ECG patterns
1/4
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
5 Terms
De Winter Pattern
The de Winter pattern is seen in ~2% of acute LAD occlusions and is often under-recognised by clinicians
Key diagnostic features include ST depression and peaked T waves in the precordial leads
Tall, prominent, symmetrical T waves in the precordial leads
Upsloping ST segment depression > 1mm at the J point in the precordial leads
Absence of ST elevation in the precordial leads
Reciprocal ST segment elevation (0.5mm – 1mm) in aVR
Typical STEMI morphology may precede or follow the De Winter pattern

Brugada Criteria (for diagnosing VT vs SVT with aberrancy)
Step-by-step Brugada Criteria (for wide-complex tachycardia):
Absence of typical RBBB or LBBB morphology → = VT
Positive or Negative concordance throughout the precordial leads → = VT
Very broad complexes > 160ms → = VT
AV dissociation visible? (P waves unrelated to QRS) → = VT
Extreme axis deviation (“northwest axis”) → = VT
Capture beats: Occur when the sinoatrial node transiently “captures” the ventricles in the midst of AV dissociation, producing a QRS complex of normal duration→ = VT
Fusion beats: Occur when a sinus and ventricular beat coincide to produce a hybrid complex → = VT
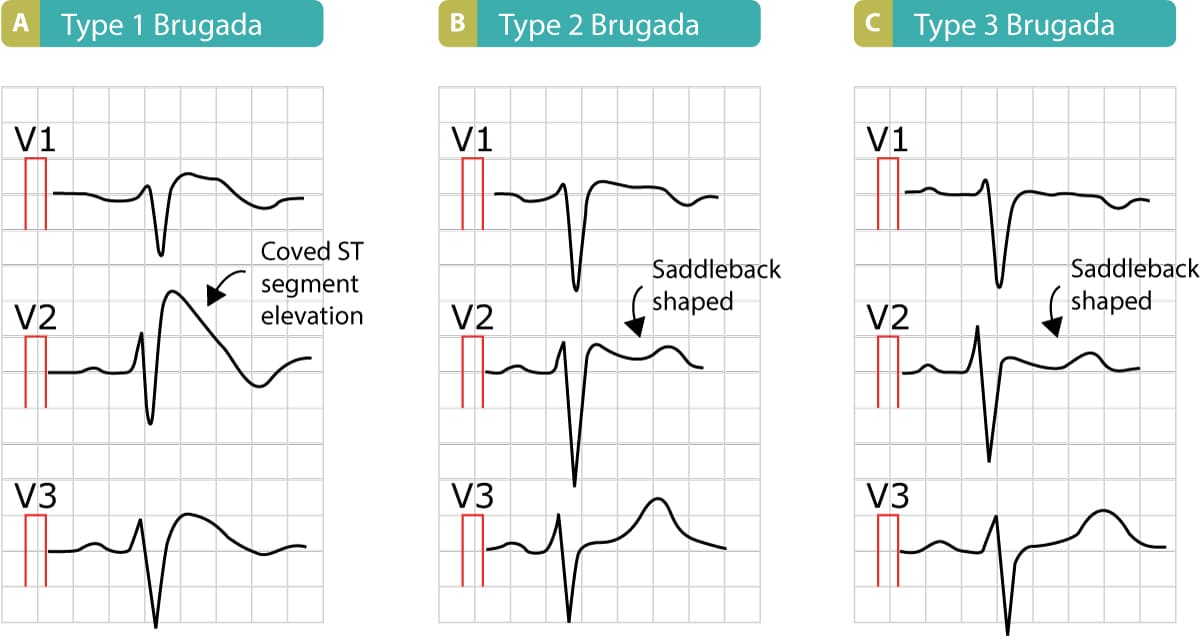
Brugada Syndrome (channelopathy associated with sudden cardiac death)
ECG: Look in leads V1–V3
Type 1 Brugada: Coved ST elevation ≥2 mm in ≥1 of V1–V3 followed by an inverted T wave
Type 2 or 3 are "saddle-back" patterns (less diagnostic)
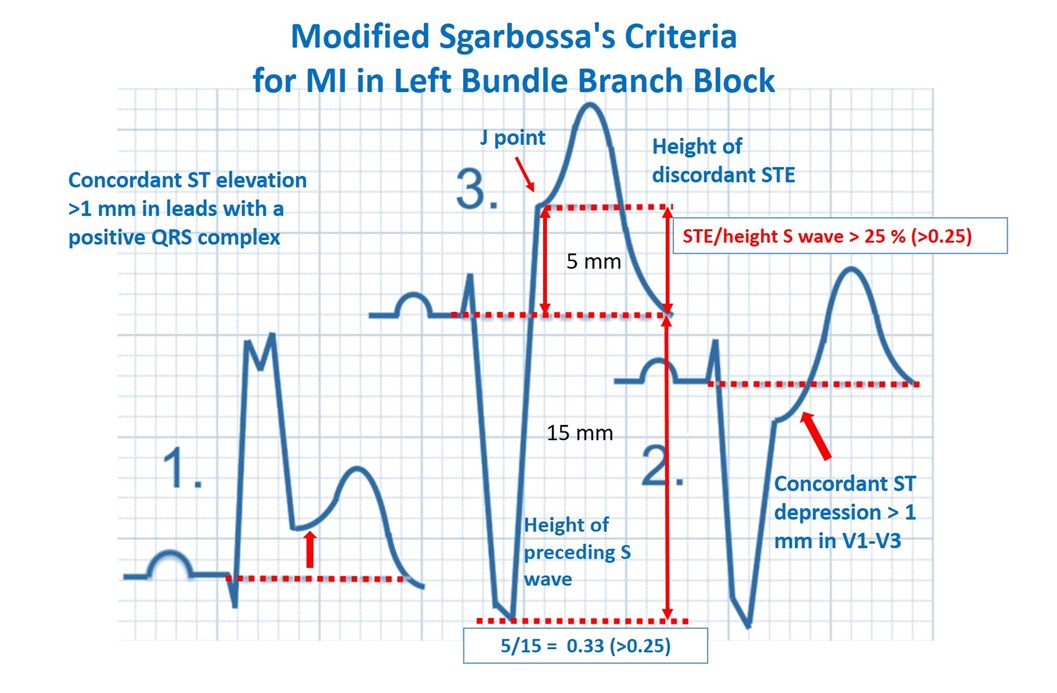
Sgarbossa Criteria (STEMI in the presence of LBBB or paced rhythm)
Original Sgarbossa Criteria:
Positive finding in any criteria is suggest OMI
Concordant ST elevation ≥1 mm in leads with a positive QRS (5 points)
Concordant ST depression ≥1 mm in V1–V3 (3 points)
ST Elevation at the J-point, relative to QRS onset, is at least 1 mm AND has an amplitude at least 25% of the preceding S-wave
An ST/S ratio of 0.20 is also very high and almost as specific as a 0.25 ratio
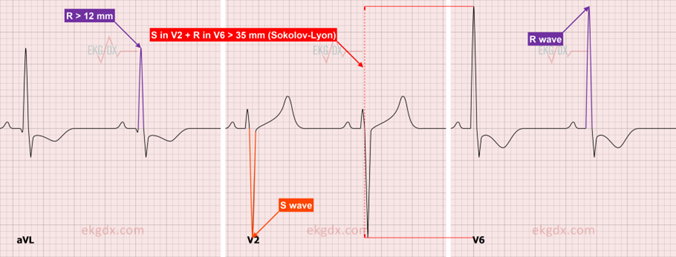
Sokolow–Lyon Criteria (for Left Ventricular Hypertrophy – LVH)
Measure S wave in V1
Measure R wave in V5 or V6 (whichever is taller)
Positive for LVH if:
S in V1 + R in V5 or V6 ≥35 mm
OR R wave in aVL ≥11 mm