Adult Health Exam 3
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
Why is delegation important in nursing?
Your State Board of Nursing Licensure requires it
State Nurse Practice Act
Nurses cannot do everything
Safe and competent patient care is complex
A team approach is needed
Interprofessional collaboration is essential to healthcare
Both the American Nurses Association (ANA) and the National Council for State Boards of Nursing (NCSBN) support nurses in using delegation safely and effectively
Delegation vs. Assigning
Delegation involves transferring authority to perform a task to another qualified individual
The person who delegates the task is still accountable
Assigning involves transferring the authority and the accountability of a task to another qualified individual
In each case, the individual chose must be appropriately trained to take on the task in question
5 Rights of Delegation

Delegation - Factors to Consider
Your role at work
Different facility policies
Your own personal experiences
Public misperceptions
Delegation - Members of the Team
RN
Is a licensed nurse
Program of completion varies but is ~ 120 hrs
Must pass the NCLEX- RN
License governed by State Board of Nursing
LPN
Is a licensed nurse
Program of completion varies but is ~ 60 hrs
Must pass the NCLEX- PN
License governed by State Board of Nursing
UAP
Is unlicensed
Some programs offer a certificate
Facilities can determine and offer required training
Delegation - Score of Practice: RN, LPN, UAP
RN
Initial assessment (admin, post-op)
Assessment of unstable clients
Admin IV push, blood products, TPN, and meds requiring titration/continuous monitoring
Access implanted devices
Interpret and analyze data requiring complex critical thinking
Care plan development
Initial and discharge teaching
LPN
Monitor RN findings and gather data (obtain BP, HR, etc)
Assessment of stable clients (focused and subsequent assessments)
Basic pt care (changing bandages, inserting catheters)
Report client status and concerns to RN/HCP
Care for stable clients with predictable outcomes (chronic, expected findings, ready for discharge, current labs)
Reinforce RN education
UAP
Assist client with ambulation, ROM< hygiene, and activities of daily living (ADLs)
Feeding and oral care for stable clients (not if risk of aspiration)
Record routine vital signs and I&Os (may measure UOP from indwelling catheter bag)
Positioning and linen change
Transfer/transport (to/form bed, chair, commode, stretcher)
Report client status and concerns to RN
Delegation - Facility Specific Training
Facilities can train LPN’s to perform tasks outside their scope of practice
Facilities can train UAPs to perform tasks outside their scope of practice
The RN retains accountability for supervision and safe execution of these tasks
RN CANNOT Delegate
Any task that involves:
Clinical reasoning
Requires nursing judgement
Involves critical decision making
Involves the nursing process
Is above the scope of practice for the LPN or UAP
The nurse is planning care for a group of clients. Which task should the nurse assign to the licensed practical nurse (LPN)?
A. Assisting a client with crutch walking following knee replacement surgery.
B. Analyzing lab data to identify issues for a client who has diabetes mellitus.
C. Performing an admission assessment on a postoperative client.
D. Developing the plan of care for a client following an amputation.
A. Assisting a client with crutch walking following knee replacement surgery.
The nurse is caring for several clients. Which task is most appropriate to delegate to the unlicensed assistive personal (UAP)?
A. Assisting the client with preparation of a sitz bath
B. Walking the post-operative client that just returned from surgery
C. Coaching the client to deep breath during painful procedures
D. Monitoring the client for signs of discomfort while ambulating
A. Assisting the client with preparation of a sitz bath
The RN is caring for a group of clients. Which tasks can be delegated to the LPN? Select all that apply
A. Provide discharge instructions to a client's spouse
B. Obtain vital signs for a client who is 8 hours post-op
C. Administer oral pain medication to a client who is 1 day post-op
D. Initiate a care plan for a client who was admitted last night
E. Administer insulin to a client who is diabetic
B. Obtain vital signs for a client who is 8 hours post-op
C. Administer oral pain medication to a client who is 1 day post-op
E. Administer insulin to a client who is diabetic
A nurse is delegating assignments for a nursing team that includes an unlicensed assistive personnel (UAP). Which tasks should the nurse delegate to the UAP? (Select All That Apply)
A. Bathe a client who had an amputation 2 days ago
B. Assist a client to ambulate using a gait belt
C. Explain a low-sodium diet to a client who has hypertension
D. Review oral hygiene with a client who is receiving chemotherapy
E. Measure and document a client's intake and output
A. Bathe a client who had an amputation 2 days ago
B. Assist a client to ambulate using a gait belt
E. Measure and document a client's intake and output
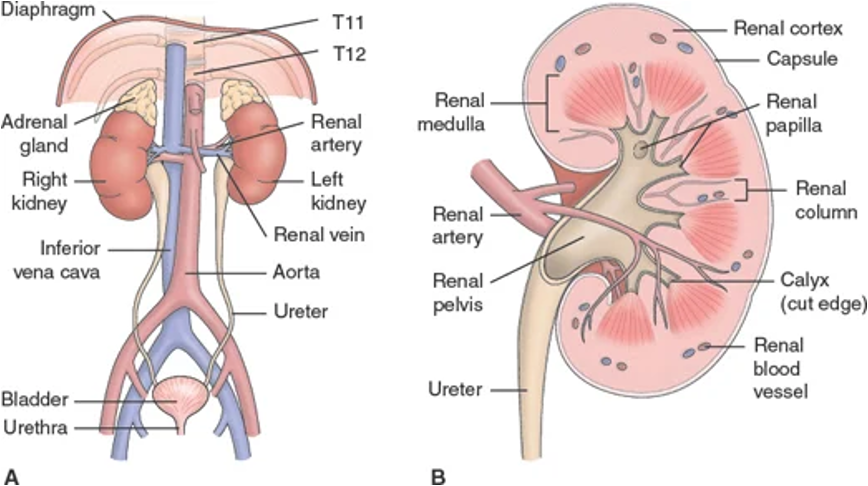
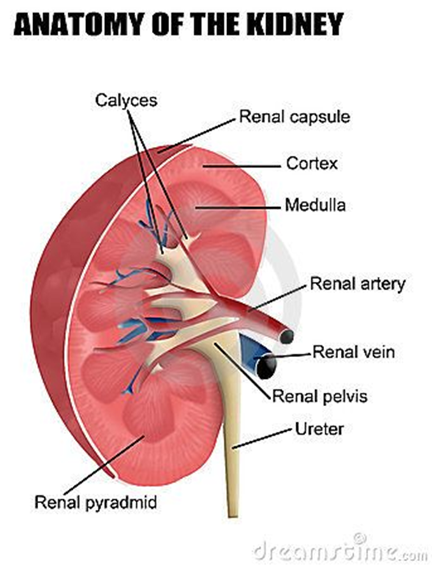
Renal/Urology - System Overview
Structures include kidneys, ureters, bladder, and urethra
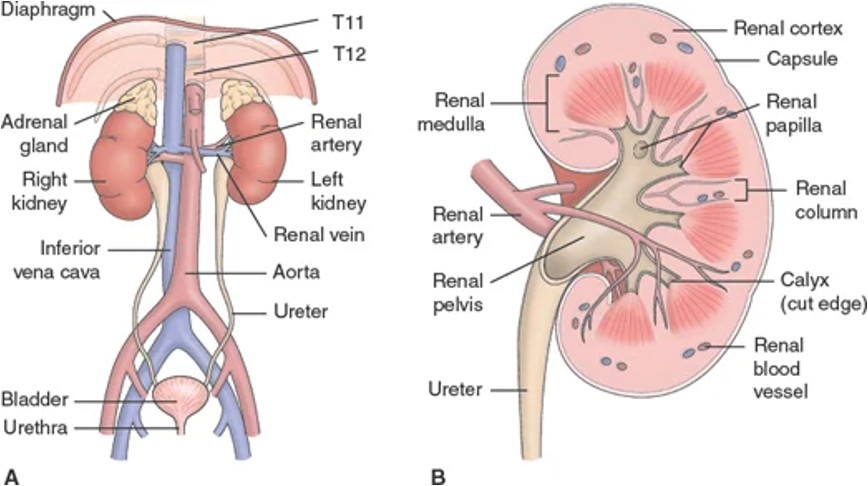
Renal/Urology: Anatomical Components - Nephrons
Cells of the kidneys
Responsible for filtration (urine production)
Consider renal replacement therapy when greater than 85% is damaged
Will autoregulate based on body’s needs
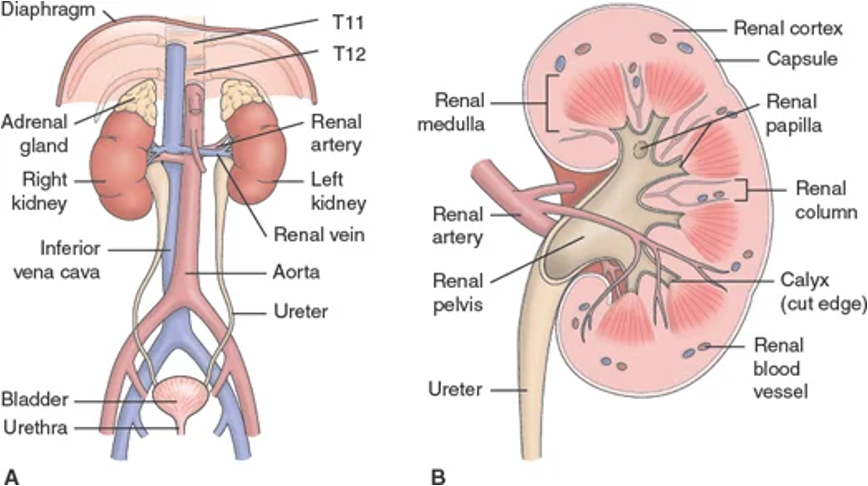
Renal/Urology: Anatomical Components - Ureters
Moves urine to bladder
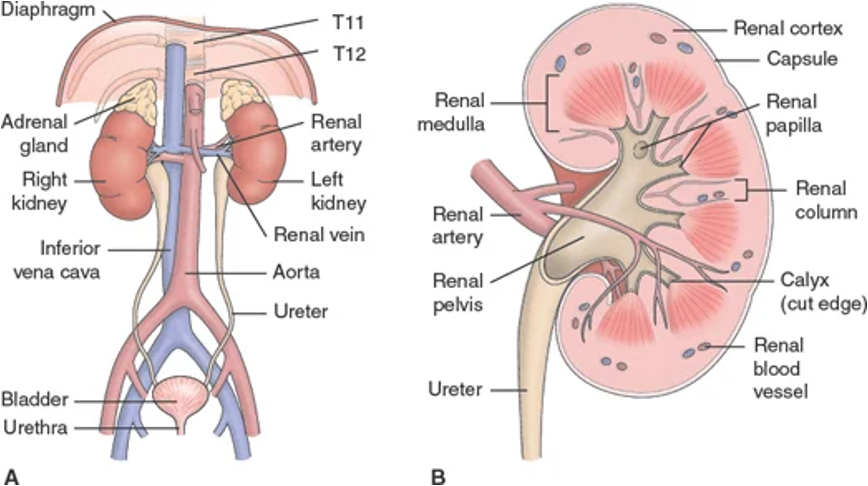
Renal/Urology: Anatomical Components - Bladder
Houses urine to be excreted and prevents urine reflux into kidneys
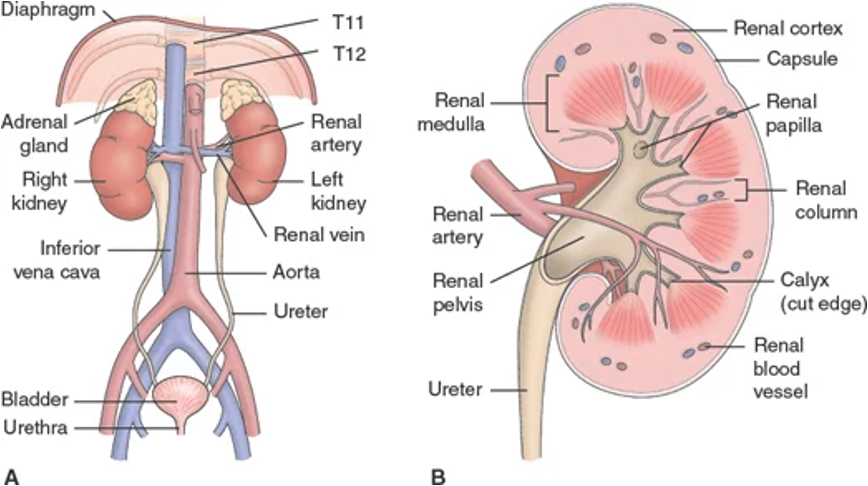
Renal/Urology: Anatomical Components - Urethra
Eliminates urine from bladder
Renal Physiology
Control of blood pressure
Control of water balance
Excretion of waste via urine formation
Regulation of electrolytes
Regulation of acid-base balance
Regulation of red blood cell production
*Production of ADH in the kidneys helps with fluid balance and BP management
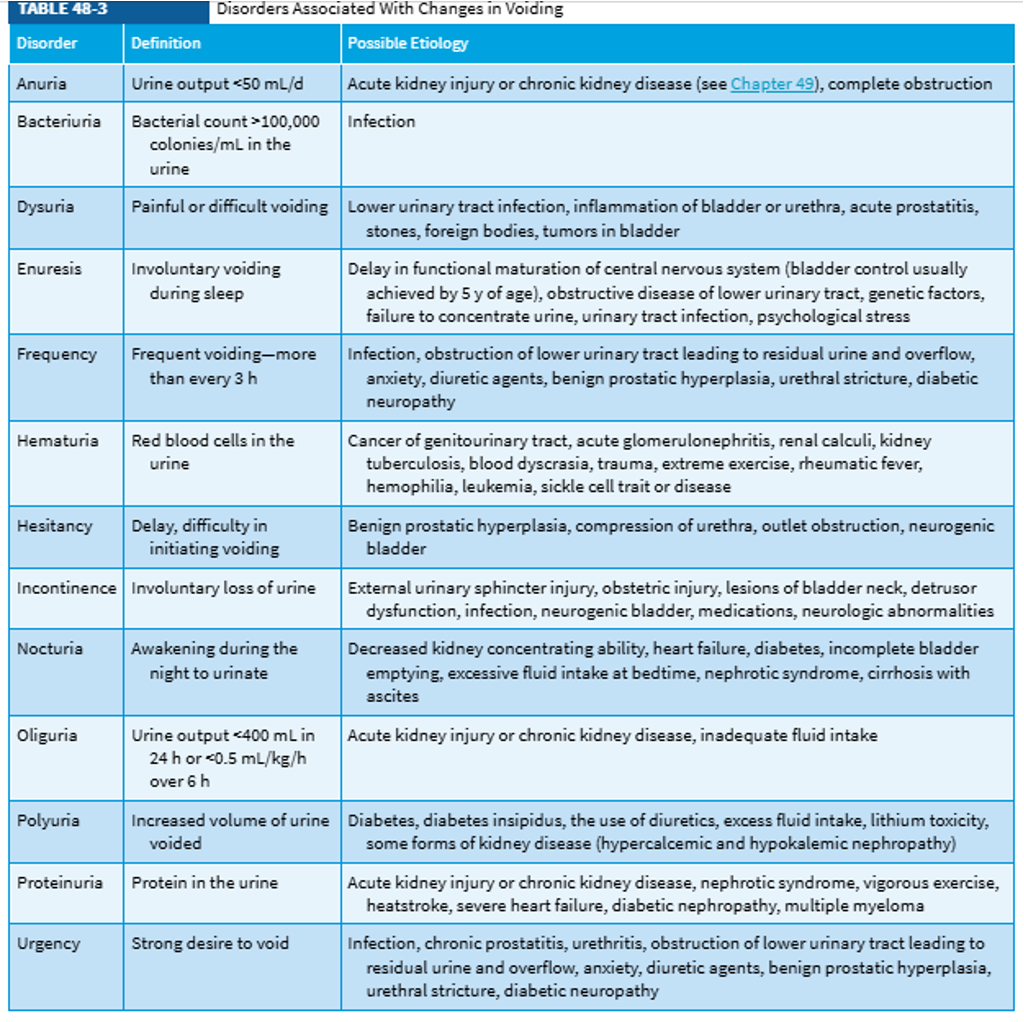
Common Urinary Symptoms
*400 mL of urine per day is the estimated minimum of what is needed to rid the body of waste
Renal/Urology - Nursing Assessment
Head-to-toe focusing on abdomen, suprapubic region, genitalia, low back and lower extremities
Palpation of the kidneys is not usual, this may indicate enlargement
Physical symptoms
Pain characteristics are important for diagnosing
Is it dull or achy? sharp or stabbing? where is it? are you having any other symptoms along with the pain?
Changes in voiding patterns or urine appearance
Are GI symptoms present? N/V, diarrhea, abdominal pain or discomfort
Unexplained anemia
Health history
Ask about risk factors
Previous stones or UTI
Family history
Genetically passed disorders
EXs: polycystic kidney disease (PKD), renal cystic diases, diabetes, CAD, pulmonary HTN
Male inferility or cystic fibrosis
Renal tumors or cancers
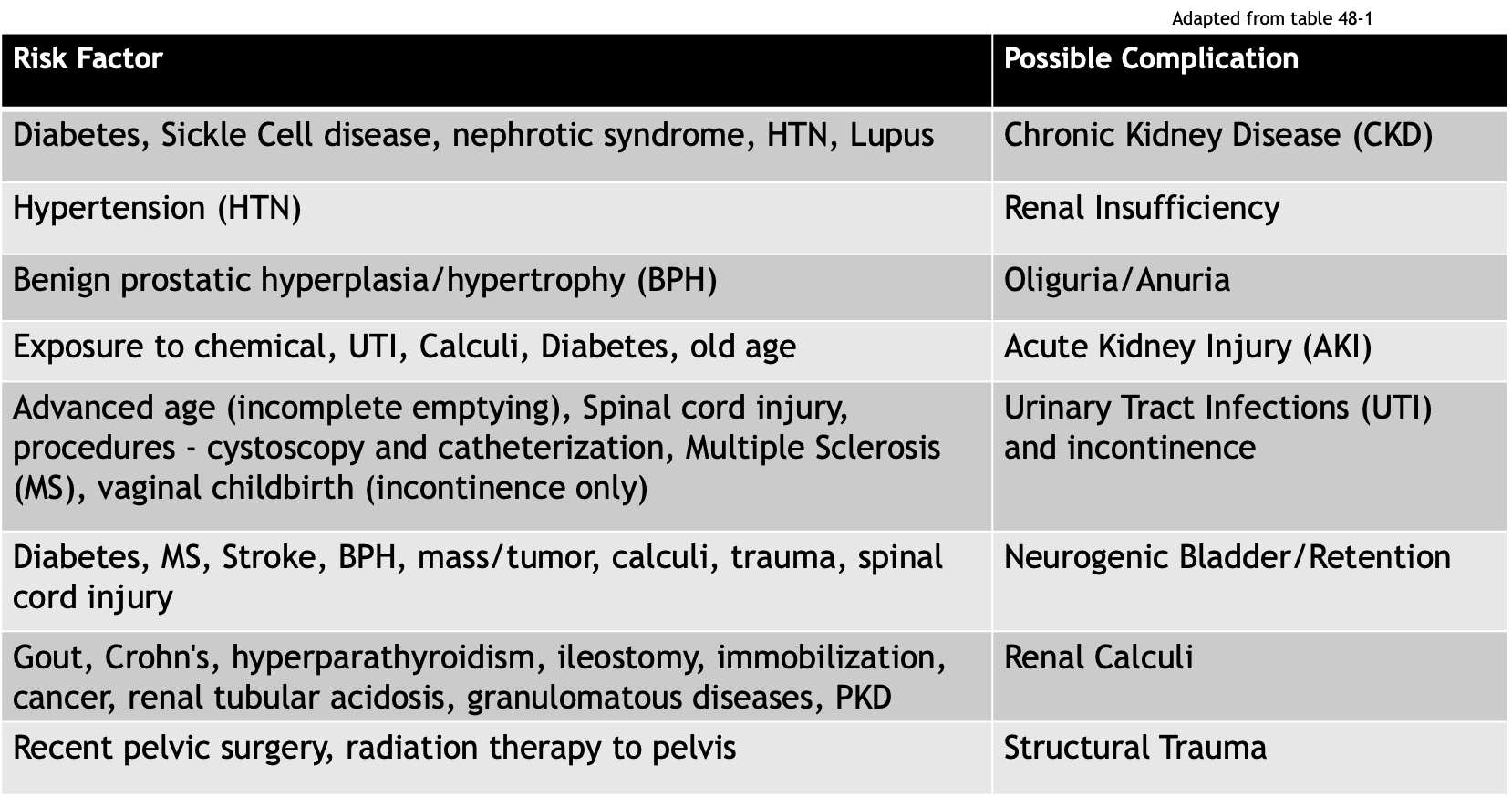
Risk Factors for Renal + Urologic Disorders
Diagnostics for Renal Function - Urine Tests: Urinalysis (US)
Checks color, clarity, pH , specific gravity, and presence of cells/protein/glucose/ketones
Diagnostics for Renal Function - Urine Tests: Urine Culture and Sensitivity (C&S)
Diagnostics for Renal Function - Urine Tests: 24-Hour Urine Collection
24-hour urine collection
Daily urine output (UO) - normal is 1 mL/kg/hr (1-2L/day)
Picture of the kidney’s ability to clear solutes from plasma
Usually measuring creatinine in urine
Diagnostics for Renal Function - Urine Tests: Osmolality
Measures presence of solutes in urine
Normal range: 200-800 (less is best!)
Diagnostics for Renal Function - Urine Tests: Specific Gravity
Measures density compared to water
Normal range is 1.005-1.025
Abnormal low can be from diabetes insipidus, glomerulonephritis, and hyperhydration
Abnoraml highs can be from diabetes mellitus, nephritis, and dehydration
Diagnostics for Renal Function - Blood Tests: BUN
8-20 mg/dL
Blood urea nitrogen (end-product of protein metabolism)
High levels indicate the kidneys are not filtering well
Diagnostics for Renal Function - Blood Tests: Creatinine
Male: 0.6-1.2 mg/dL; female: 0.4-1 mg/dL
Waste product that is not filtered appropriately in presence of renal damage
Diagnostics for Renal Function - Blood Tests: eGFR (Glomerular Filtration Rate)
Used to identify the stage of kidney disease
Decreases naturally with aging changes
Age (years)
Average eGFR
20–29
116
30–39
107
40–49
99
50–59
93
60–69
85
70+
75
Upper and lower urinary tract function changes with age
The GFR decreases, starting between 35-40 years of age, and a yearly decline of about 1 mL/min continues thereafter with a notable decrease in GFR by as much as 30%-50% by age 70
Older adults are more susceptible to AKI and CKD due to structural and functional changes in the kidney
Kidney function results may be within normal limits until the GFR is reduced to less than 50% of normal
GFR Classifications
Stage | Description | eGFR | Kidney Function |
1 | Possible kidney damage (e.g., protein in the urine) with normal kidney function | 90 or above | 90-100% |
2 | Kidney damage with mild loss of kidney function | 60-89 | 60-89% |
3a | Mild to moderate loss of kidney function | 45-59 | 45-59% |
3b | Moderate to severe loss of kidney function | 30-44 | 30-44% |
4 | Severe loss of kidney function | 15-29 | 15-29% |
5 | Kidney failure | Less than 15 | Less than 15 |
Gerontologic Considerations - Renal
GFR begins to decrease 1 point/year starting at age 35-40
Increased risk for AKI due to structural changes of the kidney
Sclerosis of renal tissues, decreased blood flow or perfusion, decreasing GFR, etc
Increased risk for dehydration and hypernatremia with a decreased stimulation of thirst
Gerontologic Considerations - Urology
Decreased bladder muscle tone and decreased vasopressin and ADH levels
Can cause an increase of residual urine
Often have incomplete emptying of the bladder and/or urinary stasis which increase the risk of a UTI and urinary urgency
Increased likelihood of nocturia
Increased likelihood of urinary incontinence
Also maybe related to mobility
May self-limit fluid intake - watch for dehydration
Symptoms may appear as other GI issues making diagnosis difficult
Acute Kidney Injury
Renal damage resulting in a rapid loss of function (impaired filtration/regulatory functions)
Criteria (only one must be present)
Increase in baseline serum Cr by 50% or more
An increase of 0.3 mg/dL within 48 hours
Decreased UO <0.5 mL/kg/h x 6 hours
Can progress to ESKD (end stage kidney disease) if not treated quickly
Changes to BUN, Cr, and GFR
Metabolic complications such as acidosis and/or fluid and electrolyte imbalances
Urine output (UO) may or may not be affected
Patients may appear critically ill showing signs of lethargy, drowsiness, headache, muscle twitching, seizures
Mortality rate can be as high as 80% - prevention is essential
Critical illness symptoms mostly reflect the symptoms of electrolyte imbalance
Phases of AKI - Initiation (1)
Begins at the initial insult to kidney function and ends when the oliguria phase starts
Phases of AKI - Oliguria (2)
Increase of serum concentration of substances usually excreted by kidneys (ex - creatinine, K+, phosphorous, magnesium); UO drops to 400 mL/day or less
Watch for uremic symptoms, life threatening electrolyte imbalances such as hyperkalemia may also develop
Some patients may be non-oliguric and still maintain normal UO of 1-2 L/day, but the substances which should be excreted are not being filtered out
*Do not confuse the “oliguria” phase with the definition of oliguria as a urinary symptom
Phases of AKI - Diuresis (3)
Gradual increase in GFR and UO, stabilization of labs with possible decrease
Continue to monitor for uremic symptoms and for possible dehydration
Phases of AKI - Recovery (4)
Labs return close to patient baseline; permanently decreased GFR will be present (1-3%)
AKI - Causes
Changes to perfusion
Intravascular volume depletion
Impaired cardiac function/decreased CO
Vasodilation
Increased diuresis (physiological or med)
Injury to renal tissue (renal ischemia)
Infections or obstruction in the renal/urologic tract
Transfusion reactions or hemolytic anemia
Trauma/crushing injuries
Rhabdomyolysis
Clinical syndrome characterized by injury to skeletal muscle fibers with disruption and release of their contents into the circulation
Myoglobin, creatine phosphokinase (CK) and lactate dehydrogenase are the most important substances for indicating muscle damage
Rhabdomyolysis-induced acute kidney injury (RIAKI) occurs following damage to the muscular sarcolemma sheath, resulting in the leakage of myoglobin and other metabolites that cause kidney damage
Nephrotic agents (NSAIDS, ACE inhibitors, chemicals, contrasts, etc)
AKI - Treatments
Goal: To restore normal chemical balance and prevent further complications
Identify and eliminate/treat the underlying cause if possible
Provide renal replacement therapy when ordered (KRT/RRT)
HD; PD; CRRT
Assess/monitor fluid balance:
Daily weights, CVP< I/O balance, total UO per 24 hours
Nutrition support: high calorie and high protein, restrict Na, K, phosphorous
Assess physical condition and labs
Turn, cough, deep breathe to prevent atelectasis and pneumonia
Skin care - bather with cool water and reposition frequently
The skin may be dry or susceptible to breakdown due to edema; therefore, meticulous skin care is important
Excoriation and itching of the skin may result from the deposit or irritating toxins in the patient’s tissues
Strict asepsis
Infection prevent with all catheters and vascular access devices
Treat fevers quickly
Plan + provide individualized education and psychosocial support
Types of Urology Disorders
Urinary tract infections
Adult voiding dysfunction
Urolithiasis and nephrolithiasis
Urinary cancers
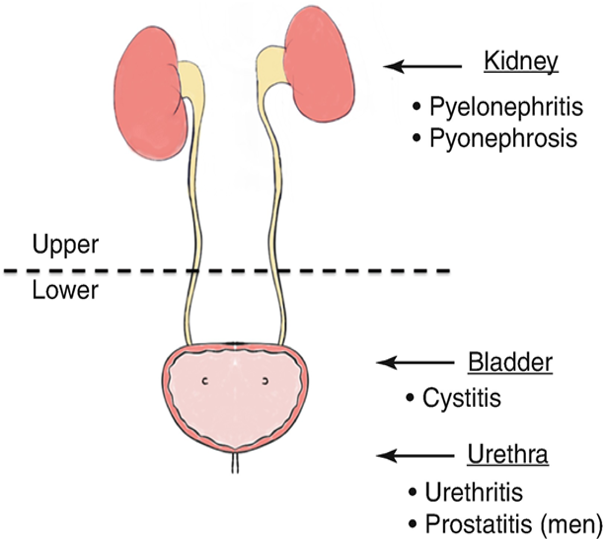
Urinary Tract Infections
Occurs when a pathogen enters the urinary tract, remember this system is sterile above the urethra
Identified by location: upper or lower
Upper UTIs include pyelonephritis, interstitial nephritis, and abscess (renal or perirenal)
Lower UTIs include cystitis (bladder), prostatitis (prostate), and urethritis (urethra)
If not treated, can lead to AKI, CKD, or urosepsis
Accounts for over 8 million healthcare visits/year
More common in females
CAUTI is the most common healthcare-associated infections and cause of secondary bloodstream infections
CAUTI is a UTI associated with indwelling urinary catheters
A UTI that occurs while the pt has an indwelling urinary catheter in place for more than 2 calendar days on the day that the infection was detected
Urinary Tract Infections - Risk Factors
General risk factors
Bacteria in the urinary tract
Female gender - anatomy (shorter), pregnancy, and intercourse
Comorbidities such as DM or gout
Immunosuppression
Urinary stasis and/or backwards flow
Instrumentation of the urinary tract (catheters/procedures)
“HARD TO VOID” acronym (another flashcard)
Age-related (geriatric) risk factors
Cognitive impairment
Frequent use of antimicrobials
Multiple chronic medical conditions
Immunocompromise
Immobility
Incomplete emptying of bladder
Low fluid intake, dehydration
Poor hygiene/stool incontinence
“Hard to Void”
Hormone changes (pregnancy, menopause)
Antibiotics (changes the normal flora)
Renal stones (obstructs flow of urine)
Diabetes (high glucose levels and poor immunity)
Toiletries (powders, perfumes, bubble baths)
Obstruction - BPH (enlarged prostate), masses/tumors
Vesicoureteral reflux *urine returns to the ureters - usually congenital)
Overextended bladder (immobility, spinal cord injury, etc)
Invasive (intercourse, indwelling catheters, procedures)
Disease states (remember the disease related complications)
Urinary Tract Infections - Supporting Data
Physical assessment:
Abnormal abdominal findings, back/suprapubic/pelvic pain
Urinary symptoms
May be asymptomatic (common with an indwelling catheter)
The nurse should inquire about association of symptoms with personal activity (ex - intercourse, hygiene, etc)
Urine characteristics: appearance with UA w/ C&S
Kidney/bladder ultrasound
Urinary Tract Infections - General Nursing Interventions
Treat with providers’ orders
Pain relief - use heat therapy or med if ordered (analgesics and antispasmodics)
Antibiotics or anti-infectives
Increase fluid intake, but avoid irritants like coffee, tea, citrus, alcohol, etc
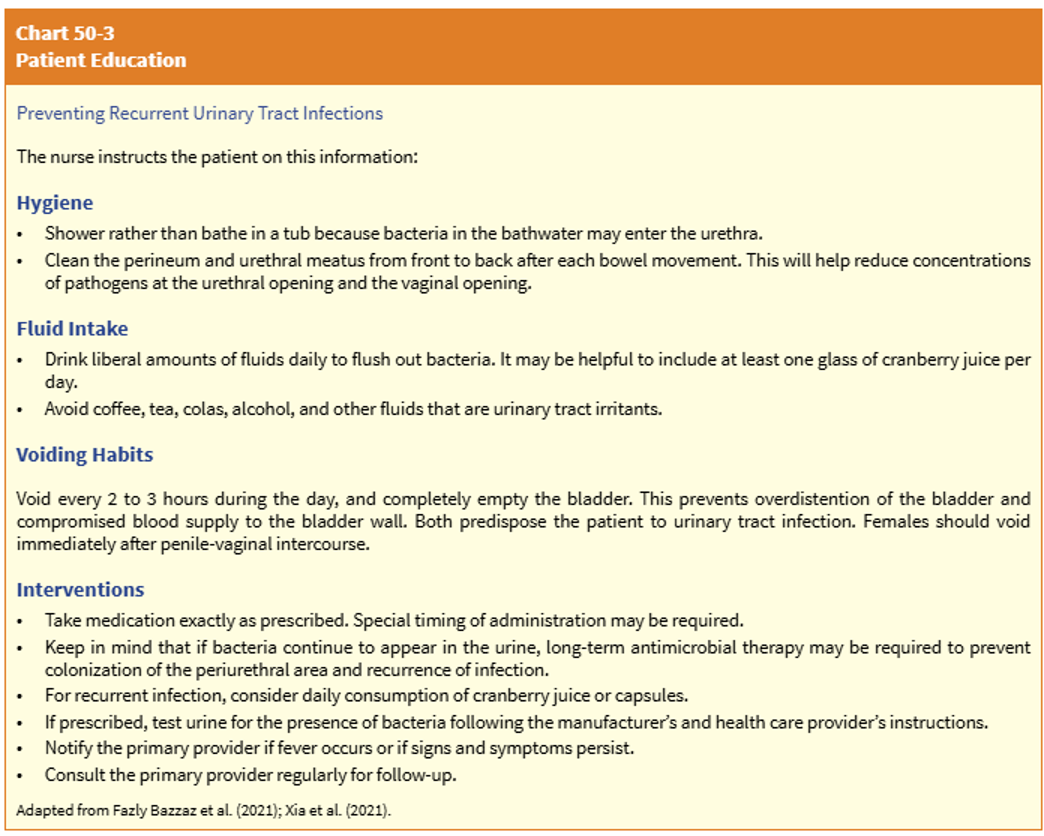
Pt education
Treatment compliance
Prevention of reoccurence by controlling modifiable risk factors
Cranberry juice/supplement for prevention of recurrent UTI
Reduce UTI incidence by 30%
Lower UTI
Bacteria migrates to the bladder and causes an infection
Most commonly, fecal organisms (like E. coli) migrate via the transurethral route
Reflux of urine from the urethra into the bladder (urethrovesical)
Commonly happens when coughing, sneezing, or straining due to an increase of bladder pressure that pushes urine into the urethra, as pressure decreases, the urine flows back to the bladder and can carry bacteria with it
Lower UTI - Nursing Considerations
Additional assessment findings
Elderly - incontinence, delirium, decreased sensation leading to no report of symptoms
Post-menopausal women - malaise, nocturia, incontinence, foul-smelling urine
Confirm with UA or basic labs, no diagnostics needed unless there is concern for spreading infection or complication
Treatment typically involves a pharmacologic agent
Anti-infective/antibiotics and urinary analgesics; 3-5 days
Nursing interventions:
Assess/monitor virals and I&Os
Use external catheters, not indwelling
Monitor for spesis and other complications like pyleonephritis or kidney fialure
Patient education related to treatment and prevention
Upper UTI
Typically caused by bacteria traveling upward from the bladder or from a blood stream infection that reaches the kidneys
AKA: pyelonephritis - bacterial infection of the renal pelvis, tubules, and interstitial tissue of one or both kidneys
Other causes can be interstitial inflammation, abscess, kidney damage, tubular cell necrosis, a bladder infection, urinary stasis, or obstructions (tumors/structures/BPH) that cause reflux from the bladder into either or the ureters (ureterovesical or vesicoureteral reflux)
Less common that lower tract infections, but a more common cayse or urosepsis
Upper UTI/Pyelonephritis - Nursing Considerations
Additional assessment findings
Acute - physical assessment may show chills, fever, low back/flank pain, N/V, headache, malaise
The chronic condition happens after several acute episodes that leave scar tissue on the kidneys, resulting in permanent kidney damage
Chronic - asymptomatic unless the patient is experiencing an acute exacerbation and may also show fatigue, poor appetite, polyuria, excessive thirst, and weight loss
CT imaging, ultrasound, or a pyelogram may also be ordered with UA and labs
Treatment typically involves a pharmacologic agent
Anti-infective/antibiotics and urinary analgesics; 2 weeks
Nursing interventions:
Assess/monitor vitals and I&Os
Monitor for complications: ESKD, HTN, and renal calculi
Patient education to prevent further infection
Patient Education for Upper and Lower UTIs
Promote adherence to antibiotic regimen
Don’t stop because symptoms stop
Promote increased water intake - 3-4L per day
Monitor their own I&Os and notify MD of abnormal changes to urine appearance/volume
Encourage/promote frequent voiding (go when you feel the need, and every 2-3 hours)
Maintain good perineal hygiene, especially important for dependent/incontinent patients
Urinate before and after intercourse
Preventive measures for any modifiable tasks
Types of Voiding Dysfunction
Incontinence - “involuntary loss of urine”
Stress - happens with sneezes, laughing, exertion, etc… (no structural changes)
M - after prostatectomy, F - after pregnancy
Overflow - overdistended bladder due to bladder muscle dysfunction or obstructed outflow
Urge - aware of need to void but can’t get to a toilet quickly enough
Functional - physical or cognitive impairment
Latrogenic - external medical factors (ex - meds)
Mixed - combo of factors
Retention - “incomplete emptying”
Voiding Dysfunction - Incontinence
Assessment should include discussion of symptoms