Spirometry Lab
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
What does spirometry measure?
airflow and corresponding changes in lung volume
Inspiratory Reserve volume (IRV)
The maximum volume above the tidal volume that we can inspire into our lungs (~3L)
Tidal Volume (VT)
Volume we inspire and expire during restful breathing.
Normally the rate of breathing is 10-12 respiratory cycles per minute and Vt is ~0.5L
Expiratory reserve volume (ERV)
Maximum volume below the tidal volume that we can expire from our lungs (~1.5L)
Residual Volume (RV)
Volume of air remaining in the lungs after full expiration (~1.2L) as we can never empty the lungs completely
Inspiratory capacity (IC)
the total amount of air that can be inspired after a tidal expiration:
= TV + IRV
Expiratory Capacity (EC)
All the air exhaled in a maximal expiration after a normal inspiration.
= VT + ERV
Functional Residual Capacity (FRC)
the amount of air in the lungs after a tidal expiration:
= ERV + RV
Vital Capacity
All the air that can be expired from a maximal inspiration
= IRV + VT + ERV
Total lung capacity
All the air that it is possible for the lungs to contain
= IRV + VT + ERV + RV
Directly measurable lung volumes
VC
IC
IRV
VT
ERV
Indirectly measurable lung volumes
RV
TLC
FRC
FEV1
Forced Expiratory Volume in One Second:
The maximal volume of gas, which can be expired from the lungs in the first second of a forced expiration from full inspiration
Uses maximal expiratory effort
Represents more than 80% of exhaled volume in healthy young adult
FVC
Forced Vital Capacity:
The maximal volume of gas, which can be expired from the lungs during a forced expiration from full inspiration
FEV1/FVC %
The proportion of the FVC, which can be expelled during the first second of expiration – expressed as a percentage
can indicate if someone has obstructive lung disease
PEF
Peak Expiratory Flow
Maximum expiratory flow that can be sustained for at least 10msecs (L/min)
Flow volume loops
The y-axis indicates flow rate (L/s). By convention, expiratory flow is positive (above zero) while inspiratory flow is negative (below zero). The x-axis indicates the volume in liters (L).
The loop "begins" when you start to exhale from total lung capacity (TLC). This is where both flow and volume are zero.
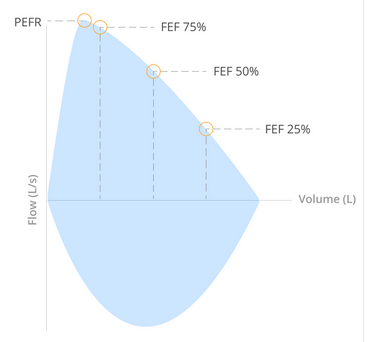
Flow volume loop expiration
Flow reaches a peak value, called the peak expiratory flow rate (PEFR). Following this, flow rate decreases linearly as more air is expired (the curve descends in a relatively straight line).
The flow during the middle half of forced expiration is referred to as forced expiratory flow (FEF). It is common to mark FEF at defined percentages of the forced vital capacity (75%, 50%, and 25%).
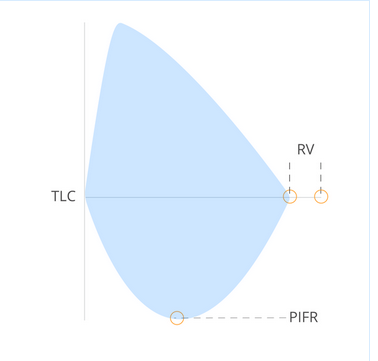
Flow volume loop Inspiration
When the flow reaches zero, you have expired as much air as possible. The only air remaining in the lungs is the RV. The difference in volume between the beginning and end of a maximal expiration is the VC.
If you now make a maximal inspiration you will at some point reach a maximal inspiratory flow rate (PIFR). Flow eventually returns to zero at TLC, effectively closing the loop. But closure of the loop is not necessary, as it is the expiratory information that is diagnostically significant.
Note that time is not shown in flow-volume loops so it is not possible to determine FEV1. This is determined from the original recordings from which the data for the flow-volume loops is derived.
Criteria for acceptable spirograms
1. Free from artefacts e.g.cough, glottis closure, early termination or cut-off, effort not maximal throughout, leak, obstructed mouthpiece
2. Good starts; low extrapolated volume
3. Satisfactory exhalation; duration >6s or a plateau in the volume-time curve
Use of peak flow meters
Reflects mainly the calibre of the bronchi / larger bronchioles
Mainly used in the management of patients with variable airflow limitation (asthma)
Very effort dependent
Records first few milliseconds
Record the best of 3 attempts
Common errors of using peak flow meters
Coughing
Spitting
Poor seal
Insufficient inspiration
Slow expiration
Obstructive lung disease
e.g. COPD, Asthma
Narrowing of airways
Restrictive lung diseases
Pulmonary fibrosis: reduction of lung volume or elasticity
DMD: Weakened respiratory muscles
Kyphoscoliosis: Thorax deformity
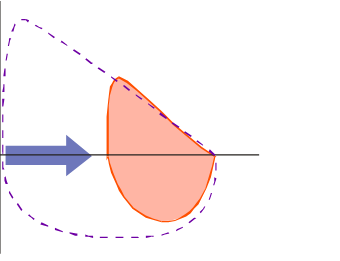
Obstructive flow volume loop
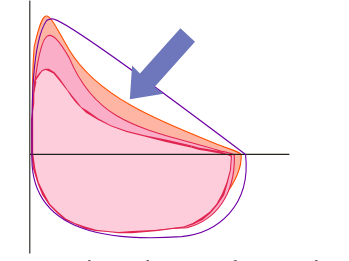
Emphysema flow volume loop
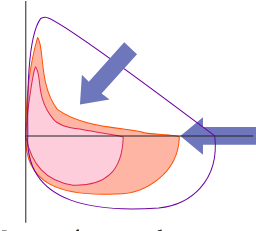
Restrictive flow volume loop
During an asthma attack, it is more difficult to expire than to inspire. Why might explain this phenomenon?
As bronchi are narrowed, they cannot widen as much with the expansion of the lungs leading to longer expiration and increase in resistance of airflow.
COPD flow volume loop features
scooped out appearance of expiratory curve
increased FRC
increased RV
Lower airway obstruction diseases
Asthma
Chronic bronchitis
Emphysema
Cystic fibrosis
Upper airway obstruction disorders
epiglottitis
upper airway tumour
foreign body obstruction