audexam 2
0.0(0)
Card Sorting
1/101
Earn XP
Description and Tags
Last updated 1:12 PM on 11/15/22
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
102 Terms
1
New cards
auricular
diff shapes/size/location of ear
2
New cards
anotia
absence of pinna
3
New cards
microtia
small/malformed pinna
4
New cards
low-set ears
ears not positioned on head as expected
5
New cards
preauricuar tags and sinuses
born with them on particular spots
6
New cards
auricular hematoma
internal bleeding of pinna; resulting from a blunt injury (or bacteria or virus (herpes) or neoplasms (cysts/tumors); can result in damage to cartilage (full- cauliflower ear or part of ear)
7
New cards
atresia
absence of external auditory canal
8
New cards
stenosis
narrowing of external auditory canal
9
New cards
acquired disorders of ear canal
impacted cerumen (overaccumulation); foreign object; otitis externa; exostosis (surfer's ear-benign bony groths under the skin in ear canal); osteoma (round bony growth/benign tumor)
10
New cards
effusion
accumulation of fluid in middle ear space
11
New cards
otitis media with effusion (OME)
serous (fluid present without infection); acute (fluid present with infection); chronic (effusion remains for a while); mucoid (purulent), glue ear (effusion became highly viscus and can bind to structures; conductive HL with a small but present ABG
12
New cards
perforation (what is it and how does it heal)
hole in the tympanic membrane; generally heals spontaneously, but sometimes only partially heals and tympanoplasty may be needed which is putting a graft over the hole in eardrum
13
New cards
causes of trauma/physical puncture or rupture of the TM
foreign object, OME
14
New cards
barotrauma
rupture of TM due to rapid or extreme pressure changes (ex. explosions, scuba diving)
15
New cards
monomere/monmeric TM
when the TM heals from perforation without the fibrous layer
16
New cards
cholesteatoma (what is it, what is it made of, what is the effect, how is it caused, how is it treated)
benign pseudotumor in middle ear; made of dead skin and keratin; can cause breakdown of middle ear and surrounding structures; can be congenital or caused by OME or trauma; has to be surgically removed
17
New cards
otosclerosis
bony growth on wall of inner ear called otospongiosis (spongy one) that eventually hardens; stapes fixation into oval window is most common(growth around footplate of stapes that limits sound transfer of whole system); can end up invading cochlea; more common in females (20-40yo, exacerbated by hormonal changes(pregnancy)) ; conductive HL; treated by a powerful hearing aid or stapedectomy surgery
18
New cards
what kind of HL is seen with otosclerosis
conductive with Carhart's notch (small dip in BC at 2000Hz)
19
New cards
myringotomy
surgeon puts a hole through TM to suck fluid out from middle ear space, if it keeps coming back they will put a PE tube (typical for kids, PE tube not common for adults)
20
New cards
stapedectomy (tx of otosclerosis)
removal of stapes bone, which is replaced with a fat pad to cover the oval window, prosthesis attached to incus, entire ossicular chain may be replaced; 90% of hearing back unless prosthesis moves which would bring back the conductive HL
21
New cards
ossicular discontinuty (what is it, what is it caused by, what kind of HL, what type of tympanogram)
separation/break of one or more ossicles but typically it is of the long process of incus; caused by trauma (slap on side of head, head injury, necrosis (death of bone) from OME or cholesteatoma); results in moderate to moderately severe conductive HL with the greated ABG possible of 60dB; typa Ad (hyper complient, high admittance)
22
New cards
glomus tumor (what is it, how does it form, what does it cause, how is it treated)
benign, slow growing vascularized (red) tumor that forms from the paraganglia (neural cells) in the middle ear (invades middle ear space); can cause pulsatile tinnitus (can hear pulse in ears) and conductive HL; requires surgical removal
23
New cards
NIHL
one of the most common forms of acquired sensorineural hearing; caused by exposure to loud sounds (impulse of sustained); damage to stereocilia starting with outer hair cells, can cause metabolic changes in cochlea, can rupture inner ear membranes; usually bilateral
24
New cards
temporary threshold shift
what NIHL begins with; muffled hearing and tinnitus for a while
25
New cards
permanent threshold shift
NIHL at exposure to sounds 3k-6k Hz, causes a notch at 4kHz
26
New cards
national institute for occupation safety and health
more conservative; max dose of noise is 8hr 85dBA within 24hr and every inc of 3dBA cuts acceptable exposure time in half
27
New cards
occupational safety and health administration
less conservative; max dose of noise is 8hr 90dBA within 24hr and every inc of 5dBA cuts acceptable exposure time in half
28
New cards
presbycusis
age related hearing loss; half of those aged 65-75 have some degree of high f SNHL
29
New cards
menieres disease what is it and symptoms
endolymphatic hydrops; episodes of vertigo w vomiting; low f SNHL; aural fullness; low pitched tinnitus ; usually unilateral at onset
30
New cards
endolymphatic hydrops
with menieres, excessive buildup of endolymph in the scala media and vestibular labrynths
31
New cards
menieres tx
may include smoking cessation, eliminating coffee, reduced salt, prescription diuretics, endolymphatic shunt (surgery to drain), destruction of inner ear structures
32
New cards
ototoxicicity
damange to organ of fearing from noxious substances, therapeutic agents (chemo drugs, aminogycosides, loop diuretics, salicylates/aspirin, antimalaria drugs); monitoring occurs
33
New cards
ototoxicic aminoglysides; chemo agents
-mycin drugs, broadband strong antibiotcs (some only affect balance=vestibulotoxic); -platin drugs, generally permanent SNHL;;;HL starts in high f as a precipitous loss that progresses to lower fs
34
New cards
ototoxic loop diuretics
treat edema (fluid build-up) in body; w congestive heart failure, lung disease, renal disease; furosemide, bumetanide; impacts the stria vascularis; dosage dependent; generally temporary
35
New cards
ototoxic salicylates
anti-inflammatory drugs (mainly aspirin); sometimes high dose is required to treat rheumatoid arthritis; can cause tinnitus and typically temporary moderate SNHL
36
New cards
ototoxic antimalarial drugs
quinine and chlorquine; generally temporary bilateral high f SNHL
37
New cards
infection of inner ear, post-natal exposure
generally a consequence of another disease 1. bacterial meningitis (bacteria access the inner ear via the cochlear acqueduct or internal auditory canal) 2. untreated OME or cholesteatoma (invades via the oval or round windows
38
New cards
infection of inner ear, in-utero exposure
1. cytomegalovirus (CMV) (delayed onset HL, other birth defects) 2. herpes zoster (cause bilateral severe SNHL) 3. syphilis (cause bilateral severe SNHL)
39
New cards
sudden SNHL
rapid onset (within hours), begins as moderate, symptoms=aural fullness/tinnitus/sometimes dizziness, causes=autoimmune disorders/viral atteck/vascular embolism/menieres/acoustic neuroma/closed-head traume
40
New cards
temporal bone fracture
result of non-penetrating trauma aka closed head injury that can lead to HL and vestibular dysfunction
41
New cards
temporal bone fracture, transverse fracture
perpendicular to otic capsule, inner ear damage likely, less common, can result in CSF leakage
42
New cards
temporal bone fracture, longitudinal fracture
parallel along petrous portion of temporal bone, generally middle ear involvement only, can result in CSF leakage
43
New cards
neural disorders, retrochoclear lesion
problem behind the cochlea (can be inside auditory nerve)
44
New cards
neural disorders, distal neural lesion
problem beyond the cochlea before the brainstem
45
New cards
neural disorders, peripheral lesion
problems with hearing that do not involve the brain
46
New cards
acoustic neuroma (aka vesetibular schwannoma or acoustic schwannoma)
beign, slow growing tumor arising from schwann cells of vestibular portion of 8th CN; found in brainstem (cerebellar-pontine angle); fills IAC and compresses nerves; results in high f SNHL; causes tinnitus and poor word recognition; abnormal ABR (auditory brainstem response) and acoustic reflexes
47
New cards
auditory neuropathy spectrum disorder (ANSD aka auditory dyssynchrony)
present at birth, results from uncoordinated firing of aud nerve (so it is unable to transmit neural output from cochlea to brainstem); SNHL, poor word rec, absent ABR, present cochlear microphonic, present OAEs
48
New cards
central auditory processessing disorders (CAPD)
nervous system related auditory deficit that interferes w processing auditory info. no cure, therapies can try to retrain brain
49
New cards
auditory processing
how the CNS utilizes/interprets auditory info
50
New cards
3 skill sets of auditory processing that can be affected w CAPD
1. auditory discrimination, 2. temporal processing, 3. binaural processing
51
New cards
auditory discrimination
Analyze acoustic differences between speech sounds
52
New cards
temporal processing
timinng interpretation: duration of a sound, how quickly sound changes, duration of entire signal aka word/phrase
53
New cards
binaural processing
communication of the the hemispheres of brain
54
New cards
levels of binaural processing
brainstem level (ears interact to help with localization and noise management), cortical level (integrating info and adding new info as it comes which is needed for convo and notetaking), separation (focus on one target and ignore everything else
55
New cards
cause of CAPD
lesions along auditory pathway inclcuding the central structures (retrocochlear, brainstem, right and left hems); could also be from central deafness but that is rare and is the complete inability to categroize sound stimuli with the peripheral system intact
56
New cards
symptoms of CAPD
diff w understand speech in noisy enviros, localizing sound source, hearing on phone, understanding prosody changes in humor/sarcasm
57
New cards
what makes CAPD diagnosis tricky
there are many conditions that can cause diff with listening, comprehension, and attention so you can't just diagnose this from symptoms
58
New cards
types of CAPD tests
detailed case history, behavioral test batteries, electrophysiologic tests
59
New cards
what age do u have to be to be properly tested for CAPD
7, because you have to have baseline of higher level processing skills such as learning, attention, language to be able to be properly diagnosed using a multidisciplinary team; the tests are hard and take forever
60
New cards
CAPD test redundancy
two tests should indicate problems, just one or all showing problems means its prob not CAPD
61
New cards
three major CAPD profiles
decoding deficits, integration deficits, prosodic deficits
62
New cards
decoding deficits
understanding speech based problem= system can't extract pitch/loudness/timing cues, considered truest of all CAPDs bc its all auiditory-based deficit, discrimination based problem, located in left hem and/or high brainstem
63
New cards
integration deficits
deficit in comm btn right and left hems (cortical), unable to combine infor and synthesizr meaning, hard to process info quickly, system becomes easily overwhelmed when lots of info is given, so someone would have a hard time taking notes
64
New cards
prosodic deficits
Unable to process the rise and fall in pitch and loudness (syllabic emphasis/intonation), Right hemisphere problem (aka Right Hemisphere APD), Difficulty with analysis and synthesis of prosodic features related to communication
65
New cards
CAPD tx
no cure all but there are 2 types: 1. bottom-up (stimulus driven, trying to help retrain system)=auditory training, skills remediation, environmental modifications such as AAC (often multiple types in various scenarios; 2. top-down (strategy driven)=language,cognitive,metacognitive strategies, educational interventions, workplace,recreational,home accommodations
66
New cards
direct CAPD tx strategies
attempt ot remediate the processing deficits directly such as one-on-one therapy options, computer based listening tasks, home-based therapies but theres not rlly evidence
67
New cards
auditory training
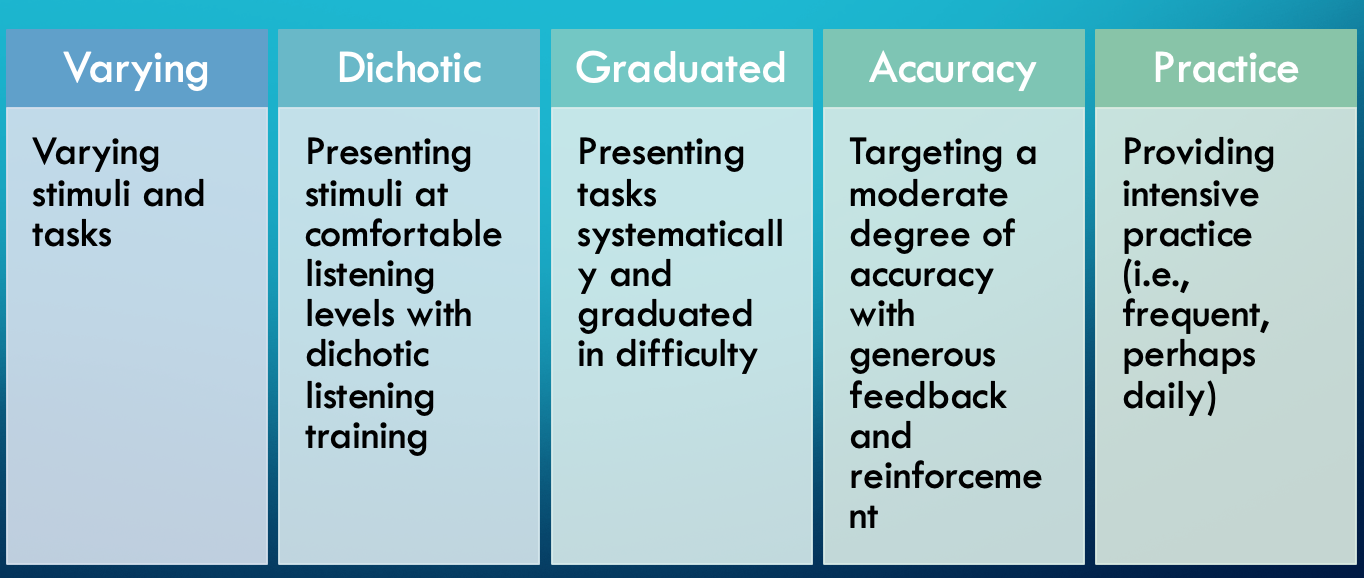
68
New cards
inner ear development in utero by month
2- vestibule vs cochlea, 3- adult form, 4-5- hair cell differentiation and rapid growth, 6- near adult size, 7- first auditory experiences
69
New cards
middle ear development in utero by month
1- eustachian tube begins, 2-ossicles begin, 3-adult form, 4-5- ossicles form and begin to ossify (harden), 7- ossicles fully ossified, 8-tympanic cavity opens
70
New cards
outer ear development in utero by month
2-canal begins, 6-pinna adult form, 7- canal opens
71
New cards
syndromic hearing loss (SHL)
HL accompanied by additional clinical features, about 30-40% of all HL; common co-morbidities: abnormalities with eye, kidney, musculoskeletal, nervous system, metabolic disorders
72
New cards
connexin 26
half of SNHL are due to mutation in GJB2 which is responsible to this inner ear protein; responsible for creation of ion channels and is located in scala media (with organ of corti) and is involved with regulating potassium levels that allow hair cells to create action potentials
73
New cards
aminoglyconside induced hearing loss
mitochondrial inheritance of a predisposition to ototoxicity from these antibiotics even permanant profound HL from just one dose
74
New cards
usher syndrome
one of most common SHL, affects retinas, autosomal recessive inheritance
75
New cards
usher syndrome: USH1
congenital severe to profound SNHL and vestibular dyfunction/early night blindness w progressive narrowing of visual field to severe blindness
76
New cards
usher syndrome: USH2
congenital moderate to severe SNHL with no vestibular dysfunction/ retinitis pigmentosa diagnoses btn 10-40yrs
77
New cards
usher syndrome: USH3
most rare type/late onset progressive HL until profound in 30s with varied vestibular problems/variable progression of retinitis pigmentosa
78
New cards
waardenburg syndrome
disorder of pigmentation of eyes,hair,skin,srtia vascularis in cochlea/autosomal dominant inheritance (1-3% of all congenital HL)
79
New cards
classifications of waardenburg
pigmentation variety (often blue eyes and white forelock): W1=60% have SNHL and dystopia canthorum (wide-set eyes)/W2=90% have SNHL/W3=SNHL, dystopia canthorum and musculoskeletal abnormalities of the upper limbs/W4= addition of Hirschsprung disease
80
New cards
why does asha think it was unethical for audiologists to sell hearing aids in the past
audiologists might suggest a higher price than is actual for their benefit
81
New cards
what kind of hearing aid do kids get
behind the ear because their ear grows too fast and it would be too expensive. also they prob need FM systems in schools and that is only way to get it
82
New cards
hearing aid fitting sequence
assessment, treatment planning, selection, development, verification, orientation, validation
83
New cards
pendred syndrome
most common cause of autosomal recessive syndromic HL/ associated with broad range of HL/ often includes enlarged vestibular aqueduct (EVA)/ progressive HL that is sometimes sudden, 65% of time there is progressive vestibular dyfunctionmay include mondini malformation (not enough turns in cochlea)/ hallmark of syndrome=goiter (thyroid dysfunction, enlarged)
84
New cards
branchio-oto-retinal (BOR) syndrome
autosomal dominant inheritance/ disruption of tissue development in neck, malformation of ears and kidneys/ brachio=second branchial arch which may result in cleft cysts or pits near collar bone/ oto=HL that can be any of the three types and may have pre-auricular pits or tags/ renal=kidney structure abnormalities which can result in end-stage renal disease later in life
85
New cards
charge syndrome
autosomal dominant inheritance/ presentation varies widely/ acronym: Coloboma (gap/hole in iris/eyelid); Heart defects; choanal Atresia (narrowing of nasal passage); Restriction (in growth/development); Genital abnormalities; Ear abnormalities (middle and inner ear problems with hearing and balance issues)
86
New cards
alport syndrome
usually x-linked/ causes progressive kidney failure which leads to end-stage renal disease where u may need dialysis and kidney transplant/ progressive SNHL which can progress to profound/ usually identified in late childhood school age and may require cochlear implantation
87
New cards
jervell and lange-nielsen
autosomal recessive inheritance/ congenital SNHL/ arrhythmia/ prologation of the QTc interval resulting in fainting or sudden death
88
New cards
stickler syndrome
can be dom or rec/ includes diffs in eyes (severe myopia), musculoskeletal (joint laxity), orofacial structures, and ears and hearing/ 5 diff subsets depending on genes encoding diff collagen types
89
New cards
stickler syndrome variants
marshall syndrome (shorter stature, similar other features)/ pierre robin sequence (cleft palate, glossoptosis which is when tongue is further back in oropharynx, micorgnathia which is small jaw)
90
New cards
treacher-collins syndrome
autosomal dom inheritance/ affects development of he bones and tissues of face (midface), affects jaw which can impact airway, feeding, and speech/ half of people with this have hearing loss=usually conductive, and is due to abnormalities of outer and middle ear aka microtia,atresia,or anotia and ossicular abnormalities
91
New cards
hearing aid candidacy
assessment of HL, resolution/consideration of medical issues related to ear/consideration of patient interest/audiometric candidacy
92
New cards
audiometric candidacy for hearing aids
minimum HL: mild HL in 500-4kHz region/ severity: if HL is too great may need CI/ WRS: poor word rec may impact benefit/ speech in noise testing: may need advanced technologies to help in noise/ loudness discomfort level (LDL) and uncomfortable level (UCL): pt may not be able to tolerate loud sounds
93
New cards
two types of basic hearing aid technologies
analog: og tech, no computer processing, sounds collected and amplified, generic fitting strategies/ digital: standard of hearing care, sounds collected and processed, highly programmable to pt's needs, better features to manage noise
94
New cards
digital features of hearing aids: multiple channels
able to adjust aid output in discrete f regions to make speech clearer
95
New cards
digital features of hearing aids: multiple programs
can put automatic settings like a restaurant setting
96
New cards
digital features of hearing aids: compression (automatic gain control AGC)
limits how loud sounds get and minimized distortion, there is a cutoff so loud sounds couldn't hurt hearing, wide dynamic range compression (WDRC) preserves the experience of loudness so they can still tell if a noise is loud of quiet but still sounds natural
97
New cards
digital features of hearing aids: directional microphones
one forward facing and one rear facing microphones, these allow the aid to determine location of speech vs noise, processing allows for Digital Noise Reduction which reduces background noise based on its freq range and location aka cuts off back microphone when they want to hear someone they are looking at
98
New cards
digital features of hearing aids: feedback reduction
phase cancellation of feedback sounds
99
New cards
digital features of hearing aids: linked hearing aids
sounds from one aid can be transmitted wirelessly to opposite ear
100
New cards
digital features of hearing aids: data logging
says how long aids are worn, user adjustments to volume and programs, and assesses pt's enviro throughout day