C. difficile Infection
1/27
Earn XP
Description and Tags
Dr. Morelli - 1 LH
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
Define non-severe c-diff
Contrast to severe c-diff
-WBC & SCr values?
NON-SEVERE:
WBC ≤ 15,000 cells/mL
Serum creatinine < 1.5 mg/dL
Severe is the same values, but >, 15k WBC and ≥ 1.5 mg/dL…
When is c-diff considered fulminant?
when there is severe systemic disease
hypotension
shock
ileus (no bowel movement/peristalsis)
toxic megacolon
When is c-diff considered recurrent?
sx recur ~8 weeks after completing treatment
Discuss infection control measures for prevention of transmission of C.difficile infection:
What kind of cleaning agents should be used?
chlorine-containing or sporicidal
When do we test patients for c-diff?
Only test symptomatic patients with with ≥ 3
loose stools in 24 hours
(many asymptomatic patients are colonized)
What is the most sensitive test for c-diff? What is the main drawback?
NAAT (PCR)… can’t differentiate infection vs colonization
What is the GDH antigen test best for?
ruling out if it’s not c-diff… (GDH antigen NEGATIVE means no c-diff… if positive, need toxin test)
What is the most specific test for c-diff?
Toxin A/B EIA
(used after GDH to confirm active disease)
(FYI) sensitivity vs specificity
sensitivity = ability of a test to correctly identify people WITH the disease
specificity = ability of a test to correctly identify people WITHOUT the disease
What are the 3 high risk antibiotics for c-diff?
clindamycin
3rd gen cephalosporins
FQs
What is the first line drug (dose/duration) for an initial episode of non-severe c-diff?
What is the alternative if $$ an issue?
What is an alternative if can’t acquire either?
1st line = Fidaxomicin 200mg PO BID x 10 days
alternatively, vanco 125 mg PO QID x 10 days
-if can’t do either - metronidazole 500mg PO TID x 10 days
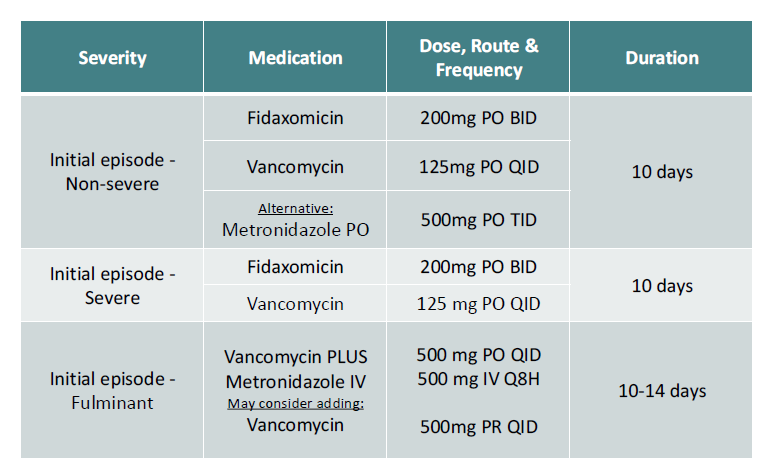
What is the first line drug (dose/duration) for an initial episode of severe c-diff?
same as non-severe MINUS metronidazole as an option!
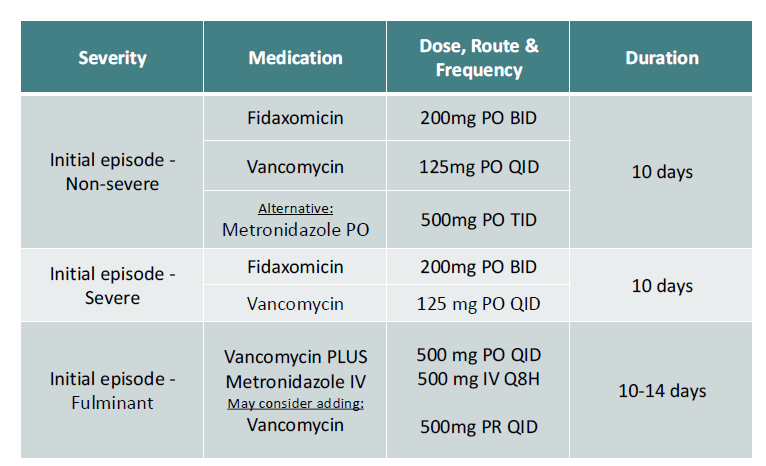
Fulminant C. difficile infection treatment
• First-line antibiotic(s)?
• Dose, route, and frequency?
• Additional therapy if ileus present?
• Duration of therapy?
oral vanco + metronidazole IV
Vanco 500 mg PO QID + Metronidazole 500 mg IV q8h
If ileus present:
• Vancomycin 500 mg PR QID
• treat for 10–14 days
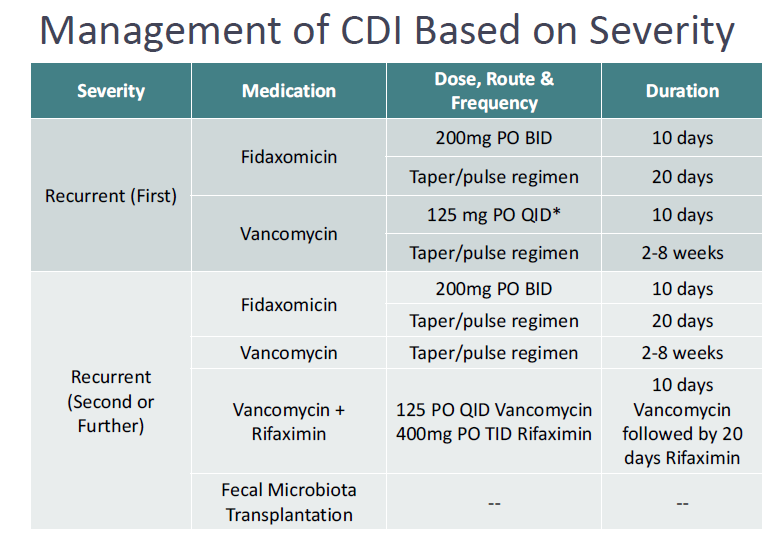
How do we treat the first recurrent episode of recurrent c-diff?
same as first line but followed by a taper/pulse regimen
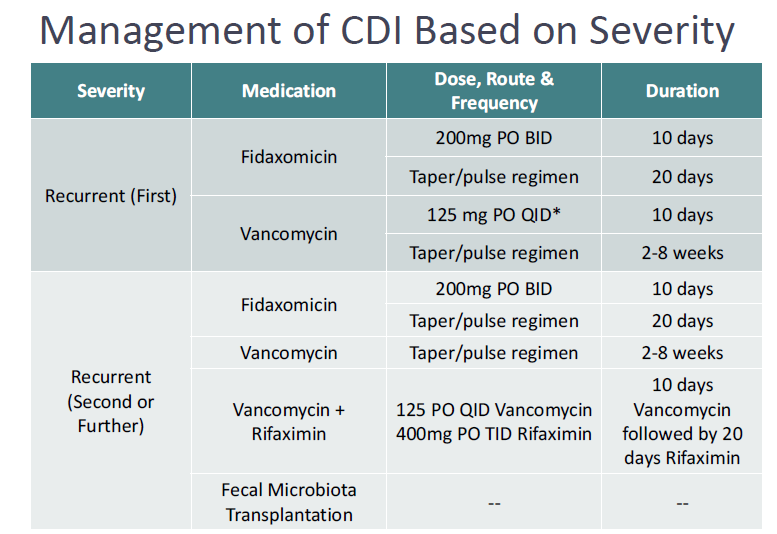
how should we treat a second or later recurrence of c-diff?
first line tapers, switch to not used first line, or a fecal transplant
(FYI) classify Clostridioides difficile
gram-positive, anaerobic, spore-forming toxigenic bacillus
(spores problematic - bacteriocidals do not kill spores)
How is c-diff spread?
oral-fecal
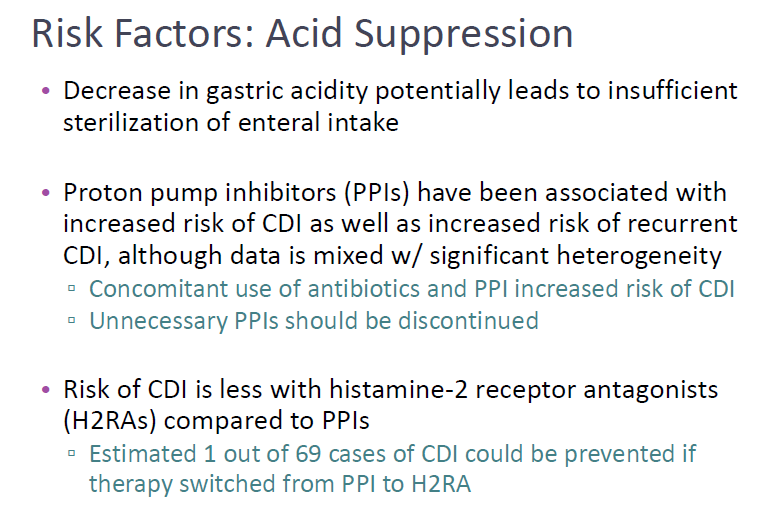
What are the medication-related risk factors for c-diff?
PPIs > H2RAs… acid suppression
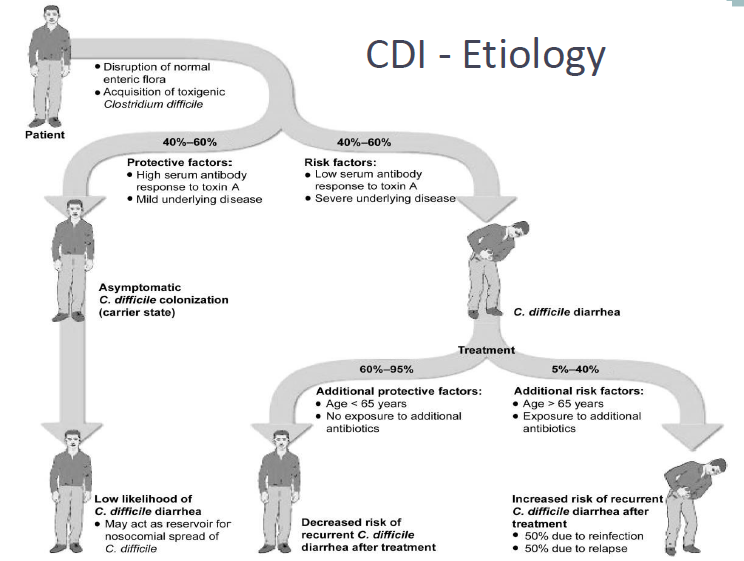
Would symptomatic c-diff be caused by a high or low serum antibody response to toxin A?
low…
MOA of fidaxomycin
RNA pol inhibition
fidaxomicin common AEs
N/V, ab pain, fevers/chills/fatigue
Warnings on fidaxomycin
macrolide and soy allergy
(not to be used in systemic infection due to minimal systemic absorption)
What is the DD interaction of cyclosporine and fidaxomycin?
Cyclosporine increases plasma concentrations of fidaxomicin and may decrease concentrations in the GI tract because of P-gp inhibition (fidaxomicin is a P-gp substrate)
Notable DD interaction of PO vanco
bile acid sequesterants
List the 3 most common ADRs of metronidazole
neuropathy
nausea
taste disturbances
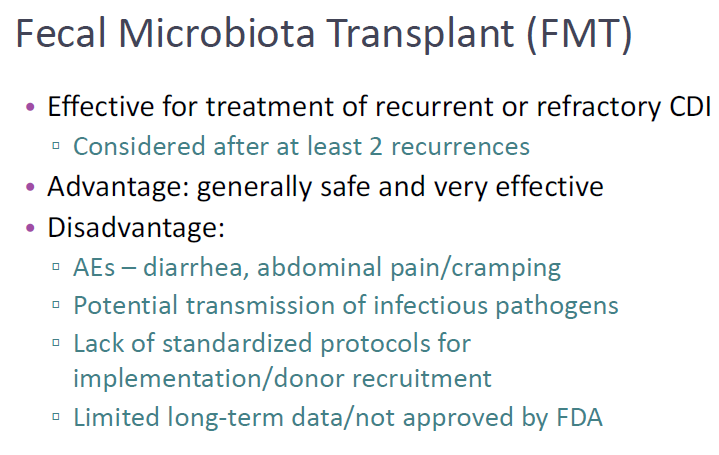
T/F - fecal microbiota transplants are more efficacious than first line antibiotics
true
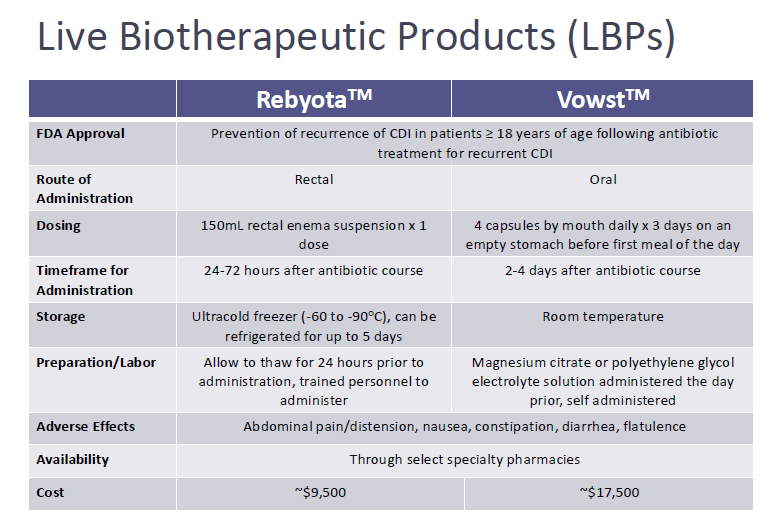
What are the two FDA-approved live biotherapeutic products that are pretty much evolutions of a fecal transplant? Which one is rectal? Which is oral?
Rebyota = R for rectal
Vowst = PO
T/F - Patients need to follow up 2-6 weeks after CDI treatment for a negative stool sample
FALSE