Perinatal Nursing
1/128
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
129 Terms
Perinatal Nursing in Canada
Provides care from pre-conceptions, pregnancy, birth (both mother & newborn), to 3 months postpartum
Defining Risk in Perinatal Nursing
Pregnancy & birth are considered normal & health (not risk)
Typically done through scoring but is typically challenging & unreliable due to accuracy of scoring
Defining normal & high risk should be based on context of situation
Challenges associated with determination of risk
Complications are varied: can be related to pregnancy or known/unknown pre-existing medical condition
Complications can occur at varying times during pregnancy & postpartum
ie: HTN or cardiac complications
Classifications can lead to unnecessary interventions such as fetal monitoring or bed rest
Can be difficult to discern abnormal symptoms based on the pretext it is normal with the risk situation
Low vs high vs complex high risk
Low risk
has predictable psycho-social & perinatal/medical health & outcomes
I.e.: stable mental & physical health
Pregnancy health on normal trajectory
High risk
has predictable psych-social, unpredictable perinatal & predictable medical health & outcomes
i.e: stable mental health / past Hx addictions or violence + stable medical conditions such as lupus or diabetes + common pregnancy complication such as gestational HTN, PPROM, or preeclampsia
Complex high risk
has unpredictable psycho-social & perinatal/medical health & outcome
i.e: current addiction/methadone or current family violence or unstable mental health or potential lethal fetal anomalies + acute medical condition such as Acute RF or active lupus + complicated pregnancy complications such as PPROM < 26 weeks or unstable twin-twin transfusion + unique medical interventions/complications
Parental Transition challenges & Supports for Low, High & Complex Risk
Low risk:
Predictable parenting challenges & needs
High independence in self-care & self-efficacy
Usually self-directed in meeting needs
Can offer community prenatal education to support self-directed learning
Best practice/theoretical approaches to teaching & learning to meet group/individual needs
High Risk
Potential for parenting transition challenges
Low-mod risk for prenatal attachment issues
Moderate independence in self-care & self-efficacy
Anticipatory guidance important
Offer community prenatal education, parenting programs based on needs (postpartum experiences or breastfeeding)
Best practice/theoretical approaches to teaching & learning to meet group/individual needs
Complex High Risk
Potential for significant parenting transition challenges with unpredictable course
High risk for prenatal attachment issues
Low-moderate independence in self-care & self-efficacy
Will need individualized learning & teaching approaches
practice/theoretical approaches to teaching & learning may not meet needs
Problems with Antenatal Risk Scoring
Accurately predicting obstetric complications is impossible
Only accurately predicts complications in less than 7% women
No evidence suggest risk-assessment tools improve maternal & neonatal outcomes
Women classified as “at risk” or “high risk” can lead to more routine or unnecessary interventions that are appropriate or effective.
Sometimes risk scoring can lead to stigmatizations of women & impose stereotypical adverse set of expectations that may or may not be true
Example: A pregnant women who is obese = high-risk pregnancy
Risk classifications can increase anxiety or fear with unnecessary interventions or wish for greater monitoring & interventions that aren’t necessary
WHO Definition of Normal Birth
Gestation between 37-42 weeks
Singleton fetus
Vertex presentation
Spontaneous onset of labour
Presence of skilled birth attendant
WHO-Euro Bologna Score
Takes into account multiple indicators to determine whether labour is managed as normal birth
Women who have a caesarean birth or have induced labour are excluded
Criteria
WHO original def of normal birth
Gestation between 37-42 seeks
Singleton fetus
Vertex presentation
Spontaneous onset of labour
Presence of skilled birth attendant
Presence of a companion at birth
No labour augmentation (mechanical or pharmacological)
Use of a partogram to monitor labour
Use of a non-supine birth position
Skin-to-skin contact at least 30 minutes within first hour
Canadian Definition of Natural Birth, Normal Birth, Normal Pregnancy/Labour & Normal Delivery
Natural childbirth = involved little or no human intervention
normal birth: excludes elective induction before 41 weeks, spinal analgesia, general anesthesia, forceps or vacuum, c-section, routine episiotomy, & continuous electronic fetal monitoring.
normal deliver: can include interventions such as induction, augmentation, electronic fetal monitoring, artificial rupture of membrane, pharmacological pain relief
Normal pregnancy & labour: can include complications such as HTN, antepartum or postpartum hemorrhage, perineal trauma + repair, NICU admin.
These definitions attempt to accept commonly used current practices as “normal” and not stigmatize women who experience these procedures & interventions as abnormal
Demedicalizing Birth
Medicalizing birth is fuelled by the idea of “at least everything possible was done to prevent a negative outcome” & “each birth has to be perfect & every available technique may be used to achieve this”
Results in routine fetal monitoring, ultrasounds, epidural anaesthetic & c-sections.
Common routine practices such as separation of mother-baby, suctioning of newborn at birth, supplementation with water or breastmilk substitutes, suctioning meconium-stained liquor & intubations & suctioning to prevent meconium aspiration are not evidence-informed & can impact fetal to neonatal transition
Having a support companion & one-one nursing ratio are two very beneficial interventions in birthing process
Purpose of Family Centered Care in Maternal & Newborn Care
Promote optimal wellbeing for mother, child & family
Increases participation of women & families in decision making process
Principles of Family Centered Care
Addresses need of woman, newborn & family + supports from pregnancy-postpartum
Sensitive to psychological + social needs
Culturally sensitive & informed
Individualized to meet families needs
Respect & dignity
Encourage family involvement in-care of newborn despite whether infant is “sick” or “healthy”
Families take active role in decision making
families offered knowledgeable & appropriate care to support breastfeeding & alternatives when needed
Confidentiality
Thrives on feedback from families
Person Centered Care
A care practice approach the focuses on the person as a whole
Takes into account person’s experience of the health or life challenges
Broader view of whole person
Takes into account needs based on SDH
Focus on empowerment through enhancing knowledge, competency & efficacy of self-care and decision making
Give them a voice to share their story & actively listen
Takes all of this in to account to guide your care
Informed Caring for the Well-being of Others
Created by Kristen Swanson
Theory based on perinatal nursing and developed to support women experiencing miscarriages
Focuses on how nurses see and understand people affects who they care for and how they provide care & how it shapes the enviroment they created and the goals of nursing care
Relationships are a central concern in nursing & include nurse-to-client, nurse-nurse & nurse-self
Swanson’s Structure of Caring
Maintaining Belief (esteem): sustaining faith in the others capacity to get through an event/transition & face a future with meaning
Aligns with strength-based approach
Having hope (not the same as false hope) & view optimism
See the positives or strengths and how they can be harnessed to move forward
Knowing (Empathetic Understanding): striving to understand an event as it has meaning in the life of the other.
Striving to understand an event as it has meaning in the life of the other
Arises from nurses knowledge of emotional, psychosocial, spiritual & cultural aspects of health & wellness as they relate to the others experiences or realities & their responses
Do not make assumptions of Judgements
Being With (Emotionally Present)
Be present & share in the meaning & feelings of others (not the nurses) reality
Convey availability: communicate they are not alone & we are here, attentiveness, physical presence (sometimes in silence)
Sharing feelings
Not burdening
Doing for (Enact for)
Doing for the others he/she would do for oneself if able
Protect dignity
Enabling (Empowering)
Enable self-care & self-healing even as you do for them
Provide resources & needed information
Prenatal Factors Affecting Transition to Motherhood
Adverse childhood experiences
Presence or absence of a support network
Difficult labor
Complication postpartum
Neonatal hospitalization
Past losses and mischarges
IVF
substance use
High risk pregnancies
Process of Transitioning to Motherhood
Engagement with maternal task is primary process facilitating transition to Motherhood
Engagement enables the secondary process of growth & rransition
Women often have unrealistic expectations of post-partum period
Inform it is normal to feel overwhelmed, uncertain & experience physical & mental exhaustion during first couple of month.
Social Discourse of Motherhood
Mothering is a social experience that is shaped by society’s structures
Due to this the social discourse of motherhood impacts women’s health
Mothering requires material, economic & social investments that are not usually economically compensated for
Ties into societal expectations of women to care for family and household without compensation
Mothering women are more vulnerable to health risk especially those with overwhelmed workloads, poverty & violence
Forms of Mothering that Do Not Fit Normative Social Discourse of Motherhood
Step mothering
mothering in lesbian couple, gay couple & transgender persons
Surrogate mothers
Mothering by very young women
Mother within a communal house-hold
Grandmothers as primary caregivers
Non-custodial mothering: foster mother
Single mom
Normal = biological & two-parent family
Preconceptual Health Interventions
any interventions that identifies and modifies any risk to male or female reproductive health or pregnancies
Reasons for Preconception Care
Critical developing period of fetus is before women know they are pregnant.
Modifiable or treatable preexisting comorbid conditions such as diabetes, substance use, etc. are linked to adverse perinatal & maternal outcomes
Exposures to toxins can negatively impact fetus
Barriers to Preconception Care
Pre-conception care not routinely being sought out (economic, access, marginalization’s)
Pre-conception care only for those who planned pregnancy
Challenges to provide health educations across diverse populations
Clinicians not being confident or knowledgeable in need for preconception care
How many pregnancies are unplanned?
½ of all pregnancies are unplanned
Integrated Psycho-Social-Medical Model During Pregnancy
Traditional guidelines for antenatal care emphasize clinical assessment but often over look psycho-social aspects of pregnancy
Studies found woman values psychological & social support as much or more than clinical care
Psychological supports: reasonable wait times, unhurried visit, continuity of care & caregiver, flexibility, comprehensive care, meeting with other pregnant women in groups & develop loving relationships with professions
Women need information not just on common discomforts of pregnancy but also warning signs indicating need for professional
View pregnant women & families as active partners in care
Provide adequate resources to prepare for child such as birthing classes
Prenatal classes are often under attended
Integrated Psycho-Social-Medical Model During Labor & Birth
Women & birthing families often report clinical birth environment stressful: quiet, gentle, supportive, & encouraging environment
Encourage skin-to-skin contact
Don’t separate mother & baby
Breastfeed when baby shows signs of readiness in a quiet environment
Encourage siblings to share in the birthing experiences
Indigenous Care
Evacuation of women for childbirth often w/o a support person to hospitals far away is common in remote communities
Community-based Indigenous midwives with an integrated approach of traditional & modern ways are ideal model
Need culture-based prenatal outreach & support programs
Ways to Optimizing Preconception Health
Encouraging women to access preconception health resources
Clinicians taking advantage of episodic visits to identify health risk & offer interventions & encourage positive healthy behaviours prior to conception
Encourage all women & men of reproductive age to develop a reproductive-life plan
Recommend folic acid to all women
Immunizations up-to-date
Review medications for potential teratogenicity & counsel women on impacts to pregnancy regardless of plans to conceive.
Promote smoking cessation & screen for drug & alcohol use
Encourage progress towards healthy weights
Screen for STI or STI risk factors
Optimize chronic medical conditions to improve perinatal & maternal outcomes
Educate on interpregnancy interval for women who have previously given birth
Cultural Dimensions of Pregnancy, birth & Post-natal Care
Impacts how woman perceives & prepares for birthing experience
Different cultures have own values, beliefs & practices related to pregnancy & birth
Some women of same culture will adhere to cultural traditional practices & some won’t
Communication with different languages is a common barrier to providing cultural-informed care
Disclaimers on Cultural Practices & Beliefs of Pregnancy
Terms used to distinguish cultural divergent groups need to be clarified from the perspective of the child bearing person, partner & family
Geographic labels often don’t define cultural uniqueness of populations living within the boarders
Recognize the political & racial forces that guide perceptions of care provider and recipient
Provider: self-reflect on what is guiding your interactions
Recipient of care: personal & ancestral history will be a basis for their perception & engagement in care experience
Culture
Is contextual
Group membership doesn’t imply total subscription to group values, beliefs, attitudes or practices
Influenced by experiences
Avoid assuming culture solely based on race, nationality or ethnicity
There is a difference from culture & race, nationality & ethnicity
Rubin’s Mother & Maternal Role Attainment
Theoretical framework of motherhood
defines maternal role attainment as a process which the mother achieves competence in the role & integrates mothering behaviours into her established role set, so that she is comfortable with her identity as a mother”
Three main principles
Relinquishment of pregnancy role & taking on role of mother is major adjustment
Postnatal maternal-infant role relationship is a continuation of maternal-fetal attachment relationship that started at pregnancy
Progression through developmental stages of new motherhood is individual
Phases of Rubins Mother /Maternal Role Attainment
Taking-in-phase (dependent): 1-2 days; mother self preoccupation as she recovers from delivery, dependent on support persons & caregivers for self & newborn care
Taking-hold phase (independent): 2/3rd day-10days/several weeks mother attempts to take back control & begins to engage with baby, initiate self care & newborn care; attachment process with baby is evident; still accepting help from others
Letting-go phase (interdependent): redefining her new role/relationships, lets go of old self & accepts the new normal.
Positive Influences on the Transition to the Mothering Role
Positive quality of prenatal attachment relationship between expectant mother & unborn baby is predictive of a positive postnatal relationship
Confidence in doing mothering task is related to a mother’s difficulty with daily routine & discrepancies between anticipated & actual maternal responsibilities
Example: If newborn is facing health issue or has care needs the mother is not able to independently for her baby
Earlier a mother holds her infant after birth the sooner the postnatal relationship begins to grow
Attachment & bonding occurs regardless of time
Transition to Fathering
Also requires their own postnatal bonding
Objective disengagement doesn’t = lack of bonding
Common for men to be silent or appear not involve
Presence of men contribute to their infant attachment
Major transitions
Commitment to fathering
Becoming father: need to determine their own identity of fatherhood
Making room for baby in their own relationship with partners
Demands of baby & finding strategies to balance demands of work, partner & baby can lead to exhaustion, stress & confusion
Require social supports
Fathering roles often include that of: provider, guide, household help & nurturer
Often w/o cultural references to look to on the fathering role, new dads can feel helpless, incapable, uncertainty and weak
Stress of fathers are often related to meeting social expectation of fatherhood rather than lack or process to acquire competencies
Lesbian Mothers
Challenges
Experience challenges accessing perinatal services & resources
Experience heteronormative, sexist, non-supportive, non-affirming & insensitive care in perinatal setting
Rely on ART for conception = great financial cost
Parenting rights are not automatic for the non-biological parent, so have to go through adoptive process
May feel disenfranchised or marginalized in a hospital system due to traditional maternal & heterosexual nature
Won’t access care b/c of fear of poor treatment & stigma
In an attempt to normalize or not discriminate clinicians often refer to lesbian families as just another “couple”. Instead an individual approach should be taken based on perspective of persons
A birth partner may feel ambiguity in their parenting roles as the focus is on the birth mother for care. Approaches include:
Assurance of desired level of partner involvement
Acknowledge role & significance of being a parenting partner
Include in conversations
Ask how they would like to be referred to (mom?)
Gay Fathers Pregnancy Process
Pregnancy occurs through surrogacy
Traditional/altruistic surrogacy: surrogate woman pregnant w/ own egg & sperm of donor or prospective father
Gestational surrogacy: donor egg inseminated with sperm of prospective father in lab & is implanted in surrogate
Sperm samples can be mixed to give both men a chance at being biological father
Surrogacy
Legal in Canada
Considered an altruistic arrangement in Canada: can’t pay mothers, only have have pay for expenses incurred
Emotional/relational issues can arise during pregnancy between partners, families, surrogate and friends
Sometimes relationship with surrogate grows and can become part of the family circle
Some surrogate can suffer separation anxiety & depression similar to mother who relinquish babies for adoption
Gay Fathers
Requires reorientation of role & responsibilities including work, caregiving responsibilities and social life
Tend to be more attentive & protective in parenting
Adoption is usually necessary for non-biological father
Integration of self-identity of father & gay man is part of fathering journey
Can have challenges in disclosing family of origin
Transgender Men Pregnancy
Can become pregnant if they retain functioning ovaries & uterus
Requires stopping testosterone treatment if they have physical transitioned to male
Will start menstruation within 6 months of stopping
Testosterone should not be considered an contraceptive
Testosterone has to be stopped during entire pregnancy because it can harm the fetus
Childbearning person should not be viewed in maternal context of pregnancy
Journey to fatherhood not motherhood
Identify as fathers or may prefer a different language (they)
Giving Birth In Canada Following Earlier Female Genital Mutilation
Involves total or partial removal of female external genitalia & or other injuries to female genital organs
Types
Removal of clitoral area, partial or total removal of clitoris &/or foreskin removal
Excision: removal of part of entire clitoris & part/all of labia minora
Infibulation/pharaonic circumcision: removal of medial parts of labia majora & the joining of two side of vulva with thorns, silk or catgut sutures. A small opening is created with the insertion of a foreign body to allow passage of urine & menstrual blood
May require to undergo gradual dilation by husband to allow sexual intercourse
Willl have to be cut to allow passage of baby & then re-sutured
Insertion of corrosive substances in vagina to facilitate “dry” sexual intercourse
Often report
Doctors don’t provide kind of birthing procedures they would prefer
Pressured to get c0section
Pressured to have male companion when female birthing companion would have been preferred
Insensivity regarding pain management
Gender Dysphoria & Pregnancy : Transgender
Some can become more connected with their bodies
Some can have increase in dysphoria
Not being able to present as male can be challenging
Female hormonal changes associated with pregnancy can be distressing
Postpartum Transgender Men
High incidence of postpartum depression
High incidence of feeling of isolation & loneliness during pregnancy & early period of parenthood is associated with high risk of perinatal depression
Exacerbation of gender dysphoria
Lack of gender inclusive resources
Lack of knowledgeable & experiences HCP
Referral to mental health services may be required
Deciding when to restart testosterone therapy
Infant Feeding Transgender Men
Language: may prefer term “chest feeding” but should ask for preference
Likely still retaining breast
May use donor milk
Referral to lactation consult might be a good idea
Risk for IPV Demographics
Woman
Children
Ingenious peoples
People w/ disabilities
Identify as LQBT
How many homicides every year is committed by a family member in Canada?
172
How many victims of violence crimes is the person responsible a family member in Canada?
Approx 85,000
How many Canadians say they have experienced abuse before the age of 15 y.o?
1/3 or under 9 million
How many Canadians say they have experienced unhealthy spousal conflict, abuse or violence in the pas t5 years?
760,000
Challenges of Gathering Stats on IPV in Canada?
Reluctant to talk about family violence
Fear of their safety or children’s safety
Depend on family member who was abusive or violent
Feel shame, blame or denial
Think no one will believe them, be blamed or judged or will be arrested
Don’t want anyone to know (it’s a personal matter)
Addressed it through other means
Felt it was minor or not important enough
IPV During Pregnancy
Fatal outcomes
homocide
suicide
Non fatal outcomes
Negative health behaviour
Alcohol & drug abuse during pregnancy
Smoking during pregnancy
Delyared pernatal care
Reproductive health
low birth weight
Pre-term labour & delivery
Insufficient weight gain
OB complications
STI/HIV’s
miscarriage
Physical & mental health
Injury
Physical impairment
physical symptoms
depression
lack of or difficulty with attachment to child
Screening for IPV
Should be screened during routine prenatal care & during hospital setting
Hospital should imbed questions about abuse in healthy history or incorporate validated screening instruments into history/assessment process
Screening should be universal: ask every person over a specific age about experiences of abuse if in a safe enviroment
Routine screening performed on regular basis
Indicator-based screening if nurse observes indicators of abuse
HCP Response to Disclosure of Abuse
Acknowledge their abuse
Validate the experience
Assess immediate safety
Explore options
Refer to support services w/ person’s consent
Document interaction
Child protection if children is involve
Risk perception in women with high-risk pregnancies
Risk perceptions is shaped by individual experiences & social constructs
Risk perceptions affects decision people make about antenatal care so it can influence well-being of mother & family
Pregnant people focus on doing research during their pregnancy to make decisions about birth. They use multiple sources of information to determine risk including advice from professional & other trusted sources & their own intuitive knowledge
Can also increase doubt on health of pregnancy & can lead to overreliance on expert opinions
If women recognize the risk posed to their pregnancy, steps can be take to ensure health of themselves & baby
Women’s perceptions of risk & the care they will accept are dependent on the context of their individual circumstances
Core principles of Perinatal care to Overcome Risk
Person centered & family centered care
Individualized care
Kindness, respect & dignity
Care is informative, respecting person's learning style, knowledge & cultural tradition
Care is collaborative: informed-decisions, made in partnership with HCP
Tradition African Birth in South Africa
Take place in supportive & secure environment often grandmother’s home
Surrounded by people she trust
Ancestral spirits protect her here
Free from polluting contacts such as mensurating women
Move to rural to urban
Not in traditional environment but rather hospital
Traditionally woman are encouraged to remain ambulant & active in 1st stage while in hospital encouraged to rest
Go from lots of social support to few
Traditional to exclude husband
Pregnancy & Birth Related CUstoms among Indian Womem
Have 11 sanskara (sacraments) governing conception, pregnancy, birth & early infancy
Believe conception involved mingling of substances from both parents
Fetus is believed to be nourished by blood transfusion from mother via fontanelle & though umbilical cord develops in last month of pregnancy
Too much food is seen as harmful
“Cooling” or “windy” foods are believed to threaten fetus
Remain tranquil during pregnancy
Supposititious beliefs are common & everyday objects can be viewed as omens
Return to mother’s house a month before birth & isolate
Mother & experience friends/family members tend to pregnant women
Experiences of High- Risk Pregnancy
Range of emotional & psychological experiences
overwhelmed by diagnosis, hospitalization & aftermath of pregnancy
Individuals measure themselves against societal norms of how an pregnancy is supposed to be
Isolation & loneliness from family & community when hospitalized & separation from baby who requires NICU or close monitoring
Fear, guilt, frustration, anxiety, sadness & grief of loss of an idealized, healthy baby
Diagnosis of high risk can impact mother post-partum into depression, PTSD, suicide, & other psychological health issue
Experiences are influenced by
Negative experiences of high risk experience throughout the pregnancy & reult in a “traumatic birth”
Poor quality care & negative attitudes of HCP
Incidence of High-risk Pregnancy & Birth experiences has Been Increasing over Past 2-3 Decades
Mean age of childbearing has been increasing
Current medical interventions are able to support women w/ complex health issues through pregnancy & childbirth
Interventions for newborn & child with congenital & chronic conditions are more effective = new population of adults experiencing high risk childbearing experiences
This effect increases the chance of a pregnancy being complicated by coincidental medical conditions and increases the risk that such conditions can impact on women’s health and merit intervention
Bed Rest & Pregnancy COmplications
Bed rest is not supported as an intervention for most pregnancy complications
Results in loss of bone & muscle mass = requires PT exercise to offset as much loss as possible
May be stressful for person, partner, & family
Patient will need help w/ coping w/ isolation, boredom, stress & worry
May take place in hospital or a home
Objects of Prenatal Care Following an Antenatal Diagnosis of a Pregnancy Complication
First visit = Confirming diagnosis of pregnancy & beginning process of obtaining health Hx to act as a basis for ongoing prenatal care
Objectives
Prevention of complication or modification of those complications that may develop
Support to meet woman’s goal to maintain pregnancy to term while meeting best health potential for mother & baby
Providing education to parents & family for the parenting role w/in context of health risk being faced
Inclusion of family to support “family-centered care”
Patient education & birth planning for high-risk pregnancy
(Questions)
How does the effect on the pregnancy or newborn health vary that of a low risk or uncomplicated pregnancy?
What is the prognosis for the mother & baby
What is the level of knowledge & understanding on the part of the expectant mother, partner & family of current health issue & potential ramifications of the birth experience?
Was the pregnancy or newborn complication anticipated pre-conceptually or is it new?
How is the current and or anticipated experience different from the envision experience?
What values, hopes & goals are held onto?
What fears & challenges are currently being experienced? What might be helpful to overcome these?
Trauma & Perinatal Health
Sources of trauma
adverse childhood experiences
IPV
Birth trauma
Sexual abuse or assault
previous perinatal loss
Mental health
Trauma increases risk of perinatal depression, anxiety, preterm labour, LBW, & infant morbidity
Pregnant women & infants are among the most vulnerable to lifelong intergenerational ramifications of trauma
Tokophobia
extreme fear of childbirth
often a result of previous trauma such as birth trauma or sexual abuse
Parents will often oft for a c-section
Trauma Informed Care 4 Rs
Realization/develop awareness of the widespread impact of trauma on general and perinatal health
Reflect on how to respond by ensuring & enabling safe care environments that acknowledge, validate, empower, build trust & invite & facilitate opportunities to have healing conversations
Recognition of signs that a patients has been triggered while receiving care and respond within timely manner
Communication that is relational & patient-centered
Anticipatory care planning for complications or trauma
Resources that help nurses to respond by providing trauma informed nursing care
Institutional care cultures for trauma-informed care & provide education & generate policies
Resisting re-traumatization
All concepts focus on safety, control & choice
Pregnancy & Substance Use Nursing Implications
All substances alcohol, tobacco, benzos, marijuana, opiates can cross the placenta and impact the fetus
Harm reduction approach = opiate agonist (methadone or buprenorphine)
Often baby is motivation to change
Stigma, fear, trauma & mental health concerns are major barriers to maternal engagement w/ care
Prejudice & judgement from HCP, internalized stigma, and estrangement to families lead to isolation, late access to care, fear to disclose substance use, vulnerability & not meeting potential
Legal concerns: implications related to parenting & custody when baby is born
All women who use or don’t use substances all share the same aspirations & dreams. The only difference is women with substance use have more obstacles standing in their way to realize and achieve these aspirations
Breastfeeding is supported & encouraged for babies experiencing neonatal abstinence syndrome or opiate withdrawal
Impacts of Substance use in pregnancy (mom, fetus, neonate)
Mom: pregnancy loss, preterm labor, HTN, blood coagulation problems, placental abruption,
Fetus: fetal grown restriction, intrauterine death, congenital defects, & developmental issues
Neonate: Neuro behaviours symptoms (tremors, extreme irritability, inconsole cry, inability to self-soother, poor sleep, hypothermia), seizures, GI & respiratory issues
Contributing Factors to Substance Use in Pregnancy
Hx of drug addiction, chronic pain
Hx of psychological, physical or sexual trauma
Hx of mental illness
SDOH
Substance Use & Impacts on Baby
Opioids use such as morphine, dilaudid fentanyl, methadone & buprenorphine result in neonatal abstinence syndrome
Buprenorphine appears to have less withdrawal symptoms that methadone but not always best choice for recovery
Cannabis, Benzodiazepines, antidepressants/SSRI’s, nicotine & caffeine may cause withdrawal symptoms but neuro effects are different
Cocaine & other stimulants can cause withdrawal but do not impact neurological effect
Alcohol doesn’t cause withdrawal symptoms but can cause congenital health issues
Neonatal Abstinence Syndrome Symptoms
Central Nervous System:
inconsolable high-pitch crying
disorganized sleep
irritability
hyperactivity deep tendon reflex
tremors
hypertonia
restlessness
seizure
Gastro
poor feeding
frantic sucking
regurgitation
projectile vomit
loose & watery stools
Autonomic dysregulation
sweating
temp
yawning
mottling
nasal stuffiness
sneezing
tachypnea
Neonatal Abstinence Syndrome Care & Management
Baby & mom cared together
skin-to-skin & kangaroo
swaddling & soothers
Do not require NICU unless other health issues requiring admission b/c it is a loud and active environment
Infant assessment & scoring for risk of signs/symptoms should be done in collab with famil
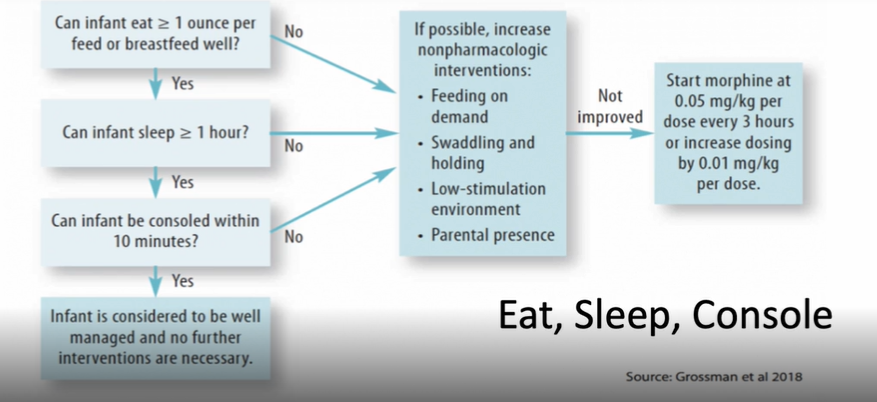
Eat, Sleep, Console Tool
Infant with NAS is regularly assessed and determined if pharmacologic treatment is required
Can infant eat >/= 1 ounce per feed or breastfeed well?
Can infant sleep >/= 1 hour?
Can infant be consoled within 10 minutes?
If all answers are yes than Infant is considered to be well managed & no further intervention needed
If any answer is no try nonpharm approach
Feeding on demand
Swaddling & holding
Low-stim enviroments
parental presence
If nonpharm don’t work start morphine @ 0.05 mg/kg per dose every 3 hrs or increase by 0.01mg/kg per dose
Medications for Neonatal Abstinence Syndrome (NAS)
A narcotic is used to control withdrawal symptoms
They are not “addicted” but physically dependent on medication
Short-acting opiated are used w/ babies to mediate symptoms & slowly withdraw them from narcotics
Typically morphine is used
Clonidine = decrease autonomic symptoms
Phenobarbital is rare but used when scores are not stabilizing & when weaning from meds is not going well
Buprenorphine is being explored as a med to assist with NAS
Breast-feeding with Neonatal Abstinence Syndrome
Baby’s withdrawal scores tend to be less w/ breastfeeding
unknown if r/t skin-to-skin or small amount of drugs in milk or both
Mothers should be in encouraged to join recovery program to breastfeed
There is concerns of breastfeeding while still on street drugs but it shouldn’t be forced to stop
Breastfeeding is affirming to mother & evidence shows it supports & aids recovery
Pregnancy & Psychiatric Medication Nursing Implications
Important to treat mental health concerns during pregnancy
Not uncommon for mental health problems to initially manifest & be diagnosed during pregnancy
Perinatal consequences of untreated mental illness in pregnancy
High risk for abortions
Broken families & homes
Partner problems
Exacerbated stress
Unstable work life balance
Other physiological co-morbid health conditions
Depression, anxiety & PTSD often need increased support & intervention in pregnancy
Approach to care should be trauma informed, relational, strength-based & patient centered
Management Approachs for Mental Health in Pregnancy
Screening, psychosocial assessment & support
Ideally initial screening occur in pre-conceptual
Psychological interventions
Pharmacological interventions
Weigh risk-benefits to mother & fetus
Doses are often adjusted
SSRI’s are most commonly prescribed antidepressant in pregnancy
Relatively safety but can mimics neural behavioral neonatal symptoms seen in neonatal abstinence syndrome
So do not assume mother uses substances, do an indepth hx
Obesity Risk of Complications in Pregnancy
Prenatal
Gestational diabetes
PIH
Pre-eclampsia
Miscarriage
Preterm labour/birth
UTI
Decreased sensitivity of ultrasound
Difficulty with FHR Monitoring
OSA
Intrapartum
Prolonged labour
Operative interventions
Perineal trauma
Hemorrhage
Anesthesia problems
Decreased sensitivity of ultrasound
FHR monitoring problems
Postpartum
Postpartum hemorrhage
Wound infection
Endometritis
Venous thromboembolism
Decreased breastfeeding rates
Fetal/Newborn
Congenital abnormalities
birth injury
shoulder dystocia
macrosomia/LGA
hypoglycemia
Fetal/neonatal demise
Neural tube defect
child/adult obesity
childhood/adult obesity-long term
Long-term Comorbidities (maternal)
Type II diabetes
HTN
Liver disease
CAD
Ischemic stroke
Cancer (colon, endometrium & breast)
osteoarthritis
Perinatal Obesity Management
Grounded in biomedical notions of disease causation & idea that weight is within the individuals control
Precludes the SDOH upon which obesity is predicted
Obese pregnant women are often stigmatized & marginalized = poor access to care and contributes to poor maternal/birthing experience
Instead we should focus our care on being person-centered, trauma-informed, relational, strength-based & SDOH informed
Chronic HTN in Pregnancy
HTN of any cause periconceptually or before 20 weeks gestation
Gestational HTN
New onset HTN that develops in a previously normotensive woman after 20 weeks gestations w/o proteinuria
Preeclampsia & eclampsia
New onset HTN after 20 weeks gestation w/
new onset proteinuria
Or in absence of proteinuria signs of multisystem involvement such as thrombocytopenia
Preeclampsia progresses to eclampsia if seizures occur
HELLP Syndrome
Hemolysis of RBC’s
Elevated Liver enzymes
Low Platelets
Multiorgan/system syndrome that can occur in severe preeclampsia or hepatic/liver involvement
Chronic HTN w/ Superimposed Preeclamps
Preeclampsia develops in woman w/ chronic HTN
Preeclampsia risk factors
Pregnancy related
nullipariy
personal or family hx
multifetal gestation
IVF
Pre-existing risk factors
Advance maternal age
Preexisting medical condition
Chronic HTN
Chronic renal disease
Thrombiphilia
Diabetes
Autoimmune disorder
Obesity
Antiphospholipid antibodies
Pree-clampsia Interventions/Treatment
Delivery is the cure
Determine optimal timing of delivery
At or beyond 37 weeks gestation
Between 34-37 weeks if preeclampsia has severe features
Between 20-34 weeks preeclampsia with severe features is ideally managed in a facility with maternal & neonatal intensive care resources
Pharmacological treatment
Stabilize BP 140-150/90-100 mmHg
Labetalol = first line for
Adalat or Nifedipine = second line
Magnesium sulfate for seizure prophylaxis
Nursing Care Preclampsia
Screen approparaitely
Identify warning signs: severe headache, RUQ epigastric pain, nausea, visual changes, difficulty breathing & swelling in face or hands
Ensure accurate BP measurement: proper position, cuff size & device
Changes in body weight: more than 3-5 Ibs per week = suggestive of fluid retention
Observe for other signs: reduced UO, edema & pulmonary edema, suggest preeclampsia associated fluid imbalance
Especially in second half of pregnancy
Preterm Labor
<37 weeks
Regular uterine contractions aren’t always detectable & present as back ache
S&s
PROM
Cervical dilation > 2 cm
Effacement exceeding 50%
change in cervical dilation or effacement detected by serial examinations
Preterm Labour Risk Factors
Medical
HTN
Preeclampsia
Thrombophilia
Connective tissue disorder
Diabetes
Intrahepatic cholestatis of pregnancy
Demographic
Maternal age
low socioeconomic
low education
Lifestyle
Alcohol/substance use
smoking
Domestic violence
no social supports
Stress
Occupational hazard
Signs of Preterm Labour
Uterine contractions w/ or w/o pain or discomfort
Feels like fetus is balling up every now & then
Abdominal or intestinal caramping w/o diarrhea
Pelvic pressure, low backache = dull
Menstrual-like cramping
change in discharge
Interventions to Prevent Preterm Labour
Management of exisitng medical comorbidites/conditions
Lifestyle modification
smoking cessation
Promotion of early & regular access to prenatal care
Routine screeining & treatment for bacteriuria
Teach all women on risk of pre-term birth & symptoms of preterm labour
Early identification ensures prevention of preterm birth
timely transfer to facility
tocolytic administration to postpone labour
antibiotic admin for prophylaxis against infection (Group B strep)
Corticosteroid admin to enhance fetal lung maturity
Magnesium sulphate admin for neuroprotection
Fetal Fibronectin Test
Fetal fibronectin is a fibronectin protein produced by fetal cells between chorion & decidua
Is adhesive that binds fetal sac to uterine lining
Vaginal swab down when preterm labour is suspected & done routinely between 22-34 weeks of gestation
Positive test = glue has been disturbed & risk of premature birth within seven days
Birth isn’t certain if positive
Is only predicator of birth & assist with decisions to transport/medical therapy
Tocolytics for Preterm labour
Medications affects uterine muscle conductivity to slow/stop preterm labour contractions
Not given to women as risk or is having imminent preterm birth
Nifedipine: calcium channel blocker; used in women less than 34 weeks gestation. Effects cardiac, vascular & nonvascular SM in addition to uterus. Requires close nursing observation & assessment
Indomethacin: NSAID; inhibits production of prostaglandins which influence onset & maintained of labour. Used for pregnancies less than 32 weeks gestation. Can be associated w/ effects on fetus after 32 weeks if used longer than 48 hours (premature closure of ducuts arteriosus & oligohydramnios)
Risk benefit should be used to determine use of meds
maternal mortality ratio (MMR)
ratio of pregnancy related deaths per 100,000 lie births
Maternal death is defined as death of woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration & site of pregnancy from any cause r/t to or aggravated by the pregnancy or its management but not from accidental or incidental causes
Main indicator of country’s health
severe maternal mobidity
conditions that are along side the continuum to maternal death, including life-threatening & disabling disease, organ dysfunction & or receipt of invasive therapy during pregnancy or within 42 days after birth
Canadian & USA Maternal Morbidity & Mortality Rates
are on the rise
Canada is underreporting their MRR
Based on WHO Canada has 3rd highest MRR
Post-partum care canada
Average length of hospital stay is 2 days after vaginal birth & 3.4 days after c-section
Postpartum care is component of maternity care that is most negatively perceived by mothers
Concerns often r/t need for inpatient care to be more person centered & flexible
Strategies to Improve Maternal Morbidity & Mortality Rates during Post-partum period
Improve standard postpartum discharge education
pain in chest
obstructed breathing or SOB
Seizures
Thoughts of hurting yourself or infant
Bleeding
Incisions that aren’t healing
Red or swollen leg that is painful or warm to touch
Temp >100.4
Headache that won’t go away or w/ vision changes
Enhance timing of postpartum care services
woman normally don’t see a doctor for 6 weeks postpartum (vaginal) or 4 weeks postpartum (c-section)
woman with high-risk concerns of pregnancies should be followed up earlier
post-partum services end 42 days post birth, but not all woman are full recovered
Improve quality of postpartum care
standardization of comprehensive assessment of physical, social & psychological well-being as well as reassessment of nonpregnancy or pre-pregnancy related health
Standardization of patient education
Women report wanting education of birth control, physical activity, sexuality, nutrition, depression, infant feeding, water retention & future complications during postpartum appointments
Enhance social & Mental health support
Reducing postoperative complications by decreasing rates of c-sections
Expand public health policies, advocacy & education outside the obstetrical realm
Indigenous Woman Disparities in Perinatal Care
2x higher risk of maternal mortality than general pop. & have higher rates of adverse outcomes
Trans-generational effects of trauma of colonization contributes to many of inequities in health and well-being
Negative experiences involved woman experiencing racism, cultural insensitivity & limited control over their care
Maternal & infant health outcomes are affected by socio-cultural & socio-economic status of Indigenous people
smoking & alcohol consumption during pregnancy
Chronic illness such as diabetes
Presence of hazardous environmental contaminants
Attachment theory
infant attachment is relationship between child & caregiver & is grounded in safety, security & protection
Child uses caregiver as a secure base to explore & as a source of comfort & safety
Maternal-infant relationships
Bonding: the initial emotional connection between birth parent & newborn; starts postnatally
Maternal-fetal attachment: relationship that develops during initial years of life; starts in prenatal period
Maternal mental health in Canada Statistics
23% of mother who recently gave birth in Canada reported feelings consistent with either post-partum depression or an anxiety disorder
31% in Nova Scotia
Neonatal Death vs Fetal Death
neonatal death: newborn - 28 days of life
fetal death: >/= 20 weeks gestation
miscarriage: < 20 weeks gestation