Rhumatology Exam 1 - RA, PsA, Lupus, Bjorn's dx, Fibromyalgia
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
16 Terms
fibromyalgia stx’s include
-widespread pain
-specific trigger points
-poor sleep, feel tired
-20-50 y/o
what are associated stx’s of fibromyalgia?
TIME PS H RNR or FIBRO (Fatigue, Insomnia, Blues, Rigidity, Ow)
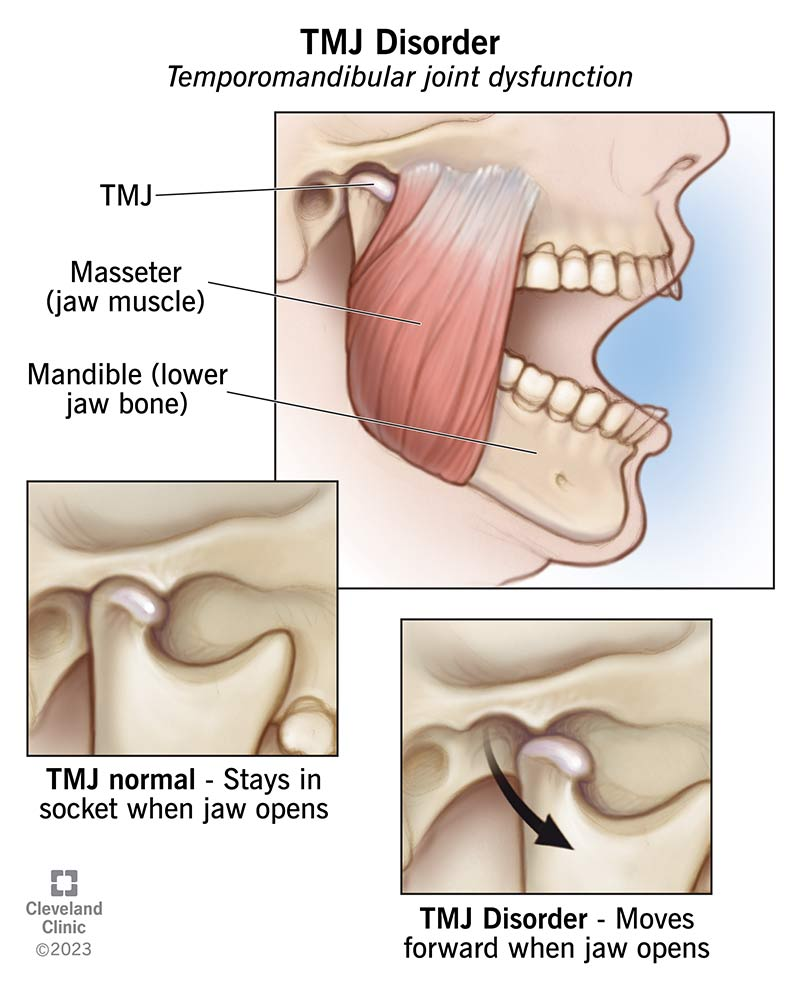
-Temporomandibular joint stx’s
-IBS
-Morning stiffness
-Exercise intolerance (musc. decond.)
-Psyc (anxiety, depression)
-Sicca stx’s (Sjogren’s; dry mouth and dry eyes)
-H/a
-RLS
-Non-cardiac chest pain
-Raynaud’s
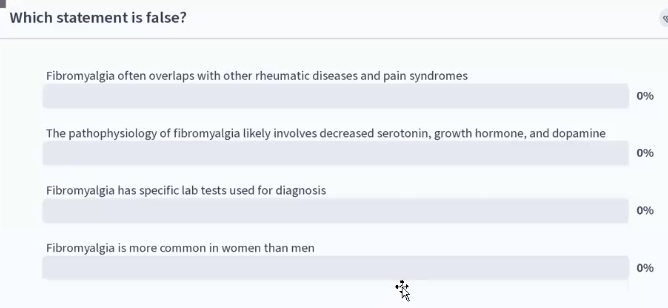
fibromyalgia overlaps with what disease states?
-chronic fatigue syndrome
-IBS
-chronic pelvic pain syndrome/primary dysmenorrhea
-migraine/tension HA
-PTSD
-RLS
-mood anxiety dx’s
-inflammatory disorders: RA, SLE
Describe how HPA Axis dysfxn relates to fibromyalgia with the dec. in 3 hormones
dec. in growth hormone → dec. tissue repair → dec. O2, Mg, ATP, PO4 → dec. fuel for body (eg dec. Mg = musc. aches)
DA → dec. limbic fxn → dec. cortisol → dec. body repair
5-HT → dec. sleep, inc. pain sensitivity → dec. cortisol → dec. body repair
peripheral mech. of fibromyalgia is via activation of what and via what kind of mito. damage?
-activation of chronic sympathetic → delta sleep disruption → musc. blood flow microconstrictions ,elevated IL-6, TNF, elevated substance P
-mito. damage from toxins → preoxidative rxns = inc. lactic acid
What are the 3 fibromyalgia diagnostic criteria?
widespread pain index (WPI) >/ 7 and stx severity (SS) score >/5 OR WPI 3-6 and SS >/9
Symptoms present at a similar lvl for < 3 mo.’s
pt does not have disorder that would explain pain
What are the updated ACTTION-APS Pain Taxonomy 3 diag. criteria?
multisite pain = 6 or more pain sites out of 9
moderate to severe sleep problem OR fatigue
multistate pain + fatigue sleep problems present for > 3 mo’s
ANS: C
There is NO specific lab tests used for diagnosis
Tx approach to fibromyalgia
no cure, thus:
pain management → pharma agents
(1st line: TCA amitryptyline 10-50mg/daily [AE’s: sedation, constipation, wt gain] [take 1 hr before bed]
SSRI: citalopram (2nd line), fluoxetine 20-80mg PO hs (dec. in fibro-fog, sleep and fatigue)
SNRI: duloxetine (Cymbarfa) [FDA approved for FM] [good for OA too] : dec. pain, dry mouth, nausea, constipation
NSRI: Milnacipran (Savella) [FDA approved for FM] (AE: insomnia)
CCB’s [co-morbid periph. neruopathy, h/a’s]:
Pregabalin (Lyrica): [approved drug for FM in US] (pregabalin > gabapentin)
Gabapentin
musc. relaxant: Cyclobenzaprine (Flexeril): dec. pain and inc. delta sleep [AE’s: EXTREME drowsiness]
DA Agonists [w/ co-morbid RLS]:
pramipexole (Mirapex)
Ropinirole (Requip)
low dose naltrexone
if pts fail:
venlafaxine (Effexor)
Buproprion (Wellbutrin) [smoking cessation]
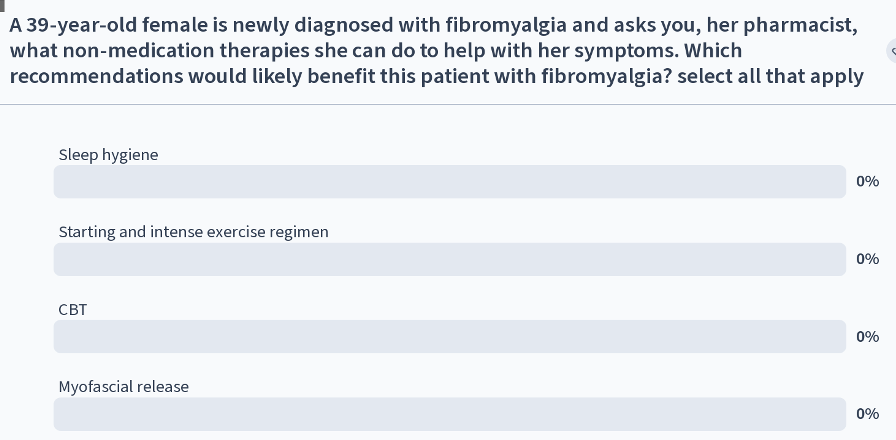
sleep management → education on good sleep hygiene, aerobic exercise (water aerobics)
psychological support → counseling, support groups, CBT
complementary options → massage, acupuncture, biofeedback, myofascial release
Treatment guidelines
APS (American Pain Society) 2004
EULAR (European League Against Rheumatism) 2007
What pharma Tx’s to avoid in Fibromyalgia?
NSAIDs and CS’s: ineffective in FM
opioids: worsen FM stx’s (AVOID)
tramadol (an cause serotonin syndrome
lidocaine transdermal patches (not effective)
alternative meds for FM
Melatonin
Magnesium = FM dec. Mg lvls (pulls water into gut → diarrhea)
capsaicin (applied multiple times per day)
medical cannabis
how to choose pharma Tx for FM based on other co-morbidities?
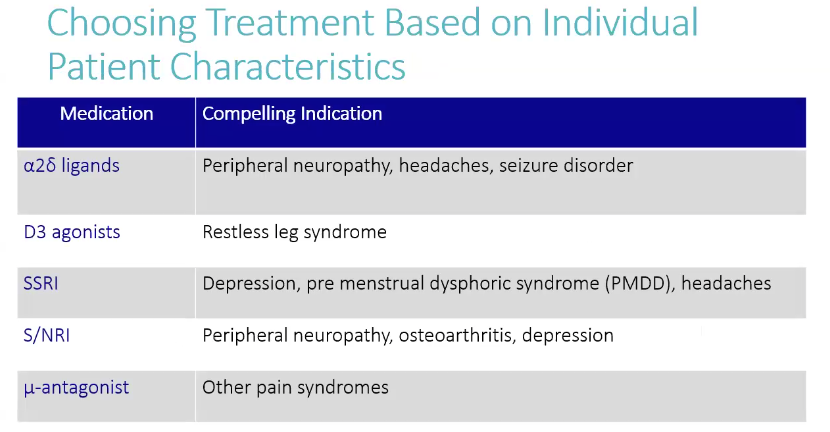
A, C, D
A.
milnacipran = can cause insomnia
B (bc FDA approved & periph. neuropathy 2ndary to diabetes)