chap. 19 - thorax, lungs
1/56
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
57 Terms
inspiration
diaphragm contracts + drops vertical chest expansion
intercostal muscles lift ribs/sternum = horizontal expansion + increase in AP diameter
creates negative pressure = air flows into lungs
expiration
passive — diaphragm + intercostals relax
chest cavity size decreases = positive pressure = air exits lungs
regulation
hypercapnia = strongest stimulus to breathe
hypoxemia = increases respirations, but less powerful
pulmonary - pleuritic pain
inflammation of parietal pleura (pneumonia, pulmonary infarction, neoplasm)
location = chest wall overlying process
quality = sharp, knife-like
severity = often severe
timing = persistent
aggravated = inspiration, coughing, movement
relieve = lying on affected side
symptoms = chest tenderness
cardiovascular - angina pectoris
temporary myocardial ischemia
location = retrosternal/across anterior (radiate to shoulders, arms, neck, lower jaw)
quality = pressing, squeezing, tight, heavy, occasional burning
severity = mild to moderate
timing = 1-3 min (10 min if prolonged)
aggravated = exertion, cold, meals, stress
relieve = rest, nitroglycerin
symptoms = dyspnea, nausea
cardiovascular - myocardial infarction
prolonged myocardial ischemia → irreversible muscle damage
location = retrosternal/across anterior (radiate to shoulders, arms, neck, lower jaw)
quality = pressure, squeezing, tightness, heaviness
severity = severe
timing = >20 min
aggravated = not always triggered; at rest
relieve = not relieved by rest
symptoms = nausea, diaphoresis, dyspnea
cardiovascular - pericarditis
irritation of parietal pleura adjacent to pericardium
location = retrosternal (radiate to shoulder, back)
quality = sharp, knife-like
severity = variable
timing = persistent
aggravated = breathing, swallowing, body position changes
relieve = sitting forward
symptoms = autoimmune conditions may present
aortic dissection
splitting of aortic wall
location = anterior chest (radiate to baclk neck)
quality = ripping, tearing
severity = very severe
timing = abrupt onset
aggravated = hypertension
relieve = nothing clearly relieves
symptoms = syncope, unilateral weakness
gastrointestinal - reflux esophagitis
inflammation from reflux stomach acid
location = retrosternal (radiate to back)
quality = burning
severity = mild to severe
timing = variable
aggravated = large meals, bending, lying down
relieve = antacids, belching (burping)
symptoms = regurgitation, dysphagia
diffuse esophageal spasm
variable motor dysfunction
location = retrosternal (radiate to back, arms, jaw)
quality = squeezing
severity = mild to severe
timing = variable
aggravated = stress
relieve = nitroglycerin
symptoms = dysphagia
chest wall pain (costochondritis)
local inflammation of costal cartilage
location = below left breast or along costal cartilages
quality = stabbing. sticking, dull, aching
severity = variable
timing = hours to days
aggravated = movement, pressing the area
relieve = local heat, analgesics
symptoms = tenderness at local sites
anxiety/panic disorder
unknown process
location = precordial; below left breast or across chest
quality = stabbing, sticking, dull, aching, or variable
severity = variable
timing = hours to days
aggravated = emotional stress
relieve = may come and go
symptoms = breathlessness, tingling in lips + hands, dizziness
AP + transverse diameter (barrel chest)
commonly results from emphysema due to hyperinflation of the lungs
normal breathing
12-20 bpm + regular
tachypnea
more than 24 bpm + shallow
fever, anxiety, exercise
bradypnea
less than 10 bpm + regular
well-conditioned athletes, med-induced depression of respiratory center, diabetic coma, neurologic damage
hyperventilation
increased rate + increased depth
extreme exercise, fear, anxiety
kussmaul
rapid, deep, labored
diabetic ketoacidosis
hypoventilation
decreased rate, decreased depth, irregular pattern
overdose of narcotics or anesthetics
cheyne-stokes respiration
regular pattern characterized by alternating periods of deep, rapid, breathing followed by periods of apnea
severe congestive heart failure, drug overdose, increased intracranial pressure, renal fialure
blot respiration
irregular pattern characterized by varying depth + rate of respirations followed by periods of apnea
meningitis or severe brain damage
ataxic
significant disorganization with irregular + varying depths of respirations
respiratory compromise
air trapping
increasing difficulty in getting breath out
COPD
decreased fremitus (99)
indicates consolidation (increases fremitus) or bronchial obstruction, aur trapping in emphysema, pleural effusion, or pneumothorax
chest expansion
unequal chest expansion can occur with severe atelectasis, pneumonia, chest trauma, or pneumothorax
bronchial sounds
high pitch, hard or hallow, loud, short during inspiration; long in expirations, trachea + thorax
bronchovesicular sounds
moderate pitch, mixed, moderate amplitude, same during inspiration + expiration
over the major bronchi-posterior; between the scapulae; anterior'“ around the upper sternum in the first + second intercostal spaces
vesicular sounds
low pitch, breezy, soft amplitude, long in inspiration; short in expirations, peripheral lung fields
crackle (fine)
high-pitched, short, popping sounds heard during inspiration + not cleared with coughing
crackles occurring LATE in inspiration associated with restrictive diseases (pneumonia, CHF)
crackles occurring EARLY in inspiration associated with obstructive disorders (bronchitis, asthma, emphysema)
crackles (coarse)
low-pitches, bubbling, moist sounds that may persist from early inspiration to early expiration
sofl separating velcro
associated conditions → pneumonia, pulmonary edema, pulmonary fibrosis-long-term COPD
pleural friction rub
low-pitched, dry, grating sound
sand paper or dry leather rubbing together
similar to crackles only more superficial + occurring during both inspiration and expirations
associated conditions → pleuritis (inflammation of the pleura = the thin, double-layered membrane surrounding the lungs + lining the chest cavity)
wheeze (sibilant)
high-pitched, musical sounds head primarily during expiration but may also be heard on inspiration (hissing sound)
air passes through constricted passages caused by swelling, secretions, tumor
associated conditions → acute asthma, chronic emphysema
wheeze (sonorous)
low-pitched snoring or moaning sounds heard primarily during expiration but may be heard throughout the respiratory cycle
associated conditions → bronchitis or single obstructions + snoring before an episode of sleep apnea, may clear with coughing
bronchophony
client says “99”
normal = words sound soft, muffled, and indistinct
abnormal = words easily understood + louder over areas of increased density (tumor, consolidation)
egophony
client says “E”
normal = soft + muffled, but “E” is distinguishable and heard as “eee”
abnormal = louder + sounds like a bleating “aaa” sound over areas of consolidation
whispered pectoriloquy
client says “one-two-three”
normal = very faint + muffled, may be inaudible
abnormal = sound transmitted very clearly + distinctly over areas of consolidation
chronic obstructive pulmonary disease (COPD)
progressive lung disease characterized by airflow limitations that it nos fully reversible
1. chronic bronchitis = inflammation + mucus production narrow the airways
2. emphysema = destruction of alveoli reduces surface area for gas exchange
s/s → shortness of breath, chronic cough, exercise intolerance, reduced oxygenation over time
risk factors → smoke exposure, having asthma, occupational exposure to dust + chemicals, exposure to fumes from burning fuels, genetics (rare)
lung cancer
1. small cell lung cancer (SCLC)
2. non-small cell lung cancer (NSCLC)
lung cancer risk factors
smoking, exposure to asbestos, radon, arsenic, diesel exhaust, air pollution, personal history of radiation exposure, personal or family history of lung cancer, exposure to many toxins
consolidation in lobe
filled with fluid, pus, blood, cells
alveoli not longer ventilated with air
causes → pneumonia, pulmonary edema, hemorrhage
obstructive atelectasis
air cannot reach alveoli, and trapped air is gradually absorbed, causing lung segment to collapse
no ventilation to the affected alveoli
causes → mucus, foreign body, tumor, shallow breathing
pneumothorax
air enters the pleural space, causing partial or complete lung collapse
TENSION pneumothorax is a medical emergency!!!! due to impaired venous return
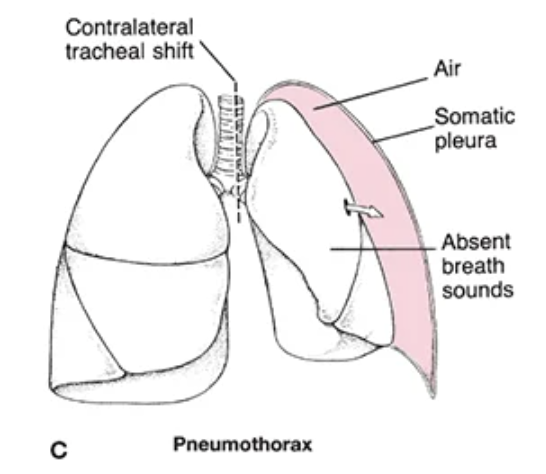
pneumothorax causes
trauma, spontaneous rupture of blebs, mechanical ventilation, underlying lung disease
pneumothorax physiology
air disrupts the negative pressure needed to keep the lung expanded
pneumothorax s/s
sudden sharp chest pain, dyspnea, absent breath sounds on affected side, hyper-resonance to percussion, tracheal shift away from affected side
pleural effusion
excess fluid accumulates in pleural space, compressing lung
lung effusion may cause tracheal shift away from the affected side
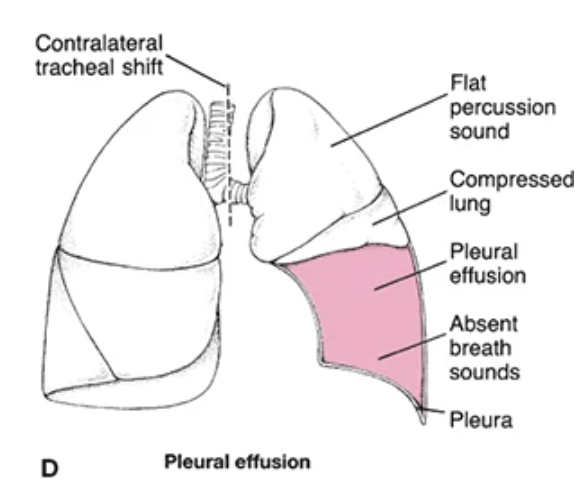
pleural effusion causes
heart failure, infection (parapneumonic effusion), malignancy, liver/renal disease
pleural effusion physiology
fluid prevents full expansion leading to decreased ventilation
pleural effusion s/s
diminished or absent breath sounds over fluid, dullness to percussion, decreased fremitus, dyspnea, chest pressure
emphysema
type of COPD characterized by destruction of alveolar walls leading to the loss of elastic recoil + air trapping
patients rely on hypoxic drive in advanced disease → important for oxygen titration
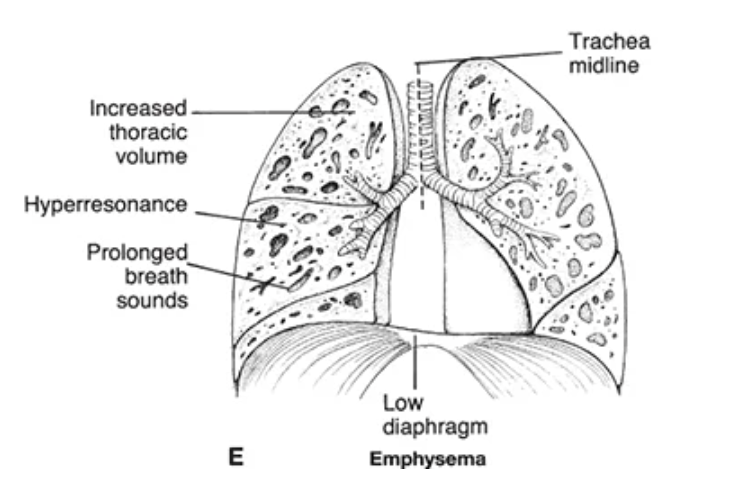
emphysema causes
long-term smoking (most common), alpha-1 antitrypsin deficiency
emphysema physiology
hyperinflated lungs (air trapping), reduced surface area for gas exchange, increased work of breathing
emphysema s/s
diminished breath sounds dur to hyper-inflation, hyper-resonance to percussion, barrel-shaped chest, prolonged expiration, dyspnea on exertion
barrel chest
AP lateral ratio 1:1

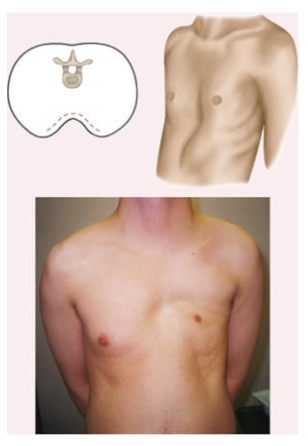
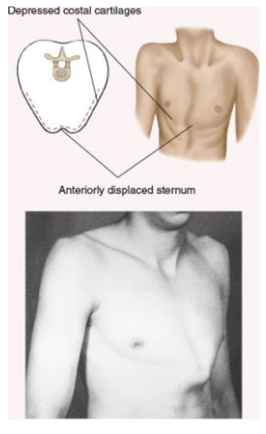
pectus excavatum
inverted sternum
pectus carinatum
everted sternum (protruding skin)
older adult considerations
dyspnea with certain activities
absent chest pain associated with pleuritis
decreased ability to cough effectively
kyphosis (rounding curvature of upper back)
decreased thoracic expansion
difficulty in deep breathing; fatigue easily
tenderness or pain at costochondral junction of ribs (seen w/ fractures, especially w/ osteoporosis)