4th cranial nerve
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
what is 4th nerve name?
trochlear nerve
supplies SO
incyclorotation, depression, abduction
inv
- CT: HyperT – SO works at N
o V pattern – bilat
o Possible E in dev
- OM: SO u/a
o o/a of contralat IR and ipsilat I/O
o Knapps classification
o limited elevation/ depression in adduction
o BHTT
- AHP: chin depression
- Conv – reduced – CI
- Torsion: bilat – excyclo
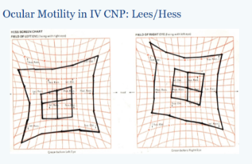
- Hess: field displaced upward to affected side
- Vertical prism fusion range
- Lateral gaze mx
- Diplopia: vertical + uncrossed - subjective torsional
can be both, congenital longstanding decompensating 4th CNP common
- Field of BSV
describe the course of the 4th nerve
nuclei in midbrain, nerves cross over as it leaves the brainstem, right 4th nuclei supplies left SO etc., wraps around back and side of brainstem and moves forward into subarachnoid space, enters cavernous sinus, supplies SO
where is the 4th nerve nuclei located?
in the dorsal midbrain, specifically at the level of the inferior colliculus
describe the location of the 4th in the cavernous sinus
located in the lateral wall, inferior to the 3rd nerve
superior to 5th nerve
list aetiologies of an acquired 4th NP in the subarachnoid space?
high ICP
ischaemia
intrinsic lesions e.g schwanomma
aneurysm
trauma
venous malformations
carotid-cavernous fistula
basal meningitis
list the aetiologies of an acquired 4th NP in the orbital
- Ischemic – hypertension, diabetes
- Compressive – tumour, aneurysm, stroke
- Traumatic – head or orbit
- Congenital
what would you observe in a pt with 4th CNP
facial asymmetry - cheekbones flatter on oneside in congential
headposture
FAT family album tomography scan - looking at old pics for congenital cases
what is the CHP?
eye is excyclo - headtilt AWAY from affected side
eye is HYPER - chin depression gets away from depression
face turn away from affected side
what muscle would you differentially diagnose from a SO?
SR vs SO
BHTT = differentiating 4th CNP from other vertical deviations
min 4 dioptre difference
what is the maximum position of action of the SO?
depression in adduction
describe 4 steps of muscle sequelae
1) primary u/a muscle
2) o/a of contralateral synergist
3) u/a or contracture of ipsilateral antagonist
4) o/a or secondary inhibition of contralateral antagonist
what would you expect to see on measurements at N and D for a 4th NP?
bigger at N>D
what is step 1 in the BHTT?
which is the higher eye?
reduces possible muscles to 4 muscles
pathway
origin
Ventral part of the periaqueductal grey of the midbrain.
level of inferior colliculus
Fibres emerge and pass dorsally around periaqueductal grey
Fibers cross in the midline
Fibres exit dorsal midbrain
In sucharachnoid space
Nerve passes around cerebral peduncle
Passes between posterior cerebral and superior cerebellar arteries
Pierces the dura at tentorium cerebelli.
Enters cavernous sinus - lies in lateral wall
Enters the orbit via Superior Ortbital Fissure
supplies SO
location of lesion + cong/ acquired
lesion in nucleus or fasicular lesion of midbrain
susceptible to damage as exit midbrain & vulnerable to CS & orbital apex
congenital or acquired
Congenital
tendon is lax and long
acquired
trauma - bilateral as 4th arise from dorsal aspect of midbrain - long route- susceptible to injury
vascular - hypertension
diabetes
SOL
inv
CH
congenital
bilateral
manifest strabismus without binocular function
binocular function - but AHP
symptoms of decompensation when pt was BV w AHP - but difficult to control dev - dip, headaches and asthenopia
older pts
facial asymmetry
acquired
unilat
bilat - closed head trauma
symptoms - cyclovertical dip - worse in down gaze
AHP - long standing dev
AHP
unilat - chin depression FT and head tilt away from affected side
bilat - chin depression - no FT or head tilt unless 1 side affected more than other
CT
c & s AHP
c - latent
s - manifest
affected eye - HyperT - N>D
eso dev
OM
u/a in pp SO
o/a contralateral IR
o/a ipsilateral IO
u/a SR secondary
bilateral
V pattern
knapps
poor elevation & depresssion in adduction of ipsilateral eye = injury to SO = muscle restriction & paresis
INV continue
convergence
reduced due to CI or vertical dev
correct dev see if conv improves
BV
C & S AHP
no BSV in bilateral
congenital - sm bsv
Hess chart
FOF
area of bsv is displaced upward to affected side
Diplopia
N test looking down
dip is vertical and uncrossed
if exo - H element of dip crossed
BHHT
CT in pp - head straight - HYper in affected eye
if positive - ↑ in affected side
unaffected side ↓
Torsion
excyclotorisoin in bilateral
Prism
temporary correct angle and AHP
Difference in SO and SR
SO
CT
Hyper dev if fixing w unaffected eye
dev N>
AHP
chin depression
OM
↑ angle on depression
Hess chart
↑ -ve displacement on depression
extorsion
common
BHTT
+VE
SR
CT
Hypo if fixing w unaffected eye
dev ↑ D>
AHP
chin elevation
OM
↑ angle in elevation
Hess
↑-ve in elevation
extorsion
rare
BHTT
-ve
differences in bilat/unilat SO palsy
unilateral
CT - hyperT dev in pp - reflect extent of palsy
OM - no reversal of hyperT and dip on lateral versions
slight V
AHP - chin depP = head tilt + turn
torsion - slight extorsion
BHTT - +ve to affected side
bilateral
CT - sl hyper dev in pp
OM
reversal of hyperT and dip on lateral versions
large V
AHP - chin depression
Extorsion - > 10^ - Mrkd Torsion
BHTT - +ve w head tilt to either shoulder
mx- congenital
Correct refractive error.
Treat amblyopia if present.
Surgical Indications:
Strabismus.
Marked abnormal head posture.
Decompensating cases with moderate/large-angle deviations.
Surgical Options:
SO tuck (for abnormal superior oblique tendons).
Weaken overacting muscles:
Inferior oblique.
Inferior rectus.
adjustable sutures
mx - acquired
Treat underlying cause (e.g. hypertension).
Spontaneous recovery common within 3–6 months.
Non-surgical Options:
Prisms - <10 - after 6m stab;e
Occlusion:
Temporary relief from diplopia during observation period.
Botulinum toxin:
inferior oblique to reduce hypertropia.
So myokomia
Definition & Features:
Rare, benign, self-limiting disorder.
Typically unilateral.
May follow acquired superior oblique palsy.
Visible under slit lamp or ophthalmoscope.
Symptoms include:
Intermittent oscillopsia.
Torsional monocular diplopia.
Causes:
Often idiopathic.
Nerve compression by blood vessels in posterior fossa.
Rare associations: multiple sclerosis, space-occupying lesions, dural AV fistula.
Neuroimaging recommended to rule out serious pathology.
Management:
Carbamazepine (Tegretol) often effective:
Alternatives: propranolol, gabapentin.
Surgery (rarely curative, for severe cases):
Superior oblique intrasheath tenotomy / nasal tenectomy.
May combine with inferior oblique recession/myectomy.
Other options: Harada–Ito, trochlea resection after failed initial surgery.
Why does 4th cnp head tilt away from affected side
E.g RSO affected
Head tilt to left as SO incyclo and depresses
So not working its going to excyclo and hypert elevate
So moving to left its going to work on unaffected muscle e.g. L SR which 3rd action is to inclyclo to compensate for the excyclo of RSO
DD
DD
TED
ocular surgery
skew deviation
incyclo in skew - suprine test resolves
excyclo in 4th
3rd CNP
MG
decompensated hyperphoria
orbital fracture
childhood strabismus
sx
Surgical Options (after ≥6 months of stability):
If inferior oblique overacts → Recession.
If superior rectus restricted → Recession.
If superior oblique lax → Tuck.
>15 prism dioptres deviation → Consider multiple muscle surgery:
Ipsilateral inferior oblique + superior rectus recession.
Ipsilateral superior oblique tuck.
Contralateral inferior rectus recession.
Combined vertical + horizontal deviations:
Surgery on both planes if horizontal >8 prism dioptres.
Use of adjustable sutures may improve outcomes.
Sx
- Unilateral
o SO tuck
o IO weakening
- Bilat
o Bilateral SO tuck
o Harada ito =torsion
longstanding or acquired
Longstanding or acquired
congential
no diplopia
large vertical fusional amplitude = adapted for a long time
Facial assymetry
minimal/ none cyclotorsion
childhood photos - long standing CHP
acquired
diplopia - actute sudden
small vertical fusional amplitude
face is symmetrical
bigger cyclotorsion
childhood - straight
o VFR
o Mx torsion – congenital 4ths no torsion due to retinal reorientation
o AHP – LS
clinical presen
- Diplopia: vertical + subjective torsion
o Worse in downgaze
- CHP
o Eye: excyclo + HyperT
o Head tilt: away from affected side
o Chin: depressed
o FT: away from affected side
Further tests
o Blood test
o Blood pressure
o MRI