Looks like no one added any tags here yet for you.
A 57-year-old male presents with the main complaint of neck pain. He first noticed the pain yesterday morning and rates the pain as 7 out of 10. Physical examination reveals a narrow band of tight, ropey muscle that extends from the superior nuchal line to the lateral aspect of the clavicle and acromion. What muscle is most likely exhibiting dysfunction? \n \n A. Levator scapulae \n B. Rhomboid major \n C. Rhomboid minor \n D. Teres minor \n E. Trapezius
E – Trapezius! Questions asking attachments of back muscles are common on COMLEX!
A 24-year-old male presents to the office with the chief complaints of right sided occipital headaches. He claims he first noticed the headaches about 2 weeks ago and claims they have not resolved. Physical examination reveals (on the right) tight, ropey muscle in the suboccipital region and burning pain along the posterior aspect of his scalp. Which of the following muscles is most likely exhibiting dysfunction? \n \n A. Obliquus capitis superior \n B. Rectus capitis posterior minor \n C. Semispinalis capitis \n D. Splenius capitis \n E. Splenius cervicus
C – Semispinalis capitis – Remember the greater occipital n (aka posterior ramus of C2) passes through the semispinalis capitis muscle and can cause a compressive neuropathy of this nerve. Also, this is ultra-high yield for COMLEX!
For each reflex, indicate the correct sensory ganglion/ganglia involved. Answers given below. \n \n A. Pupillary light reflex \n B. Corneal reflex \n C. Jaw jerk reflex \n D. Gag reflex \n E. Biceps reflex \n F. Cremaster reflex \n G. Patellar reflex \n H. Calcaneal reflex \n I. Micturition reflex \n J. Anal wink reflex
A. Retina (is essentially a ganglion) \n B. Trigeminal ganglion \n C. Mesencephalic nucleus (it’s not trigeminal…details March 2022!) \n D. Inferior ganglion of CN IX \n E. DRG C5-6 \n F. DRG L1-2 \n G. DRG L2-4 \n H. DRG S1-2 \n I. DRG S2-4 \n J. DRG S2-4
A 25-year-old female presents to the office with the chief complaints of weakness and numbness in her right upper extremity. Her history is significant for falling asleep sitting up in a chair last night; she claims that she first noticed the sensory loss and weakness when she woke up this morning. Physical examination reveals numbness in the skin overlying her first dorsal interosseous on the right. Her muscle stretch reflexes in her upper extremities are globally 2/4, except for 1/4 for her right triceps reflex. Muscle strength testing reveals (on the R): \n \n Shoulder abduction: 5/5 \n Elbow flexion: 5/5 \n Elbow extension: 4/5 \n Wrist flexion: 5/5 \n Wrist extension: 4/5 \n \n Which of the following nerves is most likely injured? \n \n A. C8 & T1 spinal nerves \n B. Lateral cord of brachial plexus \n C. Medial cord of brachial plexus \n D. Median nerve \n E. Musculocutaneous nerve \n F. Radial nerve \n G. Ulnar nerve
F – Radial nerve. Remember the radial nerve is a direct continuation of the posterior cord of the brachial plexus (it is located posteriorly in the axilla) and is at risk of compression with poorly fit crutches or “Saturday Night Palsy”. Also, she has weakness in UL extensors with no effect of shoulder abduction, so its gotta be radial n!
Radiographs from a 33-year-old male who injured himself while weightlifting reveals an avulsion fracture of the greater tubercle of the humerus. The avulsed bony fragment is displaced superiorly. What muscle is most directly responsible for the displacement of this fragment? \n \n A. Coracobrachialis \n B. Deltoid \n C. Levator scapulae \n D. Pectoralis minor \n E. Subscapularis \n F. Supraspinatus \n G. Teres major
F – The supraspinatus attaches to the greater tubercle and would pull the avulsed fragment superiorly. USMLE likes to ask about displaced bone fragments because you must know both attachment and muscle action to get it correct!
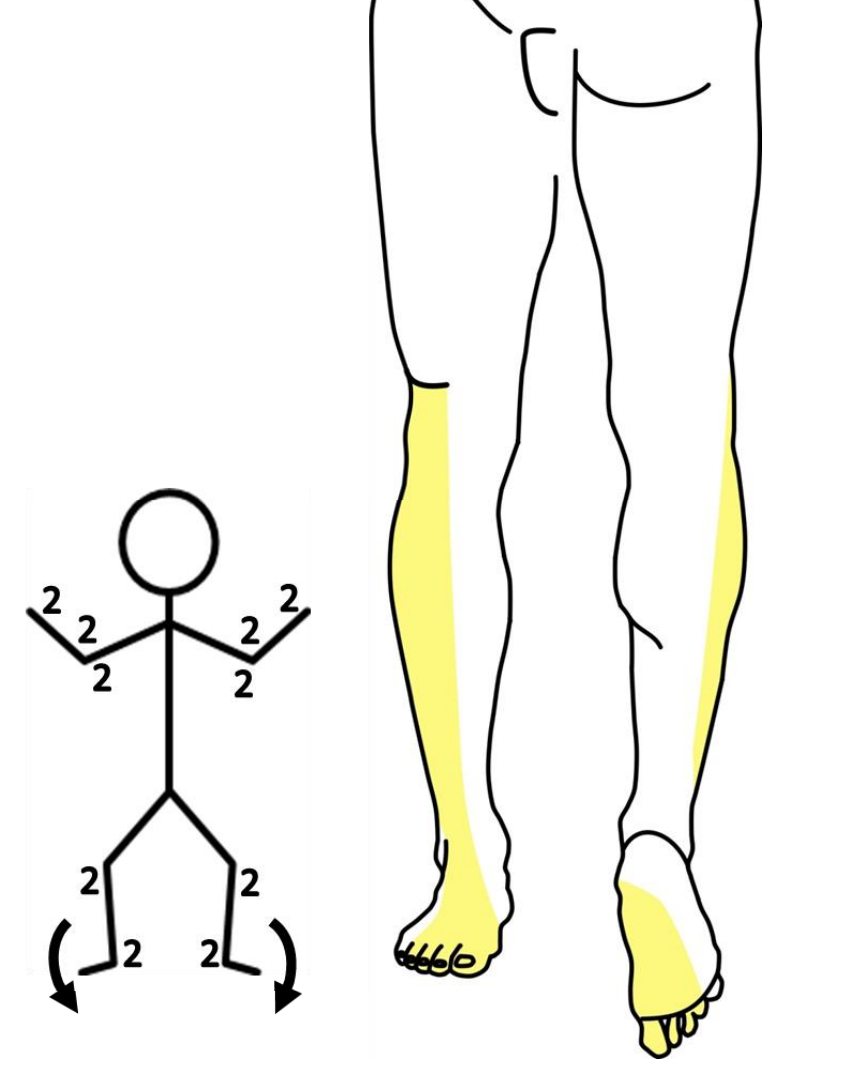
A 17-year-old male presents to the emergency room after getting hit by a car. Physical examination reveals he was hit just below the left knee. Radiographs reveal a fracture involving the proximal end of his left fibula. \n \n 1. What nerve is injured? _______________ \n \n 2. Sensation is intact (Y) or impaired (N) over the: \n Medial malleolus ___ \n Lateral malleolus ___ \n \n 3. Expected strength (on the left) in: \n Dorsiflexion = ___ \n Plantar flexion = ___
1. The common fibular nerve courses over neck of the fibula and is most likely injured. \n 2. The common fibular (and its branches: superficial and deep fibular nerves) do not supply skin over the medial or lateral malleolus. So, sensation is intact at both locations. Bonus: What nerves supply the skin here? (answer below even further) \n 3. The deep fibular nerve supplies the muscles in the anterior compartment of the leg. These muscles are used for dorsiflexion – so this action would be weak. The tibial nerve controls plantar flexion – this would be normal.
A 59-year-old female presents to the office with the chief complaint of difficulty walking and weakness in her right lower extremity. Her history is significant for poorly controlled diabetes. She claims her weakness has gotten progressively worse over the past 5 days and that she has the most difficulty rising from her chair and going up her front stairs. Physical examination reveals atrophy and fasciculations in the right gluteal region. She has 3/5 strength in extension of her right thigh. Her strength is 5/5 on the left. She has diminished pin prick sensation over her medial and lateral malleolus, bilaterally. Which of the following muscles is exhibiting dysfunction? \n \n A. Gluteus maximus \n B. Gluteus medius \n C. Piriformis \n D. Quadratus femoris \n E. Tensor fascia lata
A – Gluteus maximus extends and laterally rotates the femur and is innervated by the inferior gluteal nerve (L5-S2). She would have a gluteus lurch: http://www.youtube.com/watch?v=_HsgM_00q_c \n Her sensory loss is consistent with diabetic polyneuropathy.
A 59-year-old female is seen for back pain and lower limb weakness of two-months duration. Physical exam reveals sensory loss and weakness in both lower extremities. An MRI series of her vertebral column reveals the image to the right.
The rightward pointing arrows indicate two vertebral bodies with a defective intervertebral disk in-between. Which of the following most correctly indicates the vertebrae indicated?
A. L2 + L3
B. L3 + L4
C. L4 + L5
D. L5 + S1
E. S1 + S2
C. The rightward pointing arrows indicate the bodies of L4 and L5. Remember the sacrum curves anteriorly (its concave) and S1 is at the top (superior aspect) of this curve. So the sacral promontory is a great indicator for S1 – use this to count your vertebra.
A 59-year-old female is seen for back pain and lower limb weakness of two-months duration. Physical exam reveals sensory loss and weakness in both lower extremities. An MRI series of her vertebral column reveals the image to the right.
The upward pointing arrow indicates a pathological mass. Which of the following structures is most directly affected by the mass?
A. Anterior longitudinal ligament
B. Cauda equina
C. L4 spinal cord segment
D. S1 spinal cord segment
E. Sympathetic chain
B. Remember the spinal cord terminates at L2. So there is no spinal cord at the level indicated. The anterior longitudinal ligament and sympathetic chain are anterior or anterior-lateral to the vertebral bodies.
A 66-year-old male presents to his primary care physician complaining of ongoing lower back pain. Upon further questioning, the patient admits to weakness and numbness in his left leg. Physical examination reveals a positive straight leg test, and on the left, weakness in hip flexion and adduction and weakness in knee extension. He has diminished sensation along his medial thigh on the left. His left patellar reflex is 1/4 and his left calcaneal reflex is 2/4. All other muscle stretch reflexes are 2/4. Results from an MRI study are pending. Imaging will most likely reveal a herniation between which two vertebrae?
A. L1-L2
B. L2-L3
C. L3-L4
D. L4-L5
E. L5-S1
B. Positive straight leg test = disc herniation. Weakness in knee extension could be = L2, 3, 4 or femoral n, but we ruled out femoral n with straight leg test. His sensory loss is along his medial THIGH – this is consistent with the L3 dermatome.
A 56-year-old male presents to his primary care physician with the chief complaint of right-hand weakness after a recent job that required extensive use of a screwdriver. Physical examination reveals intact sensation throughout his right upper extremity and 2/4 reflexes globally. Results of strength testing in his right upper extremity are listed below.
-Shoulder abduction: 5/5
-Shoulder adduction: 5/5
-Elbow flexion: 5/5
-Elbow extension: 5/5
-Wrist flexion: 5/5
-Wrist extension: 3/5
-Finger flexion: 5/5
-Finger extension: 3/5
-Finger abduction/adduction: 5/5
Which of the following nerves is most likely to have been injured in this patient?
A. Posterior cord in the axilla
B. Radial nerve at the midshaft humerus
C. Deep branch of radial nerve in supinator canal
D. Superficial branch of radial nerve deep to brachioradialis muscle
E. Ulnar nerve in cubital tunnel
F. Ulnar nerve in Guyon’s tunnel
G. Median nerve between the heads of pronator teres muscle
H. Recurrent branch of the median nerve in hand
C. The pt has weakness in wrist and finger extension. He has none sensory loss. The radial n does all the extensors, but the lack of sensory findings means the lesion is distal to the split of radial n into superficial and deep branches. The superficial br is only sensory (review cheiralgia paresthetica). FYI, we like lists of muscle strength like this on COMLEX.
A 48-year-old male presents to the office with the chief complaints of numbness in his right lower extremity and difficulty walking. He claims that he first noticed these issues about 4 weeks ago and they have not improved. His muscle stretch reflexes are globally 2/4. Muscle strength is 5/5 in his left lower extremity. Muscle strength testing in his right lower extremity reveals the results provided below:
Hip extension 3/5
Hip flexion 5/5
Knee extension 5/5
Knee flexion 3/5
Dorsiflexion 2/5
Plantarflexion 5/5
Which of the following is the most likely diagnosis?
A. L4 radiculopathy
B. L5 radiculopathy
C. Entrapment of tibial nerve by tendinous arch of soleus
D. Entrapment of tibial nerve in tarsal tunnel
E. Femoral nerve mononeuropathy
F. Sciatic nerve mononeuropathy
B. The patient has normal reflexes - this immediately rules out L2-4, S1-2, femoral and sciatic nerves. He does have weakness in hip extension (glut max, inf glut n, L5-S2) and knee flexion (hammies, sciatic, L5-2) and dorsiflexion (tib ant, sciatic/com fib/deep fib, L5). L5 is common to all these things.
A 37-year-old female presents to the office with the chief complaints of numbness in her right hand and weakness in her right upper extremity. She claims she first noticed these issues about 4 weeks ago and claims they have gotten progressively worse. Physical examination reveals sensory loss in the region indicated in the accompanying figure. Strength testing reveals results as follow:
-Elbow extension 3/5
-Elbow flexion 5/5
-Pronation 3/5
-Supination 5/5
-Wrist extension 5/5
-Wrist flexion 4/5
-Finger extension 5/5
-Finger flexion 3/5
Which of the following nerves is most likely injured?
A. C7 spinal nerve
B. C8 spinal nerve
C. Median nerve
D. Radial nerve
E. T1 spinal nerve
F. Ulnar nerve
B. The sensory loss should immediately limit you to C8. Maybe ulnar n, but for ulnar I want to see sensory loss extend to medial half of middle finger and not extend above the wrist. She has weakness in elbow extension (radial n, C7-8), pronation (median, C6-8), wrist flexion (median & ulnar, C7-8), finger flexion (median > ulnar, C8).
Physical examination of a 3-year-old male reveals a continuous machinery murmur along the left 3rd and 4th intercostal spaces about 2 cm lateral to the sternum. An echocardiogram reveals abnormal flow between the aorta and pulmonary trunk. Which of the following is the most likely diagnosis?
A. Coarctation of the aorta
B. Mitral stenosis
C. Patent ductus arteriosus
D. Pulmonic stenosis
E. Transposition of the great vessels
F. Tricuspid stenosis
C is the correct answer! PDA is characterized by a machinery sounding murmur in this location.
Let’s do a quick review of sympathetic levels😊
List the correct spinal cord levels that provide sympathetic innervation to the structures listed below.
A. Internal carotid artery
B. Heart
C. Stomach
D. Midgut
E. Hindgut
F. Bladder
Remember these key points:
1. sympathetics go everywhere. It’s one of “Kulesza’s Law”. And its published: Mansour and Kulesza, 2021
2. the ANS innervates viscera = smooth muscle (arrector pili), cardiac muscle and glands
Answers: Be advised that sympathetic levels are huge on boards for anatomy and OPP! You need to have these memorized!
A. T1-4
B. T1-4
C. T5-9
D. T9-11
E. L1-2
F. L1-2
A 67-year-old male presents with near-complete blockage in his left internal carotid artery. The man elects for an endarterectomy as part of his treatment. Immediately following the procedure, the patient complains of hoarseness. Endoscopic examination of his larynx reveals that his left vocal cord cannot be abducted or adducted. Which of the following nerves was most likely damaged?
A. External laryngeal
B. Internal laryngeal
C. Recurrent laryngeal
D. Superior laryngeal
E. Vagus
E – These surgery/procedure questions are all about relationships and location!
Remember that this procedure is done to clear the internal carotid and the vessel is incised near the carotid bifurcation. Paralysis of the vocal cord indicates weakness in the posterior and lateral cricoarytenoid muscles - both innervated by the recurrent laryngeal nerve. I choose the left side because the recurrent branches from the vagus as this nerve passes over the arch of the aorta. As such, the recurrent is not at risk in this procedure. The vagus, however is situated within the carotid sheath between the carotid and internal jugular vein and is much more likely to be injured.
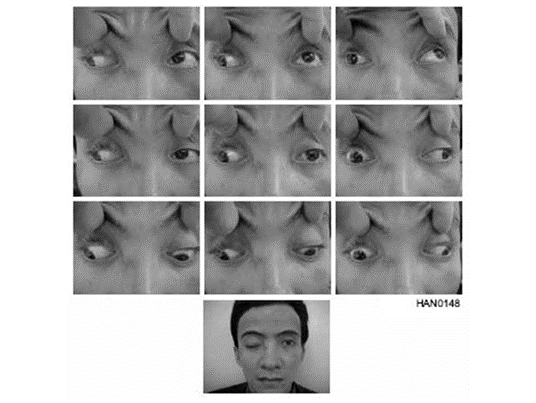
A 50-year-old male presents to the office with the chief complaint of double vision after getting hit in the head with a bowling pin three days ago. Physical examination reveals the findings shown in the accompanying figure. Testing also reveals that the diplopia is worse with leftward gaze. He has normal strength and reflexes in all four extremities; pin prick sensation is normal on his face, trunk and limbs. A CT scan is negative. What muscle is most likely weak or paralyzed?
You will see these nine panel views for testing of eye movements on boards. Promise** Don’t expect buzzword presentations. He has a weak superior oblique muscle on the right. Notice in the bottom right panel, after he adducts his right eye that he cannot fully depress (look down). This is how we test the SO muscle.
A 23-year-old female presents to the office with headaches, ringing/buzzing in her left ear and left eye pain. She has a previous diagnosis of neurofibromatosis. Physical examination reveals a corneal ulceration on the left; her pupils are equal, round and reactive to light. She has papilledema on the left. She has intact sensation on her face but she cannot wrinkle her forehead, close her eye tightly or smile on the left. She notes also that she has some difficulty eating because her mouth is dry and her sense of taste is diminished. Where is the lesion?
A. Facial canal
B. Foramen ovale
C. Internal auditory meatus
D. Jugular foramen
E. Pterygoid canal
F. Stylomastoid foramen
C – All her PE findings point to proximal injury to the facial nerve (all components of CN VII are affected). This is a classic board-style CN VII format! Vestibular Schwannomas are rare but are much more common in patients with neurofibromatosis. Papilledema is associated with increased intracranial pressure (= intracranial mass).
A 34-year-old woman presents to the office with pain in her right foot and difficulty walking. She claims that she first noticed the pain about 3 weeks ago and claims that the pain has gotten progressively worse. Physical examination reveals pain/tingling along the plantar aspect of her foot, including the tips of all toes; she has normal sensation on her heel. Her muscle stretch reflexes are globally 2/4. She has 5/5 muscle strength in dorsi and plantarflexion. An EMG study reveals fibrillations in her flexor hallicus brevis, abductor hallicus and abductor digiti minimi. Which of the following is the most likely injury?
A. Entrapment of deep fibular nerve along dorsum of foot
B. Entrapment of tibial nerve in tarsal tunnel
C. Injury to common fibular nerve at fibular neck
D. Injury to tibial nerve in popliteal fossa
E. L5 radiculopathy
F. S1 radiculopathy
Answer is B. Remember that with nerve injuries, the deficits have to be distal to the injury. In this case, all her deficits are distal to the tunnel.
A 44-year-old (gravida 2, para 2) female presents to the office with the chief complaints of pelvic and back pain, difficulty urinating and painful intercourse. She claims that when she defecates, she feels a mass in her vagina. Physical examination reveals that, during Valsalva maneuver her cervix protrudes about 4 cm inferiorly into her vaginal canal. Which of the following structures is most likely exhibiting dysfunction?
A. Broad ligament
B. Perineal body
C. Round ligament
D. Sacroiliac ligament
E. Transverse cardinal ligament
F. Uterosacral ligament
B – This is one of the more popular USMLE pelvis questions. The perineal body is the central tendon of the perineum! The most important structures in support of pelvic organs are the pelvic diaphragm, UGD and perineal body. See uterine prolapse in the Clin Supp (Pelvis & Perineum, #23).
Referred pain from a gastric ulcer is carried by which of the following neuron types?
A. GVAs with cell bodies in the celiac ganglion
B. GVAs with cell bodies in the posterior root ganglia
C. GVAs with cell bodies in the sympathetic chain
D. GVEs with cell bodies in the anterior horn
E. GVEs with cell bodies in the IML
F. GVEs with cell bodies in the posterior root ganglia
Viscero-somatic changes resulting from a gastric ulcer will most likely be identified in what dermatome/myotome?
A. C1-2
B. T1-4
C. T5-9
D. T10-11
E. T12
F. L1-2
G. S2-4
B – Visceral afferents carry pain from organs and always have a pseudounipolar cell body in a sensory ganglion
C – Foregut is T5-9
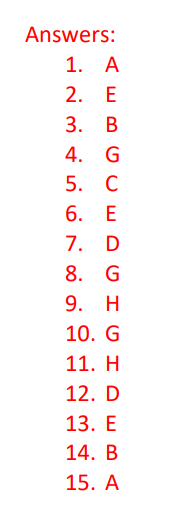
Answers and labeled image below.
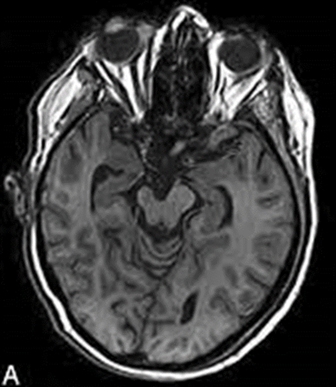
Imaging from a 22-year-old male with weakness reveals the result shown in the accompanying image. What structural abnormalities are observed?
Cerebellar herniation (Chiari malformation)
Syringomyelia
Do these after the somatosensory lecture today!
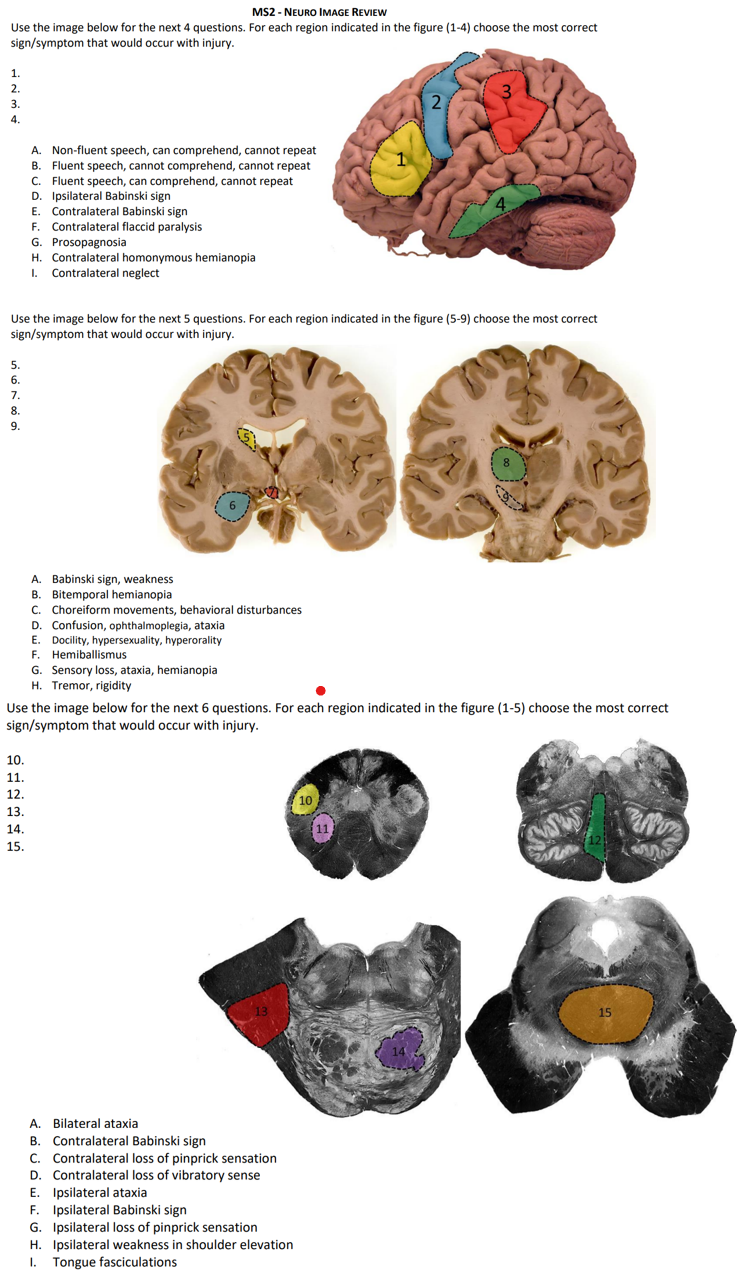
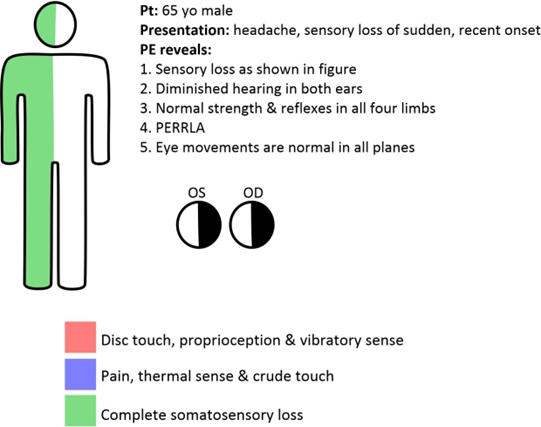
Match the signs and symptoms to the most correct lesion site.
1. Loss of vibratory sense on R UL, trunk and LL + left CN XII palsy
2. Loss of vibratory sense on R UL, trunk and LL + left CN VI palsy
3. Loss of pinprick sense on R face and L UL, trunk and LL + sagging palate
4. Loss of pinprick and vibratory sense on R UL, trunk and LL
5. Loss of pinprick and vibratory sense on R face and UL
A. Left cerebral cortex
B. Left lateral medulla
C. Left medial medulla
D. Left medial pons
E. Left thalamus
F. Right cerebral cortex
G. Right lateral medulla
H. Right medial medulla
I. Right medial pons
J. Right thalamus
C
D
G
E…could also be a large cortical lesion
A
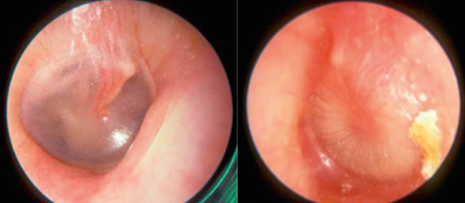
A 10-year-old male presents to the office with fever, ear pain and diminished hearing in his left ear. Physical examination reveals an opaque and yellowish tympanic membrane that is bulging into the external meatus.
The Weber test will most likely be localized to the:
A. left ear
B. right ear
C. midline
A
A 10-year-old male presents to the office with fever, ear pain and diminished hearing in his left ear. Physical examination reveals an opaque and yellowish tympanic membrane that is bulging into the external meatus.
The Rinne test, on the left side, will most likely reveal:
A. A > B
B. A < B
C. Deafness
B
A 10-year-old male presents to the office with fever, ear pain and diminished hearing in his left ear. Physical examination reveals an opaque and yellowish tympanic membrane that is bulging into the external meatus.
The boy has:
A. Otitis externa and conductive hearing loss
B. Otitis externa and sensorineuronal hearing loss
C. Otitis media and conductive hearing loss
D. Otitis media and sensorineuronal hearing loss
E. Presybcusis and conductive hearing loss
E. Presybcusis and sensorineuronal hearing loss
F. Tinnitus and conductive hearing loss
G. Tinnitus and sensorineuronal hearing loss
C
Student Doctors – Have I ever mentioned that MSK is gonna be huge? Answers below.
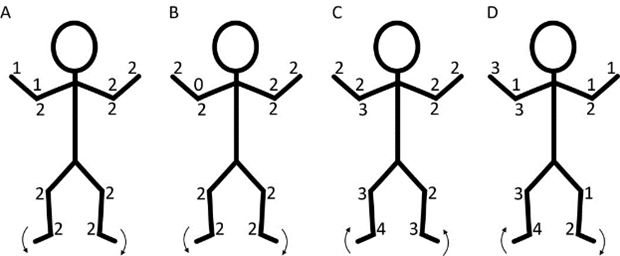
Match the patient presentation with the expected muscle strength findings. Answers below.
I. A 24-year-old male with a C6 radiculopathy
II. A 16-year-old male with a midshaft fracture of the humerus
III. A 38-year-old female with a Pancoast tumor
A Weakness in finger extension
B Weakness in finger flexion and finger abduction
C Weakness in elbow flexion
D Weakness in shoulder abduction, elbow flexion
E Weakness in shoulder abduction, elbow extension, finger extension
MSK is gonna be HUGE, parts 2!
IV. Can you give the key signs and symptoms for the following injuries?
A. Carpal tunnel syndrome
B. C6 radiculopathy
C. Ulnar nerve injury in cubital tunnel
D. Erb’s palsy
E. Klumpke palsy
F. L5 radiculopathy
G. S1 radiculopathy
H. sciatic mononeuropathy (injury in gluteal region)
I. meralgia parestheica
J. tarsal tunnel syndrome
Part 1
I. D – C6 innervates the deltoid, biceps AND brachioradialis reflexes
II. A – radial nerve = extensors
III. B – T1 radic
Part 2 (IV)
A. Carpal tunnel syndrome: weakness of thenar muscles, sensory loss on palmar aspect of digits 1-3, sensation over thenar eminence is intact!
B. C6 radiculopathy: sensory loss over lateral forearm, thumb and index finger (dorsum and palmar), diminished biceps and/or brachioradialis reflex; diminished strength in shoulder abduction, elbow flexion, wrist extension
C. Ulnar nerve injury in cubital tunnel: remember the cubital tunnel is behind the medial epicondyle (not the same as the cubital fossa; compare to injury at Guyon’s tunnel); slight clawing of digits 2-5 (slight because of paralysis in FCU and medial ½ half of FDP), radial deviation of wrist upon attempted wrist flexion, Froment’s sign, sensory loss over dorsal and palmar aspect of digits 4 and 5
D. Erb’s palsy: damage to C5 and C6 = arm held in adduction (abductors are paralyzed), arm medial rotated (lateral rotators paralyzed), extended at elbow (elbow flexors paralyzed), wrist held in slight flexion (wrist extensors paralyzed), sensory loss in C5 and C6 dermatomes
E. Klumpke palsy: complete claw hand (paralysis of all intrinsic hand muscles), sensory loss in C8 and T1 dermatomes
F. normal patellar and calcaneal reflexes (2/4); weakness in EHL, EDL, can’t walk on heel/weakness in dorsiflexion, sensory loss on dorsum of foot
G. diminished calcaneal reflex, weakness and atrophy in fibularis longus, Glut Max + gastroc, sensory loss along lateral foot
H. weakness/paralysis of hamstrings and all muscles below the knee, diminished calcaneal reflex, sensory loss along lateral and posterior leg + foot
I. numbness/burning pain along lateral aspect of thigh, no weakness (lat femoral cut n)
J. pain/tingling/burning/numbness along plantar foot, weakness in intrinsic foot muscles, normal Achilles reflex
A PET scan from a 50-year-old male with a recent diagnosis of prostate cancer reveals metastasis to his lumbar vertebrae. Which of the following indicates the most likely route of metastasis?
A. Aorta
B. Inferior vena cava
C. Local spread
D. Portal system
E. Thoracic duct
F. Vertebral venous plexus
Remember, cancer spreads by 3 main mechanisms:
1. Local spread
2. lymphatic channels
3. venous >> arterial channels
The vertebral venous plexus (aka Batson’s plexus) is a network of valveless veins that connect pelvic veins to veins draining the vertebral column and permit venous spread of cancer or infections from pelvic organs to the vertebral column and/or the brain. Breast cancer can also spread to the vertebral column through these veins.
A 48-year-old female presents to the office with chief complaints of headache, difficulty walking and vision loss. She first noticed the difficulty seeing when she backed into a parked car 3 days ago; she claims she has had difficulty walking for about the last 3 weeks. Her history is significant for a diagnosis and treatment of infiltrating ductal carcinoma in her left breast two years ago. A PET scan of her brain reveals a four 3 cm masses in her cerebellum and a 2 cm mass in her left occipital lobe. Which of the following vessels was most likely involved in metastasis from the primary neoplasm in her left breast?
A. Inferior vena cava
B. Internal carotid artery
C. Internal jugular vein
D. Internal thoracic artery
E. Middle cerebral artery
F. Portal vein
G. Superior epigastric artery
H. Vertebral artery
Cancerous cells from the breast reach the lung through the venous system (azygos system) and can also reach the vertebral column and brain through the intervertebral plexus (Baton’s plexus). However, these veins are not answer choices. If there are secondary tumors in the lung, these can spread through the pulmonary veins to the heart and then through the ascending aorta. We are reaching the posterior fossa through vertebral arteries.
A 43-year-old male presents to the office with the chief complaints of right hip pain and difficulty walking. He claims that he first noticed the pain about 1 week ago after a 10-mile run. The pain was exacerbated by a 6-mile run yesterday morning. Physical examination of the patient’s right lower extremity reveals marked tenderness over the greater trochanter; ultrasound examination reveals tendonpathy and bursitis at this site. The tendon of what muscle is exhibiting dysfunction?
A. Gluteus medius
B. Psoas major
C. Rectus femoris
D. Sartorius
E. Tensor fasciae latae
Basically, what muscle attaches to the greater trochanter – Gluteus medius. FYI - the most important muscle attachment sites are found in the Anatomy Clinical Supplement.
A 22-year-old female presents to the office with the chief complaint of right elbow pain. She claims that she first noticed this pain 3 days ago after playing racquetball. Physical examination reveals pain and tenderness over her lateral epicondyle on the right. She has intact pinprick sensation in her right forearm and hand. She has significant pain in wrist extension against resistance. This patient’s condition involves the attachment of which of the following muscles?
A. Abductor pollicis longus
B. Brachioradialis
C. Extensor carpi radialis brevis
D. Extensor indicis
E. Extensor pollicis longus
F. Supinator
The answer is C. The patient has lateral epicondylitis. This involves inflammation at the common extensor tendon (attachment of extensor carpi radialis brevis, extensor digitorum, and extensor digiti minimi). This condition can result in compression of the posterior interosseous nerve. This nerve innervates EI, APL, EPL and EPB but has no cutaneous distribution
A 20-year-old male presents to the emergency room with the chief complaints of right hip pain after an automobile accident. He was a passenger in the front seat during a head-on collision with a telephone pole. He is unable and unwilling to attempt weight bearing on his right lower extremity. Physical examination reveals his right leg is shorter than the left and his lower limb is held in a position of internal rotation and adduction.
What is the most likely diagnosis?
A. Anterior, inferior hip dislocation
B. Anterior, superior hip dislocation
C. Posterior hip dislocation
D. Midshaft femur fracture
E. Rupture of the ilopsoas tendon
These dislocation and position questions like to show up on USMLE!
Answer is C. When the femoral head is dislocated posteriorly, the normal muscle tone in the medial rotators rolls the femur medially/internally and the adductors pull the femur medially. With anterior dislocations, the femur is externally rotated.
A 20-year-old male presents to the emergency room with the chief complaints of right hip pain after an automobile accident. He was a passenger in the front seat during a head-on collision with a telephone pole. He is unable and unwilling to attempt weight bearing on his right lower extremity. Physical examination reveals his right leg is shorter than the left and his lower limb is held in a position of internal rotation and adduction.
Which of the following muscles is most directly responsible to the posture of internal rotation?
A. Gluteus maximus
B. Gluteus medius
C. Piriformis
D. Psoas major
E. Rectus femoris
These dislocation and position questions like to show up on USMLE!
B. it’s the only medial rotator
A 64-year-old female presents to the emergency room with vision loss in her left eye. She claims that she first noticed the vision loss about 60 minutes ago but claims that she can see normally now. She describes the episode of vision loss as sudden and that it involved the entire left visual field. Her history is significant for diabetes mellitus and hypertension. A CT angiogram will most likely reveal a blockage in which of the following arteries?
A. Basilar
B. Facial
C. Internal carotid
D. Maxillary
E. Posterior cerebral
F. Vertebral
A transient ischemic attack affecting vision is known as amaurosis fugax (passing darkness). It is indicative of a blockage in the internal carotid artery and is a sign of an impending stroke.
A 28-year-old female presents to the office with vision loss, difficulty walking and double vision. She claims that she has had some difficulty walking for about 2 weeks, but she noticed the vision loss 2 days ago. She notes that she had an episode of vision loss last year that resolved after 2 days. Physical examination reveals a right scotoma and reduced vibratory sense in her left upper and lower extremities. Pin prick sensation is globally intact. She has difficulty with finger to nose testing bilaterally. She has a Babinski sign on the left. Which of the following is the most likely diagnosis?
A. Amyotrophic lateral sclerosis
B. Guillain-Barre syndrome
C. Multiple sclerosis
D. Spondylosis
E. Subacute combined degeneration
F. Transverse myelitis
The answer is C.
ALS – characterized by both upper and lower motor neurons signs. No sensory loss
GB – post infection, symmetric ascending weakness
MS - relapsing/remitting signs and symptoms commonly include vision loss (**See Neuro supplement for PE, MRI and lab findings!**)
Spondos – s/s localized to spinal cord levels or multiple nerve roots
SCD – B12 deficiency (cobalamin), affects posterior columns and corticospinal tracts
Transverse myelitis – looks like spinal cord transection
A 67-year-old female presents with the chief complaints of headaches of 2-months duration and visual loss as shown in the accompanying figure. Which of the following is the most likely etiology?
A. Aneurysm, left middle cerebral artery
B. Aneurysm, right middle cerebral artery
C. Craniopharyngioma
D. Infarct in thalamus
E. Infract in optic radiation
F. Multiple sclerosis
G. Optic neuritis
B…this is a lateral compression of the R optic nerve near the chiasm (likely from an MCA aneurysm). This compresses all of the axons coming from the right eye and some (not all) of the crossing fibers from the left
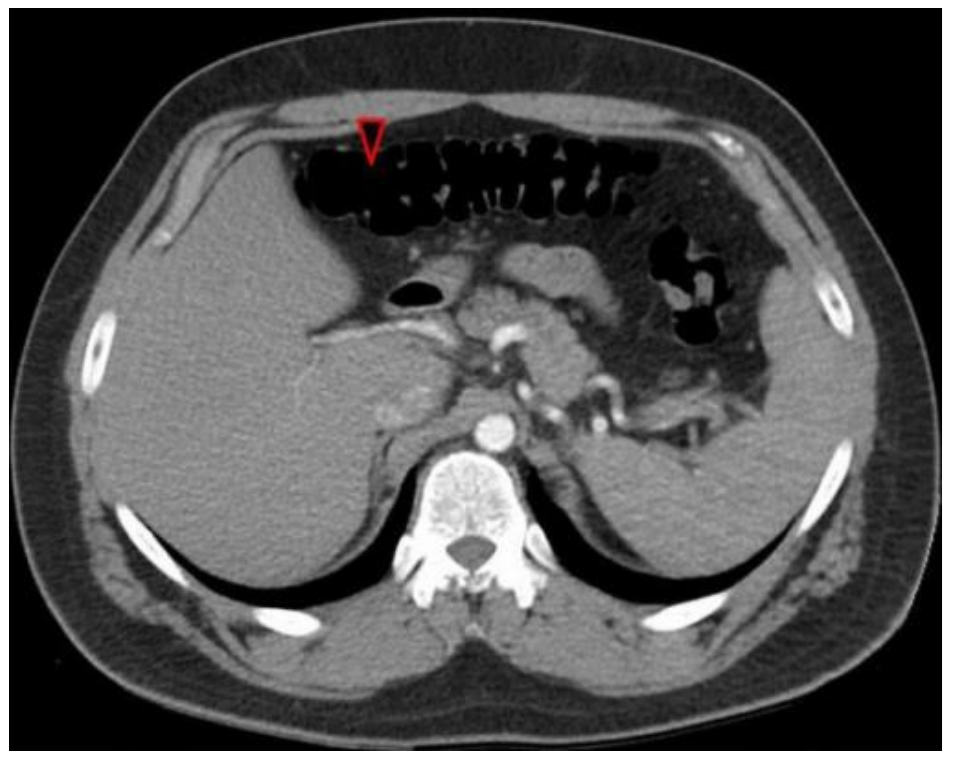
Microscopic examination of H&E-stained sections from a retroperitoneal lymph node from a 59-year-old male with abdominal pain, rectal bleeding and multiple abdominal masses on CT reveals the results shown in the accompanying image. The region indicated by the dashed circle is shown at higher magnification to the right.
What is the most likely diagnosis?
metastatic adenocarcinoma, mucinous type
None of the normal features of a lymph node are evidence. The node has been completely invaded by cancerous cells. This section shows a nice strip of simple columnar epithelium (like you might see in the colon!) that has secreted a clump of mucous material. This is a case we had in the anatomy lab recently. It is a confirmed primary tumor in the ascending colon, with metastasis to peritoneum, superior mesenteric nodes (shown in the image), liver and lung.
A 54-year-old male presents with neck pain and progressive weakness in his left upper extremity. A CT series of his cervical spine reveals stenosis of the intervertebral foramen (on his left side) between C4-C5 and C5-6.
i.) Which of the following muscles is most likely to be completely paralyzed?
A. Biceps brachii
B. Flexor carpi radialis
C. Pectoralis major
D. Serratus anterior
E. Triceps brachii
ii.) Over which of the following bony landmarks will there be decreased cutaneous sensation?
A. 1st metacarpal
B. Medial epicondyle
C. Olecranon
D. Pisiform
E. Ulnar styloid
i.) A
The stenosis compresses C5 and C6 spinal nerves. Paralyzed and weak are not the same thing. Remember for muscles to be paralyzed they need to have completely disrupted innervation. For a muscle to be paralyzed with radiculopathies, all roots supplying a muscle need to be involved.
ii.) A
Biceps brachii is innervated by C5 and C6. Other answers could be deltoid, brachioradialis. Also, the C6 dermatome is over the thumb.
A 40-year-old male presents with a recent diagnosis of a spinal meningioma compressing multiple anterior roots extending from T5 - T7, on the left. He has complete sensory loss beginning 2 cm inferior to his left nipple and extending to ~4 cm superior to his umbilicus on the left. Which other sign/symptom will most likely be found on physical examination?
A. Anhidrosis on left hand
B. Miosis
C. Mydriasis
D. Ptosis
E. Ulnar claw
F. Urinary incontinence
G. Weakness in abduction of the left upper extremity
A = preganglionic sympathetic innervation to the upper limb arises from T2 - T7 spinal cord levels. See the Clinical Supplement and the sympathetic + parasympathetic master tables for summary of ALL autonomic levels. Sympathetic levels are an ultra high yield topic on COMLEX.
A 64-year-old female presents to the emergency room with sudden onset weakness. She claims she first noticed this about 45 minutes ago. Physical examination reveals that her pupils are equal, round and reactive to light; her eye movements are normal in all cardinal planes. She can wrinkle her forehead symmetrically, but she cannot smile on the left. On attempted protrusion, her tongue deviates to the left. Pinprick and proprioception are globally intact. Strength testing reveals the following:
Left Right
Elbow flexion 0 5
Dorsiflexion 0 5
She has a Babinski sign on the left.
a.) Imaging will most likely reveal an infarct in which of the following locations? \n \n A. Internal capsule, left \n B. Internal capsule, right \n C. Medulla, left \n D. Medulla, right \n E. Midbrain, left \n F. Midbrain, right \n G. Pons, left \n H. Pons, right
b & c.) What 2 arteries supply the affect region?
a.) 5. The answer is B. This is a "pure motor" stroke in the internal capsule (affecting corticospinal and corticobulbar axons, inferior to where the thalamocortical axons [sensory] enter) on the right. The fact that all her motor signs are on the left and she has normal eye movements should tell you the lesion is on the right and rostral to the midbrain.
b.). lenticulostriate
c.) anterior choroidal
A 14-year-old male presents to the emergency room following an all-terrain vehicle accident. He is alert and oriented to person, time and place. History reveals that he landed on the right side of his head. Physical examination reveals muscle strength as indicated:
Shoulder abduction 1/5
Shoulder adduction 3/5
Elbow flexion 0/5
Elbow extension 5/5
Wrist extension 3/5
Wrist flexion 5/5
He has fasciculations in his deltoid muscle on the right side. He has complete sensory loss along the lateral aspect of his right arm and forearm and both the posterior and palmar aspect of his thumb. He has normal sensation on the dorsum of both feet. Which of the following structures is most likely damaged? \n
A. C5 & C6 posterior rami
B. C5 & C6 posterior roots
C. Left corticospinal tract
D. Medial cord of the brachial plexus
E. Musculocutaneous nerve
F. Posterior cord of brachial plexus
G. Right corticospinal tract
H. Upper trunk of brachial plexus
H – The signs and symptoms implicate injury to C5 and C6. Posterior rami only innervate deep back muscles and the skin that covers them…the posterior roots include only sensory axons (only GSA @ C5-6) – injury here would not impact strength (reflexes, yes; strength, no). The only answer choice that includes C5 and C6 is the upper trunk of the brachial plexus. Fasciculations (LMN sign!) and the sensory pattern should immediately rule out spinal cord. Spinal cord injuries result in sensory loss from the level of the lesion down the body - here it would involve the UL, trunk and LL.
A 60-year-old male presents to the office with the chief complaints of intermittent bilateral leg pain and weakness. He claims these issues are worst after he has been walking for ~15 minutes but resolve with rest. His femoral pulses are 1/4 bilaterally; his dorsalis pedis and tibial pulses are 0/4, respectively. His brachial pulses are 2/4. A CT angiography series reveals marked stenosis in the infra-renal aorta from L2 to L3.
a.). Which of the following arterial pairs most directly provides collateral circulation around the stenosis in this patient?
A. Deep circumflex iliac & subcostal
B. Inferior phrenic & superior phrenic
C. Lumbar & umbilical
D. Middle sacral & lateral sacral
E. Superior epigastric & inferior epigastric
F. Superior gluteal & inferior gluteal
G. Testicular & inferior vesical
b.) Which of the following arterial pairs most directly permits perfusion of the descending colon in this patient?
A. Gastroduodenal & superior mesenteric
B. Iliolumbar & middle sacral
C. Middle colic & left colic
D. Superior gluteal & inferior gluteal
E. Superior rectal & inferior rectal
F. Testicular & middle rectal
a.) E
b.) C
His leg pain is from claudication. Remember for ANY anastomosis question, collateral supply requires vessels arising (arteries)/emptying (veins) above the blockage to connect to vessels arising (arteries)/emptying (veins) below the blockage. So, the correct answer pair needs to include 1 proximal vessel and 1 distal vessel and they actually need to connect. Because of the level and extent of the blockage in this patient, the lumbar arteries (and their anastomoses with iliolumbar arteries) are not viable options. Beware - anastomosis questions are popular on USMLE!
Patient A: [see accompanying image- red] A 24-year-old male presents to the emergency room after a skateboarding accident with the chief complaint of wrist pain. A radiograph of his wrist reveals the accompanying image. What is the diagnosis?
A fractured ulnar styloid and:
A.) Avulsion fracture of the first metacarpal
B.) Dislocated lunate
C.) Fractured scaphoid
D.) Fractured capitate
E.) Fractured hamate
Patient B: [see accompanying image- blue] A 74-year-old female presents to the emergency room with shoulder pain after a falling down her basement stairs. Physical examination reveals a proximal arm deformity and sensory loss over the lateral aspect of her proximal arm. Radiographs reveal the accompanying image. What muscle is most likely paralyzed?
A.) Biceps brachii
B.) Pectoralis minor
C.) Serratus anterior
D.) Subscapularis
E.) Supraspinatus
F.) Teres minor
Patient A = B [FOOSH injury & most commonly dislocated carpal bone!] Kulesza Pro Tip: If you get a lateral view of a wrist its probably a lunate dislocation. If you only get a frontal view, its probably a scaphoid, or 5th metacarpal fx
Patient B = F [axillary n: also innervates the deltoid :) ]
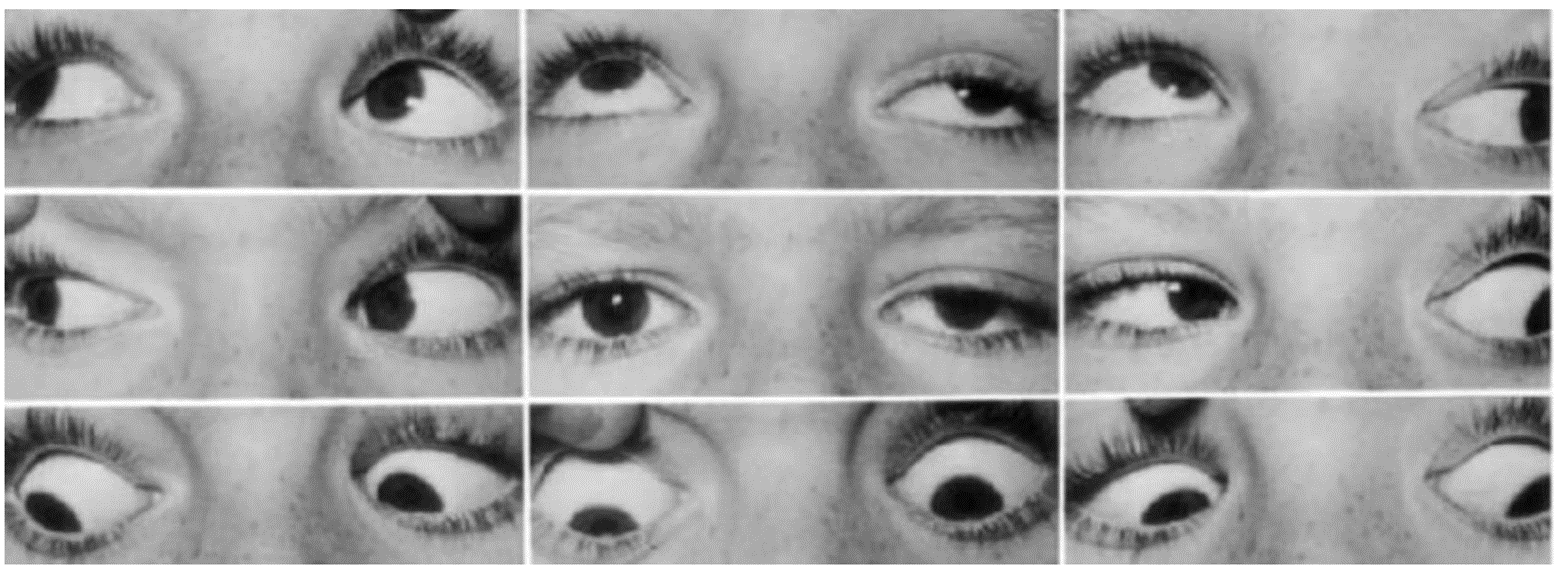
A 17-year-old male presents to the office with the chief complaints of nausea, vomiting, headaches and double vision. His body temperature is 101.5° F (38.6° C). He claims that he has not felt well for the past 2 days after getting hit in the head by a pumpkin. Testing of extraocular muscles reveals the results shown in the accompanying figure (bottom panel = attempted forward gaze). What nerve is most likely injured?
A. Left CN III
B. Left CN IV
C. Left CN VI
D. Right CN III
E. Right CN IV
F. Right CN VI
**Such multi-panel images are commonly used on boards to illustrate diplopia**
This is a case of injury to the right oculomotor nerve (D). Remember, the center panel usually has all the answers! Here, the center panel shows that R eye down and out. Then the bottom panel shows marked ptosis – these 2 provide all the info needed to ID this as a R CN III palsy. Remember, in the 9 panel figure the center image shows front gaze: there are some very good clues in that image – the R eye is directed inferior and lateral (“down and out”) from unopposed action of the LR and SO. His R eye can only abduct. Remember that this sequence is used to **isolate** the action of specific eye muscles. For example: the top right panel shows testing of different muscles in each eye (R eye: abduction + elevation = SR; L eye: adduction + elevation = IO).
A 4-month-old male presents to his pediatrician with the chief indication that he is not using his left upper extremity. His history is significant for a difficult vaginal delivery. Physical examination reveals the boy’s left upper extremity is held in a position of adduction, extension and internal rotation. His grip strength is symmetric. EMG testing reveals fibrillations in the biceps brachi and brachioradialis muscles on the left. Which of the following most correctly indicates the muscles paralyzed in this patient?
A. Infraspinatus, deltoid and brachialis
B. Latissimus dorsi, triceps brachii and pronator teres
C. Pectoralis major, latissimus dorsi and pronator teres
D. Pectoralis major, triceps brachii and lateral 2 lumbricals
E. Trapezius, deltoid and flexor carpi ulnaris
“A” – This is an upper brachial plexus injury (Erb’s palsy), which results in paralysis of muscles innervated by the ventral rami of C5 – C6 (deltoid [can’t abduct], S.I.T.S. [can’t externally rotate], biceps brachii, coracobrachialis and brachialis [can’t flex at elbow]). As a result, the intact muscles are unopposed (namely, pecs, lats, triceps), resulting in a posture of adduction, extension and internal rotation. FYI….he would have sensory loss too (C5 – 6 dermatomes), but the lil’guy can’t tell you.
A 44-year-old female presents to the office on follow up examination from a hysterectomy 1 week prior. She complains of weakness in her left lower extremity and numbness on the inside of her left thigh. Strength testing in her left lower extremity reveals:
Thigh extension: 4/5
Thigh flexion: 5/5
Thigh adduction: 2/5
Her muscle strength is 5/5 throughout her right lower extremity. Her muscle stretch reflexes are globally 2/4. An EMG study reveals fibrillations in her left gracilis muscle, but normal responses in paraspinals, gluteus maximus and vastus lateralis. Which of the following most correctly indicates the affected nerve and the correct spinal cord levels? \n \n A. Common fibular; L2-3 \n B. Common fibular; L5-S2 \n C. Femoral; L2-4 \n D. Femoral; L4-5 \n E. Genitofemoral; L1-2 \n F. Genitofemoral; L4-5 \n G. Obturator; L1-2 \n H. Obturator; L2-4 \n I. Sciatic, L4-S3 \n J. Sciatic, S1-2 \n K. Tibal; L2-4 \n L. Tibial; L4-S3
H; Fun Fact: Obturate = to close or block
Imaging from a 44-year-old male with low back pain over the past 3 months reveals the results shown in the accompanying image. A postero-lateral disc herniation is indicated by the yellow asterisk. Which of the following most correctly indicates the level of the herniation and a sign/symptom that would be consistent with this injury?
A. L3/4; fasciculations in gracilis
B. L3/4; sensory loss over lateral malleolus
C. L4/5; patellar reflex of 3/4
D. L4/5; sensory loss over medial malleolus
E. L5/S1; calcaneal reflex of 1/4
F. L5/S1; fasciculations in vastus medialis
G. S1/2; Trendelburg sign
H. S1/2; urinary incontinence
E: The indicated herniation is between L5 and S1. This will most likely involve S1 and signs/symptoms would be consistent with an S1 radiculopathy. The vastus medialis is innervated by L2-4.
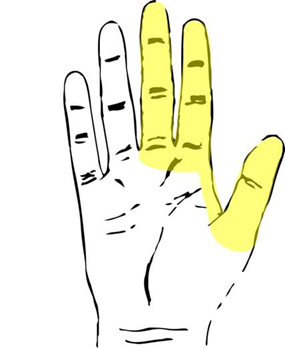
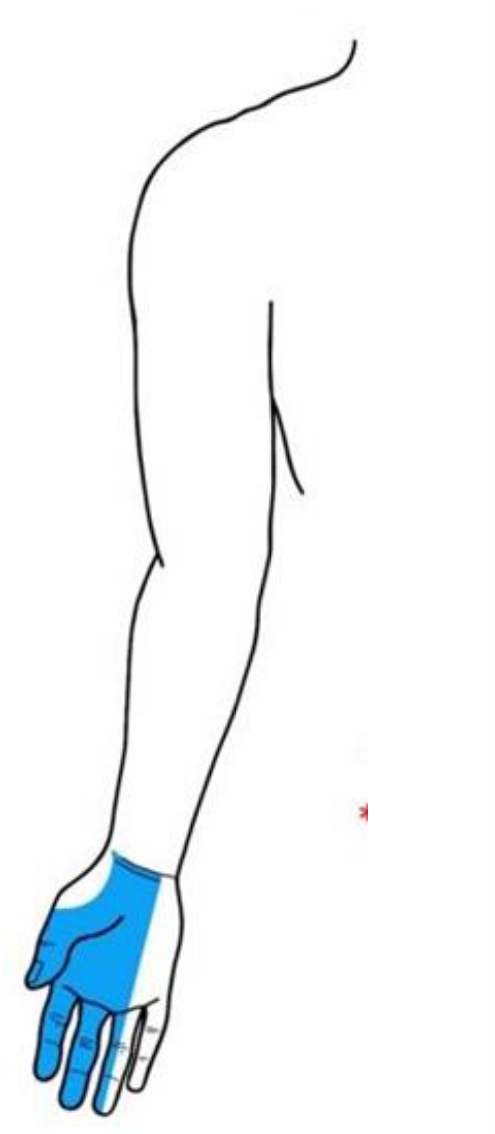
A 48-year-old female presents to the office with tingling and weakness in her right hand. Physical examination reveals her tingling is limited to the region indicated in the accompanying figure. An EMG study reveals +2 fibrillations in the abductor pollicis brevis. What structure is most likely injured?
A.) C5 spinal nerve
B.) C6 spinal nerve
C.) C7 spinal nerve
D.) Median nerve in the axilla
E.) Median nerve in the carpal tunnel
F.) Median nerve in the forearm
G.) Musculocutaneous nerve in the axilla
H.) Radial nerve in the arm
I.) Radial nerve in the forearm
J.) Ulnar nerve in Guyon’s tunnel
K.) Ulnar nerve in the forearm
[E] The palmar branch of the median nerve arises proximal to the carpal tunnel but does not pass through it – it is sparred in carpal tunnel syndrome. Compressions/entrapment of nerves at specific locations is a high yield topic/concept for COMLEX and USMLE! Review UL Nerve Injuries in the Clinical Supplement!
For each reflex, indicate the correct location of the motor (efferent) neurons. Answers given below.
A. Pupillary light reflex
B. Corneal reflex
C. Jaw jerk reflex
D. Gag reflex
E. Biceps reflex
F. Cremaster reflex
G. Patellar reflex
H. Calcaneal reflex
I. Plantar reflex
J. Micturition reflex
K. Anal wink reflex
A. Dilate pupil = Edinger-Westphal à Ciliary ganglion (GVE)
B. Close your eye = Facial nucleus
C. Contract master + temporalis = Trigeminal motor nucleus
D. Pharyngeal constrictors = Nucleus ambiguous
E. Contract biceps = anterior horn, C5-6
F. Elevate testicle = anterior horn, L1-2
G. Contract quadriceps = anterior horn, L2-4
H. Contract gastrocnemius = flex anterior horn, S1-2
I. Contract toes flexors/extensors = anterior horn, S1-2
J. Contract bladder/reflex sphincters = spinal cord, S1-3 à hypogastric plexus/intramural ganglia (GVE)
K. Contract sphincters = anterior horn, S2-4 (Onuf’s nucleus)
A 67-year-old male presents to the office for follow up after suffering a stroke 2-months previous. Physical examination reveals his pupils are equal round and reactive to light and accommodation; all extra-ocular movements are intact. He has a Babinski sign on the left. He can wrinkle his forehead symmetrically but cannot smile on the left. Sensory testing is not performed at this time. An imaging study (administered 2-days ago) reveals the result shown in the accompanying image.
1. What tracts are degenerated in the image?
2. The infarct is in what vascular territory? (3 acceptable answers, give me 1).
1. Corticospinal, corticonuclear….maybe fronto, parietal, occipital, temporopontine (i.e. the corticopontine tracts)
2. The normal eye movements rule out the midbrain as the lesion site. The degeneration in the patient’s right cerebral peduncle (and normal eyes) suggests the lesion is superior to this level - internal capsule, or hemisphere = lenticulostriate, anterior choroidal, MCA main stem
A 16-year-old female presents to the office with the chief complaint of right hip pain. She claims she first noticed this pain about 1 hour ago after jumping over a hurdle. Physical exam reveals tenderness along the lateral aspect of her proximal femur on the right. A radiograph reveals a 2cm by 1 cm avulsion fracture of the greater trochanter. The action of what muscle is most directly responsible for this avulsion? \n \n A. Adductor brevis
B. Adductor longus
C. Adductor magnus
D. Biceps femoris
E. Gluteus maximus
F. Piriformis
G. Psoas major
F. Piriformis.
This is straight up muscle attachments. Lucky for you, there is a list of high yield attachments in your Clinical Supplement (Lower Limb, #4). It won’t surprise you that piriformis is a very popular muscle on COMLEX and you’ll see it in both anatomy and OPP questions. For completeness, there are other muscles that attach to the greater trochanter too - gluteus medius + minimus, obturator internus + externus and the gemelli brothers
Study Tip: Psoas major is also very popular! It attaches to the lesser trochanter and functions in hip flexion and lateral rotation. See also psoas abscess – Clin Supp, Lower Limb, #26.
ANS Review - I’m sure this isn’t a surprise but, ANS will be super high yield on COMLEX and you’ll encounter ANS items in both Anatomy and OPP questions (which together is ~30% of the exam). Answers below.
Fill in the Blank, part 1: Indicate the spinal cord segment(s) that provides preganglionic sympathetic neuronal cell bodies for each of the following structures.
\n 1. Cerebral Vasculature \n 2. Nasal Mucosa \n 3. Heart \n 4. Liver and gallbladder \n 5. Midgut \n 6. Large intestine (through rectum) \n 7. Bladder \n 8. Testes \n \n Fill in the Blank, part 2: Indicate the location of PREGANGLIONIC PARASYMPATHETIC cell bodies for each of the following structures. \n \n 9. Ciliary muscle \n 10. Submandibular gland \n 11. Sublingual gland \n 12. Parotid gland \n 13. Heart \n 14. Midgut \n 15. Kidneys \n 16. Bladder
See the Clinical Supplement for all pre and post ganglionic cell bodiesJ
Part 1: For sympathetics, preganglionic cell bodies are always in the IML. The IML extends from T1-L2 and is arranged in a head to tail (viserotome) pattern. For example:
T1-4 – head, thoracic organs
T5-9 – foregut
T9-11 - midgut
L1-2 – hindgut & pelvic organs
\n 1. T1-4 \n 2. T1-4 \n 3. T1-4 \n 4. T6-9 right \n 5. T9-11 \n 6. L1-2 \n 7. L1-2 \n 8. T10-11
Part 2: For parasympathetics, preganglionics are cranio/sacral and the dividing line is the border between midgut and hindgut.
\n 9. Edinger-Westphal Nucleus (midbrain) \n 10. Superior Salivatory Nucleus (caudal pons) \n 11. Superior Salivatory Nucleus (caudal pons) \n 12. Inferior Salivatory Nucleus (rostral medulla) \n 13. Dorsal Vagal Nucleus (medulla) \n 14. Dorsal Vagal Nucleus (medulla) \n 15. Dorsal Vagal Nucleus (medulla) \n 16. Sacral Parasympathetic Column (sacral cord)
A 43-year-old female presents for follow up examination approximately 24 hours after laparoscopic gastric sleeve surgery. She complains of pain in her left shoulder. Physical examination reveals that her abdominal wall sutures are intact. She notes that her pain is worse when she takes a deep breath or leans forward. Which of the following is the most correct mechanism for this patient’s shoulder pain?
A. Irritation of parietal peritoneum
B. Irritation of C5 spinal nerve
C. Irritation of the greater splanchnic nerve
D. Referred pain from stomach
E. Referred pain from transverse colon
F. Referred pain from liver
[A] – Shoulder pain in the context of a body cavity issue is most likely going to result from irritation of the phrenic nerve, diaphragm or membranes innervated by the phrenic n (pericardium, mediastinal or diaphragmatic pleura or parietal peritoneum). In this case, the patient’s shoulder pain is from enlargement/stretching of the peritoneal sac with gas (CO2) from a laproscopic procedure. The C5 spinal nerve is found in the neck and is not likely to be irritated from this procedure. Referred pain from the stomach, colon and liver does not map to the left shoulder (See ANS levels in the Clin Supp!). Liver/gallbladder would be R shoulder.
1. Where is the lesion?
2. The infarct is in what vascular territory?
Just a reminder that Neuro is going to be a significant chunk of the Anatomy you will encounter on COMLEX & USMLE. Strokes should be considered very high yield – lucky you have the Cheat Sheets! By the way, neurodegenerative diseases are also going to be high yield in “Anatomy” but also Pathology. See the Neuro Clin Supp!!!
1. Left thalamus = only sensory issues! The pattern of sensory loss tells you the lesion is above the pons. The normal strength and reflexes means CST is intact (so NOT internal capsule). The normal eye movements rule out most of the brainstem.
2. Thalamogeniculate. Cannot be main stem PCA since this would include paramedian branches that supply midbrain (=CN III).
A 49-year-old male presents to the office with the complaints of neck pain and headaches over the past 3 days. Physical examination reveals a band of tight, ropey muscle that extends from the spinous processes of C7-T2 to the mastoid process on the right. What muscle is exhibiting dysfunction?
A. Longissimus capitis
B. Longus colli
C. Semispinalis capitis
D. Spinalis capitis
E. Splenius capitis
F. Trapezius
E. Splenius capitis
This is a straightforward muscle attachment question. The splenius capitis extends from spinous processes to the mastoid process. Longissimus extends from transverse processes to transverse processes, spinalis goes from spines to spines. The transversospinal group (semispinalis, multifidus + rotatores) all extend from transverse processes to spines. High Yield Tip: Be sure to review attachments and innervation of the trapezius.
A 54-year-old male presents to the emergency department with the chief complaint of chest pain that radiates down his left arm. An EKG reveals ST elevations in 2 contiguous leads. Imaging reveals the infarct involves most of the sternocostal surface of the heart and the inferior aspect of the interventricular septum. Which vessel is most likely occluded?
A. Circumflex
B. Left anterior descending
C. Left marginal
D. Posterior interventricular
E. Right coronary
F. Right marginal
E. Right coronary
The right coronary artery extends from the aorta until it becomes the posterior descending (posterior interventricular). The RCA (in a right dominant heart) supplies the right atrium, SA node, the sternocostal surface of the RV, the diaphragmatic surface of the RV. Its terminal branch (posterior descending a) supplies the AV node and the inferior 1/3 of the interventricular septum. The LAD (aka anterior interventricular, widow maker) supplies a small portion of the sternocostal surface of both ventricles and most of the IV septum. High Yield Tip: Images of EKGs are very popular on boards!
A 57-year-old female presents to the emergency department with the chief complaints of stomach pain and bloody sputum of two weeks duration. Endoscopy reveals an ulcer that has perforated the posterior wall of the 2nd part of the duodenum. Which of the following structures is most in danger of injury?
A. Aorta
B. Gall bladder
C. Pancreas
D. Renal artery
E. Splenic artery
F. Stomach
G. Superior mesenteric artery
D. Renal artery
Anatomy on USMLE is going to focus on relationships and support (support = arterial supply and venous/lymphatic drainage) of abdominal organs. High Yield Tip: Be sure to review what structures are posterior to the stomach (Clin Supp, Abdomen #35) and duodenum (Clin Supp, Abdomen #36).
A 50-year-old male presents to the office with the chief complaints of stomach pain and spitting up blood. Imaging reveals a tumor involving the fundus, cardia and body of the stomach. Which of the following spinal cord levels is responsible for carrying pain from this lesion?
A. T12
B. L1-2
C. T1-4
D. S2-4
E. T5-9
F. T10-11
F. T5-9
ANS levels are going to be huge for Anatomy and OPP. See Clin Supp, Abdomen #97 & 98. High Yield Tip: Sympathetics go everywhere.
A 59-year-old male presents to the office with the chief complaint of bloody feces. Physical examination reveals a large rectal mass that encompasses nearly the anterior wall of the rectum. Which of the following dermatomes/myotomes is most likely to exhibit somatic dysfunction?
A. T12
B. L1-2
C. T1-4
D. S2-4
E. T5-9
F. T10-11
A. L1-2
Please, please, please memorize these levels! See Clin Supp, Abdomen #97 & 98
A 30-year-old male presents for surgical removal of a thyroid carcinoma localized to the inferior aspect of his left thyroid lobule. During surgical removal of the diseased portion of the gland, what nerve is most at risk of iatrogenic injury?
A. External laryngeal
B. Glossopharyngeal
C. Greater splanchnic
D. Internal carotid
E. Recurrent laryngeal
F. Spinal accessory
E. Recurrent laryngeal
Location is key here: the inferior thyroid artery supplies the inferior aspect of each thyroid lobule. Remember the inferior thyroid artery and recurrent laryngeal nerve are traveling buddies!
High Yield Tip: The laryngeal traveling buddies are:
Internal laryngeal n (sensory above vocal cords) + superior laryngeal a
External laryngeal n (cricothyroid m) + superior thyroid a
Recurrent laryngeal n (sensory below cords+the rest of the muscles)+inferior thyroid a
During surgery to remove a parotid carcinoma, it becomes necessary to sacrifice several nerve branches coursing transversely through the gland. Which of the following signs/symptoms will most likely be present as a result of injury to these nerves?
A. Absent corneal reflex
B. Fasciculations in the masseter
C. Dye mouth
D. Hyperacusis
E. Hoarseness
F. Loss of pinprick sensation on the face
A. Absent corneal reflex
Branches from the facial nerve course through the parotid gland. These branches are only motor to the muscles of facial expression. There are no parasympathetic or special sensory axons remaining in these branches of the facial nerve. The masseter is a muscle of mastication and is supplied by the mandibular division of CN V.
High Yield Tip: Facial nerve injuries are high yield on both exams! You should be able to differentiate patterns of facial nerve signs/symptoms with injuries in these locations:
frontal lobe/internal capsule/cerebral peduncle
pons
facial nerve (internal meatus; facial canal; stylomastoid foramen; parotid gland)
A 50-year-old male presents to the office with the chief complaints of headaches and a droopy eyelid on the left side. His history is significant for a left carotid endarterectomy 1 week ago. Physical examination reveals (on the left) a constricted pupil and red, warm skin on his cheek. Extraocular movements are normal in all cardinal planes. Which of the following structures was most likely injured during this patient’s surgical procedure?
A. Interomediolateral cell column
B. Oculomotor nerve
C. Sympathetic chain
D. T1 spinal nerve
E. Vagus nerve
E. Vagus nerve
The key here is where the procedure is being performed in the body! The goal of the procedure is to clean out the internal carotid, which splits off from the common carotid at about CV4. The left recurrent laryngeal nerve branches from the vagus inferior to the aortic arch. So, in this procedure (especially on the left) the recurrent laryngeal nerve is not at direct risk of injury…but the vagus nerve is very much at risk…and at this level the vagus nerve is carrying all the axon that will be the recurrent. The paralyzed vocal cord clues you in to paralysis of the posterior and lateral cricoarytenoid muscles. The cricothyroid muscle (innervated by the external laryngeal nerve) is also intact (=midline thyroid cartilage; Clin Supp, Head #30i).
During surgical repair of a lacerated spleen in a 19-year-old male after an automobile accident, the splenorenal ligament is clamped to control bleeding. Which of the following structures is most at risk of iatrogenic injury?
A. Cisterna chyli
B. Iliohypogastric nerve
C. Left adrenal gland
D. Left kidney
E. Pancreas
F. Sympathetic chain
E. Pancreas
The splenorenal ligament (see most recent version of the Clin Supp, Abdomen, #19) is a fold of peritoneum that extends between the spleen and left kidney. It includes the tail of the pancreas and the splenic artery, vein and associated lymphatics and autonomic nerves. The kidney is not actually within the ligament. High Yield Tip: USMLE likes to ask about clamping of peritoneal ligaments – especially what is in them and what organs would be affected by clamping them.
Imaging from a 17-year-old male with lower limb claudication reveals the result shown in the accompanying image. Which of the following arteries plays the most significant role in carrying blood around this blockage?
A. External carotid
B. Internal thoracic
C. Lateral thoracic
D. Profunda brachial
E. Superior gluteal
F. Vertebral
B. Internal thoracic
The arteriogram shows a coarctation of the aorta and tortuous vessels that are carrying blood around the blockage. You should also expect rib notching from dilated intercostal arteries. See Clin Supp, Thorax #41.
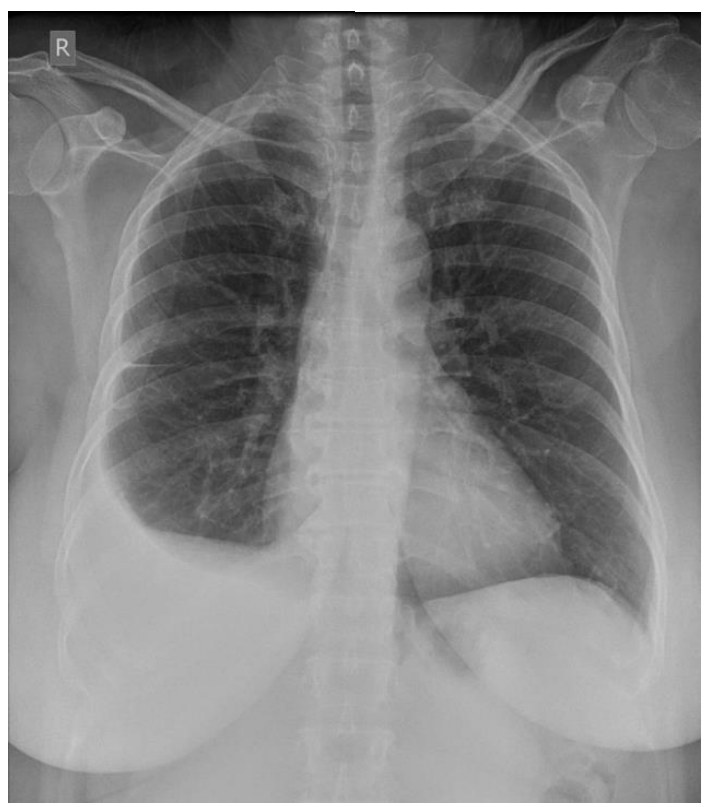
A chest radiograph from a 60-year-old female reveals the result shown in the accompanying image. Her medical history is significant for breast cancer 8 years ago for which she received chemo and radiation therapy. To remove this fluid, thoracocentesis should be performed at which of the following locations?
A. Midaxillary line, 6th intercostal space
B. Midaxillary line, 9th intercostal space
C. Midclavicular line, 4th intercostal space
D. Midclaviculiar line, 10th intercostal space
E. Scapular line, 6th intercostal space
F. Scapular line, 8th intercostal space
D. Right midaxillary line, 9th intercostal space
You need to use the radiograph to identify the right pleural effusion. The thoracocentesis needs to be done on the right side. See Clin Supp, Thorax #14.
High Yield Tip: Remember the costodiaphragmatic recess extends between ribs 6-8 (midclavicular line), 8-10 (midaxillary line) and 10-12 (scapular line).
During laproscopic repair of an indirect inguinal hernia in a 15-year-old male, a staple is placed in the interval between the inguinal ligament and testicular vessels. What nerve is most likely to be injured by this staple?
A. Femoral
B. Iliohypogastric
C. Ilioinguinal
D. Obturator
E. Pudendal
F. Subcostal
A. Femoral
This is the Triangle of Pain. See Clin Supp, Abdomen #8f. High Yield Tip: You should be expecting inguinal/femoral hernia questions on both exams.
A 40-year-old gravida 2, para 2 female presents to the office with the chief complaints of pelvic pain, constipation and dyspareunia. Physical examination reveals that on attempted Valsalva maneuver, her cervix protrudes to her vaginal orifice. Which of the following structures is most likely dysfunctional?
A. Broad ligament
B. Fascia of the obturator internus
C. Perineal body
D. Round ligament of the uterus
E. Suspensory ligament of the ovary
F. Uterosacral ligament
C. Perineal body
I am very confident you are going to see this question or one very similar on USMLE. High Yield Tip: Memorize Clin Supp, Pelvis & Perineum, #23b.
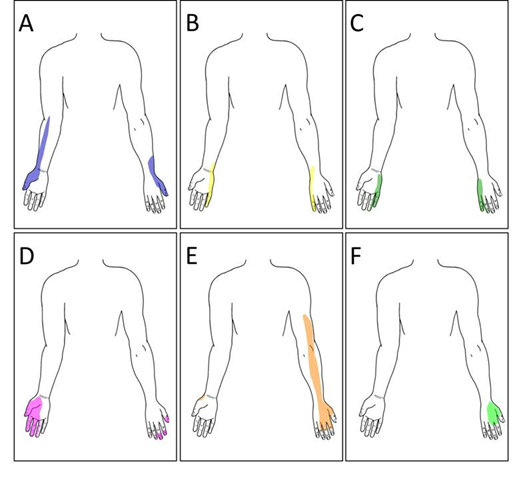
A 44-year-old male presents with complaints of shoulder pain and numbness in his right upper extremity. Physical examination reveals diminished pin-prick sensation in the region indicated in the accompanying figure. Where is the lesion?
A. C5 spinal nerve
B. C6 spinal nerve
C. C8 spinal nerve
D. Median nerve
E. Musculocutaneous nerve
F. Radial nerve
G. Ulnar nerve
B. C6 spinal nerve
This is a high probability item on COMLEX. You need to be able to recognize this pattern of sensory loss as being a dermatome pattern and not a peripheral nerve pattern (e.g. median, ulnar). High Yield Tip: The UL Cheat Sheets are a great review for nerve injuries in the upper limb!
A 68-year-old male presents to the emergency room with the chief complaints of sudden onset weakness in his left lower extremity. His muscle stretch reflexes are globally 2/4 except for his left lower extremity (0/2). He has a Babinski sign on the left. He has diminished pinprick and position sense in his left lower extremity. He has a tactile aphasia with his left hand. A CT will most likely reveal an infarct in what vascular territory?
A. Anterior spinal
B. Left posterior inferior cerebellar
C. Left vertebral
D. Right anterior cerebral
E. Right posterior spinal
F. Right vertebral
E. Right cerebral hemisphere
This one can be tricky since his issues are restricted to his left LL. Remember the big 3 tracts (corticospinal tract, posterior columns/medial lemniscus & spintothalamic tracts) cross the midline at different levels of the CNS. Review this in the Neuro Supplement! Because of this, spinal cord injuries result in incongruous patterns of sensory loss (CL loss of pin prick; IL loss of position sense). Since the diminished pinprick sensation overlaps with the loss of position sense, the lesion has to be midbrain or higher. Then, because the sensory loss and weakness are limited to his LL, the lesion is most likely in the territory of the anterior cerebral artery. A small lesion in the right internal capsule is also possible, but the hemisphere is better answer. High Yield Tip: The Brain Syndrome Cheat Sheets (+the Neuro Supplement) provide a great review of neuroanatomy! Also…there is going to be neuro on both exams!
A 60-year-old male presents to the office with the chief complaints of back pain, difficulty walking and sensory loss in his right lower extremity. Physical examination reveals sensory loss and reflexes as shown in the accompanying image. Strength testing will most likely reveal which of the following?
A. Dorsiflexion 0/5
B. Plantar flexion 1/5
C. Knee extension 2/5
D. Hip flexion 3/5
E. Hip extension 3/5
E. Hip extension 3/5
This is a L5 radiculopathy and is a very high probability item on COMLEX. Again, you have to recognize this as a spinal nerve pattern and not common fibular nerve (see bottom of the foot). Remember that L4, L5, S1 and S2 all supply the gluteal muscles – so injuries to these nerves will also have weakness in hip extension and/or hip abduction. High Yield Tip: See LL Cheat Sheets. Just a reminder that ~95% of disc herniations are LV4-5 or LV5-SV1
A. Dorsiflexion 0/5 B. Plantar flexion 1/5 C. Knee extension 2/5 D. Hip flexion 3/5 E. Hip extension 3/5
A. Compression of median nerve in carpal tunnel
B. Compression of median nerve in cubital fossa
C. Compression of radial nerve in axilla
D. Entrapment of radial nerve in supinator canal
E. Entrapment of the ulnar nerve in cubital tunnel
F. Entrapment of the ulnar nerve in Guyon’s canal
B. Compression of median nerve in cubital fossa
Median nerve injuries are high probability on both exams. The key to this one is to remember that the superficial palmar branch (supplies the skin over base of thumb) does not go through the carpal tunnel. This patient’s pattern of sensory loss is consistent with injury to the median nerve proximal to the carpal tunnel. High Yield Tip: Be sure you can differentiate injuries to median and ulnar nerves at the elbow and wrist.
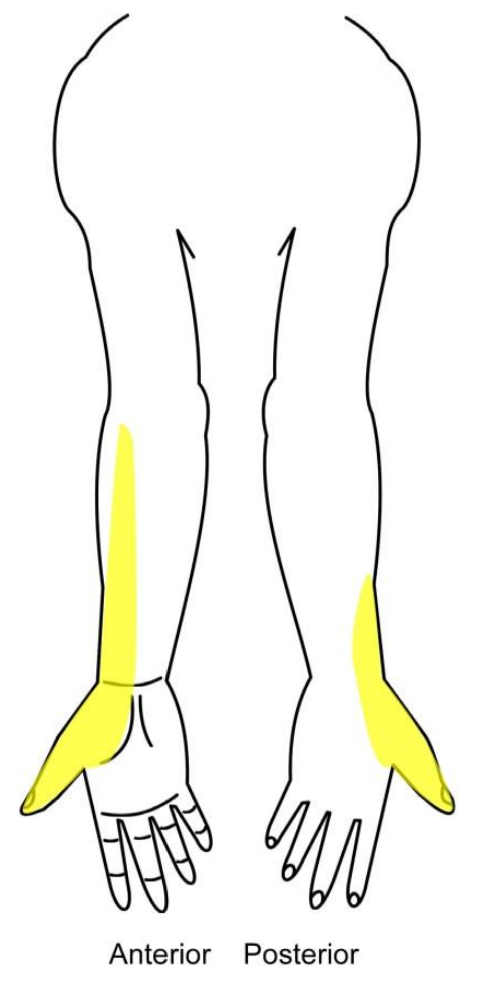
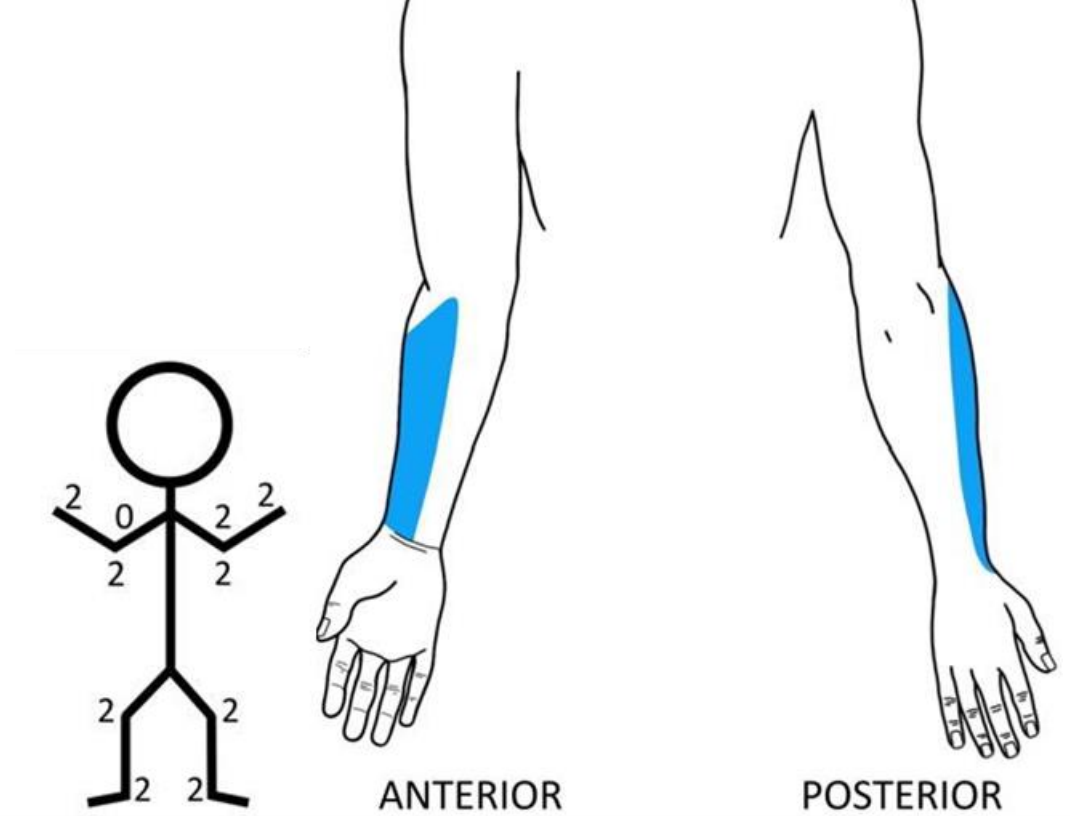
A 27-year-old male presents to the emergency room after falling of his motorcycle and injuring his right upper extremity. Physical examination reveals sensory loss and reflexes as shown in the accompanying image. What nerve is injured?
A. C5 spinal nerve
B. C6 spinal nerve
C. Medial cord of brachial plexus
D. Median nerve
E. Musculocutaneous nerve
F. Posterior cord of brachial plexus
G. Ulnar nerve
E. Musculocutaneous nerve
Here you have to differentiate a C6 radiculopathy from a musculocutaneous nerve injury. Remember, the C6 dermatome involves both the anterior and posterior aspects of the thumb. The C6 myotome involves both the biceps and brachioradialis muscles. The musculocutaneous nerve only innervates the muscles in the anterior compartment of the arm and the region of skin shown in this figure. High Yield Tip: See UL Cheat Sheets.
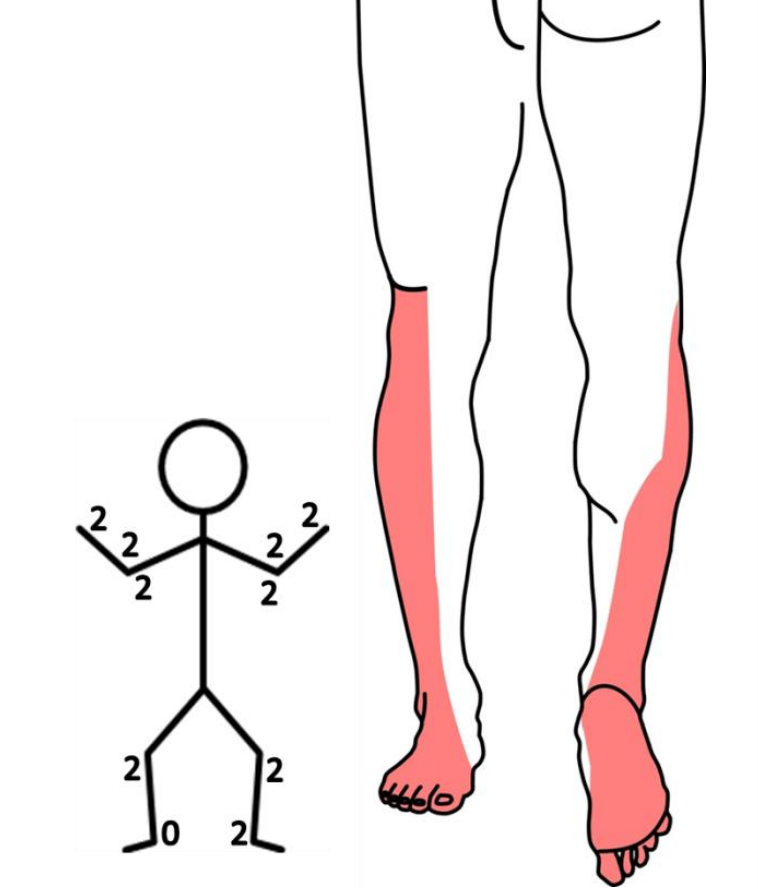
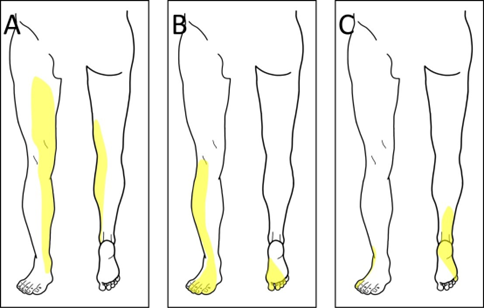
A 65-year-old male presents to the office with the chief complaints of weakness in his right lower extremity. He claims he first noticed this about 1 week ago. His history is significant for hypertension and diabetes mellitus. Physical examination reveals sensory loss and reflexes as shown in the accompanying figure. He has 5/5 strength in hip extension. What nerve is injured?
A. Common fibular nerve
B. L4 spinal nerve
C. L5 spinal nerve
D. S1 spinal nerve
E. Sciatic nerve
F. Tibial nerve
E. Sciatic nerve
The pattern of sensory loss is consistent with tibial and common fibular nerves. The normal strength in hip extension further rules our L5 and S1.
High Yield Tip: I would recommend watching some videos of people with things like:
Trendelenburg sign: https://www.youtube.com/watch?v=ZUPQp5oxXj8
foot drop: https://www.youtube.com/watch?v=STZszh4K1Fo
femoral nerve injury: https://www.youtube.com/watch?v=O8H5FDYv34
gluteus maximus gait: https://www.youtube.com/watch?v=_HsgM_00q_c
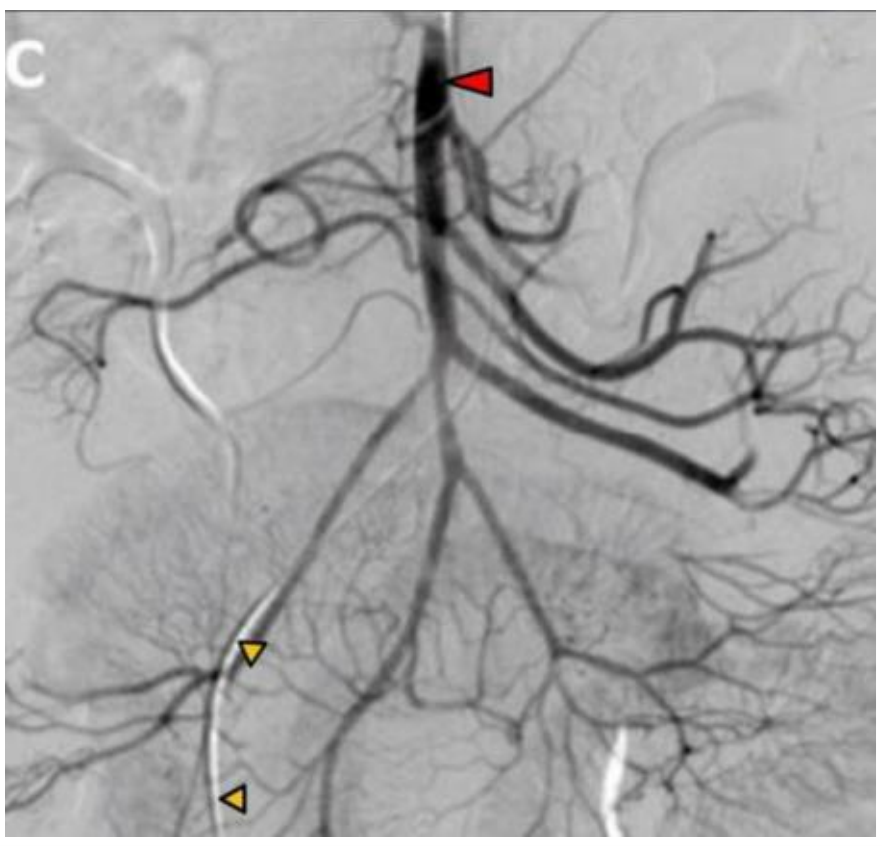
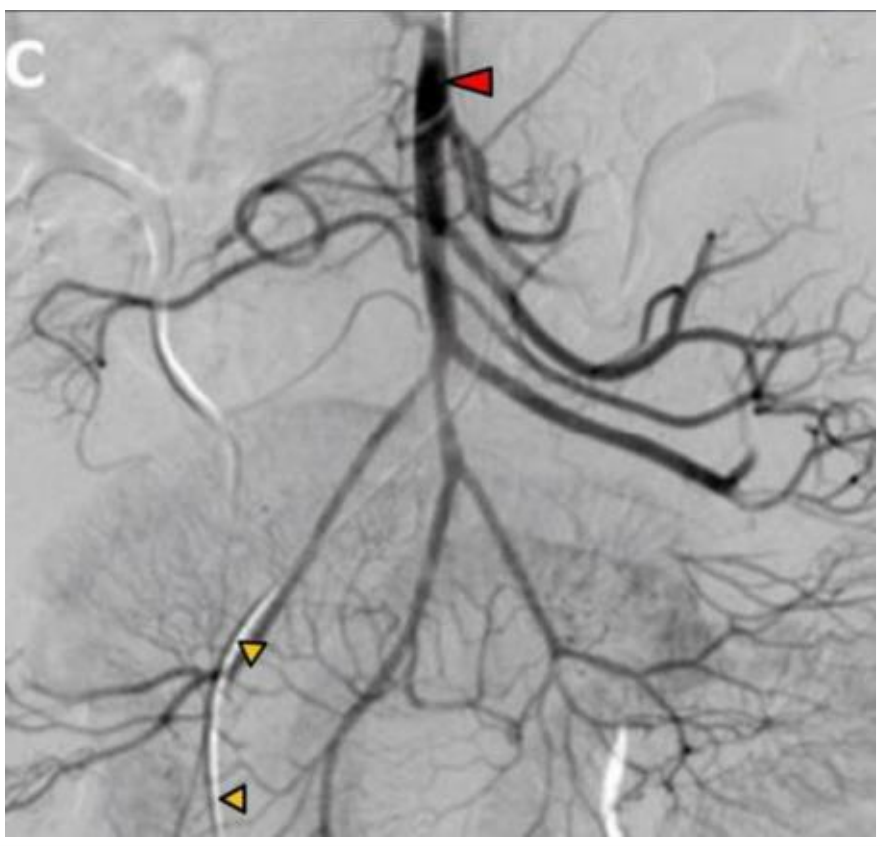
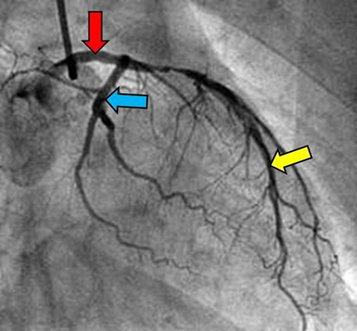
An arteriogram from a 33-year-old female with abdominal pain reveals the image shown in the accompanying image. What artery is indicated by the red arrowhead?
A. Aorta
B. Celiac trunk
C. Inferior mesenteric artery
D. Internal iliac
E. Superior mesenteric artery
E. Superior mesenteric artery
An arteriogram from a 33-year-old female with abdominal pain reveals the image shown in the accompanying image. The catheter (orange arrowheads) is in what vessel?
A. External iliac
B. Femoral
C. Inferior rectal
D. Internal iliac
E. Internal pudendal
A. External iliac
Qs 75 & 76) The abdominal pain is a clue we are looking at an abdominal vessel. There is no (tortuous!) splenic artery…or common hepatic (splitting to form a T) à this rules out celiac. Remember that the SMA has branches directed to both the right and left of the main trunk. The IMA only has branches to the patient’s left. The catheter for this study goes into the femoral artery and then to the external iliac, common iliac and then aorta. Since we still see branches of the SMA, the images is too far superior to have femoral artery in the image and the arrowheads are not high enough to be common iliac.
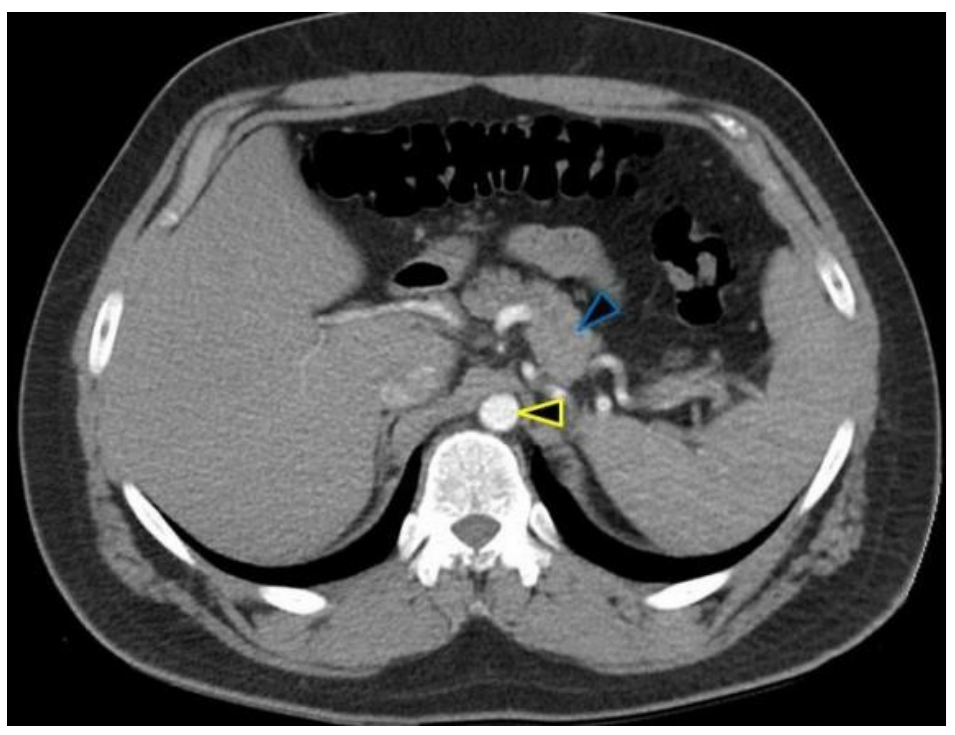
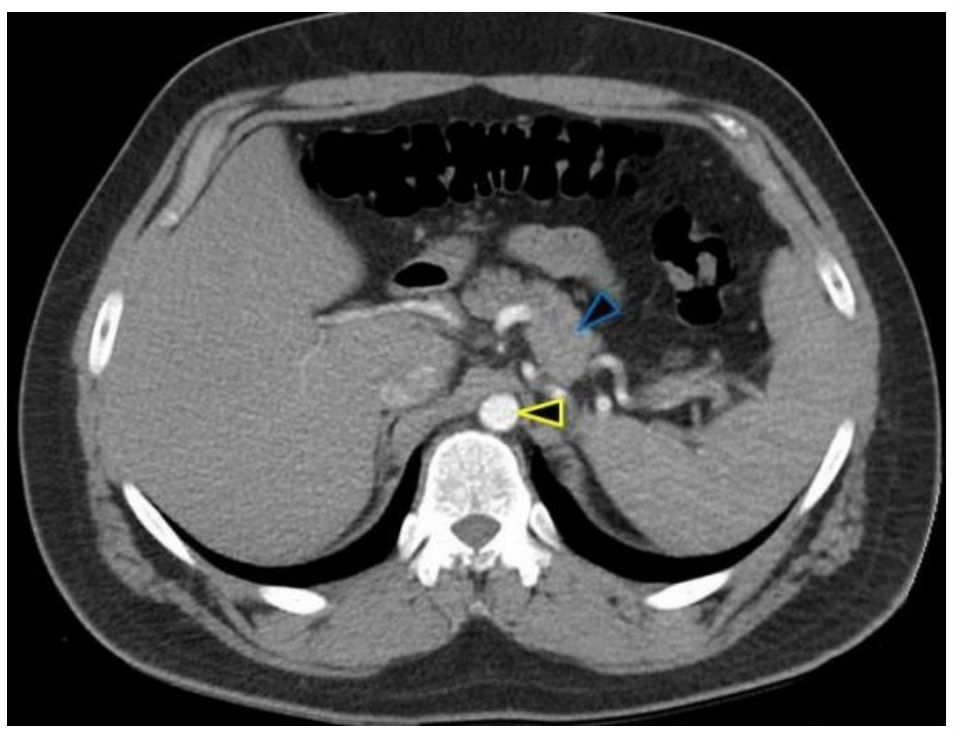
A CT scan from a 55-year-old male reveals the result shown in the accompanying image. What structure is indicated by the yellow arrowhead?
A. Aorta
B. Duodenum
C. Inferior vena cava
D. Lumbar lymph node
E. Superior mesenteric artery
A. Aorta
A CT scan from a 55-year-old male reveals the result shown in the accompanying image. Blood supply to the structure indicated by the blue arrowhead is from what artery?
A. Common hepatic
B. Left gastric
C. Proper hepatic
D. Renal
E. Splenic
F. Superior mesenteric
E. Splenic
(Qs 77 & 78 ) I promise you are going to see abdomen CT images on USMLE. And it is very likely that you get second order questions à ID something and then they ask you about blood supply or lymphatic drainage. Practice this! Anyway, there is arterial contrast in this image – a round structure along the left side of the vertebral column will be the aorta. If there isn’t contrast, look for plaques along the wall of the aorta. This section is high – near the liver, so the IVC is embedded in the liver. The blue arrowhead indicates the pancreas. This is a super high yield ID for USMLE. The pancreas should be behind (posterior to) the stomach and be kind of fluffy. Look for a tortuous splenic artery nearby entering the spleen.
High Yield Tip: Practice identifying stuff on CT!
Upper GI: https://radiopaedia.org/cases/ct-abdomenpelvis-upper-axial-labelling-questions?lang=us
Lower GI: https://radiopaedia.org/cases/ct-abdomenpelvis-lower-axial-labelling-questions?lang=us
A 24-year-old female presents to the office with the chief complaints of tenderness and pain in her right cheek and jaw. She claims she first noticed this about a week ago and claims it has gotten progressively worse. Physical examination reveals a calculus in her right parotid duct. Which of the following nerves is most directly responsible for this patient’s perception of pain?
A. Auriculotemporal
B. Deep petrosal
C. Glossopharyngeal
D. Greater petrosal
E. Lesser petrosal
F. Vagus
A. Auriculotemporal
Remember that the parasympathetic innervation to the parotid gland is from CN IX (tympanic n à lesser petrosal n, then hitchhiking on the auriculotemporal n). The auriculotemporal nerve is a branch from CN V and provides GSA innervation to the connective tissue capsule of the parotid. Inflammation and swelling of the parotid gland results in stretching (pain!) of the capsule and somatic pain. High Yield Tip: The GSA pattern is the same for the submandibular and sublingual glands.
A CT scan from a 55-year-old male with a history of bloody diarrhea reveals the result shown in the accompanying image. What spinal cord levels provide sympathetic innervation to the organ indicated by the red arrowhead?
A. T12
B. L1-2
C. T1-4
D. S2-4
E. T5-9
F. T10-11
F. T10-11
The red arrowhead indicates the transverse colon (see the haustra and gas). The proximal 2/3 of the transverse colon is midgut. Blood supply to the midgut is from the superior mesenteric artery and lymph drains to superior mesenteric nodes. When you review gut stuff, you should simplify all the support into foregut, midgut and hindgut patterns. I promise this is adequate!
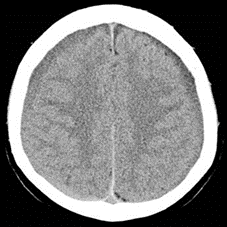
A CT scan from a 72-year-old female with sudden onset sensory loss and somnolence reveals the result shown in the accompanying image. Which of the following is the most correct diagnosis?
A. Astrocytoma
B. Epidural hemorrhage
C. Intraparenchymal hemorrhage
D. Medulloblastoma
E. Meningioma
F. Multiple sclerosis
G. Subarachnoid hemorrhage
C. Intraparenchymal hemorrhage
Remember that fresh blood is bright white on CT. In this case, there is a hemorrhage in the right thalamus. Also note the calcification of the pineal gland and choroid plexus. This lesion would result in a pure sensory stroke (VPM/VPL - CL loss of pain, thermal sense, proprioception and vibratory sense) and a CL homonymous hemianopia (lateral geniculate)
Physical examination from a 22-year-old female with diplopia reveals the results shown in the accompanying image. What nerve is injured?
A. Left CN II
B. Left CN III
C. Left CN IV
D. Left CN VI
E. Right CN II
F. Right CN III
G. Right CN IV
H. Right CN VI
B. Left CN III
You can expect these 9 panel images on both exams. Remember, look to the center image (5) first! You can often make the diagnosis form that center image. In this case, the center image shows left ptosis. Then compare the R pupil (5) to the left pupil in image 4 = mydriasis. This is all you need to call this a left CN III lesion. With CN IV injuries, the affected eye will be “down and out” in the center image. With CN VI injuries, the affected eye will be slightly adducted in the center image. High Yield Tip: See Eye Syndrome Cheat Sheets for a quick review!
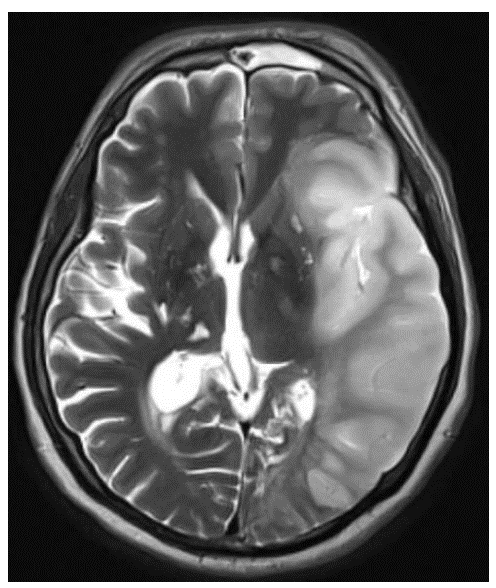
A T2 MRI from a 59-year-old male with sudden onset weakness reveals the result shown in the accompanying image. Which of the following signs/symptoms will most likely be found on physical examination?
A. Alexia without agraphia
B. Bitemporal hemianopia
C. Contralateral neglect
D. Diplocusis
E. Dysdiadokinesia
F. Global amnesia
F. Global aphasia
The image shows a large left main stem MCA infarct that involves Broca’s area, Wernicke’sarea and the deep white matter that connects these regions (arcuate fasciculus). Alexia without agraphia results from injury to the left splenium of the corpus callosum (PCA territory). A bitemporal hemianopia results from injury to the optic chiasm. Contralateral neglect involves damage to the right parietal lobe. You probably never hear of diplocusis. I’m ok with that. Dysdiadokinesia is a sign of damage to the cerebellum.
High Yield Tip: I would advise watching some videos of:
Expressive Aphasia: https://www.youtube.com/watch?v=f2IiMEbMnPM&t=42s
Receptive Aphasia: https://www.youtube.com/watch?v=3oef68YabD0&t=14s
A CT scan from a 60-year-old male with sudden onset weakness reveals the result shown in the accompanying image. He first noticed the weakness about 30 minutes ago. He is alert to person, time and place. His pupils are equal, round and reactive to light and accommodation. The infarct (indicated by the arrowheads) is within what vascular territory?
A. Anterior choroidal
B. Lenticulostriate
C. Long circumferential branches from the basilar
D. Paramedian branches from the basilar
E. Paramedian branches from the posterior cerebral
F. Thalamoperforators
D. Paramedian branches from the basilar
A CT scan from a 60-year-old male with sudden onset weakness reveals the result shown in the accompanying image. He first noticed the weakness about 30 minutes ago. He is alert to person, time and place. His pupils are equal, round and reactive to light and accommodation. Which of the following signs/symptoms will most likely be found on physical examination?
A. 3/4 patellar reflex on left
B. Babinski sign on right
C. Fasciculations in the tongue
D. Inability to smile on left
E. Mydriasis on right
D. Inability to smile on left
(Qs 84 & 85) The first part of this question is identifying where the lesion is (rostral pons) since the s/s don’t really give you any clues. You should be able to identify this as pons because of big, rounded belly of the basilar pons. You can also see the 4th ventricle and some of the cerebellum. Since the lesion is in the medial pons, the blood supply is paramedian branches of the basilar artery. Remember that in acute injuries (stroke) reflexes are diminished. Hyper-reflexia takes at least a few days to develop. There is a Babinski sign, but on the left. This injury to too rostral to impact the hypoglossal nucleus so there would be no fasciculations in the tongue. Mydrasis occurs with injury to CN III – this lesion is too far caudal. For a quick review, see Brain Syndrome Cheat Sheets and Neuro Supplement (Brainstem #9: Common Lesions of the Pons).
High Yield Tip: There is going to be Neuro on both exams - and they are not going to show you where the lesion is.
Student Doctors - See if you can guess the lesion/etiology from changes in muscle stretch reflexes (COMLEX likes "deep tendon reflexes") and 1 other hint! See the attached figure and the clues below. Answers at the bottom!
Pt A: 50-year-old male with reflexes as shown and sensory loss over his right thumb
Pt B: 25-year-old male with reflexes as shown and sensory loss over his right lateral forearm
Pt C: 27-year-old female with reflexes as shown, diffuse loss of vibratory sense and scotoma in R eye
Pt D: 49-year-old male with reflexes as shown, no sensory loss
Pt A = C6 radiculopathy: both biceps and brachioradialis are C5-6
Pt B = musculocutaneous n mononeuropathy: injury to this nerve paralyzes the biceps, coracobrachialis and brachialis…and results in sensory loss along the lateral forearm
Pt C = prob multiple sclerosis, a history of relapsing/remitting s/s would be key; could be spinal cord compression – I would want to see sensory loss and incontinence; remember that elevated reflexes, especially when they are asymmetric are consistent with injury to the corticospinal tract
Pt D = ALS (upper and lower motor neuron signs and no sensory loss): you need to see a combination of upper and lower motor neurons signs without sensory loss
A routine ultrasound of 26-year-old female in her 20th gestational week reveals polyhydramnios. This finding is most consistent with which of the following congenital anomalies? \n \n
A. Aniridia
B. Ectopia cordis
C. Horseshoe kidney
D. Renal agenesis
E. Situs inversus
F. Spina bifida with myeloschisis
G. Tracheo-esophageal fistula
[G] – Remember that normal levels of amniotic fluid are maintained by the fetus swallowing a certain volume/day. Any upper GI blockage (especially a trachea-esophageal fistula!) can result in polyhydramnios.
For purposes of review, you should also consider anomalies that might lead to oligohydramnios (genitourinary, placental abnormalities).
Ectopia cordis and spina bifida with myleoschisis (holes in the embryo) would lead to elevated alpha fetoprotein.
Student Doctors – UL nerve injuries are high yield on COMLEX & USMLE!
Guess the lesion/etiology from patterns of sensory loss.
See the figure and the clues below. Answers at the bottom!
Pt A: 50-year-old male with neck pain
Pt B: 55-year-old male with hand weakness
Pt C: 22-year-old female after falling from her bicycle
Pt D: 24-year-old female after motor vehicle accident
Pt E: 17-year-old male with sharp force penetrating trauma to right UL
Pt F: 30-year-old female after external fixation of forearm fracture
Pt A: C6 radiculopathy – sensory loss is limited to the C6 dermatome!
Pt B: C8 radiculopathy – sensory loss is limited to the C8 dermatome!
Pt C: Ulnar n at elbow (fx of medial epicondyle!) – ulnar nerve does not innervate any skin proximal to the wrist, also see medial aspect of the 4th digit
Pt D: Median n at elbow – involvement of the skin over the thenar eminence indicates that the injury involves the median nerve proximal to the carpal tunnel
Pt E: Radial n in axilla – sensory loss covers the entire radial n distribution (none fingertips)
Pt F: Radial n at elbow or superficial br of radial n – sensory loss is limited to the territory of the superficial br of the radial n
Student Doctors - See if you can guess the lesion/etiology from patterns of sensory loss!
See the attached figure and the clues below. Answers at the bottom!
Pt A: 60-year-old female with poorly controlled diabetes and difficulty walking
Pt B: 50-year-old male who says his right foot slaps the floor when he walks
Pt C: 58-year-old male with difficulty walking
A. Femoral n but could also be L3 & L4 radiculopathies. Strength testing would be able to differentiate these: remember besides muscles in the anterior compartment of the thigh, L4 innervates tibialis anterior. So, an L4 radiculopathy would include weakness in dorsiflexion. The femoral n does not innervate tibialis anterior.
B. L5 radiculopathy. He has foot drop! Remember the tips of the digits are innervated by the same nerve that innervates the palmar/plantar surface of the hand/foot. Check it: the medial and lateral plantar nerves (from the tibial) innervate the skin along the plantar aspect of the foot and the tips of the corresponding toes. How to rule out common fibular nerve: this nerve does not innervate the tips of the toes or any skin along the plantar surface of the foot. With an L5 radiculopathy, there should be normal reflexes (2/4) but weakness in hip extension, medial & lateral rotation (ß Its all in the hips!), knee flexion and dorsiflexion, inversion and eversion. See Clinical Supplement, Lower Limb #16 Joints and Myotomes
C. S1 radiculopathy. The sensory loss is most consistent with the S1 dermatome. It covers only parts of the sural and tibial nerve territories. Intact sensation on the plantar aspect of the foot (digits 1-4) rules out isolated injury to the tibial n. Intact sensation on the dorsum of the foot rules out common fibular and sciatic. Together, these indicate an injury more proximal than formation of the sciatic nerve (i.e. spinal nerve). There should be a diminished Achilles/calcaneal reflex and weakness in hip extension, lateral rotation, knee flexion, plantarflexion and eversion.
Note: 95% of all disc herniations are between L4-5 or L5-S1 and L5 & S1 radiculopathies are very common LL board questions!
A 54-year-old male presents to the office with urinary incontinence, difficulty walking and weakness in his hands. He first noticed these issues 2 months ago and claims his weakness has gotten worse over the past 2 weeks. His pupils are equal, round and reactive to light and all extraocular movements are intact. He can wrinkle his forehead and smile symmetrically. His muscle stretch reflexes are 3 - 3+/4 globally and his plantar reflex is extensor on both sides. He has diminished vibratory and position sense in his lower extremities. Which of the following is the most likely diagnosis?
A. Amyotrophic lateral sclerosis
B. Cerebellar hemorrhage
C. Cervical spinal cord compression
D. Diabetic polyneuropathy
E. Guillain-Barre syndrome
F. Multiple sclerosis
G. Pontine hemorrhage
H. Syringomyelia
A. Amyotrophic lateral sclerosis – requires both upper and lower MN signs
B. Cerebellar hemorrhage – this would be sudden onset + ataxia
C. Cervical spinal cord compression – Yes! Compression of the cervical spinal cord by a herniated disc, osteophytes, hypertrophied ligamentum flavum, etc can cause this pattern of incontinence, weakness and sensory loss. Remember the axons controlling the sphincters traverse the brainstem and spinal cord and can be damaged anywhere along their course. If this doesn’t sound familiar, see the bladder stuff on pages 29-30 of the Neuro supplement.
D. Diabetic polyneuropathy – stocking/glove sensory loss
E. Guillain-Barre syndrome – post-infectious ascending paralysis, diminished reflexes
F. Multiple sclerosis – waxing and waning vision loss, INO, weakness, sensory loss, not symmetric
G. Pontine hemorrhage – cranial nerve signs, ataxia
H. Syringomyelia – symmetric dermatomal loss of pinprick sensation
Just a reminder that “plantar reflex is extensor” = Babinski sign (You should know both terms)
Neuro! Answers below.
Just a reminder of all the highly recommended Neuro resources available on the Convergence course page. Specifically, I highly recommend the Neuro Clinical Supplement and Brain Syndrome Cheat Sheets for board study!
A 64-year-old female presents to the emergency room with vision loss in her left eye. She claims that she first noticed the vision loss about 60 minutes ago but claims that she can see normally now. She describes the episode of vision loss as sudden and that she could not see anything from her left eye. Her history is significant for diabetes mellitus and hypertension. A CT angiogram will most likely reveal a blockage in which of the following arteries?
A. Basilar
B. Facial
C. Internal carotid
D. Maxillary
E. Posterior cerebral
F. Vertebral
A transient ischemic attack affecting vision is known as amaurosis fugax (=passing darkness) and is very popular on COMLEX/USMLE. It is indicative of a blockage in the internal carotid artery and is a sign of an impending stroke. See Neuro Supp, Blood Supply #5.
A 28-year-old female presents to the office with vision loss, difficulty walking and double vision. She claims that she has had some difficulty walking for about 2 weeks, but she noticed the vision loss 2 days ago. She notes that she had an episode of vision loss last year that resolved after 2 days. Physical examination reveals a right scotoma and reduced vibratory sensation in her left upper and lower extremities. Pin prick sensation is globally intact. She has difficulty with finger to nose testing bilaterally. She has a Babinski sign on the left. Which of the following is the most likely diagnosis?
A. Amyotrophic lateral sclerosis
B. Guillain-Barre syndrome
C. Multiple sclerosis
D. Spondylosis
E. Subacute combined degeneration
F. Transverse myelitis
The answer is C.
ALS – characterized by both upper and lower motor neurons signs. No sensory loss
GB – post infection, symmetric ascending weakness
MS - relapsing/remitting signs and symptoms commonly include vision loss (**See Neuro supplement for PE, MRI and lab findings!**). I would advise being able to ID MS plaques (Dawson’s fingers) on imaging.
Spondos – s/s localized to spinal cord levels or multiple nerve roots
SCD – B12 deficiency, affects posterior columns and corticospinal tracts
Transverse myelitis – looks like spinal cord transection
A 56-year-old male presents to the office with difficulty walking and weakness in his left lower extremity that has gotten progressively worse over the past month. Physical examination reveals [on the left] diminished pinprick and vibratory sense along the anteromedial aspect of left leg. His patellar reflex [on the left] is 1/4 (all other muscle stretch reflexes are 2/4). Muscle strength in his left lower extremity is as follows:
Hip: flexion 3/5; extension 5/5
Knee: flexion 5/5; extension 2/5
Ankle: dorsiflexion 4/5; plantarflexion 5/5
Which of the following is the most likely etiology?
A. Compression of the spinal cord at the level of LV1
B. Femoral neuropathy
C. Herniated disc between LV3 and LV4
D. Impingement of the posterior roots at L4 and L5
E. L5 radiculopathy
F. Tumor eroding the lumbosacral trunk
C. A herniated disc between LV3 and LV4 will most likely impact the L4 spinal nerve. The weakness in knee extension rules out lumbosacral trunk. The weakness in dorsiflexion rules out injury to the femoral nerve. The weakness in knee extension rules out L5.
A coronary arteriogram from a 53-year-old male who presented with the chief complaints of chest pain and shortness of breath reveals the accompanying image. What vessels are indicated by red, blue and yellow arrows respectively?
A. Left coronary, AV nodal, posterior interventricular
B. Left coronary, circumflex, left anterior descending
C. Left coronary, left marginal, left anterior descending
D. Left coronary, right coronary, left anterior descending
E. Right coronary, right coronary, left anterior descending
F. Right coronary, right marginal, posterior interventricular
G. Right coronary, SA nodal, posterior interventricular
[B], USMLE is biased towards viscera and body cavities and they really like to ask about blood supply. Also, the questions about the vessels are often 2nd order. For example:
The indicated artery supplies what part of the conducting system? For review of this type of question for coronary arteries see Anatomy Clinical Supplement, D. Thorax #27-33!
During surgery to resect a parotid carcinoma, it becomes necessary to sacrifice a nerve identified anterior to the mastoid process and inferior to the external auditory meatus. Which of the following signs/symptoms will most likely be present as a result of this iatrogenic injury?
A. Absent corneal reflex
B. Decreased taste sensation
C. Dry eye
D. Dry mouth
E. Flaccid paralysis of the masseter
F. Hyperacusis
G. Loss of pin-prick sensation on the face
Facial nerve questions are very popular on COMLEX & USMLE and they are not going to tell you its facial nerve. You’ll get clues about its relationships: in the parotid, emerging from the stylomastoid foramen, etc.
A – The nerve being sacrificed is the terminal branch of the facial nerve which innervates facial muscles and provides a tiny bit of GSA innervation to the auricle (see Ramsey Hunt syndrome!). At the point of injury here, the greter petrosal nerve, the beautiful chorda tympani and nerve to stapedius have already left the nerve and will not be affected. This rules out B, C, D and F. CN V innervates the masseter and provides sensory innervation to the face (E & G).
A 48-year-old female presents to the office with headaches, difficulty walking and vision loss. She first noticed the vision loss after backing into a parked car 3 days ago; she claims she has had difficulty walking for about the last 3 weeks. Her history is significant for a diagnosis and treatment of infiltrating ductal carcinoma in her left breast two years ago. A PET scan reveals three 2 cm tumors in the superior lobe of her left lung, one 3 cm tumor in the superior lobe of her right lung and two 3 cm masses in her cerebellum and a single 2 cm mass in her left occipital lobe.
i. Which of the following vessels was most likely involved in metastasis from the primary neoplasm to her right lung?
A. Inferior vena cava
B. Azygos vein
C. Internal jugular vein
D. Internal thoracic artery
E. Portal vein
F. Superior epigastric artery
ii. Which of the following vessels was most likely involved in metastasis from the primary neoplasm to her cerebellum?
A. Inferior vena cava
B. Internal carotid artery
C. Internal jugular vein
D. Internal thoracic artery
E. Middle cerebral artery
F. Portal vein
G. Superior epigastric artery
H. Vertebral artery
i. B
ii. H
Cancerous cells from the breast reach the lung through the venous system (azygos system) and can also reach the vertebral column and posterior fossa (brainstem & cerebellum) through the intervertebral plexus (i.e., Baton’s plexus).
If there are secondary tumors in the lung, these can spread through the pulmonary veins to the heart and then through the ascending aorta à subclavian a à vertebral arteries.
A 65-year-old female presents with her daughter and the chief complaints of headache, weakness and confusion. She is oriented to her name, but not the date or place; she can recall 1 of 5 items after 5 minutes. Physical examination reveals papilledema. Her muscle stretch reflexes are globally 3+; she has bilateral Babinski and Hoffman signs and pronator drift. A CT scan reveals the accompanying image. What is the most likely diagnosis?
A. Epidural hematoma
B. Intraparenchymal hemorrhage
C. Intraventricular hemorrhage, lateral ventricle
D. Intraventricular hemorrhage, third ventricle
E. Subarachnoid hemorrhage, ambient cistern
F. Subarachnoid hemorrhage, cisterna magna
G. Subdural hematoma, acute
H. Subdural hematoma, chronic
CT scans of intracranial hemorrhage are popular on COMLEX and USMLE! And you may have to differentiate acute versus chronic blood.
The Correct Answer is H.
In fact, she has bilateral subdural hemorrhages that are chronic (been there for a week or so).
Remember that on CT, fresh blood is bright white (hyperdense = brighter than brain) and it “fades” (becomes hypodense = darker than brain) with time.
Remember:
Epidural = lemon shaped
Subdural = banana shaped
Subarachnoid = blood in sulci and/or cisterns (outlines the brainstem)
A 10-year-old male presents to the office with fever, unilateral ear pain and diminished hearing. Otoscopic examination reveals the result shown in the accompanying figure.
i. The Weber test will most likely be localized to the:
A. left ear
B. right ear
C. midline
ii. The Rinne test, on the left side, will most likely reveal:
A. A > B
B. A < B
C. Deafness
iii. The boy has:
A. Otitis externa and conductive hearing loss
B. Otitis externa and sensorineuronal hearing loss
C. Otitis media and conductive hearing loss
D. Otitis media and sensorineuronal hearing loss
E. Presbycusis and conductive hearing loss
F. Presbycusis and sensorineuronal hearing loss
G. Tinnitus and conductive hearing loss
H. Tinnitus and sensorineuronal hearing loss
The images show both of his tympanic membranes. Remember, the cone of light begins at the umbo and is directed anterior and inferior. The image on the left is the right tympanic membrane; the image on the right is the left tympanic membrane and shows otitis media. Otitis media results in conductive hearing loss. The answers are:
i. A
ii. B
iii. C
A 22-year-old female presents to the office with the chief complaint of right elbow pain. She claims that she first noticed this pain 3 days ago after playing racquetball. Physical examination reveals pain and tenderness over her lateral epicondyle on the right. She has intact pinprick sensation in her right forearm and hand. She has significant pain in wrist extension against resistance. This patient’s condition involves the attachment of which of the following muscles?
A. Abductor pollicis longus
B. Brachioradialis
C. Extensor carpi radialis brevis
D. Extensor indicis
E. Extensor pollicis longus
F. Supinator
The answer is C. The patient has lateral epicondylitis. This involves inflammation at the common extensor tendon (attachment of extensor carpi radialis brevis, extensor digitorum, and extensor digiti minimi). This condition can result in compression of the posterior interosseous nerve. This nerve innervates EI, APL, EPL and EPB but has no cutaneous distribution.
A 19-year-old male presents to the emergency room after injuring his left arm in an attempt to rollerblade down a flight of stairs about 30-minutes ago. He has his left upper limb in a makeshift sling and he refuses to move the limb. Radiographs of the limb reveal a midshaft humerus fracture. If there is nerve damage as a direct result of the fracture, what muscle will most likely show signs of dennervation? \n A.) 1st and 2nd lumbricals
B.) Biceps brachii
C.) Brachialis
D.) Deltoid
E.) Flexor carpi ulnaris
F.) Latissimus dorsi
G.) Palmar interossei
H.) Palmaris longus
I.) Supinator
J.) Supraspinatus
K.) Teres major
L.) Triceps brachii
Answer is “I”. Mid-shaft humerus fracture is a classic Step 1 scenario! The radial nerve is most likely injured (as it courses along the radial groove). Innervation to the triceps is from branches that arise superior to this injury, so the triceps are spared. Remember, the radial nerve innervates all muscles in the posterior compartments of the arm and forearm (and the brachioradialis). You should immediately think “drop wrist” and sensory loss over the dorsum of the hand between 1st and 2nd digits.



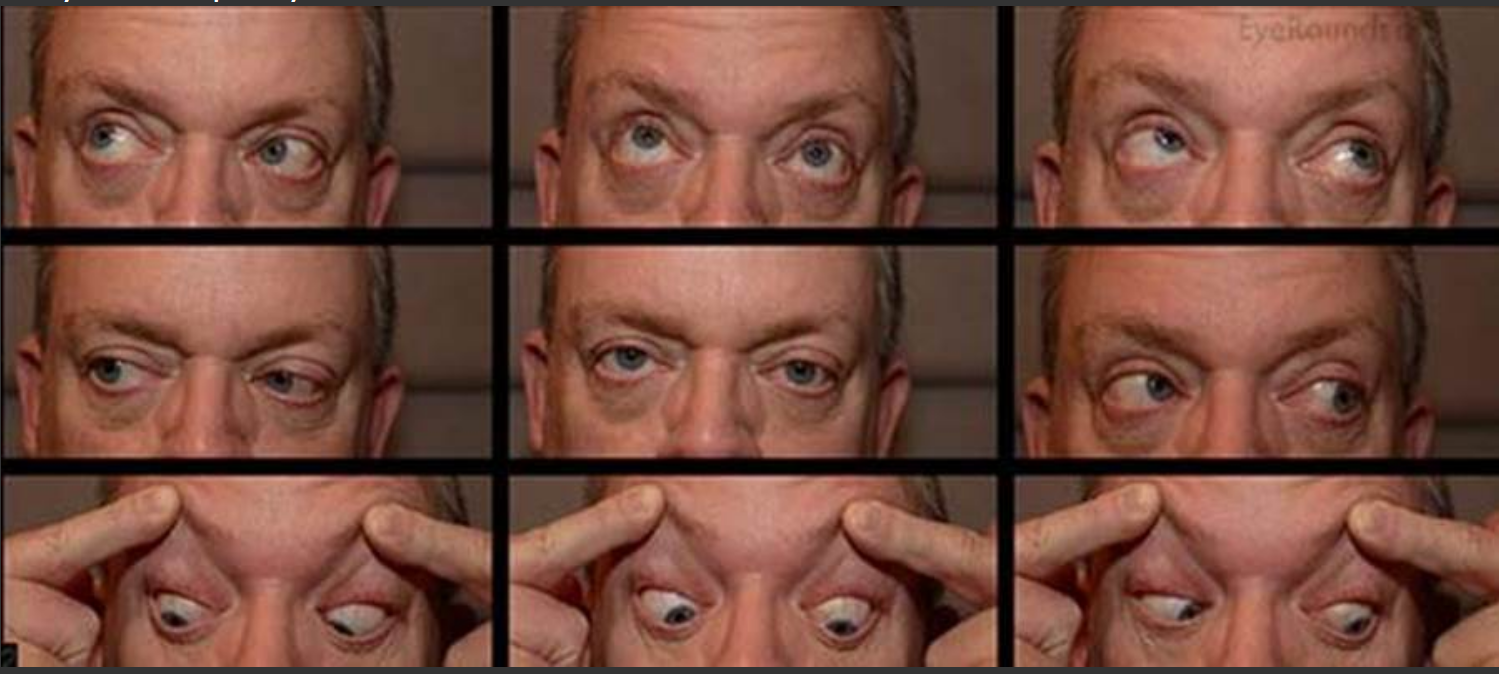

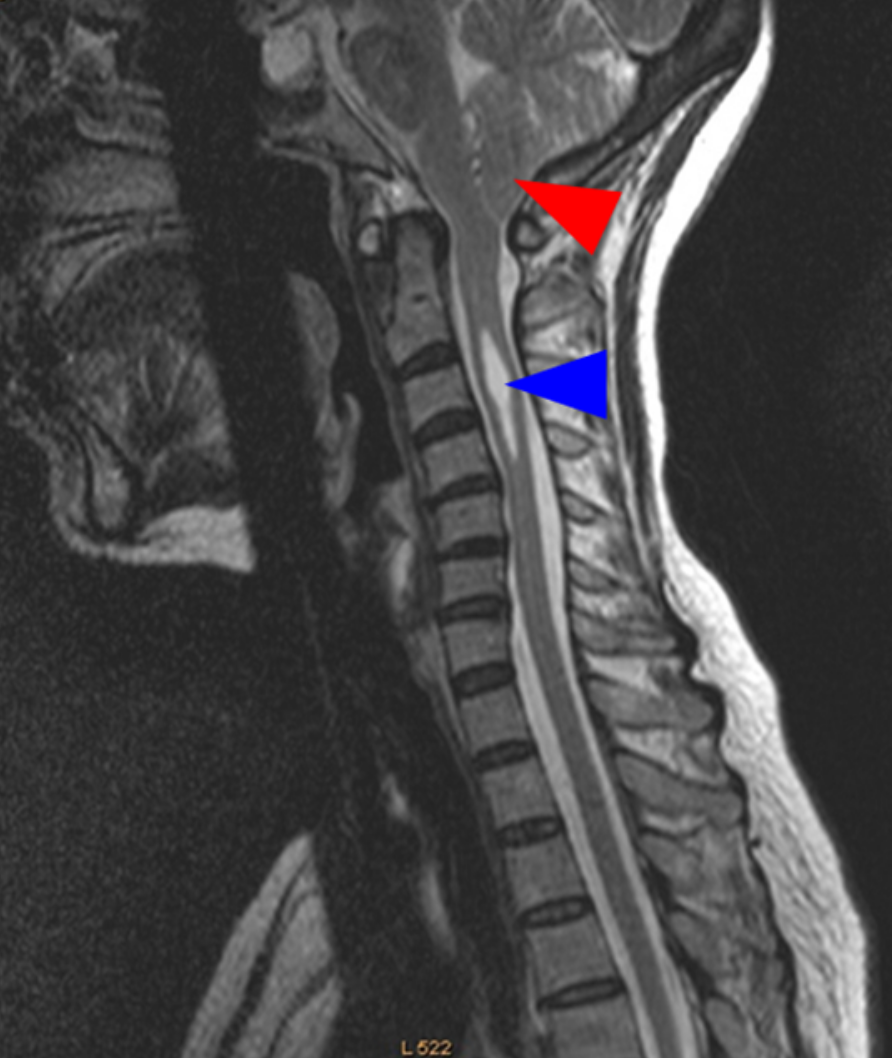
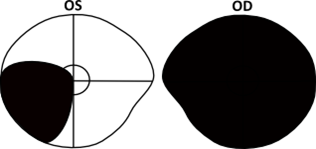
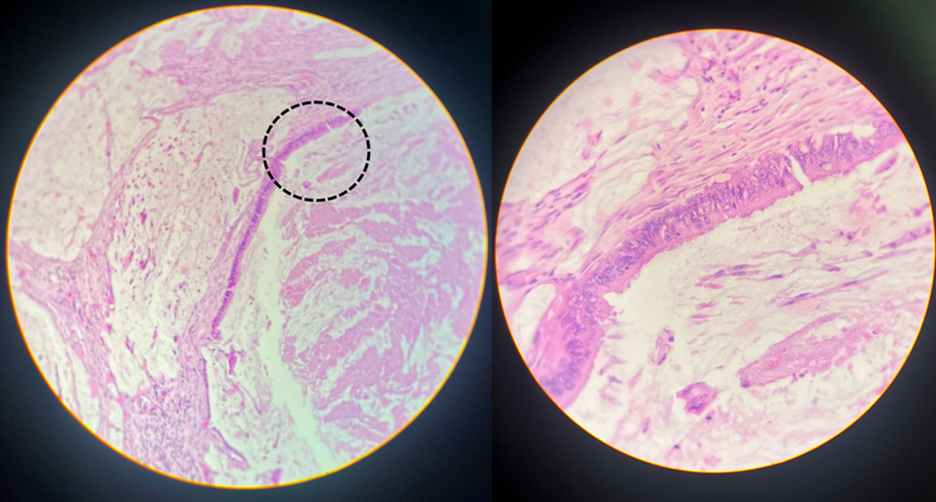
![<p>Patient A: [see accompanying image- red] A 24-year-old male presents to the emergency room after a skateboarding accident with the chief complaint of wrist pain. A radiograph of his wrist reveals the accompanying image. What is the diagnosis?</p><p>A fractured ulnar styloid and:</p><p>A.) Avulsion fracture of the first metacarpal</p><p>B.) Dislocated lunate</p><p>C.) Fractured scaphoid</p><p>D.) Fractured capitate</p><p>E.) Fractured hamate</p><p></p><p>Patient B: [see accompanying image- blue] A 74-year-old female presents to the emergency room with shoulder pain after a falling down her basement stairs. Physical examination reveals a proximal arm deformity and sensory loss over the lateral aspect of her proximal arm. Radiographs reveal the accompanying image. What muscle is most likely paralyzed?</p><p>A.) Biceps brachii</p><p>B.) Pectoralis minor</p><p>C.) Serratus anterior</p><p>D.) Subscapularis</p><p>E.) Supraspinatus</p><p>F.) Teres minor</p>](https://knowt-user-attachments.s3.amazonaws.com/6f4f4d2f4cec421b81558c6ad504ebb4.jpeg)