Derm Oncology 1
1/62
Earn XP
Description and Tags
Know and understand the behaviour most common skin and subcutaneous tumour types • Understand the clinical effects of cutaneous and subcutaneous tumours • Describe general approach including staging, treatment, and prognosis (particularly mast cell tumours)
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
63 Terms
tumour in dogs3
most common species to have tumour
1/3 of all neoplasm
most is benign (60-80%)
tumour in cats 3
2nd most common species to have tumour
¼ of all neoplasm
most is malignant (65%)
primary or metastasis common in cutaneous tumour?
name 2 presentation associated with metastasis
mostly primary
but occasionally metastatitc leision
multiple cutaneous metastasis
lung-digit syndrome
digital and cutaneous metastasis
associated with lung cancer in cats
how are cutaneous tumour classified 3
Tissue of origin (epithelial, mesenchymal, vascular)
Cell of origin if possible (e.g. mast cell tumour, lmyphoma, histiocyte or melanocyte)
According to degree of malignancy
also look at the table in notes
see notes
most common skin tour in dog and cat
name top 3
dog
MCT, lipoms, hisyiocytoma
cat
basal cell tumour, mast cell tumor, SCC
cause of cutaneous/ subcutaneous tumour 6
UV radiation (esp sun and UVB—> SCC)
Chemical carcinogens
Irradiation
Physical agents + damage
Viruses (e.g. papillomas)
Inflammation (e.g. implicated in FISS)
during examination,
feature suggesting malignency 6
to consider 2
Rapid growth
Fixation
Invasion into overlying skin or deep tissues
Ulceration
Poorly defined margins
not all aggressive lesions show these features.
pseudocapsule formation: sarcomas seem well demarcated
Mast cell tumour can mimic lipoma (soft cutaneous or subcutaneous masses)
approach to diagnosing cutaneous/ subcutaneous tumour
FNA, cytology, biopsy
name FNA good and bad
useful for
when do you skip NFA and skip to biopsy
what else to do after FNA: gold standard
cutaneous and subcutaneous mass lesions
Superficial, ulcerated, very inflamed—> biopsy
Histology gold standard – Submit after resection
cytology
used for differentaiting 2 and can provide 1
note if inflammation is marked
neoplastic from inflammatory
malignant from benign
cells surrounded by inflammatory cells show changes impersonating malignancy
dysplastic vs neoplastic change
biopsy types and which one better
Small punch needle
may not be representative
Incisional biopsy (wedge)
good sample for histology
ncisional biopsy removes a portion of tumour for diagnostic purposes
The golden rules of incisional biopsy:7
Plan biopsy site
Sample selection: representative part of the lesion
Avoid major structures
Avoid necrotic, haemorrhagic or infected areas
Incision position
entire biopsy tract can be removed during subsequent sx
large incision
harvest without xs tissue manipulation
Minimise instrumental manipulation
Avoid diathermy, cryosurgery etc.
Include a portion of normal tissue only if easy to do
Ensure adequate fixation
Excisional biopsy widely used in skin tumor removal, then submission for histology.
indication 3
benign proliferative epithelial tumours
highly likelihood clinical diagnosis is correct + minimal margins required
knowledge of histogenesis of the mass will not change surgical dose
Clinical contraindications for excisional biopsy for cutaneous and subcutaneous masses 8
Rapidly growing mass
Ill-defined or poorly demarcated lesion
invaginate to underlying and overlying tissue
Peritumour oedema or erythema
ulceration
FISS
prev. FNA suspicious for MCT or STS
nost undiag —> sarcoma.
Non-diagnostic FNA
Staging of skin tumour 4
name what/ why would you do it
Proper recording of the primary mass
Measure tumour
photograph
identify the locationon body map
diagnose tumour via FNA, cytology, biopsy
FNA and examination of nodes
if enlarged
if suspicious or known malignant tumour/ MCT
Further diagnostics
indicated depending on pathology of lesion and evaluation
General treatment options for skin tumours
treatment of choice?
wb huge tumours? what if it is on extremety
incompletely excised tumour
name other treatment modality 4
Complete surgical excision is standard of care
Cytoreductive surgery; Amputation if on extremities
Radiation therapy for incompletely excised tumours
photodynamic therapy, cryosurgery, laser ablation and hyperthermia
epithelial tumours: name 6 possible epithelial cell ddx
most common?
Squamous cell carcinoma
Basal cell carcinoma
Perianal gland carcinoma
Sebaceous gland tumour
Sweat gland tumour
Tumours of hair follicles
what is SCC ?
prevalnece in cat ad dog
behaviour 1
in which site is SCC commonly seen in both cats and dogs?
Malignant tumour of squamous epithelium
15% of feline and 5% of canine cutaneous tumours
behaviour varies with site and species.
SCC is an important tumour in oral cavity of cat and dog.

canine papilloma
common in
caused by
progression 2
care with papilloma px
Young dogs
Viral (DNA papillomavirus)
Usually regress,but possible malignant transformation to SCC
usually immunosuppressed
feline SCC: prevalence
more common in
affected area
singl/ multiple leision?
older animals (median age 10–12 years)
nasal planum, pinnae, eyelids, and other head and neck sites.
30% multiple lesions at presentation
feline SCC: cause
what sepcial feature may cause hgiher SCC risk
caused by UV exposure from sunlight (UVB)
white hair coat 13x the risk of non-white cats : melanin protection
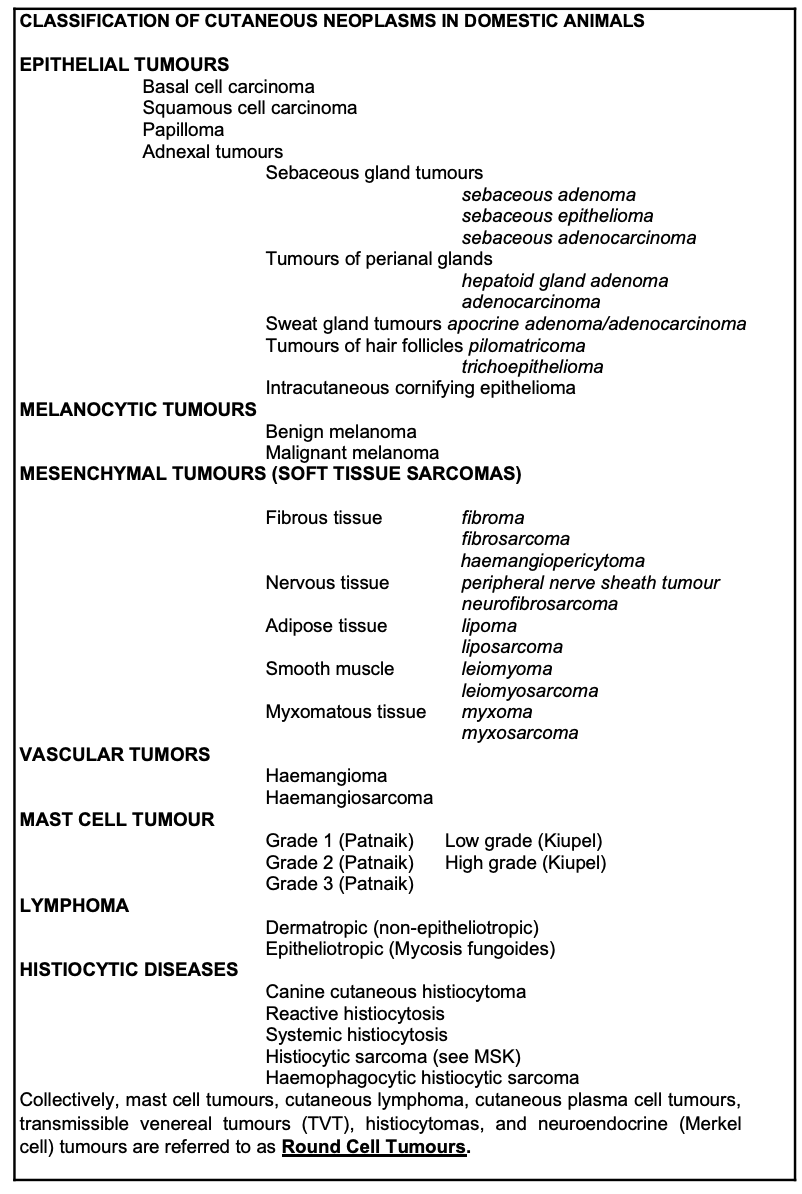
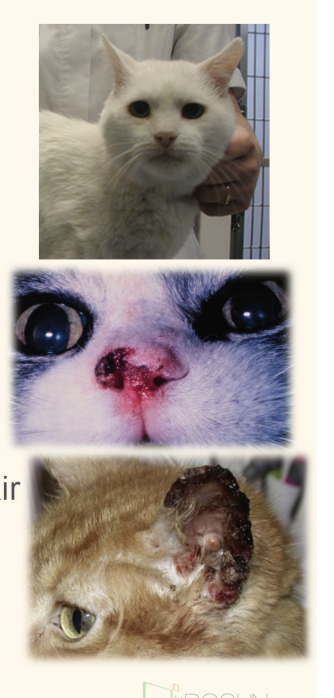
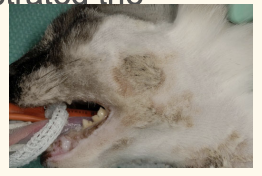
three stages in feline SCC development, give simple description
referring to the picutre
Actinic keratosis (a)
pre-cancerous
dysplasia due to chronic UV exposure
Carcinoma in situ (b)
have not penetrated basement membrane
Invasive SCC (c)
penetration of basement membrane
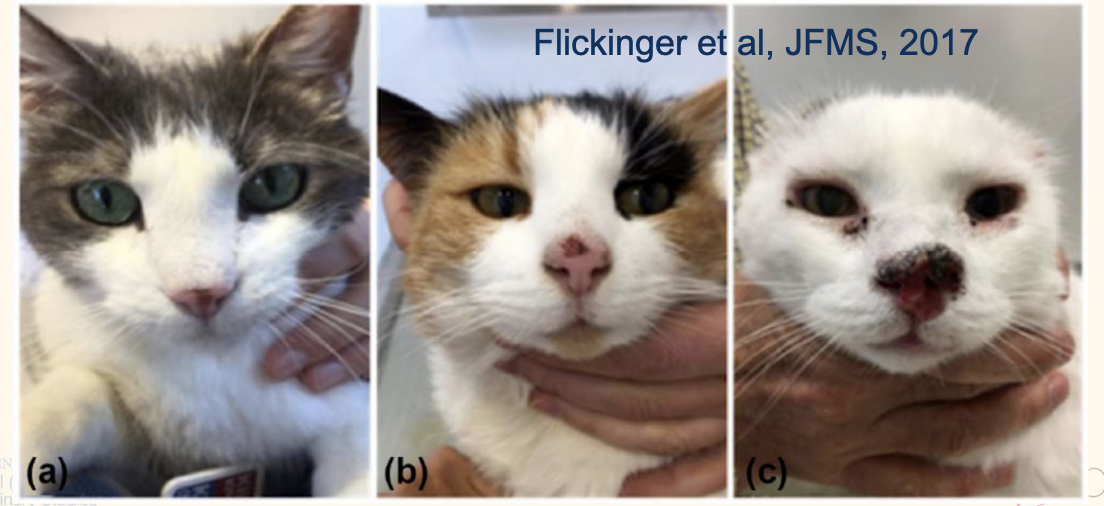
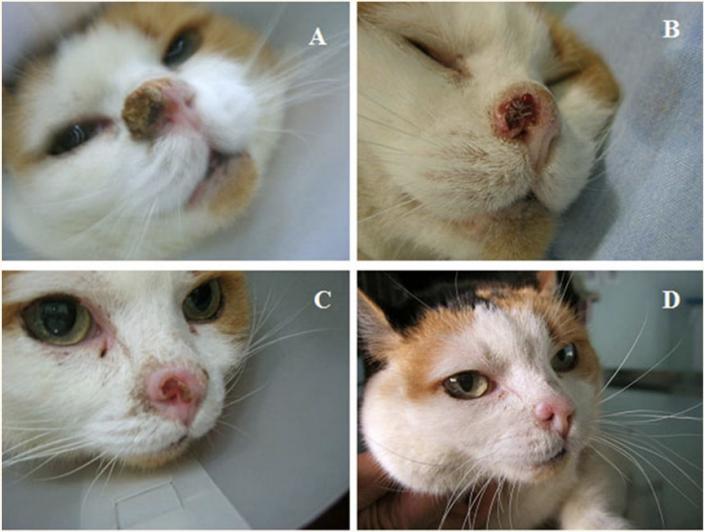
feline scc appearance and clinical presentation
appearance 4
any paraneoplastic syndrome?
variable appearance
plaque like
crusting and ulceration common
ucerated, crateriform or fungiform
associated fibrous tissue—> indurated (thickened or hardened)
hypercalcaemia rarely
feline SCC diagnosis
wich diagnostic method is preferrred?
what do you do if there is multiple affected area? what do you have to keep in mind when submitting sample?
FNA is unreliable, incisional biopsy is recommended
often multiple abnormal areas —sample all
some areas will be dysplastic/AK; others overt SCC.
label all the samples!
feline SCC: metastatic potential
metastasis ssociated with
name 2 location
associated with advanced disease
locoregional nodes first
progress to pulmonary metastases
feline SCC tx option 6
best approach other than early detectio
list the 2 type of radiotherapy
Surgical excision
Radiotherapy
direct beta radiation (strontium 90) control carcinoma insitu
external beam (orthovoltage) in early stage local control
Photodynamic therapy
Intralesional chemotherapy
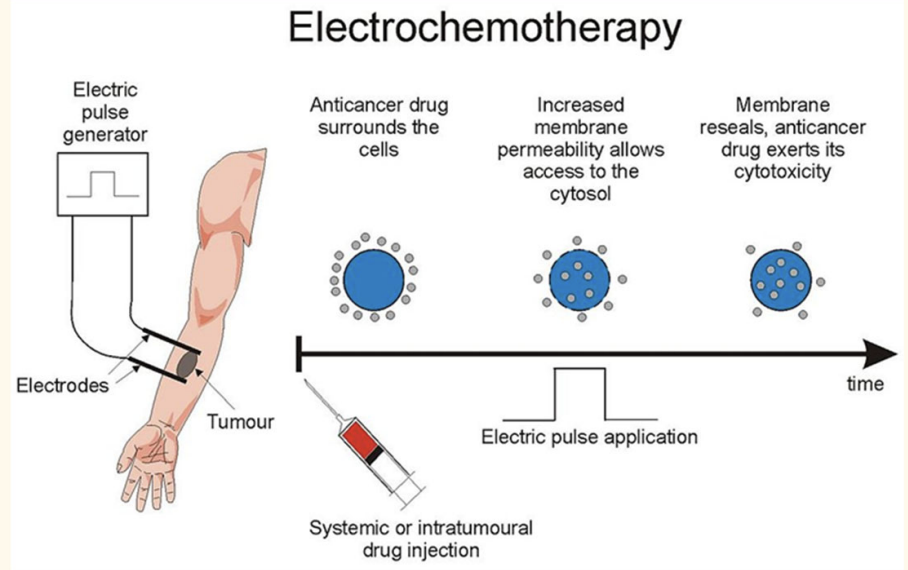
Electrochemotherapy
Topical imiquimod
Surgery:
what approach gives the best long-term control?
ear, nose, eyelid,
Wide surgical excision provides long term control: Pinnectomy, nosectomy etc
Pinnectomy— >1.5 years tumour control
nasal planum tumour —> good local control, but must achieve margins (refer)
Enbloc resection of lower eyelid tumours —> good control (refer)
most successful in smaller tumour
Feline SCC: Radiotherapy:
what is the 2 type of radiotherpay
name what kind of tumour you would use this on
name 1 feature of orthovoltage
name 3 advantage of strontium 90 plesiotherapy
external beam (teletherapy) or direct beam (brachytherapy)
external beam— orthovoltage
superficial, exophytic tumour <2cm
satge T1 better outcome than that of T3
Direct beam— strontium 90 plesiotherapy
supercifial SCC (<2mm in depth)
carcinoma insitu control, sparing of local normal tissue, repeatable
Feline SCC: Photodynamic therapy
what is it how do you do this?
what are the considerations if outdoor cat?
what kind of tumour does this work on
how long does it control?
Local or systemic administration of photosensitiser
Administration of light (appropriate wavelength) to activate the drug several hours later
reasonably well tolerated
Local adverse effects
keep cat away from bright light and indoors for two weeks
Small, non-invasive, early stage tumours only : control 5-35 months
Feline SCC: Photodynamic therapy
advantage 4
Non-invasive
does not require multiple GAs
Reasonable results with good case selection
can be repeated
Electrochemotherapy: feline scc
how is this achieved?
response rate? remission?
concern?
Intralesional or systemic bleomycin (good response rates)
High response rates but variable duration
depending on lcoation
priocular/ heaad and neck> nasal planum> cutneous
Possible significant local side effects
Feline SCC: cryotheraoy and carboplatin
cryo: what tumour can u use it on)
cryo response rate?
carboplantin response rate?
concern— hwy we dont use it
Cryotherapy
[Small (<2cm, superficial) tumours only]
Aggressive—>good local control of pinnae and eyelid.
nasal planum poorer response. o
Intralesional carboplatin
73% CR, 55% progression free @ 1y
Safety: major concern!
Prevention of feline SCC 3
name 1 approch that does not work
high riskers should avoid sunlight at height of day
UV light-blocking film for windows
outdoor cats: sunblock
avoid ingestion •
impossible to administer to the nasal planum without being licked off.
Tattooing does not decrease the incidence of SCC
name a form of cutaneous in-situ carcinoma (basement intact)
presenation 1
treatment of choice 1
name one pother treatment
what is its activity 3
name 5 side effects
Bowenoid carcinoma in situ
• multiple sites
Surgery treatment of choice
Imiquimod cream (aldara)
immunomodulator with antitumour and antiviral effects
local erythema, increased liver enzymes and neutropenia, hyporexia and vomiting
Canine SCC
prevalence
most common site3
association/ predisposing factor of sites 2
older dogs, median age 10–12 years
The most common sites and association
Nasal planum—(inflmamation?)
Nailbed (subungual)— large breed, dark hair coat
Ventrum — UV exposure
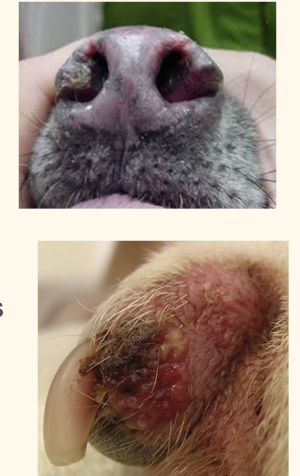
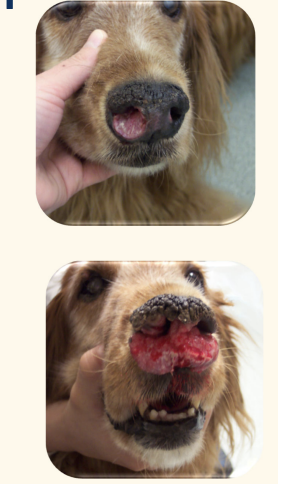
canine SCC: nasal planum presenation
treatment of choice
what about radiotherapy?
what if the owner does not want to do sx, and want to opt for short term palliative care?
prognosis?
More difficult to manage than in cats
Aggressive resection
poorly radiosensitive
combination of radiotherapy and intralesional chemotherapy
poor prognosis :(
canine Subungual SCC
why is staging important when you see subungual scc in dog
tx
what if it comes back after eh tx?
to rule out lymph node metastasis (common)
Treatment: sx, no adj therapy needed
ampute affected digit at the level of the MC/P, MT/P, or proximal IP level
limb amputation
melanocytic tumours arise from melanocyte at? 4
anywhere but most comonly
basal layer of the epidermis: cutaneous or dermal melanoma
epithelium of the gingiva: oral melanoma
nail bed: digital melanoma
ocular structures: iris etc
melanocytic tumour Predisposed breeds include 5
Standard and Miniature Schnauzers
Doberman
Scottish Terrier
Irish and Gordon Setters
Golden Retrievers
melacytoma vs melanoma
what is the main difference that inidcate malignancy of melanoma?
Benign – melanocytoma
hairy skin
Malignant – melanoma
oral, digital, subungual
Cutaneous/nailbed melanoma
malignant melanoma can be _____
spreading route: 2
early metastasis can be seen at
Malignant tumours may be AMELANOTIC
lymphatic and haematogenous routes.
regional LN or distant metastases—> staging!

Approach to melanocytic tumours— work up 3
History and clinical examination
Fine needle aspiration or biopsy
Staging (regional LNs, lungs +/- visceral organs)
Approach to melanocytic tumours— tx for benign cutaneous leision
Benign cutaneous lesions
(pigmented, located on haired skin, <2 cm in diameter, mitotic rate < 3/10 HPF)
complete excision surgery is curative
Approach to melanocytic tumours— tx for primary malignant tumour
Primary malignant tumours
removal of LN
complete radical surgical excision
margins of up to 3cm necessary
Nail Bed/ digital melanoma: Treatment
what is the standard treatemnt
what about radiotherapy
what else would you do other than sx?why? ( esp dog oral melanoma)
sx: amputation of the affected digit
all 3 phalanges to ensure adequate surgical margin
Limb amputation may be necessary to achieve an adequate margin
Draining lymph node(s) removed at the same time
radiotherapy
Sensitive to RT but irradiation of foot is challenging (toxicity to pads)
immunotherpy: delay/ prevent metastasis
tyrosinase – involved in melanin biosynthesis
intradermal vaccine
safe in cutaneous and nailbed tumours, but of unknown efficacy.
Feline cutaneous melanoma
malignancy compared to ocular or oral melanoma
treatment/ management?
Cutaneous melanoma uncommon
Less malignant than ocular or oral
Surgical management
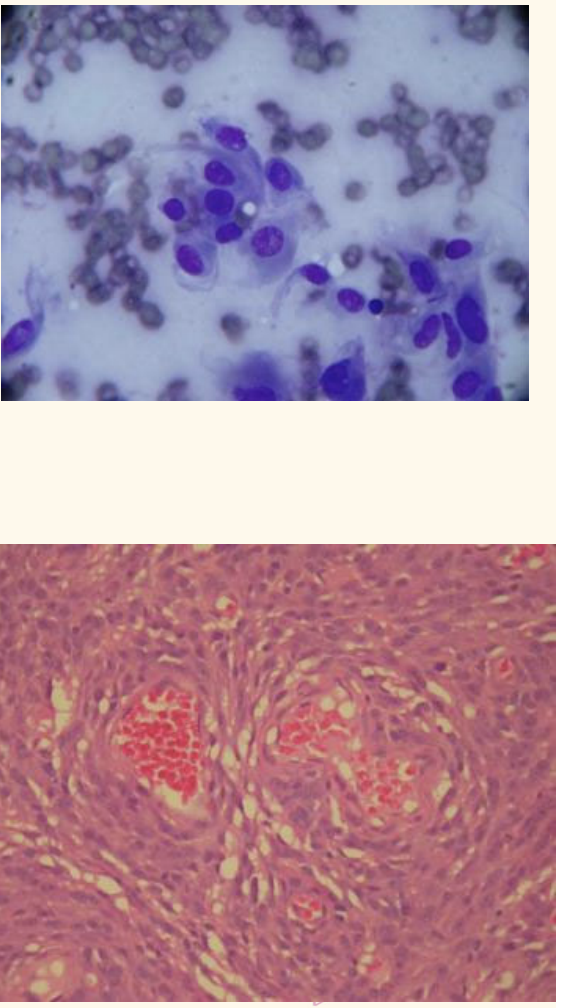
Soft tissue sarcomas
malignancy/ aggressiveness?
how do you confirm behaviour?
LN metastasis?
Infiltrative and locally aggressive
sx—> histopath to confirm complete excition and grade
predicts behaviors
Nodal metastases uncommon
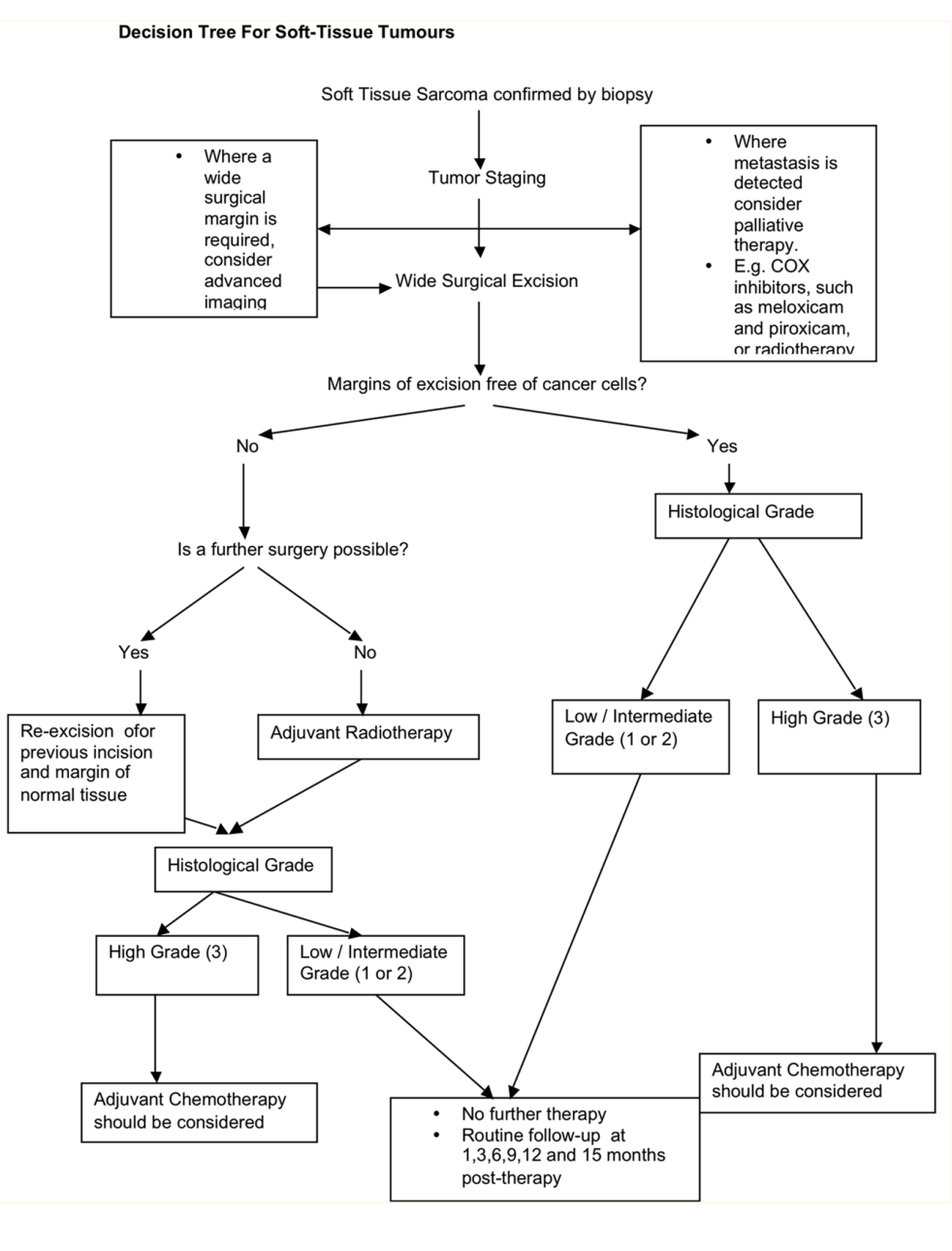
decision tree for STS
see notes
Feline Injection Site Sarcoma is associated with vaccine/ inflammation.
describe FISS
name a few vaccine 2
comon origin? name most comon type
characterised by____
recurrence rate?
how do you determine chances of metastatis?
chronic inflammation in a genetically predisposed cat
Rabies, FeLV vaccines
mesenchymal in origin – fibrosarcoma
Characterised by very aggressive local behaviour
High recurrence rates
10-20% meatstasis overall; 40-50% if histologically high grade
FISS latency period for tumour development
a few months to several year
Recommendations for vaccination: to avoid FISS 4
Avoid vaccinations in the interscapular space
Subcutaneous rather than intramuscular
Rabies/FeLV vaccines on the distal aspect of the right (rabies) and left (FeLV) pelvic limbs
vaccine only after strong consideration of patient’s exposure risk
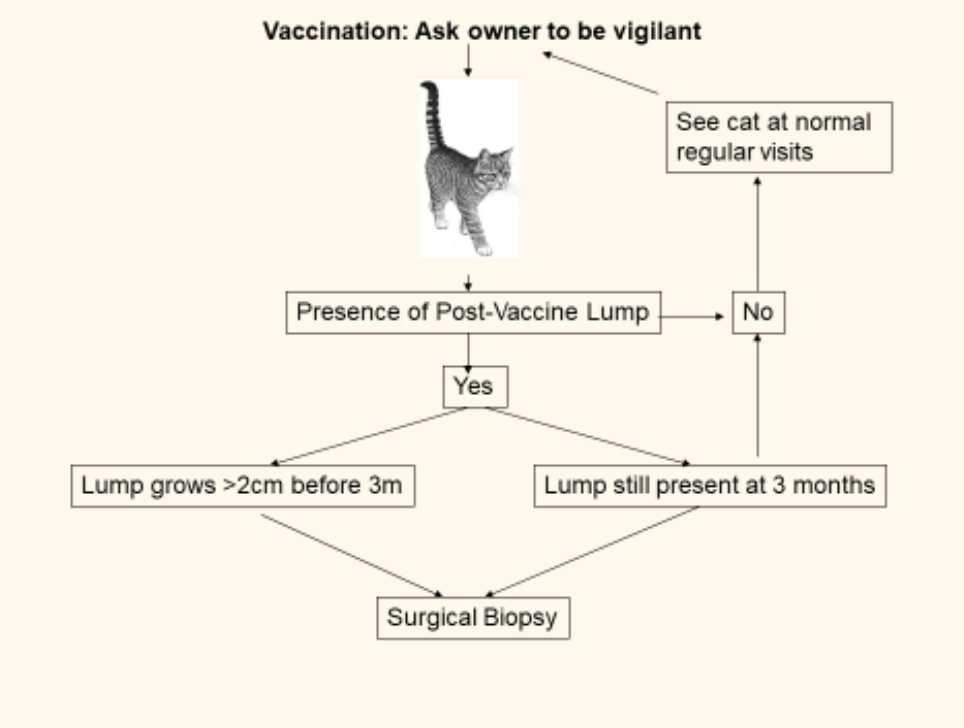
Approach to Suspected FISS
2 approaches to investigate fiss
name 2 disadvantage to FNA
incisional/ excisional biopsy?
wha would you do for sx plannign
Examination
firm cutaneous or subcutaneous mass
3-2-1 rule for investigation
present 3 months or longer
greater than 2 cm diameter
continues to increase in size 1 month posst injection
FNA: may not be diagnostic
Inflammatory component may be harvested
Sarcoma component may not exfoliate well
Incisional biopsy preferred
Excisional biopsy guarantees treatment failure
recurrence 66days,
extend tumor bed every resection
to plan sx: complete staging involving advanced imaging
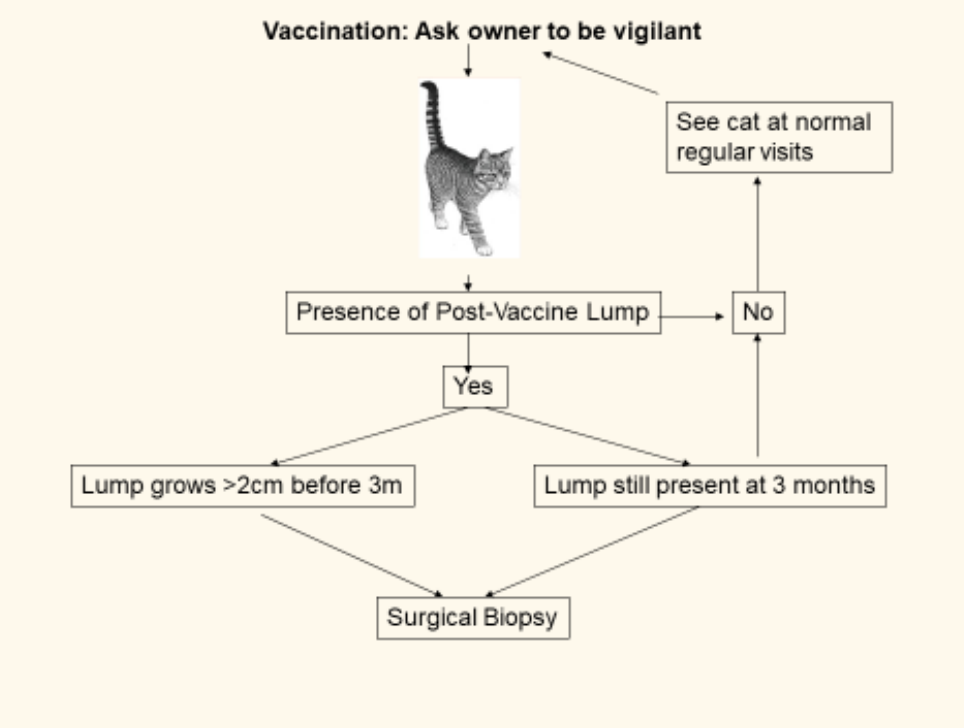
flowchart to FISS
Tx selection for local/ locoregional therapy
main challnege
main modalities 2
what else can be used post-op for local immmunotherapy?
Local disease control is the main challenge
surgery and radiotherapy are the main modalitie
Infiltration of IL-2 (local immunotherapy).
Tx selection for systemic therapy: FISS
role of post op chemotherpay 3
how else can u use chemo
role of medx is limites
post-operative chemotherapy in high grade tumour—uncertain.
Metronomic chemotherapy used instead of radiotherapy (but unproven) or in multimodal approach
FISS: sx
concerns
to do this properly
high recurrence rates, 66days
increase per repeat surgeries
greater if histologically margins unclear
RADICAL + 3 to 5 cm margins
normal tissue
multiple tissue planes, body wall
ostectomy as indicated.
FISS: Radiotherapy
mainly used pre/ post ogg?
benifits pf radiotherapy
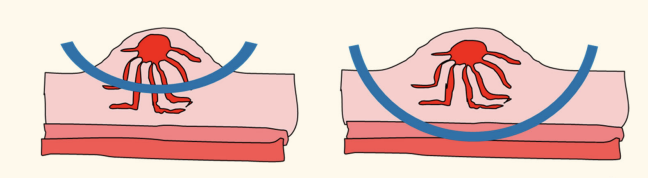
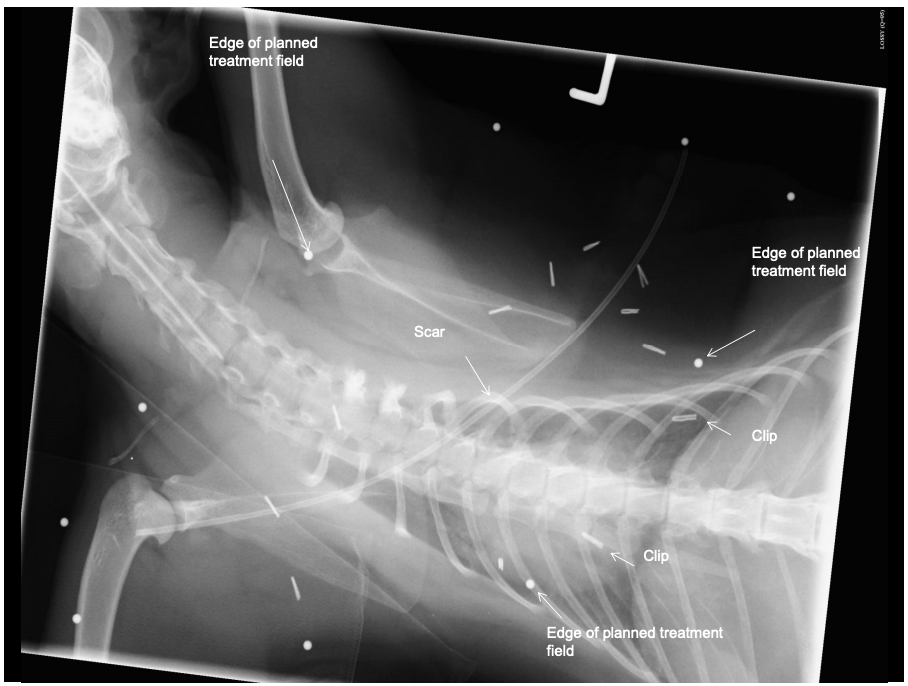
problem w post op radiation? 5
what couls improve survival but done less?
pre-op or post-operatively
benefit in delaying or preventing recurrence and increasing survival times
Problem with post-op radiation?
Not knowing where tumour was
Long and complex scars
post-op tissue migration (use surgical clips!)
Unable to identify microscopic disease in the gross cat
Important structures deep to tumour bed
Pre-operative radiation followed by radical surgical excision +/- post operative radiation
Round Cell Tumours of the Skin and Subcutis 3
Histiocytic tumours
Mast cell tumours
Lymphoma
Histiocytic skin leisions include:
list 3, from most benign to most malignant
and say what celll origin
give one extra one for extra point
Canine cutaneous histiocytoma
Arise from epidermal Langerhan dendritic cell – Benign
Reactive histiocytosis (cutaneous or systemic)
Arises from activated interstitial dendritic cell
Cutaneous involvement: histiocytic sarcoma
Arises from interstitial dendritic cell
(Haemophagocytic histiocytic sarcoma
macrophage lineage cell)
Canine cutaneous histiocytoma
prevelaence, age at pfresentation
breed predispose 4
14% of all skin tumours, young dogs (<3 years) mostly
Boxers, dachshunds, cocker spaniels and bull terriers
Canine cutaneous histiocytoma
clin presentation
progression
diagnostic— what do you expect to see
treatment of choice? if that doesnt work?
presentation:
raised, often hairless lesions
may grow rapidly
Cytology usually diagnostic,— pleomorphic round cells with a lymphoid infiltrate
may regress spontaneously
but if not, surgical excision and submit mass for histology.
Lipoma
2 situation when it is a concern
what malignancy can this be mixed up with? what makes it difficult to diff?
Benign tumour of adipocytes
infiltrating+ attach to muscle
—>Recurrence
Remember LIPOSARCOMA
hard to dx as dissolve in fixative
both fatty adipocytes look similar