Lecture 2: Assessment of Sexual Offenders
1/81
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
82 Terms
What are some of the reasons we might assess sex offenders?
risk level
treatment needs
interests
potential victims
legal reasons
Content of Assessment Interview
demographic info
childhood experiences
experience of abuse
education history
employment history
protective aspects
relationship history
offense history
description of current offense
Why carry out an assessment with sex offenders?
decision making about sentencing
determine risk level
treatment needs
criminogenic needs
dynamic risk
allow access to children?
level of immediate risk
release decisions
intensity of supervision in the community
What does functional analysis determine?
the underlying motives & functions for the offending behaviour
What does functional analysis typically involve?
obtaining detailed information about the antecedents, the behaviours, and consequences of offending (the ABC model), to look for patterns and determine the reinforcing and maintaining factors of the behaviour
blank → blank → blank
antecedents; behaviours; consequences
What kind of info might we want to gather in an assessment interview?
family history
risk factors
relationships they have
social support
underlying psychological disorders
paraphilic interests
sexual interests
access to victims
who might be at risk
info of the offence itself
triggers
Functional Analysis
Behaviours carried out along with the accompanying thoughts and emotions
Not always a straightforward task with offenders due to some level of denial being common
Cannot assume they’re being completely truthful
Risk Assessment
What does ‘Risky’ mean?
risk of recidivism
the type of reoffending
predicting sexual/violent offending
suicide
Risk for what?
type of reoffending (ex: any general, violent, sexual)?
reconviction, new charges, allegations
same crime or more serious crimes (ex: noncontact escalating to contact/violent offending)?
institutional sanctions?
harm of any kind?
danger to self?
over what time period?
imminently? next year? next 10 years? ever?
Generations of Risk Assessment
Clinical Judgment
Actuarial Assessment
Dynamic Assessment
Clinical Judgment
Unstructured
Based on experience and some level of knowledge of literature
Actuarial Assessment
Static, actuarial, based on factors empirically related to recidivism
Standardized assessment
Cannot measure change
Strong evidence
Dynamic Assessment
Standardized assessment, measures change
Some include Structured clinical judgement
Fewer validation studies but good evidence
(Risk Assessment)
includes explicit measures of change
Similar to third but with an integrated case management plan
Static Factors
Unchangeable, historical factors
Statistically related to recidivism
Also called actuarial assessment
e.g., previous offending history, age, relationship history
Static factor was also called?
actuarial assessment
Dynamic Factors
Potentially changeable factors; Amenable to change
overcome the limitations of purely static actuarial instruments
Statistically related to recidivism
Also called criminogenic need factors
e.g., antisocial cognitions, self regulation problems
Evidence that they are related to recidivism
Dynamic factors is also called?
criminogenic need factors
Static Assessment: STATIC-99
10-item inventory
Widely researched and validated
Displays good predictive validity
However:
Not validated for use with women
Not validated for offenders under the age of 16
Not validated for offenders whose only offence involves the possession of child sexual abuse material offenses or statutory rape
Evidence of discrepancies between races
What areas does Static-99 assess?
sexual deviance
range of potential victims
persistence (sexual offending behaviour)
general level of anti-sociality
Static-99: Sexual Deviance
measured by whether the offender has offended against male victims, has never had a long- term relationship, and/ or has committed non-contact sex offences
Static-99: Range of potential victims
measured by whether the offender has offended against unrelated and/or stranger victims
Static-99: Persistence (sexual offending behaviour)
measured by prior number of sexual offences
Issues with Static Risk Assessment
provides a probability, not a certainty of future recidivism
developed around official recidivism events, thus each risk category inevitably underestimate true re-offense rates
may lead clinicians to ignore unusual factors that are relevant to the individual case
misleading for individuals not represented or validation samples
they take no account of acute risk factors that might indicate imminent re-offending
most don’t indicate which factors need to be addressed in treatment for risk to be reduced
Dynamic Risk Factors (Thornton)
Deviant sexual interest
Pro-offending (or distorted) attitudes
Socio-affective (or relational/ intimacy) problems
Self management/ Emotional regulation difficulties
Evidence-supported Dynamic Risk Factors
atypical (deviant) sexual interests
antisocial cognitions/pro-offending attitudes
relationship problems
self-regulation problems
atypical (deviant) sexual interests risk factors
paraphilic sexual interests
sexual preoccupation
antisocial cognitions/pro-offending attitudes risk factors
offense supportive attitudes & beliefs
hostile masculinity
non-compliance with intervention
relationship problems risk factors
capacity for adult relationships
emotional congruence with children
negative social influences
self-regulation problems risk factors
impulsivity
lifestyle instability
emotional regulation problems
problem solving deficits
What risk factors do you think would increase someone’s future sex offending?
managing emotions
multiple previous offenses
lack of social support
ecology/situational context
substance abuse
age
when the offending started
juvenile
lower age = increase risk
Dynamic Risk Assessment: STABLE 2007
13-item inventory based on sexual and non-sexual dynamic risk factors
Intended for use with a static risk assessment
5 domains:
Social influences
Intimacy deficits
Self-regulation
Sexual self-regulation
Cooperation with community supervision
Displays good predictive validity
Evidence of discrepancies between races
Acute (contextual) Risk/’Panic Now’ Factors
‘the concept of risk is inherently contextual, as hazards arise in particular circumstances’
No matter how good an actuarial assessment is, it can never take into account fluctuations in contextual/proximal factors
Acute Assessment: ACUTE 2007
7-item inventory based on sexual and non-sexual dynamic risk factors
● Victim access
● Hostility
● Sexual preoccupations
● Rejection of supervision
● Emotional collapse, i.e., evidence of severe emotional disturbance/ emotional crisis
● Collapse of social supports
● Substance abuse
Intended for use with a static risk assessment
Displays good predictive validity
Components of a 4th Generation Risk Assessment
Static risk assessment
Dynamic risk/ risk-needs assessment
This dynamic assessment can be further divided into the assessment of
Stable
Acute factors
Includes a measure of treatment change
Risk/ Case Management Assessment
Overall Assessment Process
Interview
clinician
• Psychosocial History
education
• Offending history
• Personality characteristics
• Psychometrics
test for impulsivity
test for distorted
• Collateral information
Assessing Risk
risk principle
Utilize one of the risk assessment measures that we discussed previously
Best evidence is for actuarial/ static and combined static/dynamic
How should assessment inform treatment?
what type of treatment is most effective for the individual
how intense the treatment should be
Use overall risk level to guide?
the intensity of treatment
Can you think of any issues with static risk assessment?
doesn’t take into consideration of dynamic factors
Risk Principle
Treatment intensity should be proportional to risk level
Assessing Need
need principle
Dynamic Risk Assessment measures (e.g., SARN)
Psychometrics designed to tap into specific Need areas (e.g., distorted attitudes)
Interview
Collateral information
Need Principle
Treatment should target criminogenic need
i.e., those psychological risk factors such as deviant sexual interests, pro-offending attitudes, socio-affective problems and emotional dysregulation
Assessing Responsivity
responsivity principle
Psychometrics designed to tap into specific responsivity areas
Interview
Collateral information
E.g., Motivation, Intellectual Disabilities, Psychopathy, Denial, Treatment Readiness
blank characteristics will be what is actually addressed in treatment
need
Assessing responsivity will dictate?
whether any deviations need to be made from the standard format of treatment
treatment style should be tailored to meet the learning style, and abilities of offenders
What do protective factors decrease?
the risk of recidivism
Examples of Protective Factors
prosocial involvement
intelligence
strong social support
blank traits will be drawn upon & strengthened to address/overcome treatment needs
protective
What are challenges to offender risk assessment?
Limited resources (e.g., interviews are time consuming and expensive)
• Use of single or multiple assessments?
• Gender-specific or generic instruments?
• Accounting for ethnic and cultural variations
• Accounting for new types of crime and criminals
• Facilitating re-entry and reintegration
Evaluating Evidence through?:
assessment
treatment
Assessment
Examine which items/ measures predict sexual recidivism
AUC of the ROC
Treatment
Examine which approaches reduce recidivism/ bring about change
How do we compare different risk assessments measures?
ROC (Receiver Operating Characteristics) AUC (Area Under the Curve) Analysis
• Ranges from 0 to 1
• 0.5= chance prediction
• 1= perfect predictive accuracy
• AUC values of .56, .64, and .71 are interpreted as small, moderate, and large predictive accuracy effects
• Example of Interpretation: AUC of .70 indicates that there isa 70% chance that a randomly selected recidivist from the sample would have a higher risk score than a randomly selected nonrecidivist.
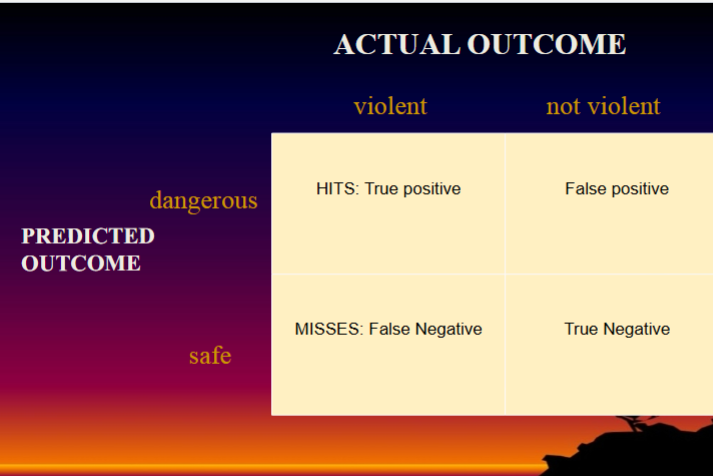
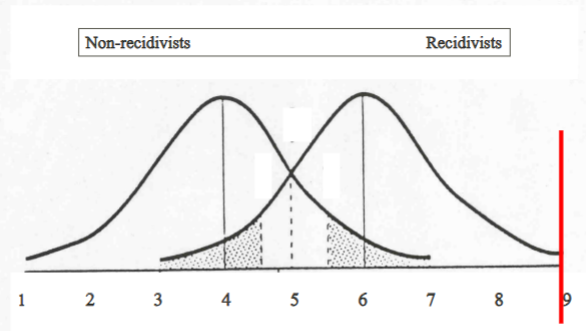
Hit Rates & False Alarms
We plot hit rates against false alarms for each point on a risk assessment measure to give area under the curve analysis
• If we take anybody above the red line as predicted to be dangerous…
• Anybody scoring above the red line who are recidivists are hits, i.e., the correct identification of those who have offended again
• Anybody scoring above the red line who are non-recidivists are false alarms
Hits
Anybody scoring above the red line who are recidivists
Ex: the correct identification of those who have offended again
False Alarms
Anybody scoring above the red line who are non-recidivists
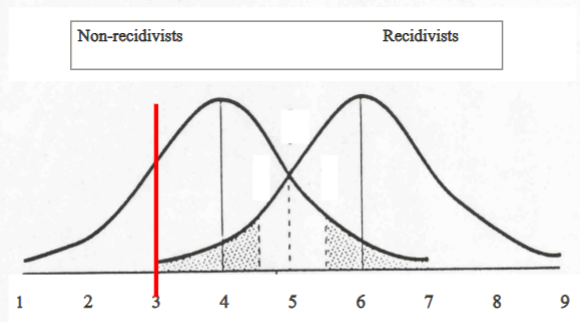
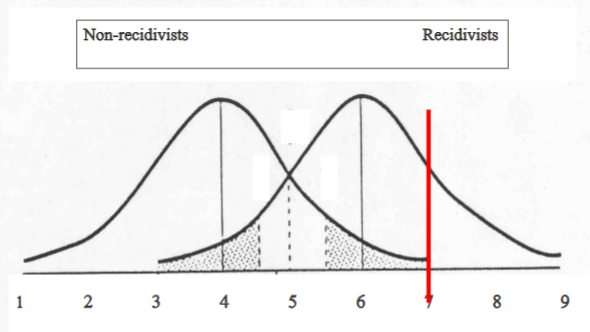
Score on a Measure (Static-99)
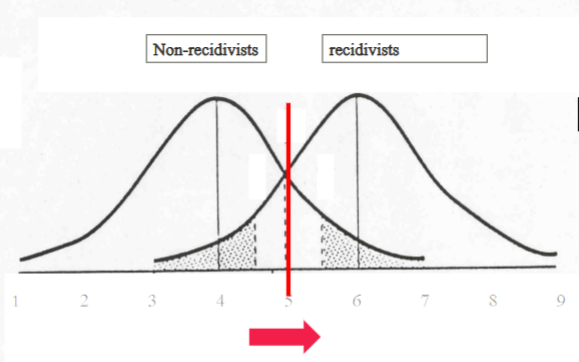
Here if we say anybody above 3 is dangerous, then, hit rate is high (100%), false alarm rate high (70%)
Here if we say anybody above 7 is dangerous, then, hit rate is low (30%), false alarm rate low (0%)
Anchor points: Here if we say anybody above 1 is dangerous, then, hit rate is low (100%), false alarm rate low (100%)
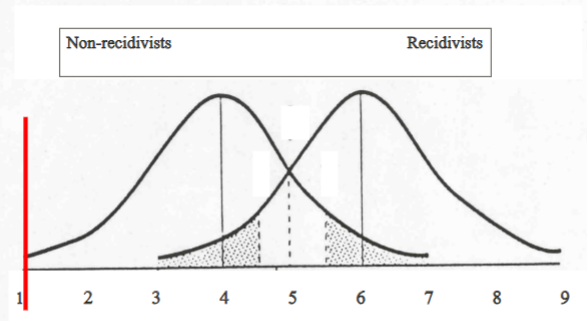
Anchor points: Here if we say anybody above 9 is dangerous, then, hit rate is low (0%), false alarm rate low (0%)
Comparison of Approaches
Individual studies suggest AUC is best for combined Static and Dynamic
• Average AUC for static/actuarial instruments to be 0.68 (averaged over
50 findings)
• Unstructured clinical judgment to be 0.58 (averaged over 12 findings)
More recent meta-analysis AUC predicting sexual recidivism
total of 31 studies, containing 169 effect sizes from 45,673 risk judgments
• Unstructured risk assessment= 0.625 (5 studies)
• Structured risk assessment= 0.721(5 studies)
Evaluating treatment of effectiveness
• Random assignment
• Descriptive
• Risk Band
• Incidental cohort
what was the offense rate
• Statistical control of group differences
• Matched controls
• Within treatment change
how well does groups work in treatment
• Meta-analysis
pull tg exisiting elements and combine the results
Offender is high risk; what questions might you ask?
past history
triggers
mental health conditions
substance use
If you were a clinician who needed to assess someone who had committed a sex offense, what would you do?
early/late onsets
background characteristics
risk assessment measure
What does the risk principle support?
varying the intensity of treatment according to the risk level of the individual
Structured Assessment of Risk and Need-Treatment Needs Analysis (SARN)
a clinical framework used to assess sexual offenders’ risk, need, and progress in treatment; treatment planning tool
SARN process
actuarial risk is first measured using the RM 2000
SARN uses clinical ratings to assess 16 items that measure Thornton’s (2002) four dynamic risk domains
uses a scoring protocol that determines the relevance of each factor both as a proximal factor leading up to the offence, and as a factor in the individual’s life in general
What does the ACUTE-2007 assess?
the risk for both sex/violent recidivism and a total score for risk of general recidivism
Motivation for treatment
it can range from acceptance of accountability for offending to a willingness to attend treatment
Random Assignment/Randomized Control Trials
offenders are randomly placed in either a group that will receive treatment, or a no treatment control group
provide the most conclusive evidence for treatment effects
controls any pre-existing (known and unknown) differences that exist between the groups
observed differences can be attributed to treatment. Any differences that are evident between the groups occur by chance
Limitations of Random Assignment/Randomized Control Trials
there is still the risk of differential attrition between the treatment and control group, posing a threat to the internal validity of the study
expensive to conduct
practical issues arise that include the likely unwillingness of most large institutional systems to approve of the random allocation of dangerous sexual offenders to a non-treatment group for various reasons related to the real life implications of such a decision
Descriptive
simply followed a group of treated offenders and reported recidivism rates without any comparison to a group of untreated offenders
Risk Band Analysis
compare the observed recidivism rates of the treated group to the rates of reoffence predicted by published risk assessment measures
does not require a comparison group to be created and allows for examination of risk level by treatment interaction
Limits: lack of a control group poses a threat to internal validity because it does not allow for the examination of the effect of no treatment
Incidental Cohort Designs
compare treated offenders with a comparison group of offenders who did not receive treatment for reasons that are not likely to be related to risk level
can confound treatment effects with the time of measurement.
Statistical control of group differences
allows treated and untreated groups to be compared even if they are found to differ on important risk factors
Matched comparison groups
matching the offenders who attended treatment, with those who did not, on factors related to recidivism
Within-treatment Change
Looking at whether or not the group members demonstrate changes in the areas that they are meant to demonstrate change in(i.e., areas targeted in treatment) is a useful way of examining the relationship between treatment effectiveness and reconviction
avoids problems with cohort, jurisdiction, selection bias, and differences in follow-up because all offenders in the study begin at approximately the same time
Limits:
Studies looking at change within treatment alone (i.e., without relating them to recidivism) cannot provide evidence on their own for the effectiveness of treatment due to lack of an untreated comparison group.
They are also often limited by the quality of the psychometrics tests that are used to evaluate the changes.
Comparison of Approaches
designs quantitatively combine the results from a number of studies to determine if there is an overall effect amongst the studies as a whole
allows for even small effect sizes to be detected given the large sample size that results from amalgamating a number of studies