DHYG 210: Occlusal Exam
1/34
Earn XP
Description and Tags
Tues, Sept 23rd 2025
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
35 Terms
What is Dental Occlusion
The relationship that occurs when the maxillary and mandibular teeth come together in functional contact
4 Aspects to an Occlusal Examination
The morphology of the dentition
Physiological state of the dentition
The dentition and the temporomandibular articulation
Habitual patterns of dental contact
Describe the two ways we measure physiological integrity
Structural integrity
Evaluated by examining the teeth for excessive or premature wear
Ex. cracking of enamel, fractured cusps, and failing restorations are some of the signs
Mobility (structure of teeth, etc)
Another cardinal test of physiological integrity
Doesnt signify perio disease, but may indicate excessive occlusal loading
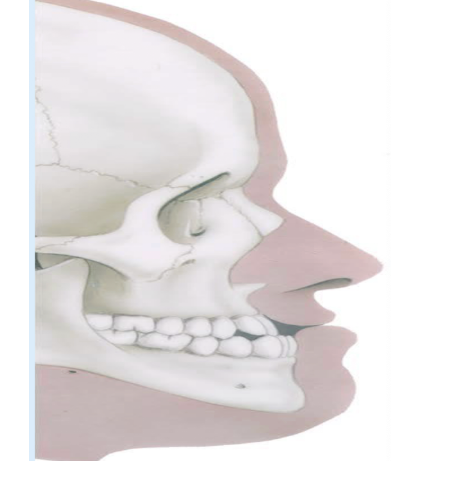
Describe the structure and function of the TMJ Articulation
Structure
Composed of condyle in a fossa with a disc interposed between two bony surfaces
The TMJ is lubricated
Function
Functions with a degree of rotation followed by translation down the eminence as jaw opens (the jaw first rotates and then slides)
Teeth alignment
Intercuspal tooth position needs to be stable to allow for proper joint function
Tooth guidance needs to be in harmony with jaw function
Pathology (problem w/ TMJ) can include: disc malposition, myalgias (muscle pain) and intra-articular joint inflammation
Describe the 4 components of the TMJ examination
Palpation - assessment of tenderness bc it is a possible signs of inflammation; assess intra-meatally and by lateral pole
Joint sounds - ideally checked w/ stethoscope, and you need to distinguish between click, pop, crack or crepitus; also check for timing
Range of motion - objective measure; inter-incisal distance; measure if client experiences pain or no pain; vertically and laterally; f-35 and m-40, laterally 8mm
Jaw trajectory - mandibular deviations from midline on opening and closing (if jaw moves off center instead of up and down)
Describe what the Intercuspal Position is
It is where the teeth have the most contact and your jaw is in a comfortable, stable position
“the best fit” of your teeth when you bite down

What is an Acquired but “Functional” Intercuspations
When the teeth doesn’t line up in a “perfect/normal” way, but the person has adapted to it and the bite still functions normally

What is an Ideal Static Occlusal Contact?
When the upper and bottom teeth hits where its supposed to hit

What does the Actual Maxillary Occlusal Contact look like in a Normal Adult?
The ideal is 34 contacts, but the average in a healthy young adult is 14 contacts
Most of us function quite well without meeting the ideal number of contacts
What are the most important aspects of an occlusal examination?
It is the inspection of tooth wear patterns
While some patterns of wear are due to malocclusion, others are simply the consequences of a habit (ex. Being an oboe player would change your teeth into a circular shape?)
What do mild and moderate occlusal wear depend on?
Whether considered mild or moderate, wear depends on age and social circumstances of an individual
What are the mechanisms of Non Carious Cervical Lesions? (damage at the cervical not caused by caries)
Endogenous (attrition)
damage from forces inside the mouth
Normal occlusal function - such as chewing and deglutition (swallowing)
Parafunction - harmful habits such as bruxism and clenching
Exogenous (abrasion/friction)
damage from outside forces or habits
Abrasion by overzealous brushing, flossing, tooth pick use
Habits - nail biting and pen chewing
Occupational behaviours - sewing, playing instruments
Oral appliances - orthodontic, or prosthodontic (crowns, dentures, implants)
Ritual behaviours, ethnic practises
What is the theory of the Abfraction?
A proposed explanation for NCCL
The idea suggests that the loss of cervical tooth structure is due to flexural forces (blending stresses) rather than caries
The forces come from repeated (cyclic) non-axial loads, meaning pressure that isn't straight up and down but grinding or off-centered biting
What is Bio-corrosion and what are their 3 different causes
Bio-corrosion: chemical or enzymatic breakdown of teeth (from inside or outside), leading to enamel and dentin loss - “melting” of tooth structure
Three different causes:
Endogenous: bacterial acid degradation and acid reflux or bulimia - non metallic corrosion
Exogenous: (chemical acids) such as lozenges, carbonated drinks, fruits
Proteolytic corrodents: enzymatic breakdown of teeth, such as enzymes in caries, protease from pancreas, and pepsin from stomach
What are the multifactorial causes of wear?
Attrition due to normal function and parafunction
Abrasion and erosion due to environmental influences
Bio-corrosion or chemical erosion due to specific types of food, bulimia, or stomach reflux
Loss of tooth structure due to physical means and/or habits
What is the purpose of an Occlusal Examination Protocol?
To visually assess the dentition so you can document the gross form of the occlusion (such as tooth position, arrangement, and contact pattern)
Record occlusal contacts between maxillary and mandibular teeth
Determine molar classification
Document and record areas and degree of tooth wear
Visually assess dynamic tooth contact patterns (ex. Canine rise vs group function)
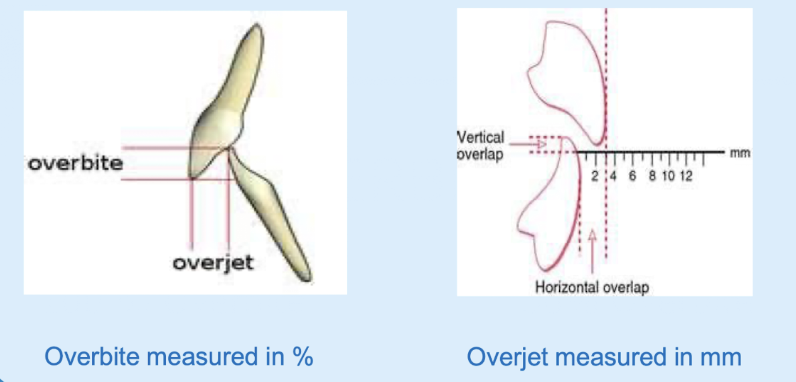
What is Overjet and Overbite and how are they measured?
A measure of vertical and horizontal overlap
Overbite
how much the upper central incisor overlaps the lower central incisors
measured in %
Overjet
the distance between the lingual surface of the upper central incisor to buccal surface of the lower central incisors
measured in mm
What is an Openbite Malocclusion
When the anterior teeth do not touch when the mouth is closed, usually only the 2nd molars are the only occlusal contact points
Why it happens:
Tongue thrust habit
Possible thumb sucking habit as toddler
Orthodontic relapse

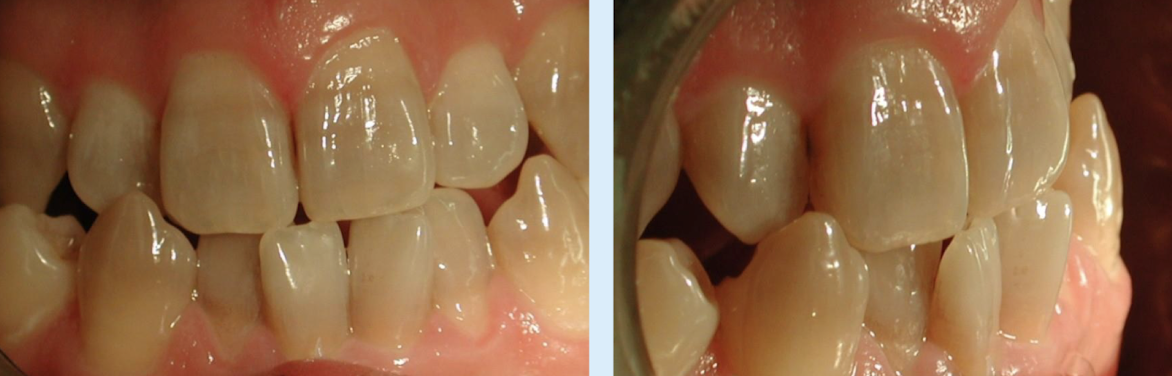
Anterior Crossbite
when a single or multiple anterior teeth sits behind the lower teeth

Posterior Crossbite
when the upper premolar/molar sits behind the lower teeth

Class I
defined by a normal molar and canine relationship
where mesiobuccal cusp of upper 1st molar is located over mesiobuccal groove of lower molar


Class II
where the jaw is retrognathic
Malocclusion
Skeletally and Dentally retrognathic ( overbite)
First molar relationship more distal; upper canine is more forward than lower

Deep Class II Malocclusion
Characterized by an upright upper and lower anterior and an increased overjet and overbite

Class III
it is prognathic
A malocclusion
Skeletally and Dentally pronathic ( underbite)
the lower 1st molar is in front of the upper 1st molar; lower canine is also infront of upper
Class III malocclusion
Multiple crossbites
when the lower canine-lateral-central sits in front of the upper

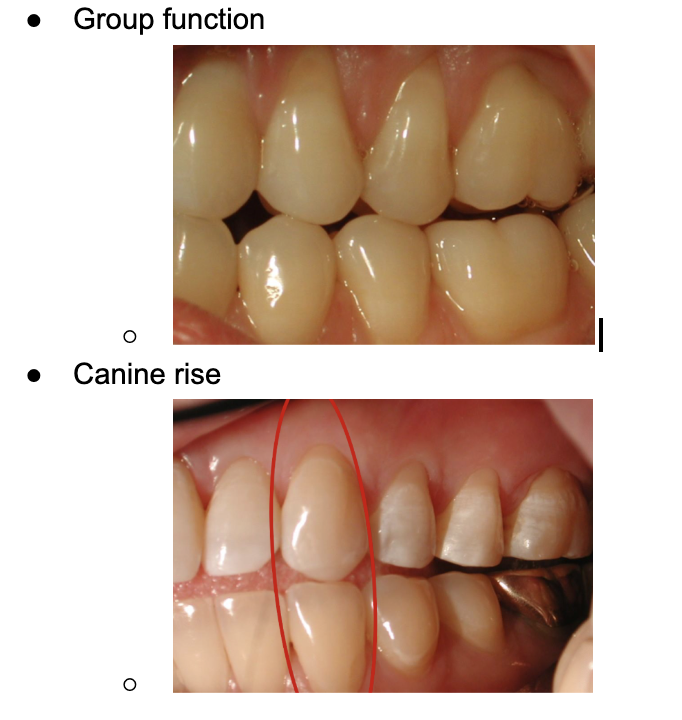
What are the two latero-protrusive jaw movements? (how the tooth move side by side)
Group function - multiple posterior teeth sharing the load during lateral movements, can lead to wear and TMJ stress
Canine rise - only the canines contact during lateral movements
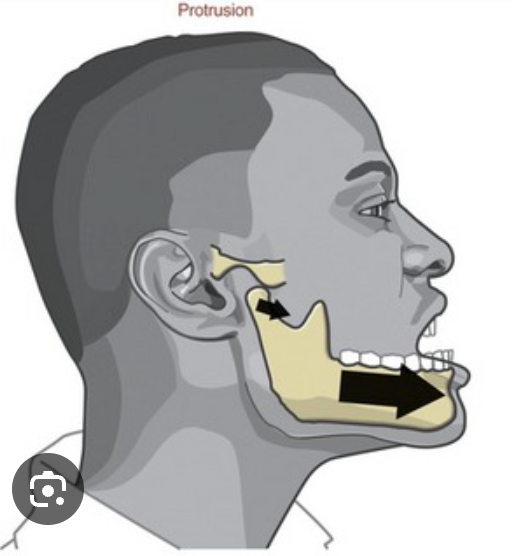
What are Protrusive Movements?
when the mandible moves forward from the normal bite position - guided by the anterior teeth and also protects the posterior teeth from wear
What is Bruxism and the two types?
Diurnal or nocturnal parafunction affecting up to 20% of the population
Two types: awake bruxism and sleep bruxism
What is Awake Bruxism
Tooth clenching and/or jaw bracing triggered by mental concentration, emotional stress, and/or anxiety - people with this are usually aware of their habits
What is Sleep Bruxism (SB)
Unconscious tooth grinding and clenching - affects about 8% of the population, can be mild, moderate or severe
Moderate to Severe SB is consider a sleep disordering when following criteria are met:
Frequent grinding noises at least 5x per week confirmed by a sleeping partner
Non-masticatory tooth wear in at least one sextant with (not from chewing food, but from bruxism):
enamel reduction
dentin with loss of crown
Masseter muscle hypertrophy of 2-3 times the normal muscle volume during contraction
What is Abnormal Repetitive Movement Disorder and what are their two overlapping types?
Jaw clenching and tooth gnashing or grinding
Two overlapping types: awake (AB) or sleep bruxism (SB)
How is a Repetitive Jaw-Muscle activity characterized by?
Clenching or grinding of teeth and/or bracing or thrusting of the mandible
Night-bruxer (Adult) - what are their characteristics?
Someone with long history of parafunction
Occlusal and cervical wear in both arches
Hypertrophic masseters commonly
Complaints of sensitivity being on and off
Restorative and esthetic needs due to breakdown
What is Lower Anterior Wear
Severe wear due to parafunctional habit, nighttime bruxism, and worsens with opposing metal ceramic crowns