persist for days in cool conditions
Delayed or very weak in emaciated persons
Very rapid onset in infants
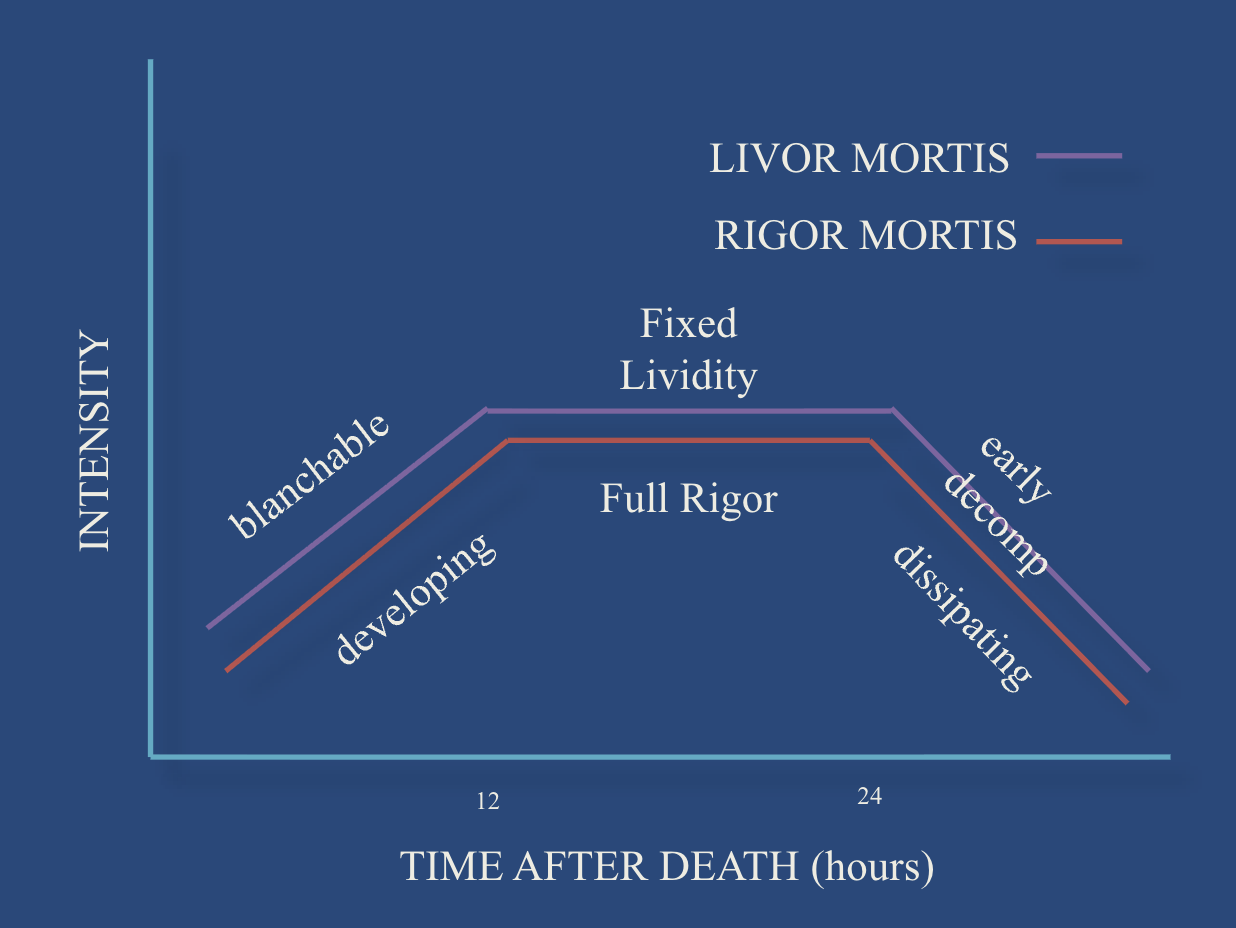
General chart for livor → rigor motis
Body temperature
Qualitative Assessment: generally used, as frozen,
cold, warm, or hot
Quantative Assessment: measurement
- important assumptions: normal body temperature
and uniform cooling
- time since death = 37 C – rectal T + 3
- time since death = 98.6 – rectal T
1.5
Caveats re: Algor
Low accuracy or reproducibility
– Conduction (contact heat), radiation (infrared,
solar), or convection (hot or cold air) may alter
– Altered if hypo/hyperthermic state prior to
death
– Slower with high body fat, or many clothes
– Faster with immersion in water, immature
individual/low body fat and high surface
area, or if there is a high gradient between
body and environmental temperature
When and How to take a body temperature
Cases where time of death is an issue and the time
interval is considered within hours
Usual: rectal temperature (make note of such and
watch for induced trauma)
Other methods: axillary; ear canal; incision into
liver
Record the temperature reading time
Two parts of decomposition?
Autolysis
Putrefaction
Autolysis
Breakdown of cells and organs
Aseptic chemical process (intracellular enzymes)
Accelerated by heat
Slowed by cold (stopped by freezing!)
Some organs faster than others
Putrefaction
Due to bacteria and fermentation
GI tract flora primarily responsible
Accelerated in septic individuals
Responsible for the odor
Two main variables: the environment and the
body
Sequence of events
#1
Greenish discoloration of the lower quadrants of
the abdomen (24-36 hrs)
Greenish discoloration of the head, neck, and
shoulders
Swelling of the face
Marbling (hemolysis of blood in vessels with
reaction of Hgb and H Sulfide)
Generalized bloating (60-72 hrs)
Green abdoment-first indication
#2
Vesicle formation
Skin slippage
Hair slippage
Diffuse green to green-black body color
Decomposition fluid (“purge”) from mouth and
nose
“Degloving” of the hand skin
Marbling
Hgb with HS along vessels

Generalized bloating

Vesicle/bleb formation
Dehiscence of surgical scars

Decomposition-variations
“mummification”
– occurs when
body has been
left in a very dry,
hot environment
(desert; enclosed
space in summer;
attic)
• Slows decomp
• Adipocere -
Bodies in water
or damp
environments
• Clostridium
bacteria make
enzyme that
hydroxylates
fatty acids
• AKA – grave
wax
Fats are hydrated and dehydrogenated;
takes several months; more likely in areas
of body having higher fat content (ie, thorax,
buttocks, thighs)
Adipocere

Insect Activity
Forensic entomology
Identification of the
type of insects and
the stage of
development
Flies – most common
Eggs to maggots to
pupa (6 – 10 days)
Collection of proper
specimens
Blowflies most commonly
associated with corpses;
eggs laid at hours to 1-2
days after death
• Blowflies arrive first
• Immediate activity if
daylight
• Ovipositing (egg laying) in
mouth/orifices/wounds first
• Larvae can ingest 95% of the
body mass
Blowflies: Biological Clocks
• Larvae (“maggots”)
undergo 3 moults
(instars), 6-10 days,
eating their way to
adulthood
• Largest (3rd instar)
migrate away from
body to find cool,
dark area to generate
pupal casing
• Pupae hatch into flies,
12-18 days,
depending on exact
species
(Genus Calliphoridae)

Pupal casings

Insect activity-Ants/roaches
Vitreous potassium
K+ increases after
death from cellular
breakdown
Generally reliable
rate of increase
However: potential
for variability is + 10
hrs in the 1st 24 hr
(and much higher
beyond!)
Gastric emptying
Attempt to establish a time interval between eating
and death – BEWARE!!
“small meal” digested in 1 hr, “large meal” takes 3
to 5 hrs (Spitz and Fisher)
“light meal” digests in ½ to 2 hrs; “medium meal” 3
to 4 hrs; “heavy meal” 4 to 6 hrs (Adelson)
“meal emptying time is a variable phenomenon in
healthy subjects with significant differences from
day to day in the same and in different individuals”
(Brophy et al.)
Scene investigation clues
Uncollected mail or newspapers
Whether the lights are on or off
TV schedule opened to a time and date
How the individual is dressed
Any food out or dirty dishes about
Sales receipts or dated slips of paper (check
clothing)
When last seen or routine change observed
Cardiac pacemaker / implantable
defibrillator
Smart watch
Cell phone
Last text, etc.
How best to state a TOD?
Evaluate all three (lividity, rigidity, body
temperature) together
Evaluate with the historical information
Evaluate with the environmental conditions in mind
Evaluate the individual (body size, clothing, general
health)
Then, give a range estimation only…..
AI
Anthropophagy
Most common: house hold pets


Tache Noire
Post mortem artifacts
anthropophagy
Tache noire
Dismemberment
CIVIL & CRIMINAL CASES
• CIVIL CASES
– Dispute between 2 or
more parties.
– Plaintiff – files
complaint.
– Serves copy of complaint
on defendant.
– Monetary compensation
or cease & desist
defendant’s actions.
• CRIMINAL CASES
– Prosecutor Attorney
representing govt.
– Defendant or group of
defendants.
– Defendant if guilty -
is sentenced – Prison /
fine.
– Defendant if not
guilty- is released.
CIVIL CASE PROCEDURE
• Plaintiff files complaint against Defendant.
• “Discovery” – Provide relevant documents to each
other including copies of documents, identity of
witnesses.
• Process of assembling the evidence.
• Submits “motions” for court ruling.
• “Deposition” – answer questions under oath, in
presence of court reporter.
• Mediation / Arbitration - Settlement
If no “Settlement” then “trial” is scheduled.
• At trial witnesses testify under supervision of a
judge who applies rules of evidence.
• Witnesses may be sequestered.
• Court reporter keeps record of proceedings.
• Clerk of court keeps record of documents.
• “Objection” if witness says something not based on
witnesses personal knowledge.
• Judge makes ruling on objection.
At conclusion of evidence each side gives a closing
argument.
• Judge explains the law to the jury.
• Jury to decide if defendant harmed plaintiff.
• Plaintiff must convince jury by a “preponderance
of evidence” i.e. “More likely than not” that
defendant is responsible for the harm that plaintiff
has suffered.
• Occasionally “bench” trial – no jury.
“Discovery”
Provide relevant documents to each
other including copies of documents, identity of
witnesses.
“Deposition”
answer questions under oath, in
presence of court reporter
CRIMINAL CASES – PROCEDURE
• Prosecutor and Defendant.
• Prosecutor presents evidence to “Grand Jury”.
• Which reviews if there is “probable cause” or
sufficient evidence to require a defendant to stand
trial.
• If so, Grand Jury renders an indictment.
– Defendant arrested if not already in custody.
• Initial appearance – Judge advises the defendant of
the “charges” filed.
• Determines “probable cause” & release or jail.
Defendants not able to afford an attorney –
appointed a public defender or private attorney.
• “Arraignment” – When defendant enters a plea to
the charges made by prosecutor.
• “Guilty” plea and “plea bargain”.
• If defendant pleads guilty the judge normally will
schedule a “hearing” to determine the “sentence”
after review of pre-sentence review and other
documents.
If no guilty plea – limited discovery & motions
to suppress evidence if obtained in violation of
constitutional rights.
• Burden of proof is on prosecutor – standard is:
“beyond a reasonable doubt”.
• Defendants do not have to prove innocence
only prove “room for doubt”.
• Jury decides guilt or not.
• If guilty then defendant sentenced. If not guilty
then defendant is released “Acquittal”.
“Arraignment”
When defendant enters a plea to
the charges made by prosecutor.
STRUCTURE OF FEDERAL COURTS
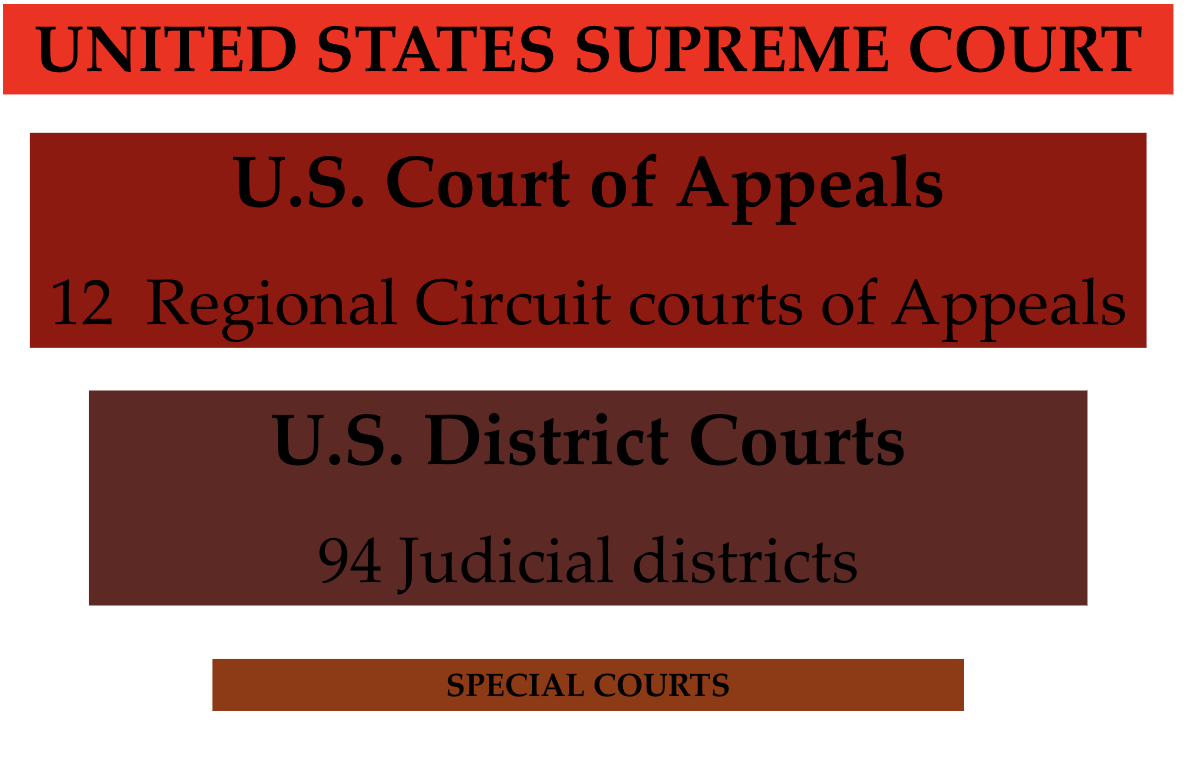
JURISDICTION OF FEDERAL COURTS
Limited jurisdiction – only certain type of
cases as determined by Congress.
• Must be actual cases not hypothetical
issues.
• Plaintiff aggrieved or legally harmed.
• Usually involves cases where
– “Federal question” involves federal laws.
– A litigation against a state government.
– Citizens of different states.
– Potential damages above $75,000.
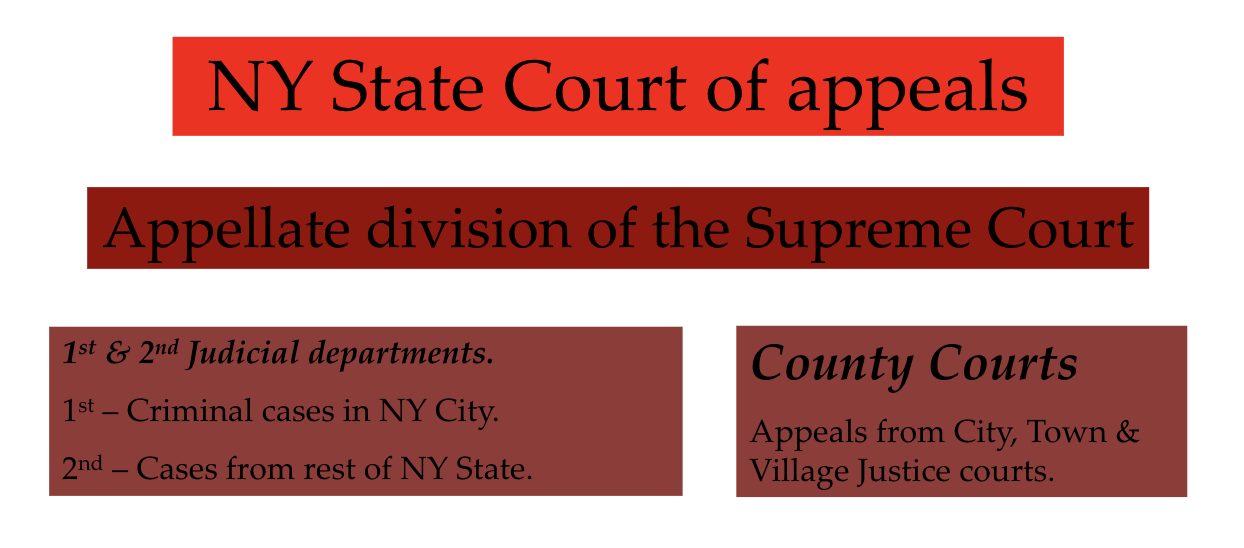
STRUCTURE OF CRIMINAL
COURTS IN NEW YORK –
Appellate courts.
The Scientific Method
• Scientific method: using observation and
theory to test scientific hypotheses
• To be scientific, a method of inquiry must be
based on gathering observable, empirical and
measureable evidence subject to specific
principles of reasoning
• Collection of data through observation and
experimentation, formulation and testing of
hypotheses
Scientific Report
• Objective
– Materials/Methods
– Data/Results
• Measurements, descriptions, observations
• Photographs
• Subjective
– Analysis of data/results
– Diagnoses, conclusions, discussion, opinion
• Separation
• Another expert should be able to read your
report and, based on the objective data in the
report, be able to come to an independent
conclusion
• Not be told by author what they should
conclude
• Now, 6 months from now, or 6 years from
now.
• Opinions
– Differ
– May change with time, additional information,
etc.
– Often best left for courtroom
Importance of objectivity
• Description
• Observation
• Documentation
• NOT determination/diagnosis
Daubert
• The Daubert standard is a rule of evidence
• Prohibits unqualified expert testimony
• Judge is the “gatekeeper”
• Expert’s testimony must be 1) relevant; and 2)
reliable, “rests on a reliable foundation”, to a
“more likely than not” standard of finding by the
judge.
• A conclusion qualifies as scientific knowledge if
the proponent can demonstrate that it is the
product of sound scientific methodology a/or
derived from the scientific method
Some features of acceptable
scientific knowledge
• Empirical testing – testable technique
• Subject to peer review and publication
• Known or potential error rate.
• Standards and controls must exist.
• Theory/technique generally accepted by a
relevant scientific community.
– Daubert supersedes the Frye rule in federal court,
and some state courts; Frye rule only required
general acceptance by a relevant scientific
community.
Challenges Identified in NRC Report
• Disparities in FS community
• Lack of mandatory certification and
accreditation or standardization
• Broad range of disciplines with differing
guidelines
• Interpretative nature of forensic evidence
• Need for research to establish limits and
measures of performance
• Admissibility of FS evidence in litigation
• MANDATORY laboratory accreditation
• Establish routine QA/QC measures
• Establish a national code of ethics for all
forensic science disciplines
• Improve graduate education programs
• Political pressures on work/results
Cognitive Bias
• Systematic “error” in way of thinking that
effects decisions and judgement
• Unconscious
• 175+
• Anchoring
• Band-wagon effect
• Placebo effect
• IKEA effect
Contextual Bias
• Judgement influenced by information
irrelevant or inappropriate for the task
• Interpreting data based on extraneous
information which is NOT NEEDED to reach a
determination
Confirmation Bias
• Tendency to look for, interpret, favor and
recall information that supports one’s
hypothesis and ignore falsifying information
• Spinning
– Gun control
– Politics
– Forensic
– Experimental
Practice of medicine
• History most important component of
diagnosis (56-76%)
• Physical exam (17-18%)
• Laboratory data (2-3%)
• Clinical medicine
– SOAP
Evidence and Witnesses
• Types of Evidence:
• Written or documentary.
• Certificates and reports.
• Oral testimony as affidavits.
• Types of Witnesses:
• Witness to fact.
• Expert witness.
• Forensic witnesses are usually expert.
Forensic Pathologists
as Expert Witness
• Usually perceived as impartial.
• Full time specialists in medico-legal cases.
• Experienced in police & judicial procedures.
• They or their staff, including investigators or
laboratory personnel have gathered the
evidence, performed the examination,
preserved and are presenting the evidence.
• Normally opinion is not disputed, though there
may be disagreements on interpretation.
Tactics during Cross-Examination
• Attempt to upset, frighten, anger, embarrass,
humiliate the witness.
• Witness versus printed authority.
• Answer question with “yes” or “no”.
• Repeated explanation.
• Repeating a previously given answer with
slight distortion.
• Question with several different questions.
• Occasionally, testimony in previous cases.
What part of the death certificate does blunt force injury go
Part 1 or part 2
Skin tags
Point to the direction from where the force is coming from
Battle sign
Brusing behind ears
Avulation
Skin flap
hematoma
nitial Stages (Days 1–3): The hematoma appears red, blue, purple, or black as blood pools and oxygen is lost.
Transition to Green/Yellow (Days 5–10): The body breaks down hemoglobin into biliverdin (green) and then bilirubin (yellow), causing the bruise to change color.
Final Stage (Golden/Brown, Days 10–14+): The yellow color deepens to a golden brown as hemosiderin is formed, which is the final stage of breakdown before the bruise is reabsorbed.
What Gold Means: A gold or yellow color is a positive sign that the body is effectively breaking down the old, pooled blood
Brain hemorrhages
Intracerebral Hemorrhage (ICH): Bleeding occurs directly within the brain tissue itself.
Subarachnoid Hemorrhage (SAH): Bleeding occurs in the area between the brain and the thin tissues covering it.
Subdural Hemorrhage: Bleeding occurs between the surface of the brain and the dura mater (outer membrane).
Epidural Hemorrhage: Bleeding occurs between the skull and the dura mater
Basilar skull
back
cambium
skull cap
Subgaleal hemorrhage
No pressure on brain bc of scalp A subgaleal hemorrhage is a rare, potentially fatal neonatal condition where blood accumulates in the loose connective tissue between the skull periosteum and the scalp aponeurosis. Caused by ruptured emissary veins during birth—often via vacuum or forceps—it presents as a soft, boggy, shifting scalp swelling, risk of hypovolemic shock, and a ~20–25% mortality rate.
Flail chest
Flail chest is a life-threatening injury occurring when
≥3is greater than or equal to 3
≥3
adjacent ribs are fractured in
≥2is greater than or equal to 2
≥2
places, creating a free-floating, unstable segment that moves paradoxically (sucking in on inhalation, pushing out on exhalation). It causes severe pain, respiratory distress, and potential hypoxia. Caused by major blunt trauma (e.g., motor vehicle accidents), it requires prompt hospital care, including pain management, oxygen, and potential surgical fixation
.
Alanto occipital dislocation
a rare, life-threatening injury involving the separation of the skull from the cervical spine, often termed "internal decapitation". It is a high-energy trauma injury (e.g., motor vehicle accidents) frequently causing immediate fatality due to severe brainstem or spinal cord damage, though survival is increasing with early detection and surgical stabilization, commonly via occipito-cervical fusion