POM II - Labor and Delivery - Exam 5
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
Labor
Regular painful uterine contractions resulting in changes in cervical effacement and dilation
Braxton Hicks Contractions
Irregular, generally painless or slightly uncomfortable uterine contractions that occur during pregnancy and do not lead to cervical change
Cervical Dilation
the opening of the cervix during labor, measured in centimeters from 0 to 10
Cervical Effacement
stretching/thinning of the cervix to prepare for delivery, measured from 0-100%
Engagement
When the fetus drops into the pelvic inlet, near delivery
Station
The position of the fetal head in relation to the ischial spines of the pelvis, measured from -3 to +3
Fetal presentation
the part of the fetus that enters the birth canal first
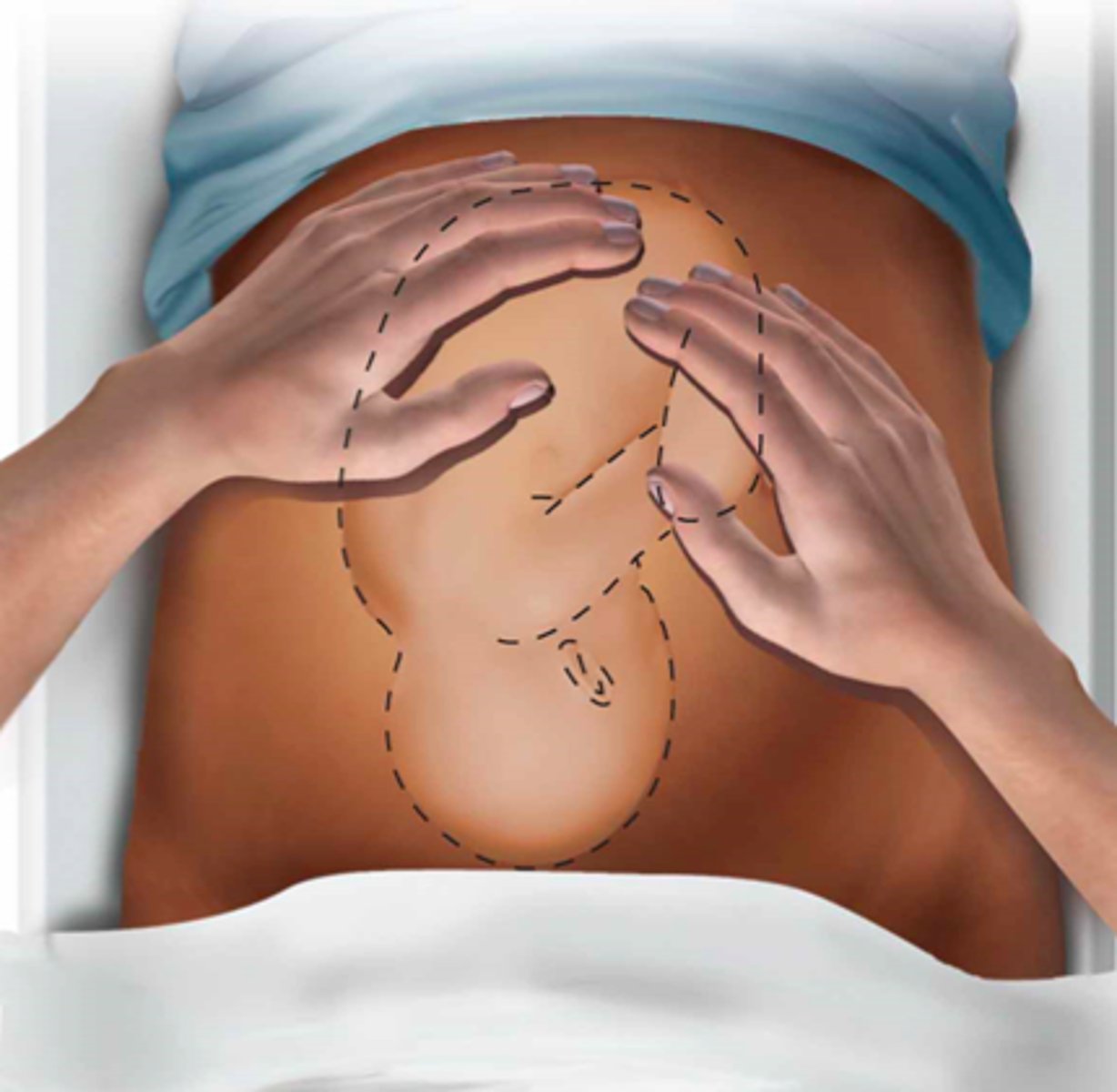
Leopold's Maneuvers
Abdominal examination of fetal position begins with what?
Fundal Grip - 1st manuever
Examiner places both hands on each upper quadrant of the patient's abdomen and gently palpates the fundus of the uterus with the tips of the fingers to define which fetal pole is present in the fundus
hard and round
if a fetus is cephalic, how should it feel with the fundal grip?
Podalic Fetal Position - Fundal Grip
one will note a large, nodular body with an uneven surface, non-ballotable, and not very mobile
Second Leopold Maneuver
palpation in the periumbilical regions with both hands by applying gentle but deep pressure

Second Maneuver - Purpose
to differentiate fetal spine (a hard resistant structure) from the limbs (irregular, mobile small parts) to determine the fetus' position
Third Leopold Maneuver
suprapubic palpation by using the thumb and fingers of the dominant hand
examiner ascertains the fetus' presentation and examines its station
if presenting part is not engaged, a movable body can be felt
Allows for assessment of fetal weight and volume of amniotic fluid

Fourth Leopold Maneuver
Palpation of bilateral lower quadrants to determine if the presenting part of the fetus is engaged in the mother’s pelvis
Examiner stands facing the mother’s feet. With the tips of the first 3 fingers of both hands, exert deep pressure in the direction of the axis of the pelvic inlet.

diverge
For the Fourth Maneuver, In cephalic presentation, the fetus' head is considered engaged if the examiner's hands _________ as they trace the fetus' head into the pelvis
Stage 1 of Labor
Interval between onset of contractions and full cervical dilation (10 cm).
Stage 1 Latent Labor
-Associated with slow dilation
-Mild contractions, variable in duration
-Can usually talk through contractions
-0-6 cm
Stage 1 Active Labor
Associated with a faster rate of dilation
Moderate to strong contractions lasting 45-90 seconds and occurring every 2-5 minutes
Analgesia and or anesthetic
6 to 10 cm
Stage 2 of Labor
Interval from complete cervical dilation (10 cm) to expulsion of the fetus (baby delivered)
Starts when mother has strong desire to “push” with contractions
Stage 3 of Labor
Interval from expulsion of fetus to expulsion of placenta
Best to look for lacerations/tears before placenta delivers
Inspect for completeness/abnormalities
Sent to pathology
hours to days
what is the length of latent stage 1 of labor?
hours
what is the length of active stage 1 of labor?
30 mins to 3 hrs
what is the length of stage 2 in a primigravida (1st pregnancy) woman?
5-30 min
what is the length of stage 2 of labor in a multiparous woman?
<30 min
what is the length of stage 3 of labor?
<6 cm
how much is the cervix dilated in latent stage 1 of labor?
6-10 cm
how much is the cervix dilated in active stage 1 of labor?
fully dilated at 10 cm
how much is the cervix dilated in stages 2 and 3 of labor?
Common Labor Positions
Lateral (Sims) position
Partial sitting position
Lithotomy position -> Advantageous if fetal manipulation or need for optimal surgical exposure is anticipated
every 30 min
when should you do fetal monitoring during stage 1 of labor?
every 15 min
when should you do fetal monitoring during stage 2 of labor?
continuously
when should you do fetal monitoring in at risk pregnancies?
Engagement
First Cardinal Movement
Fetus descends into pelvic inlet
Descent
Second Cardinal Movement
Passage through pelvis
Flexion
Third Cardinal Movement
Flexing fetus neck, smallest diameter of head passes through pelvis
Internal Rotation
Fourth Cardinal Movement
Passive rotation of presenting part (head) from its original position (transverse) to AP as it passes through the pelvis
Extension
Fifth Cardinal Movement
Occurs once descended into introitus
External Rotation
Sixth Cardinal Movement
After fetal head reflexes, it rotates (fetal head outside the mother)
Helps deliver anterior shoulder
Expulsion
Seventh Cardinal Movement
Delivery of fetus
Brandt-Andrews Maneuver
Gentle, steady traction on the cord combined with upward pressure on the lower uterine segment
Traction with 1 hand
Counter-traction with other hand ("lifting" the uterus)
placental separation (impending expulsion)
should start Brandt-Andrews Maneuver when there is clinical evidence of what?
Placental Separation S/S
Fresh show of blood
Umbilical cord lengthens
Fundus of uterus rises up
Uterus becomes firm and globular
Brand-Andrews Maneuver Comp
uterine inversion -> potentially fatal, but very rare
increased risk of postpartum hemorrhage
Postpartum Uterus
attempts to return to pre-pregnancy size and condition (AKA involution)
Fundus of uterus decreases in height by 1 cm per day
By 1 wk postpartum, about the size of a grapefruit, may no longer be palpable through abdomen
1st Degree Vaginal laceration
skin around vaginal opening tears
heals spontaneously in about 3 weeks
2nd Degree Vaginal Laceration
Vaginal Tissue and Perineal muscles (supports uterus, bladder, rectum)
Needs repair, pain meds, and stool softeners
3rd Degree Vaginal Laceration
Vaginal tissue, perineal muscles, and muscles around anus
Surgical repair, pain meds, stool softeners
4th Degree Vaginal Lacerations
all of the above tissues and lining of rectum
Surgical repair, pain meds, stool softeners
Complications: fecal incontinence, painful intercourse
<500 mL
what is normal expected blood loss during vaginal delivery?
>500 mL blood loss with S/S of hypovolemia (dizziness, fatigue, thirst, and dry mucous membranes)
what is considered postpartum hemorrhage?
PP Hemorrhage Causes
Tone (70%) --> Atonic uterus
Trauma (20%) --> Lacerations, hematomas, inversion, rupture
Tissue (10%) --> Retained tissue, invasive placenta
Thrombin (1%) -->Coagulopathies