Chapter 14 - Learning and Memory
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
64 Terms
What is Learning?
A relatively permanent change in behavior as a result of experience.
What is Memory?
The ability to recall or recognize previous experiences.
At what level are Learning and Memory defined?
At the Behavioral level.
It is assumed that these functional behavioral changes are related to structural changes in the nervous system.
What do Mental representations result from? At what level does this happen?
or Memory traces (engrams) result from physical changes in the brain, both at the level of synapses (synaptogenesis) and nucleus of neurons (neurogenesis).
NB: The brain transforms the world; the world transforms the brain.
What are the 2 Classic types of learning?
Pavlovian / Classical conditioning
Operant conditioning
What happens in Classical conditioning?
A Neutral stimulus (e.g. a tone) is paired with an unconditioned stimulus (air puff) that elicits an unconditioned response (eye blink).
Once paired, the neutral stimulus becomes a conditioned stimulus that elicits the same response as the unconditioned stimulus (= conditioned response).
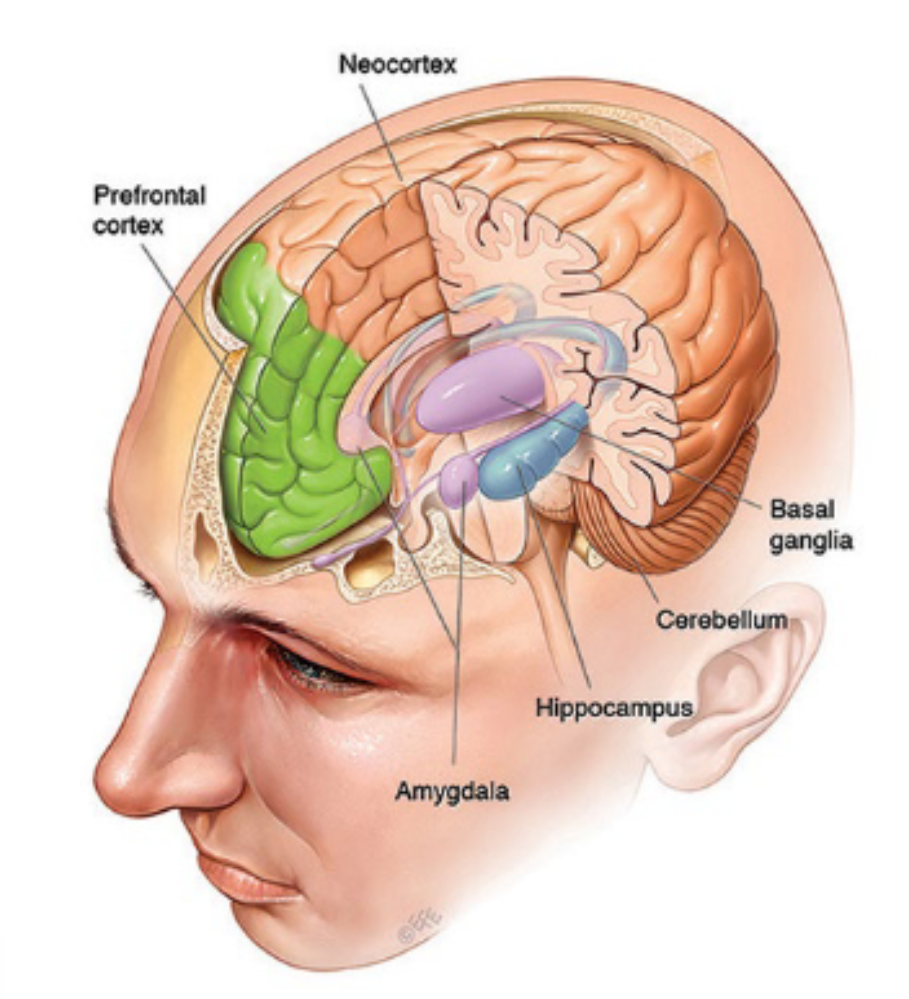
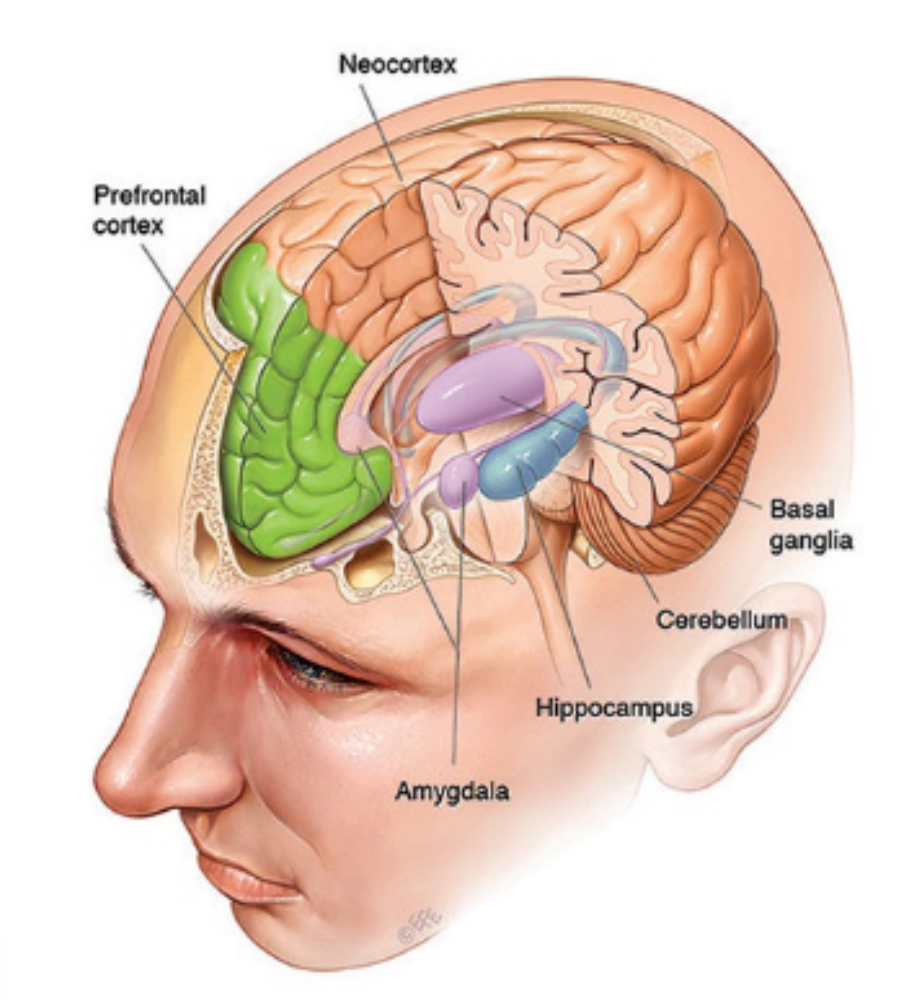
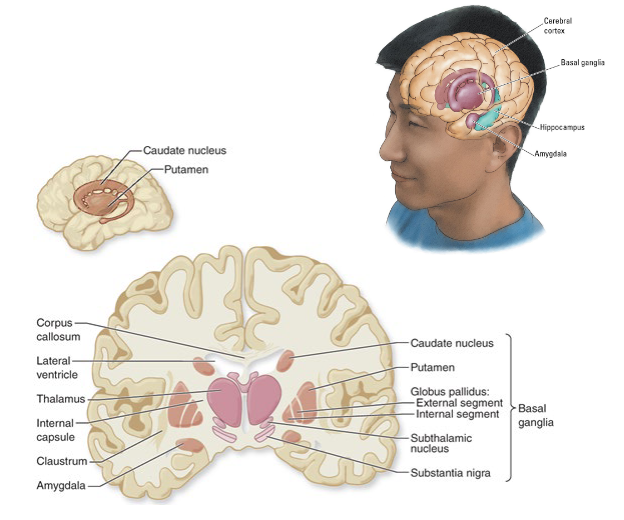
What parts of the brain are involved in Fear conditioning? What parts for Motor conditioning?
Fear conditioning → Amygdala.
Motor conditioning → Basal ganglia, cerebellum
What happens in Operant conditioning?
Learning through reinforcement.
Consequences of a specific behavior increase or decrease the probability of the behavior occurring again.
e.g. perform task (e.g. peck buttons in specific sequence) to acquire reward (food).
What type of learning are the two types of conditioning (Classical and Operant)?
Both types of conditioning are a form of implicit learning (unconscious).
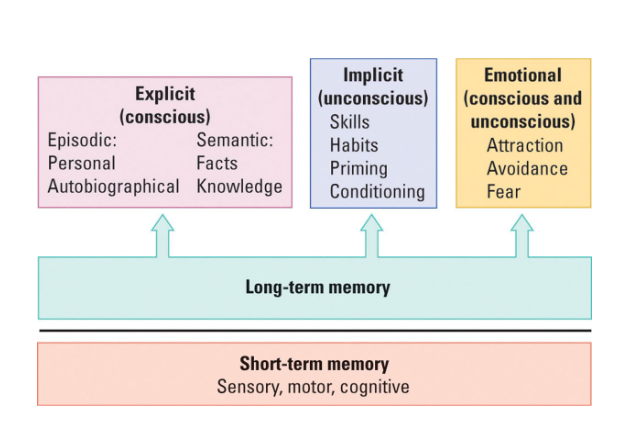
What are the 2 types of Memory that we have?
Explicit memory (conscious)
Implicit memory (unconscious).
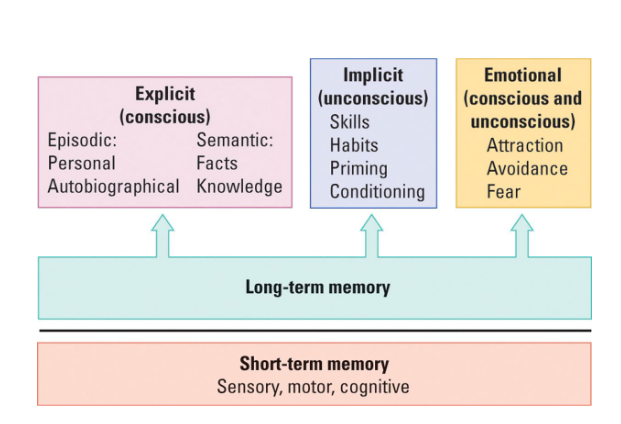
What are the characteristics of Explicit memory?
Conscious
Semantic (facts), episodic (personal)
Top-down (higher-order, conceptually driven cognitive processing)
Knowing that/what
e.g. search for specific object while ignoring others.
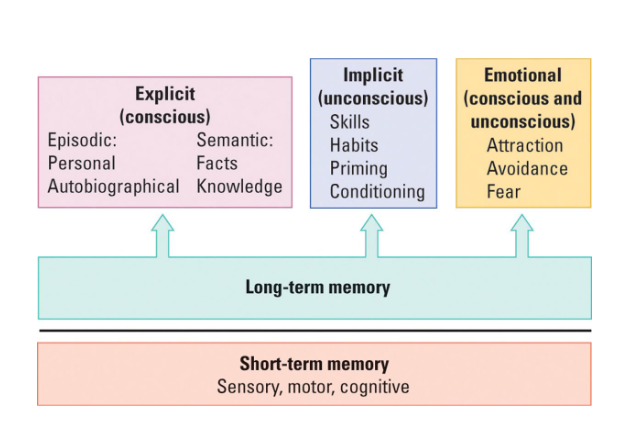
What are the characteristics of Implicit memory?
Unconscious
Skills, habits
Bottom-up (driven by data/sensory input)
Knowing how
e.g. recognizing a specific object.
What happens in Amnesia?
Partial or total loss of Explicit memory.
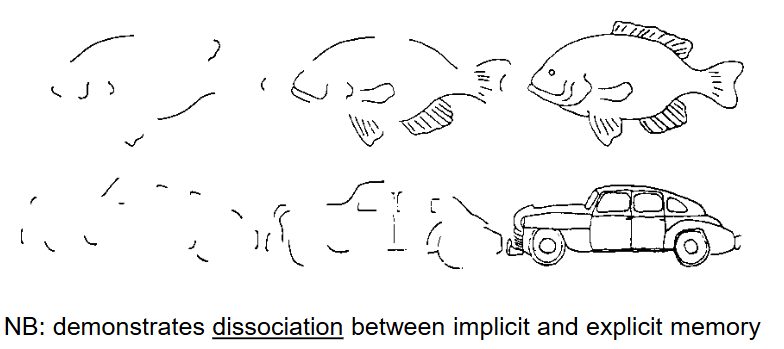
What happens in Impaired explicit memory?
e.g. No conscious recollection what happened during the training.
What happens during Intact implicit memory?
e.g. Being able to learn how to recognize incomplete pictures.
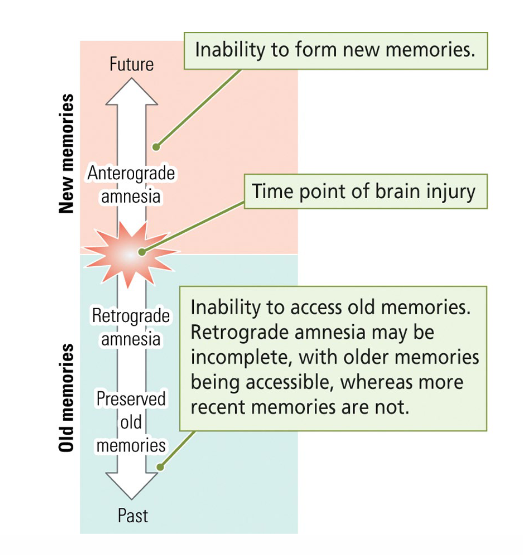
What are the 2 types of Memory loss? What happens?
Anterograde amnesia: No storage of new memories.
Retrograde amnesia: Loss of existing memories (may be incomplete).
What are the Symptoms of Korsakoff Syndrome?
Retrograde + Anterograde amnesia, and impaired short-term memory (progressive).
What is the Cause of Korsakoff Syndrome?
Thiamine (vitamin B1) deficiency, usually due to malnutrition and prolonged intake of large quantities of alcohol.
What is the Neural mechanism of Korsakoff Syndrome?
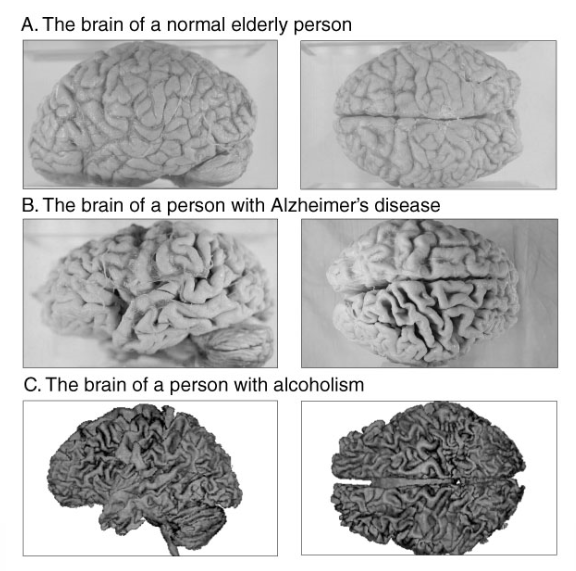
Cell death in midline diencephalon, including medial thalamus and mammillary bodies in the hypothalamus, also cortical atrophy (loss of brain tissue).
What is Cortical atrophy?
Loss of brain tissue.
What happens to individuals with Korsakoff syndrome?
They have little insight into their dysfunctions (frontal lobe impairments due to atrophy) → Make up plausible stories about past events based on actual experiences.
What are the 3 stages of Memory consolidation? What happens in these stages?
Encoding
Fragile, must compete with existing and new memories and thus at risk of being abolished (mostly during the day).
Storage
Relatively permanent representation, requires structural changes → Learning (best done during quietness/sleep).
Recall
Retrieval of memories, integration with existing memories, open to further consolidation → Reconsolidation (mostly during the day, maybe during sleep as well).
NB: Using the same space for studying probably reduces the likelihood of memory changes due to reconsolidation.
What time is the best of Memory storage?
Sleep.
What is Karl Lashley known for?
He searched for the location of the physical memory trace in the brain for 30 years.
He made thousands of different lesions in the rat brain and determined whether memory was affected (physiological psychology).
He did not find where the memory trace is located.
He did find a relationship between the size of the lesion and the severity of the memory problems.
What was the conclusion of Karl Lashley’s findings for Localizing the memory trace?
Memory cannot be distinguished to a single cortical area, but is instead distributed throughout the cortex.
What are the 2 Neural basis of Memory types?
Short-term memory
Long-term memory
Explicit memory
Implicit memory
What is the Neural basis for Short-term memory? What are the areas of the brain involved in this type of memory?
Reverberation → ‘Resonating’ action potentials.
Main area: Frontal lobe (prefrontal cortex).
What is the Neural basis for Long-term memory? What areas of the brain are involved in this type of memory?
Consolidation → Structural changes.
Explicit memory
Main area: Medial temporal lobe (including hippocampus and amygdala).
Semantic: default mode network (ch8)
Episodic: hippocampus, ventromedial prefrontal cortex (vmPFC).
Implicit memory
Main area: Basal ganglia (motor learning), also cerebellum.
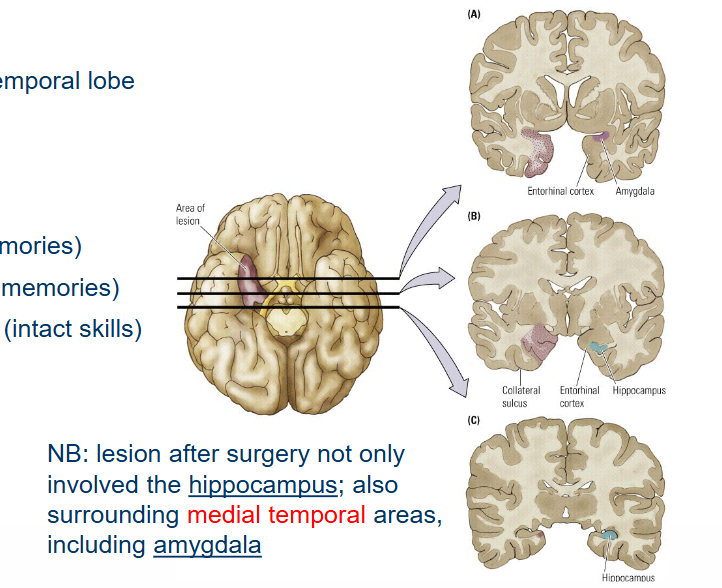
Patient H.M. suffered from Severe epilepsy. Where did this epilepsy originate from? What surgery was performed?
Severe epilepsy originating from medial temporal lobe.
Surgery: bilateral hippocampectomy.
NB: Lesion after surgery not only involved the hippocampus; also surrounding the medial temporal areas, including amygdala.
What happened to Patient H.M. after surgery?
His surgery: bilateral hippocampectomy.
Severe anterograde amnesia (no new memories)
Little or no retrograde amnesia (intact old memories)
Little or no problems with implicit memory (intact skills).
What was the conclusion that was found after Patient H.M’s performed surgery?
Hippocampus contains a mechanism to “store” new explicit memories.
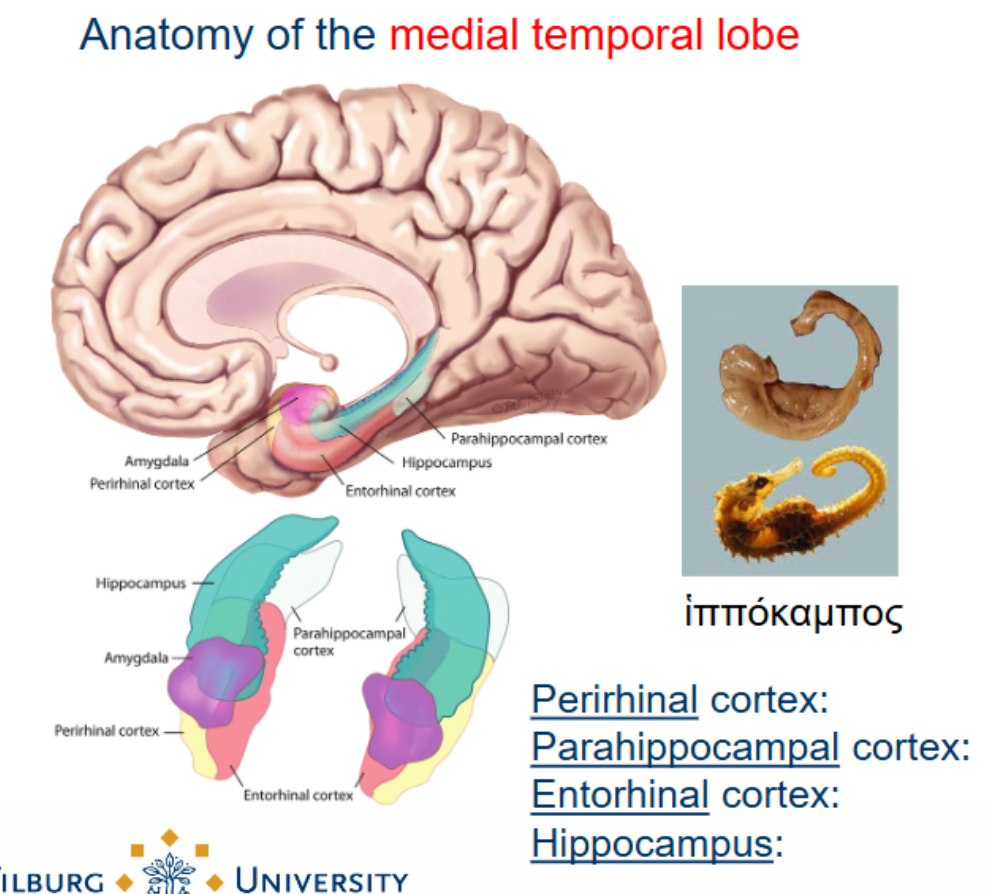
What is the Anatomy of the medial temporal lobe?
Perirhinal cortex: visual object memory (input visual ventral stream).
Parahippocampal cortex: visuospatial memory (input from parietal regions).
Entorhinal cortex: integration of visual memory (affected first in Alzheimer).
Hippocampus: mainly spatial memory (places, recalling object location).
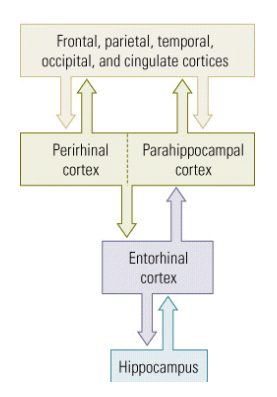
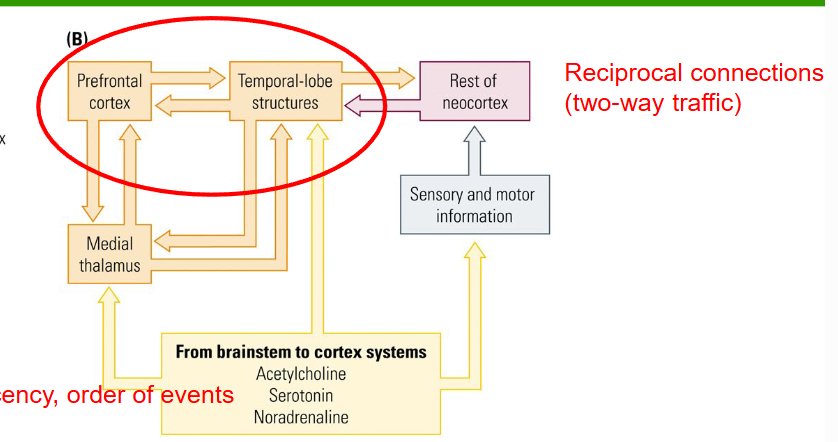
Medial temporal lobe connections are reciprocal; what does this mean?
There is a two-way traffic.
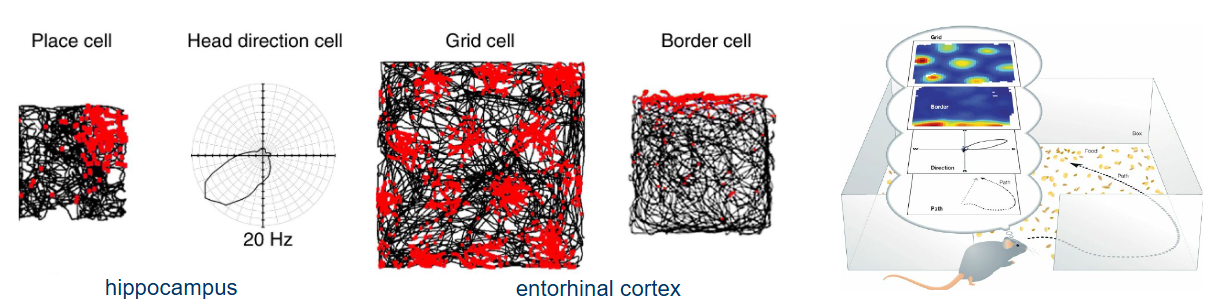
What cells does the Neural Global Positioning System consist of and what does each cell do?
Place cells in hippocampus fire only if an animal is in a certain place, regardless of its orientation.
Head direction cells in hippocampus fire (discharge) when head points in specific direction (vestibular system).
Grid cells in entorhinal cortex form a virtual grid to estimate size of environment.
Border cells in entorhinal cortex fire exclusively at edges and boundaries of the local environment.
What is the role of the Prefrontal cortex regarding Memory?
Short-term memory, recency, order of events.
‘Reverberation’ (of action potentials).
Frontal lobe receives input from all sensory systems.
Many multimodal cells that process complex information.
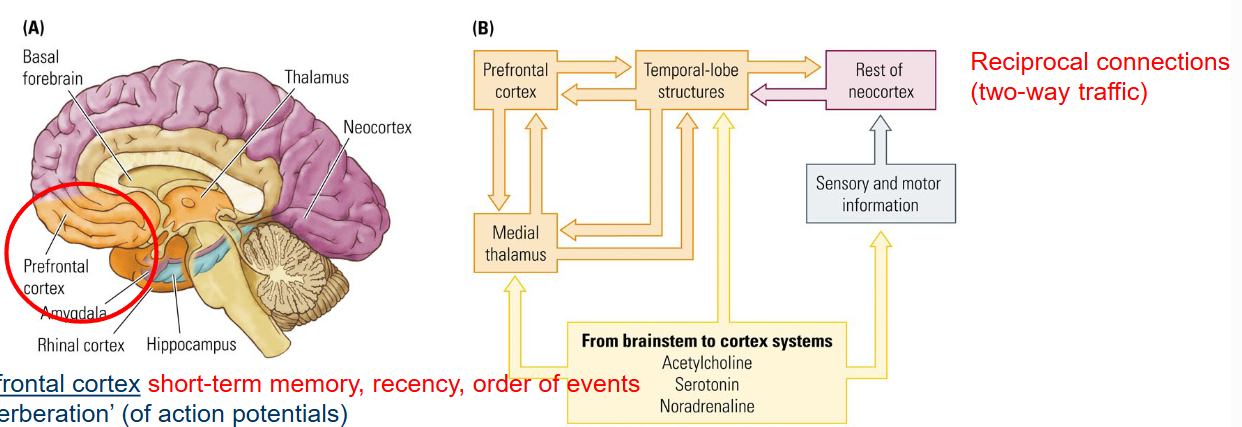
What are the 3 Neurotransmitters that are involved in the pathway from the Brainstem to Cortex systems?
Acetylcholine
Serotonin
Noradrenaline
Via which route does the Short-term memory turn into Long-term memory?
Prefrontal cortex to medial temporal lobe.
What are the 3 Neural connections for Explicit memory?
Prefrontal cortex
Prefrontal cortex to medial temporal lobe
Medial temporal lobe projects back to the neocortex
What happens when the Medial temporal lobe projects back to the neocortex?
Keeps sensory experiences ‘alive’ in the brain (i.e. neural record of experience outlasts the actual experience).
We remain conscious of what is processed and stored (enable conscious recall of explicit memories).
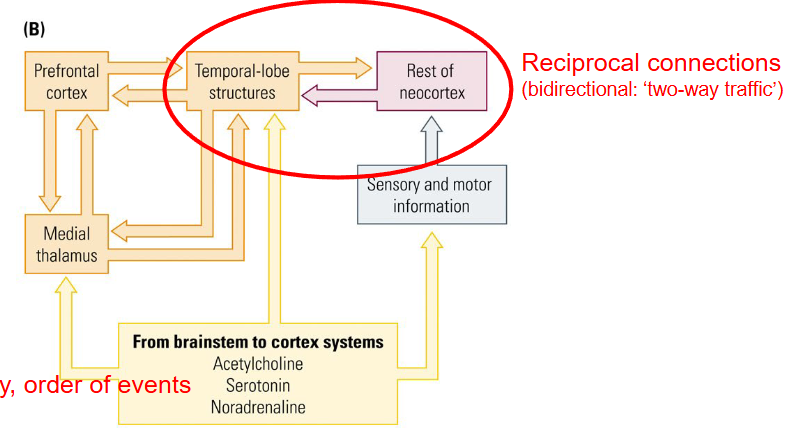
Which neural connection allows us to remain Conscious of what is processed and stored?
Medial temporal lobe projects back to the neocortex.
What are the Symptoms of Total loss of Explicit memory?
Anterograde amnesia
Retrograde amnesia
Severely impaired short-term memory (~30 seconds)
Clive Wearing suffered from Total loss of explicit memory and could only retain information for 30 seconds before he forgot it again.
What is the Cause of Total loss of Explicit memory?
Damage to the hippocampus, temporal lobe and frontal lobe due to herpes simplex encephalitis (viral infection of the brain).
NB: Clive Wearing was still able to play the piano, learn new practices → So implicit memory still largely intact.
Dissociation between implicit and explicit memory.
Patient J.K. had
Above average intelligence (engineer)
Diagnosed with Parkinson’s disease
Basal ganglia dysfunction
What were his symptoms?
Intact explicit memory (daily events, long-term).
Impaired implicit memory (skills, habits); e.g. does not remember how to turn on the lights, switches off the radio using TV remote control.
What is the conclusion regarding Patient J.K.?
The Basal ganglia is the main structure for implicit memory.
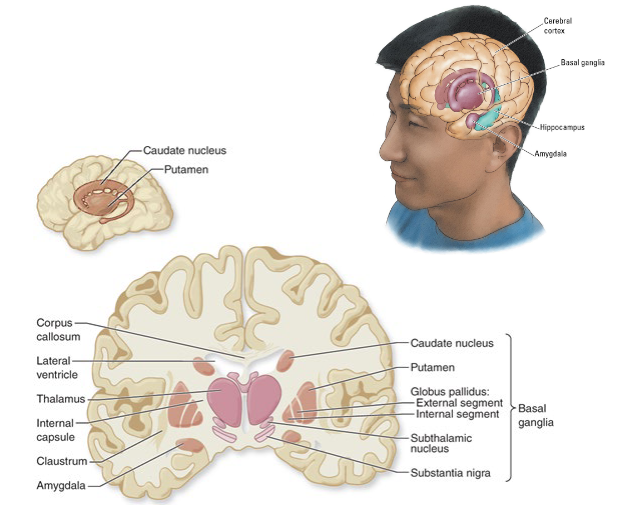
The Neural connections for Implicit memory are unidirectional; what does this mean?
One-way traffic.
NB: no feedback to neocortex → implicit memory is unconscious.
Substantia nigra provide ‘fuel’ for basal ganglia (dopaminergic).
What explains that Implicit memory is unconscious?
No feedback to neocortex (neural connections for implicit memory are unidirectional (one-way traffic)).
What is Basal ganglia traditionally viewed as?
As ‘volume’ control of motor areas (see ch11) → Implicit memory is linked to action.
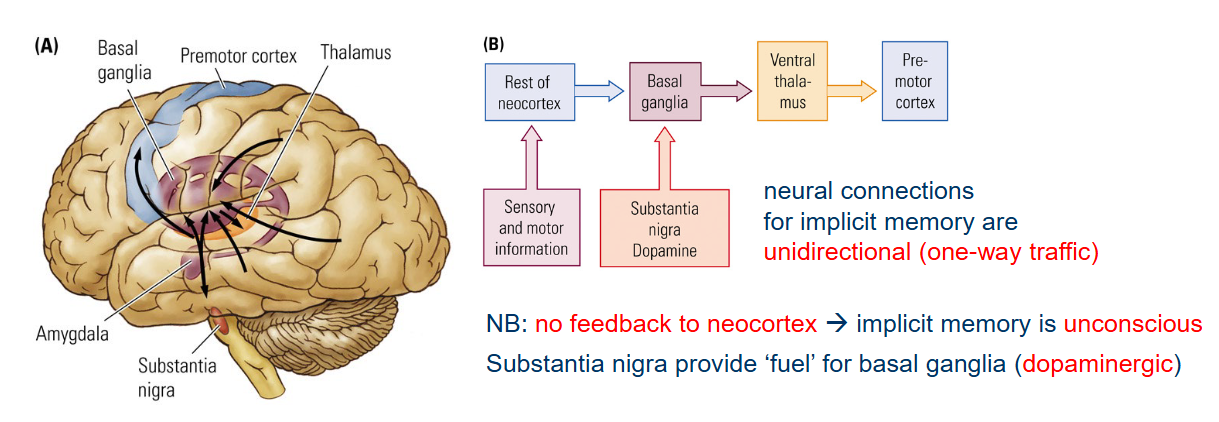
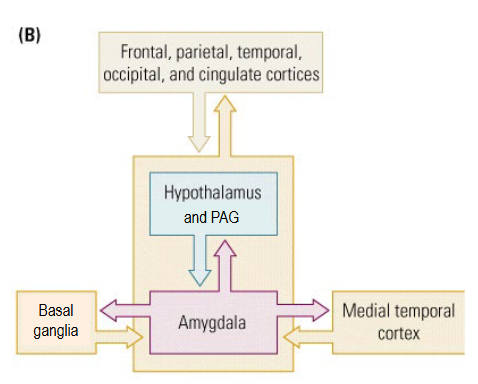
What is the Neural connection for Emotional memory?
Amygdala is essential for emotional memory → Evaluates sensory information for emotional and motivational meaning (see ch12).
Emotional memory could be both explicit and implicit.
e.g. specific anxiety (explicit)
e.g. generalized anxiety (implicit)
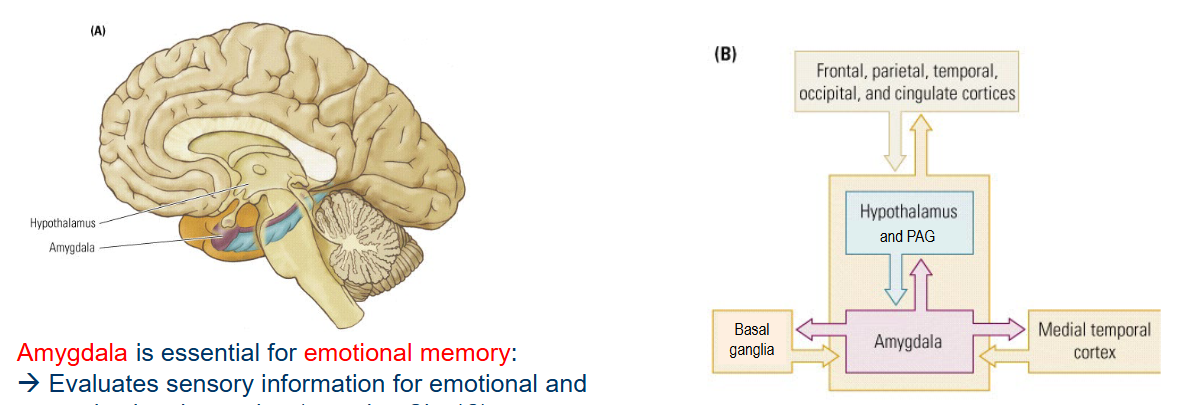
What happens when there is a lesion in Amygdala?
No emotional memory, but intact explicit and implicit memory.
NB: exact neural mechanisms involved in emotional memory are still largely unclear.
What happens in Long-term potentiation (LTP)?
Strong bursts of high-frequency stimulation (e.g. 100 Hz) changes synaptic transmission in such a way, that subsequent weak stimulation produces a larger EPSP lasting for ~90 mins.
Enhances transmission in an existing synapse (increases neurotransmitter release).
Enhances communication between neurons (increases postsynaptic sensitivity).
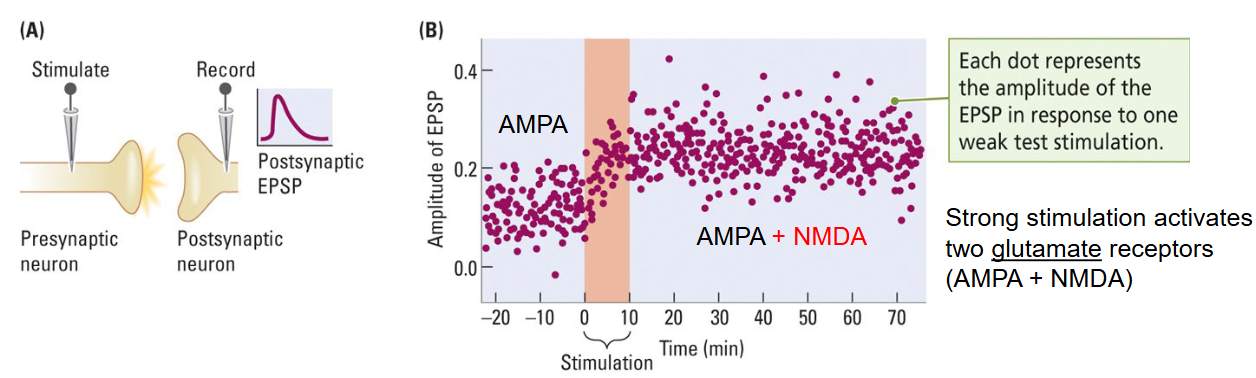
What receptors does strong stimulation of LTP activate?
Two glutamate receptors (AMPA + NMDA).
What is the working mechanism for Long-term potentiation (LTP)?
AMPA receptors respond to weak stimulation and produce the initial EPSP → Na+ influx.
NMDA receptors are ordinarily blocked by magnesium ions.
Strong bursts of high-frequency stimulation (e.g. 100 Hz) may remove the magnesium ions from the NMDA receptors.
NMDA receptors now also respond to weak stimulation → Influx of Ca2+.
→ Second messenger → Increased function and/or increased number of AMPA receptors → larger EPSP.
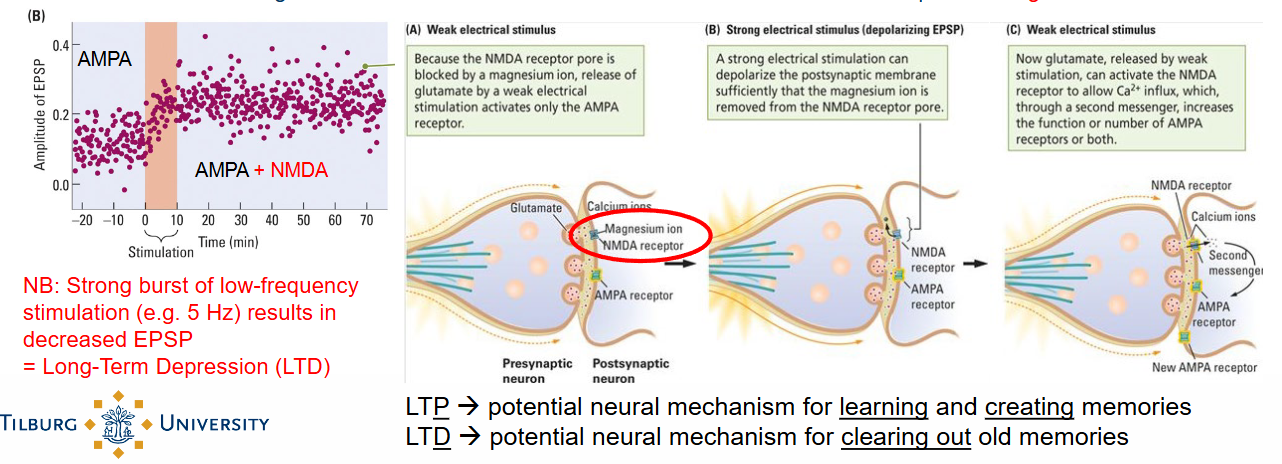
What is Long-Term Depression (LTD)?
NB: Bursts of low-frequency stimulation (e.g. 5 Hz) results in decreased EPSP = Long-term depression (LTD).
What is the difference between LTP and LTD?
LTP → potential neural mechanism for learning and creating memories.
LTD → potential neural mechanism for clearing out old memories.
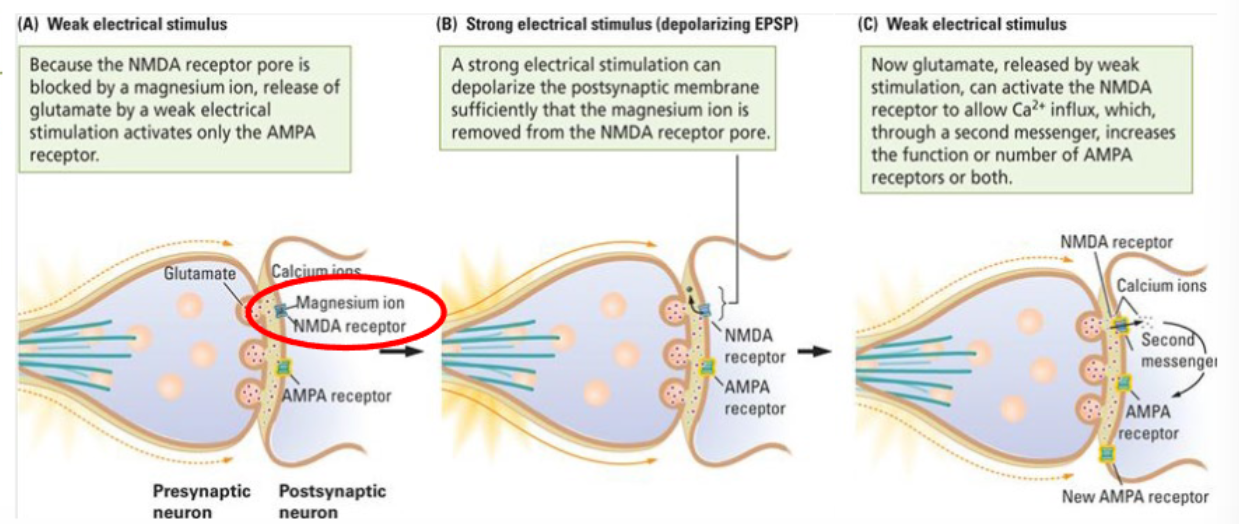
What are the 3 steps of Long-Term Potentiation (LTP)?
Weak electrical stimulus:
Because the NMDA receptor pore is blocked by a magnesium ion, release of glutamate by a weak electrical stimulus activates only the AMPA receptor.
Strong electrical stimulus (depolarizing EPSP):
A strong electrical stimulation can depolarize the postsynaptic membrane sufficiently that the magnesium ion is removed from the NMDA receptor pore.
Weak electrical stimulus:
Now glutamate, released by weak stimulation, can activate the NMDA receptor to allow Ca2+ influx, which, through a second messenger, increases the function or number of AMPA receptors or both.
What are 6 different cases in which we can see Brain plasticity?
Experience
Environmental influences
Motor learning
Cortical reorganization
Chemically induced changes
Recovery after brain damage
What happens in Brain plasticity regarding Experience?
Modification of existing circuits (synaptogenesis).
Creation of new circuits (neurogenesis).
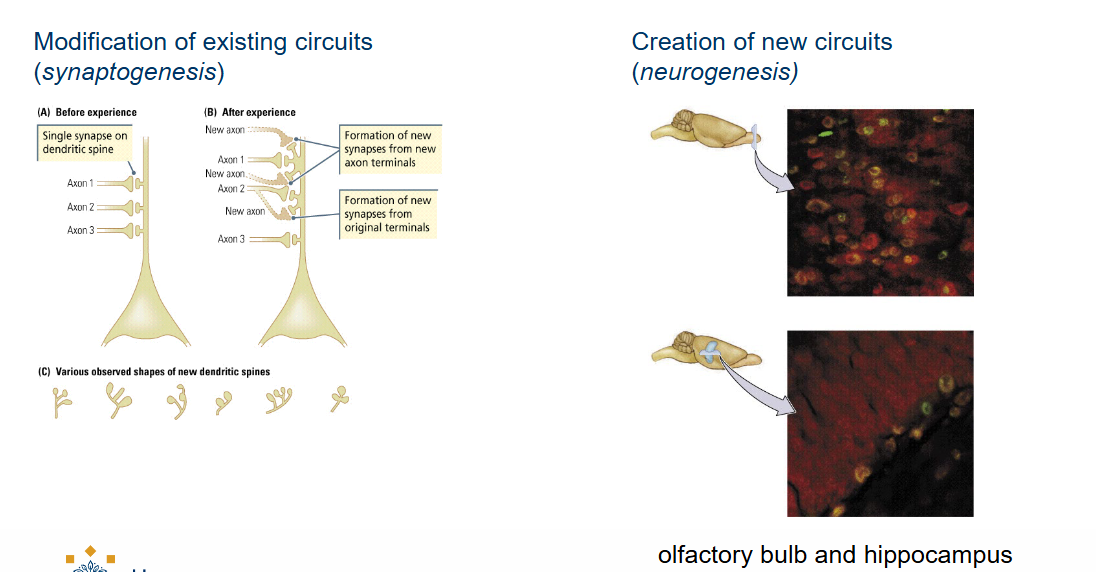
What is involved in the Neurogenesis?
= Creation of new circuits.
Olfactory bulb
Hippocampus
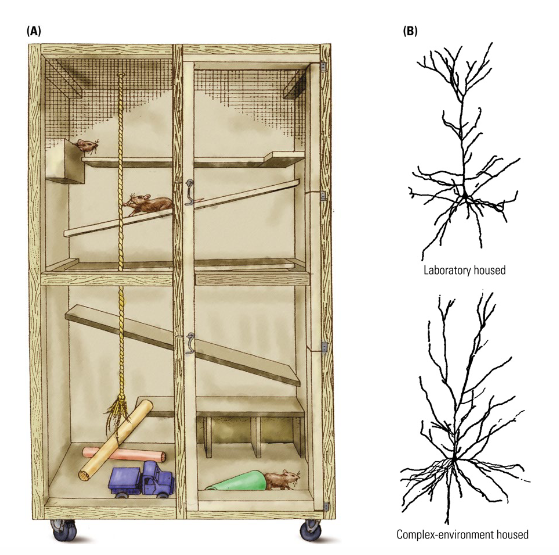
What are the effects of Environmental influences on Brain plasticity?
Growing up in an enriched environment leads to structural changes:
Increased brain weight (~10%)
Larger dendritic tree
More dendritic spines
More synapses
More blood vessels
NB: Increased connectivity may result from increased sensory, motor and social experience induced by enriched environment (see ch8).
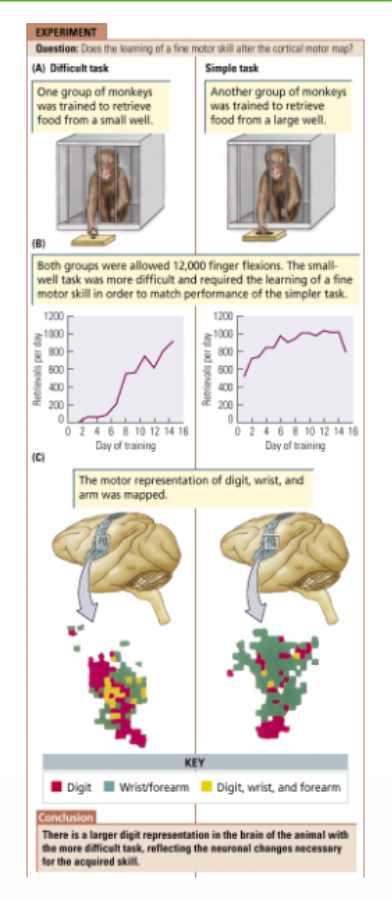
What are the Experimental evidence for Motor learning?
Training of fine motor skills changes the somatotopic arrangement in the motor cortex:
Larger representation of fingers in monkeys trained in difficult motor task compared to simple motor task.
What are the observations in humans we have made regarding Motor learning?
e.g. Larger motor area for finger of the left hand in professional violin players compared to controls (can be tested using TMS, MEG, MRI).
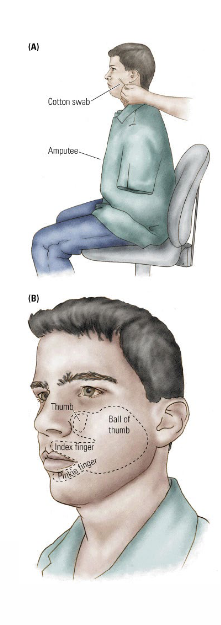
What happens in Cortical reorganization?
Peripheral stimulation of the face produces the sensation of touch at the amputated arm (i.e. phantom pain).
Occurs because the ‘unused’ (“deafferented”) areas in the somatosensory cortex (e.g. for the lost arm) start to respond to input from adjacent areas (e.g. the face).
At the cortical level, the ‘arm area’ is now mapped to the face.
This is called cortical reorganization.
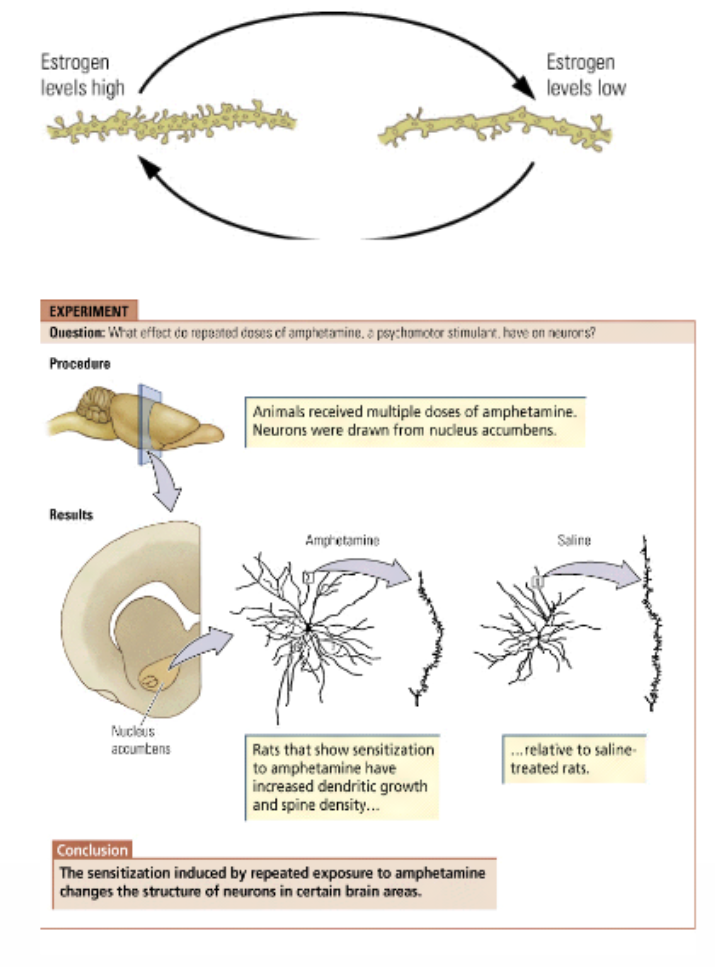
What are the 3 examples of Chemically induced changes? What happens?
Hormones (ch8)
Can influence synaptic organization.
Glucocorticoids (stress) may lead to hippocampal cell death.
Estrogen fluctuations (menstrual cycle) may alter dendritic spines (and synapse) numbers.
Neurotrophic factors (ch8)
Stimulate the development of stem cells to neuraon or glial cells.
Induce synaptic reorganization as well.
Psychoactive drugs (ch6)
Sensitization induced by repeated drug intake may enhance behavioral effects due to increased dendritic growth → Drug-induced behavioral sensitization in amphetamine.
What are the 3 ways in which Recovery after brain damage can be demonstrated?
“The three-legged cat”
Behavioral adaptation, e.g. writing with the left hand.
Learn new ways to solve the problem → Compensatoin strategies.
Reorganization of existing neural circuits
Interventions: behavioral therapy, neurotrophic drugs, electrical brain stimulation, deep brain stimulation (DBS).
Learn to do more with less neurons (e.g. constrained-induced therapy).
Replacedment of damaged neurons
Transplantation of fetal stem cells from aborted embryo’s → only moderate effects, lots of ethical issues.
More recently: transplantation of own stem cells or stimulation of existing stem cells in subventricular zone.
Still in experimental stage (e.g. animal-models of Parkinson’s disease).