Looks like no one added any tags here yet for you.
diabetes mellitus
abnormally high plasma glucose concentration (hyperglycemia)
results from inadequate insulin secretion, abnormal target cell responsiveness or both
what are the types of diabetes?
type 1 diabetes
type 2 diabetes
gestational diabetes → around 20 wks pregnant
pre-diabetes (impaired glucose metabolism or borderline diabetes → can lead to type 2 diabetes)
contributing factors of diabetes
hereditary (not exclusively genetic)
diet related
lifestyle
symptoms of diabetes
polyruria - frequent urination due to excessive production of urine
polydipsia - frequent drinking due to excessive thirst
polyphagia - frequent eating due to excessive hunger → weight loss despite an increase in appetite
above symptoms are more for type 1 diabetes
type 2 diabetes symptoms are usually insidious (have no symptoms)
type 1 Diabetes
onset usually during childhood ( < age 10 )
faster onset and can be more dramatic (e.g. overnight)
autoimmune → possibly triggered by a virus
body attacks pancreatic β cells
type 2 diabetes
onset is for > 35 year olds
onset takes longer to occur
metabolic disorder → variations in enzymes → may not be optimal
risk factors of type 2 diabetes
obesity (high BMI)
physical activity
risk increases with age
ethnicity
gender (male > female)
urine measurements for diabetes
glucosuria → measuring the amount of glucose in urine
ketouria → if ketone bodies are being made in urine = high blood ketone levels → possible type 1 diagnosis / uncontrolled long term type 2 diabetes
fasted blood glucose
fast overnight (10-12 hrs)
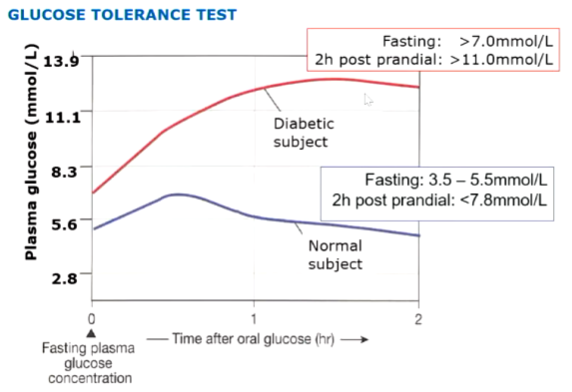
glucose tolerance test
fast overnight, then take blood sample, then drink a set glucose load, then take blood sample again an hr and 2 hrs from zero
fasted state
normal person: 3.5 - 5.5 mmol/L
diabetic person: > 7.0 mmol/L
fed state (2hrs post)
normal person: <7.8 mmol/L
diabetic person: >11.0 mmol/L → even after 2 hrs glucose levels have not dropped
glycated haemoglobin
aka glycosylated haemoglobin (HbA1c)
action of glucose non-enzymatically binding to haemoglobin
once haemoglobin is glycated (glucose bound), it loses its ability to transport oxygen
is a reliable indicator of diabetic control over the past 3-4 months
normal HbA1c: 4-6%
↑ HbA1c = ↑ risk of progression of diabetic complications (e.g. diabetic nephropathy)
blood insulin
not commonly measured
complications of diabetes mellitus
neuropathy → weakness, numbness and pain from nerve damage
nephropathy → kidney disease
retinopathy → patchy vision
diabetic ulcers
amputations
diabetic coma
death
increased chance of having a stroke
blood glucose control
glucose dependent insulin secretion is modulated by a number of hormones and neurotransmitters released from peripheral ANS
ACh facilitates the release of insulin in a glucose-dependent fashion via M₃ receptors on pancreatic β-cells
hormones: glucagon and adrenalin indirectly stimulate insulin release by promoting glucose entry into the blood stream
somatostatin inhibits glucagon and insulin release
glucose levels and fed/fasted state
before eating, an individuals glucose levels are low
after eating, blood glucose levels rise
glucose levels fall over time
insulin amounts should correlate with blood glucose levels
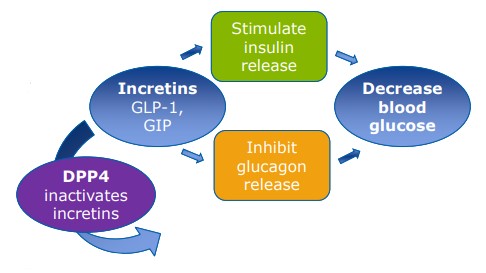
what are incretins?
promote secretion of insulin to decrease blood glucose levels
produced and secreted by GIT (enteroendocrine cells - L cells in ileum)
e.g. glucagon-like peptide 1 (GLP-1)
what are the physiological effects of incretins on the pancreas?
increase insulin secretion from β cells
suppress glucagon secretion from α cells
what are the physiological effects of incretins on the GIT?
delay gastric emptying
decrease gastrointestinal peristalsis
what is the bioavailability of incretins?
has a short half-life (1-2 min) in blood
rapidly degraded by dipeptidyl peptidase-4 (DPP4) → inactivates incretins
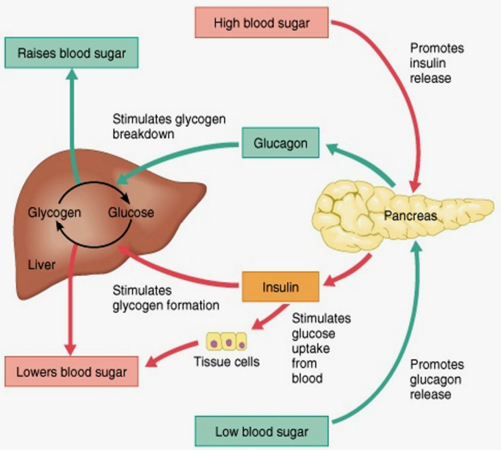
what is the hormonal balance in the fed state?
insulin dominates to reduce blood sugar levels and package glucose away after eating
what is the hormonal balance in the fasted state?
glucagon dominates to increase blood sugar levels
after 18 hrs of fasting - starved state → liver depleted of glycogen → gluconeogenesis
glucose transporters
are protein channels in cell membranes that facilitates movement of glucose across membrane
cell membranes are fatty lipid bilayers while glucose is hydrophilic
→ as such, glucose cannot easily cross cell membranes
GLUT 1
glucose transporter 1 protein
location:
brain
kidney
colon
placenta
erythrocyte
function:
uptake of glucose
GLUT 2
location:
pancreatic β cells
liver
small intestine
kidney
function:
rapid uptake and release of glucose
GLUT 3
location:
brain
kidney
placenta
function:
uptake of glucose
GLUT 4
location:
adipocyte
heart
skeletal muscle
function:
insulin stimulated glucose uptake
GLUT 4 is the only glucose transporter that requires insulin
GLUT 5
location:
small intestine
function:
absorption of glucose
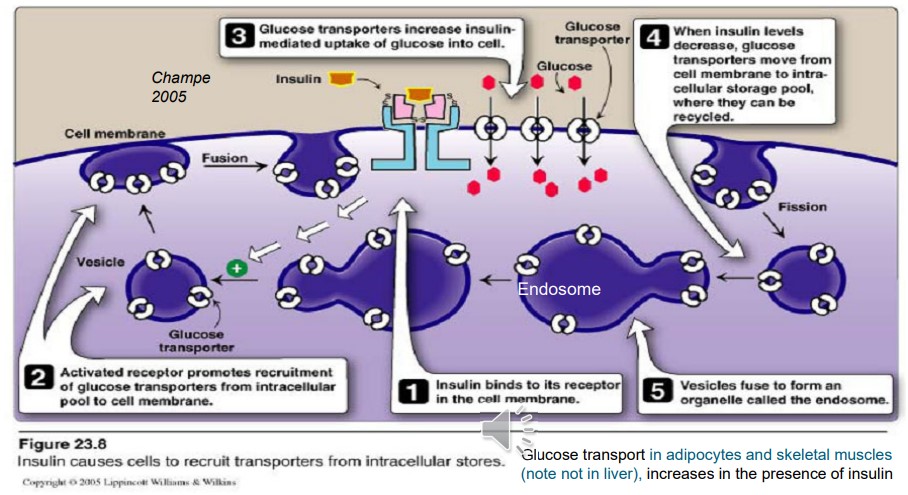
membrane effects of insulin
insulin binds to an insulin receptor in the cell membrane
activated receptor promotes recruitment of insulin-sensitive glucose transporters from the intracellular pool to the cell membrane
glucose transporters then become embedded in the cell membrane and increase insulin mediated uptake of glucose into cell
this then promotes the storage of glucose into glycogen, protein or fat
when insulin levels decrease, glucose transporters move from cell membrane to the intracellular storage pool, where they can be recycled
vesicles fuse to form an organelle called the endosome
what is hyperglycaemia?
increased blood glucose levels in blood
normal response to hyperglycaemia
an increase in BSL is detected by the pancreas
pancreas releases insulin
graded amount depending on what level of glucose is detected
insulin binds to insulin receptors on adipocytes and muscle cells
glucose transporters (GLUT4) are recruited to the surface of the cell membrane to allow for glucose entry into the cell → contributes to the production of TGs and amino acids
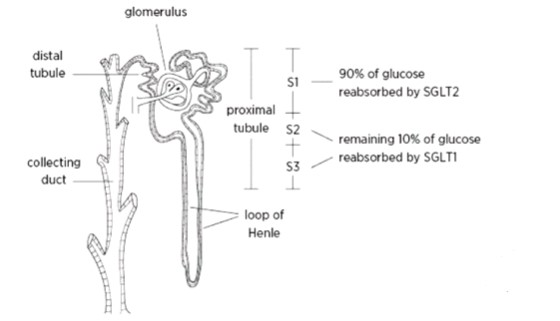
renal absorption of glucose
glucose is reabsorbed thru the proximal tubule via sodium-glucose transporters (SGLT1 and 2)
concentration gradient of sodium pulls glucose back in (glucose goes against its concen gradient)
transporter requires both Na and glucose to bind for it to work
SGLT₁ + SGLT₂
location:
small intestine
kidney
function:
active uptake and reabsorption of glucose
glucose homeostasis via kidneys
transfers all plasma glucose into urine within the nephron, but subsequently completely reabsorbs the filtered glucose (via SGLT1 and SGLT2), unless plasma glucose reaches a threshold of ~180mg/dL (10mmol/L)
therefore, under physiological conditions, no glucose is present in the urine
when threshold is exceeded, SGLTs become saturated and excess glucose is excreted → glucosuria
SGLT2 is highly expressed in the epithelial cells of the proximal tubule
in healthy humans, SGLT2 is responsible for 80-90% of renal glucose reabsorption
SGLT2 is the recent target for drug therapy in patients with type II DM
pathophysiology of type 1 diabetes
high blood glucose levels
pancreas produces little to no insulin
person will start shedding muscle because adipocytes (muscle cells) will think there is no sugar available → rapid weight loss
tissues require insulin to uptake glucose
insulin sensitive cells do not identify glucose as there is no insulin
therefore they feel starved and will try to make glucose for energy
solubilise muscle and fat deposits → produces glucose and ketone bodies
ketogenesis
more ketone body synthesis than normal
breakdown of glucose for energy (glycolysis), fatty acids and amino acids = acetyl CoA formation
acetyl CoA enters TCA cycle
if there is excess acetyl CoA, it forms ketone bodies
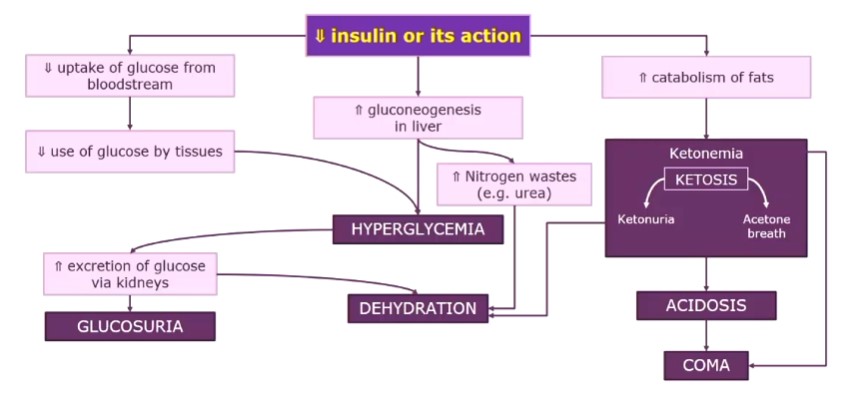
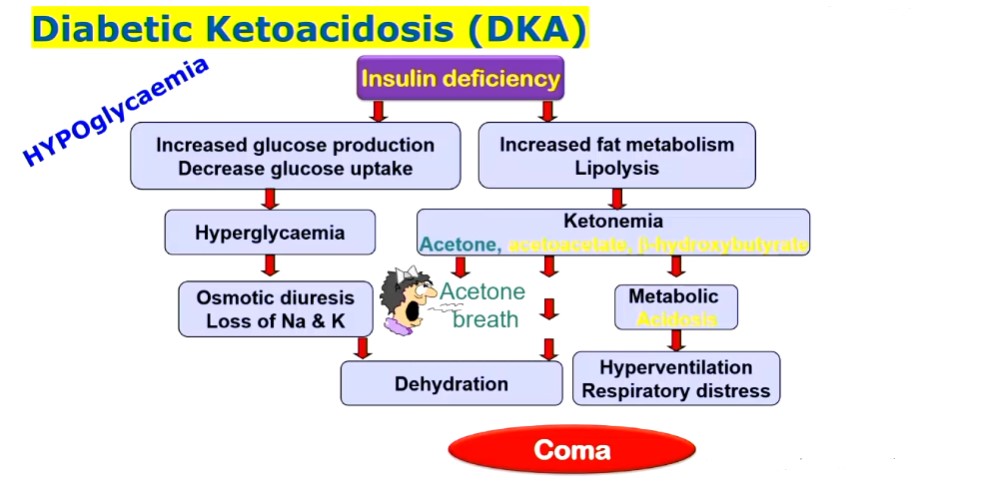
diabetic ketoacidosis
insulin deficiency → increased glucose production (gluconeogenesis) BUT decreased glucose uptake = hyperglycaemia → increased excretion of glucose (and water) via kidneys = dehydration
insulin deficiency → increased fat metabolism (lipolysis) → ketonemia (high amount of formation of ketone bodies) = acetone breath, metabolic acidiosis → hyperventilation respiratory distress
pathophysiology of type 2 diabetes
diminished effects of insulin → pancreas produces a normal amount of insulin but it is ineffective
blood glucose levels are normal, insulin builds up so insulin levels are high
however shedding of fats and proteins still occur, but at a slower rate
adipocytes break down to produce glycerol → undergoes gluconeogenesis to produce glucose
although they are shedding more than normal, you may not pick up any ketone bodies as it is happening at a much slower rate
glucose lowering medications
replenish insulin
insulin injections (mainly for type 1 but may be used in combination therapy for type 2) → but risk of hypoglycaemia if too much insulin is used
increase insulin secretion
promote insulin action
increase incretin levels
slow intestinal digestion/absorption of carbohydrates
reduce glucose reabsorption in kidneys (SGLT2 inhibitors)
important drug related sites for diabetes
gut
small instestine
different glucose transporters → absorption
incretins = ↑ insulin secretion
pancreas
rapid glucose uptake
GLUT2
glucokinase metabolism
synthesis, storage and release of insulin
liver
rapid uptake and release of glucose
GLUT2
insulin receptor binding stimulates glycolysis and inhibits gluconeogenesis
fat and striated muscle (heart and skeletal)
insulin dependent uptake of glucose
GLUT4
kidneys
active reabsorption of glucose
filters all, reabsorbs with sodium
SGLT co transporters
diabetes insipidus
occurs when the body cannot balance fluid levels in a healthy way
fluid in the blood is filtered thru kidneys to remove waste and afterwards most of it is reabsorbed with a small amount leaving the kidneys along with waste
ADH (vasopressin) is required to reabsorb the fluid filtered by the kidneys back into the blood stream
in diabetes insipidus, conditions that cause the brain to make too little ADH/ disorders that block the effect of ADH cause the body to make too much urine
central diabetes insipidus
lack of ADH released in the body due to the pituitary gland or hypothalamus in the brain being damaged/unable to respond to a decrease in osmolality
as such the production, storage and release of ADH is affected
nephrogenic diabetes insipidus
kidneys are unable to respond to ADH
due to V2 ADH receptor mutation and/or AQP2 gene mutation
urinary system
2 kidneys → produce urine from blood
urine travels down paired ureters
stored in urinary bladder
forced through urethra and expelled
function of the kidney
to maintain homeostasis by regulating volume and composition of blood:
achieving electrolyte balance
controlling blood pH
excretion of nitrogenous and other waste products
but more specifically:
H₂O regulation
inorganic ion balance
body pH regulation
removal of metabollic waste from blood
gluconeogenesis (glucose from amino acids)
hormone secretion
erythropioetin → stimulates production of RBCs
renin → BP regulation
activation of vitamin D
gives hormonally active metabolite → calcitriol
water balance
urine → 60% of water loss
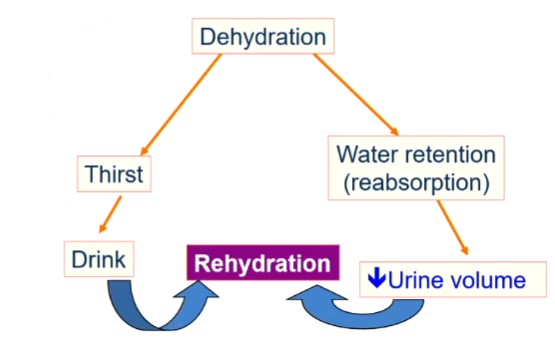
dehydration
results in ↑ water retention (reabsorption) = ↓ urine volume → rehydration
also results in thirst → if person responds to it, they will drink → rehydration
kidney anatomy
located close to spinal chord
account for 0.4% of body weight (150g) each
surrounded by adipose tissue → limits injury
collagen fibres hold renal capsule to surrounding tissue
secretional anatomy of the kidneys
has 1.25million nephrons per kidney
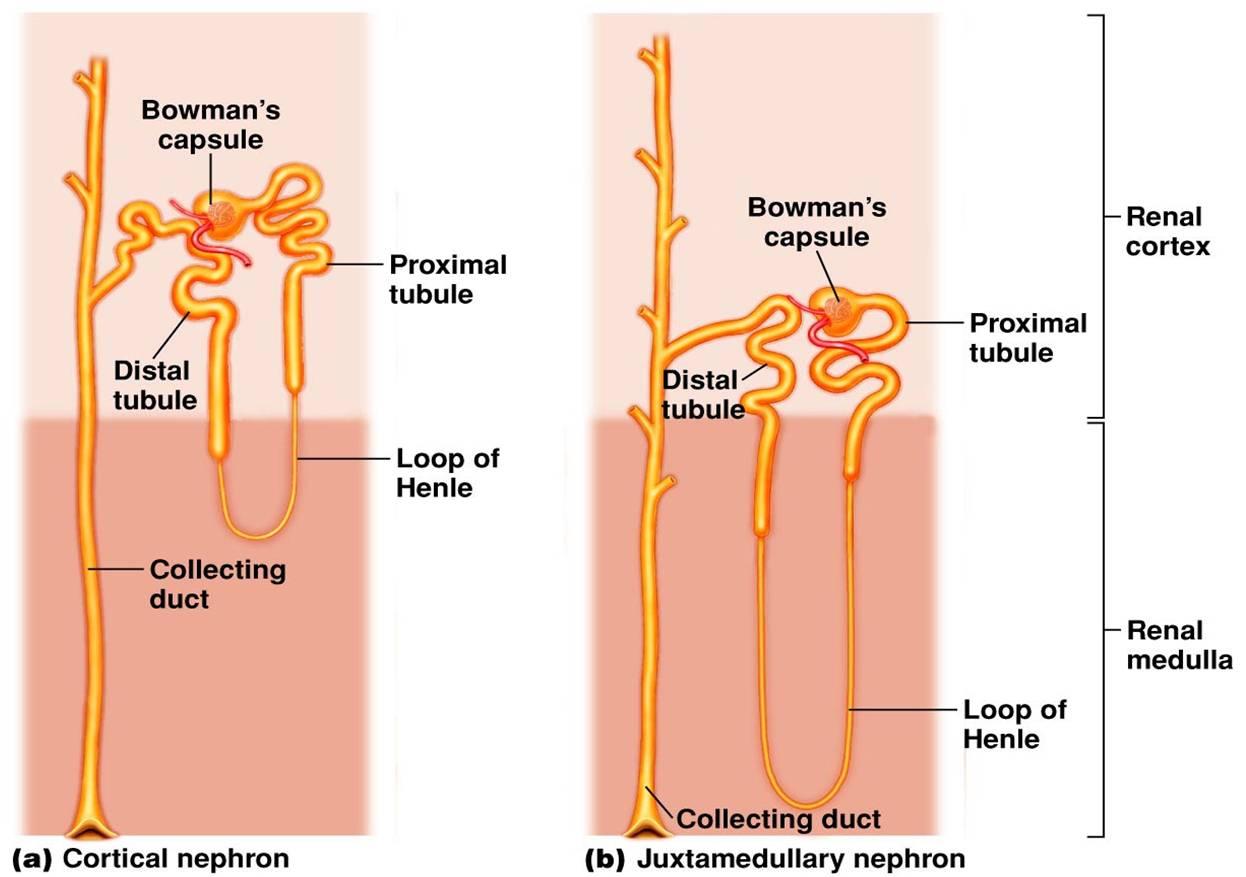
cortical nephron - most abundant (85%), most reabsorption/secretion
juxtamedullary nephron - less abundant (15%), concentration of urine
has a more pronounced loop of Henle (deep into the medulla) → better at concentrating urine
vascular components of the nephron
afferent arteriole
glomerulus (glomerular capillaries)
efferent arteriole
peritubular capillaries
afferent arteriole
carries blood towards/to the glomerulus
glomerulus
tuft of capsules that filters a protein free plasma into the tubular component
efferent arteriole
carries blood away from the glomerulus
peritubular capillaries
supplies the renal tissue
involved with exchanges with the fluid in tubular lumen
tubular component of the nephron
Bowman’s capsule
proximal tubule
loop of Henle
distal tubule and collecting duct
Bowman's tubule
collects the glomerular filtrate
proximal tubule
uncontrolled reabsorption + secretion of selected substances
due to high concentration of mitochondria
loop of Henle
in juxtamedullary nephrons only → establishes osmotic gradient in renal medulla which allows kidney to produce urine of various concentrations
distal tubule + collecting duct
variable, controlled reabsorption of Na⁺ and H₂O
variable secretion of K⁺ and H⁺
fluid leaving duct is urine, which then enters renal pelvis
juxtaglomerular apparatus
produces substances involved in the control of kidney function
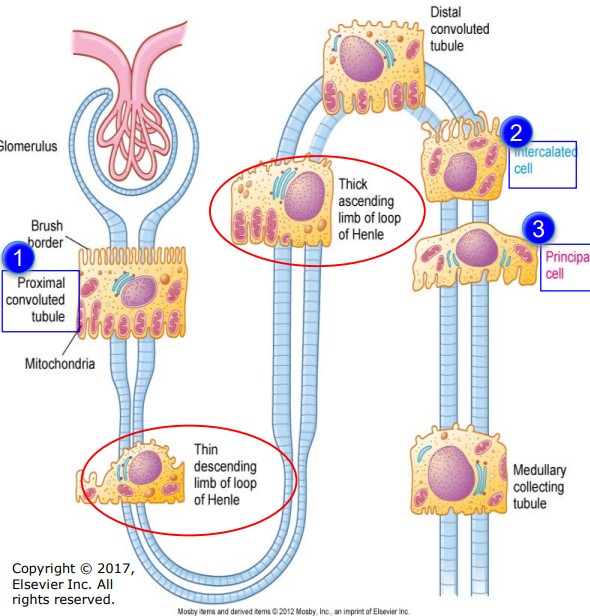
epithelial cells of segments of nephron tubules
proximal tubule
high no. of mitochondria
promote reabsorption of glomerular filtrate
intercalated cells
secrete H+/HCO3-
reabsorb K+
principal cells
reabsorb Na+ and H2O
secrete K
glomerular filtration (GF)
non-discriminant filtration of protein-free plasma from glomerulus into Bowman's capsule
mostly protein free → all constituents except for red blood cells and plasma protein
i.e. H2O, nutrients, electrolytes (ions Na+, Cl-, HCO3-, wastes (urea), etc.
fluid must pass through 3 layers of glomerular membrane:
pores between fenestrations within endothelial cells of the glomerular capillary wall
an acellular basement membrane composed of collagen and glycoproteins (negatively charged)
filtration slits between the foot processes of the podocytes in the inner layer of the Bowman’s capsule
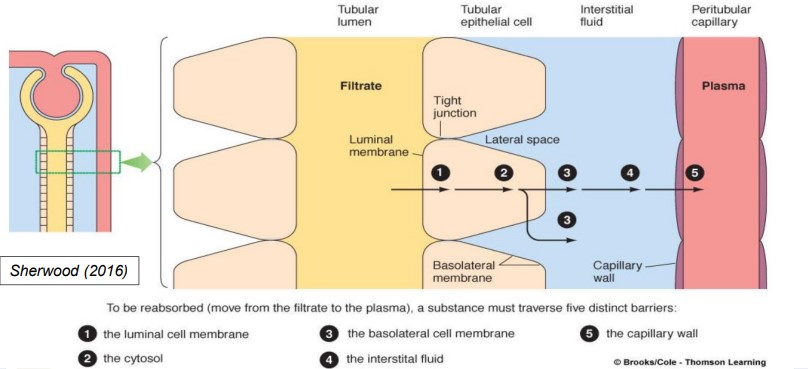
tubular reabsorption (TR)
highly selective movement of filtered substances from the tubular lumen into the peritubular capillaries
essential materials returned to blood (maintain composition and volume for constancy of internal environment)
keeps unwanted filtered material in tubular fluid to be excreted as urine
amount excreted = amount secreted + amount filtered - amount reabsorbed
tubular secretion (TS)
selective movement of non-filtered substances from the peritubular capillaries into the tubular lumen
involves trans-epithelial transport but in opposite direction to reabsorption
second route of entry into tubules for select substances
therefore hastens elimination of certain compounds
amount excreted > amount filtered
basement membrane
acellular → lacking cells
large plasma proteins cannot be filtered → can’t pass thru capillary pores
however pores are just barely large enough to allow albumin to pass thru
albumin → smallest plasma protein
gelatinous layer → negatively charged layer of collagen and glycoproteins
discourages filtration of small plasma proteins (repels albumin + other plasma proteins which are also negatively charged)
however the <1% of albumin that filters thru are picked up by the proximal tubule (via receptor mediated endocytosis) → degraded into AAs that are returned to the blood
urine is generally protein free
diseases characterised by albuminuria (albumin in urine) are a result of disruption of the -ve charges within the basement membrane which makes the glomerular membrane more permeable to albumin
forces involved in glomerular filtration
filtration as per other capillaries, except:
glomerular capillaries are more permeable than other capillaries
balance of forces across the glomerular membrane is such that filtration occurs across the entire length of the capillaries
efferent is narrower than afferent
three passive physical forces that accomplish GF
glomerular capillary blood pressure (P GC)
pressure exerted by blood in glomerular capillaries
depends on heart contraction and resistance of blood flow offered by afferent and efferent
plasma-colloid osmotic pressure (𝛑 GC)
proteins do not pass to Bowman’s capsule (BC)
concentration of H2O is higher in Bowman’s capsule
results in H2O moving by osmosis down its concen gradient from the BC into glomerulus → opposes the GF
Bowman’s capsule hydrostatic pressure (P BC)
pressure exerted by the fluid in the initial part of the tubule
tends to push fluid out of BC and opposes filtration of fluid from glomerulus into BC
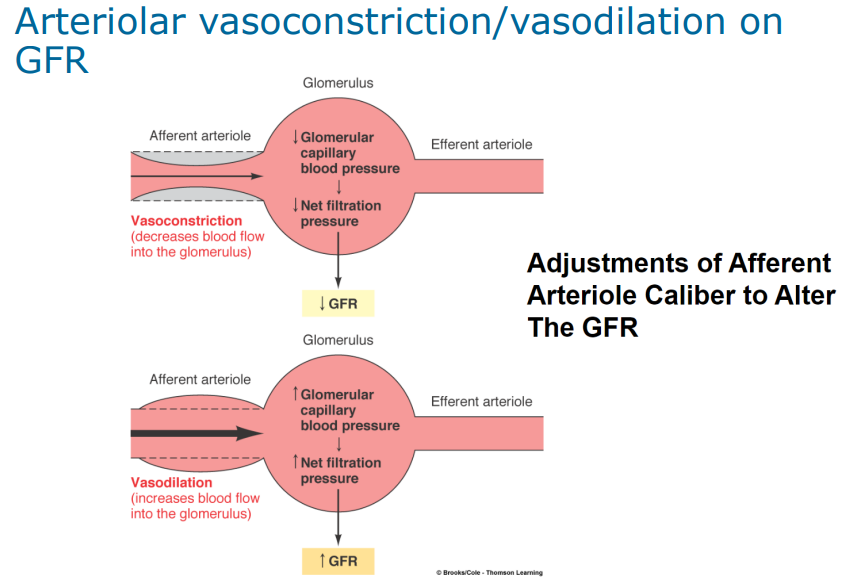
effect of arterial pressure on glomerular filtration rate (GFR)
efferent arteriole is narrower than afferent
afferent carries blood to glomerulus
efferent carries blood away from glomerulus
basically: whatever doesn’t leave the glomerulus via the efferent arteriole will get filtered out - hence the glomerular filtration rate
vasoconstriction: ↓ blood flow into glomerulus = ↓ GFR
vasodilation: ↑ blood flow into glomerulus = ↑ GFR
glomerular filtration rate (GFR) is directly related to…
renal blood flow
which is regulated by:
autoregulatory mechanism (tubuloglomerular feedback)
neural regulation
hormonal regulation
tubuloglomerular feedback
is the principal intrinsic autoregulatory mechanism
keeps renal blood flow, and thus GFR relatively constant
macula densa cells in distal tubule sense change in filtered Na+
↑GFR and ↑Na+ = macula densa cells stimulate afferent arteriole to vasoconstrict, thus reducing GFR
↓GFR & ↓Na+ = macula densa cells stimulate afferent arteriole to vasodilate therefore increasing GFR
neural regulation
kidney blood vessels (afferent and efferent arterioles) are innervated by the ANS mainly by sympathetic fibres
stimulation → renal arteriolar vasoconstriction = ↓renal blood flow = ↓GFR
stimulation is achieved when…
there is a decrease in the systemic arterial bp
exercise
haemorrhage
severe hypoxia (low O2 levels)
also participates in hormonal regulation of renal blood flow
no significant parasympathetic innervation
hormonal regulation
renin-angiotensin system activation ↳ ↑ renal blood flow → ↑ GFR
renin: an enzyme made and stored in cells of arterioles in juxtaglomerular apparatus
its release is stimulated by:
↓ BP in afferent arterioles
↓ [NaCl] in distal convoluted tubule
sympathetic nerve stimulation of β-adrenergic receptors on juxtaglomerular cells
RAAS exerts physiological effects stabilise blood pressure and preserve extracellular fluid (ECF) volume during hypotension / hypovolemia
this occurs via:
↑ Na⁺ reabsorption
sympathetic nerve stimulation
systemic vasoconstriction
thirst stimulation and drinking
tubular processes
highly selective + variable
quantity reabsorbed depends on amount required to maintain proper composition and volume of internal fluid volume
tubular reabsorption
transfer of substances from tubular lumen into the peritubular capillaries (involves transepithelial transport)
essential materials filtered are returned to the blood
tubular secretion
involves transepithelial transport but in the opposite direction to reabsorption
second route of entry into tubules for select substances
therefore hastens elimination of certain compounds
trans-epithelial transport
passive transport → occurs down electrochemical / osmotic gradient
active transport → occurs against electrochemical gradient
requires energy (e.g. ATP or cotransporter, SGLT1)
e.g. movement of glucose, amino acids and other organic nutrients, Na⁺, electrolytes (PO₄³⁻)
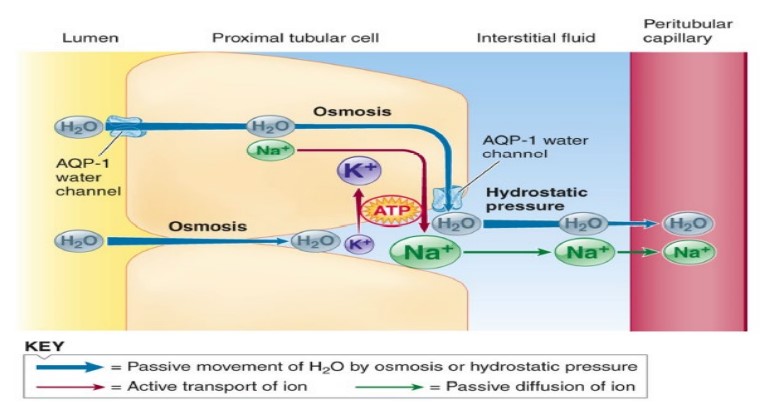
Na⁺ (and Cl⁻) absorption
basolateral Na⁺ / K⁺ pump actively transports Na⁺ from tubular cell to interstitial fluid within the lateral space
establishes concentration gradient for passive movement of Na+ from interstitial fluid to peritubular capillary
high concen of Na+ in interstitial fluid → low concen in capillary
active Na⁺ reabsorption allows for passive reabsorption of Cl⁻ and H₂O in urea
electrochemical gradient generated by Na⁺ → drives reabsorption
H₂O reabsorption
passive reabsorption through length of tubule
osmotically follows actively reabsorbed Na⁺
via water channels (aquaporins, AQPs)
AQP-1 → proximal tubule which are always open
AQP-2 → in principle cells in distal parts of nephron which open in response to ADH/vasopressin
glucose + amino acids
kidneys maintain glucose levels in blood
transfers all plasma glucose into urine within the nephron, but subsequently completely reabsorbs the filtered glucose (via SGLT1 and SGLT2) UNLESS plasma glucose reaches a threshold of 180mg/dL (10mmol/L)
therefore, under physiological conditions, no glucose is present in urine
when exceed threshold, SGLTs become saturated and excess glucose is excreted → glucosuria
SGLT2 is highly expressed in the epithelial cells of the proximal tubule
in healthy humans, under normal conditions, SGLT2 is responsible for 80-90% of renal glucose reabsorption
recent target for drug therapy in patients with type 2 diabetes → SGLT2
glucose reabsorption
Na⁺ dependent secondary active transport in proximal tubule
uses energy provided by concentration gradient of one Na+ molecule across the cell membrane to push another molecule (glucose/amino acid) against its concen gradient
Na+ is going down its concen gradient (higher in urine than blood)
while glucose is going against its concen gradient
Active SGLT₂ and GLUT₂ transport glucose in renal proximal tubule cell
tubular maximum
each carrier is specific for a specific type of substance
SGLT → glucose, not amino acids
limited number of each carrier type is present in tubular cells
upper limit on how much of a particular substance can be actively transported
tubular maximum (TM) is reached when all carriers are occupied → i.e. cannot take additional passengers at that time
any quantity of substance filtered beyond its TM is not reabsorbed and escapes into urine
with the exception of Na+, all actively reabsorbed substances have a Tm
aldosertone promotes the insertion of more active Na+/K pumps in the distal and collecting tubular cells
kidneys can regulate the reabsorption of some of the substances that display carrier-limited reabsorption, e.g. kidneys regulate PO₄³⁻ but not glucose
active reabsorption of electrolytes (PO₄³⁻)
PO₄³⁻ is actively reabsorbed + regulated by kidneys
transport carriers are located in proximal tubule
tubules can reabsorb PO₄³⁻ up to normal plasma concentration and excess spills into urine → excretion
reabsorption of PO₄³⁻ and Ca²⁺ is subject to hormonal control (parathyroid hormone can adjust the quantity conserved)
descending limb of the loop of Henle
highly permeable to H₂O → via abundant, always open AQP1 channels
doesn't actively reabsorb Na⁺
Na+ is leaked in but is not actively reabsorbed into tubular cell from lumen
ascending thin limb of the loop of Henle
impermeable to H2O
permeable to NaCl
ascending thick limb of the loop of Henle
impermeable to H2O
active reabsorption of NaCl
tubular secretion
same basic principle as reabsorption but in reverse direction
many substances that are reabsorbed are secreted at different parts of tubule
e.g. urea
most important substances are secreted by tubules:
H⁺, K⁺, urea and other organic anions and cations
urea movement in the nephron
always via passive diffusion
proximal tubule
mildly permeable to urea
reabsorption occurs as H₂O is reabsorbed so urea becomes concentrated in tubule
thin loop of Henle
secretion of urea due to greater concentration in surrounding interstitium compared to tubule
thick loop of Henle and distal convoluted tubule (DCT)
highly impermeable to urea
given large amount of H2O reabsorption → urea is highly concentrated
collecting ducts
highest permeability to urea
ADH promotes specific urea transporters to be added increasing permeability → reabsorption into interstitium
K⁺ secretion
one of the most abundant cations in the body → very impt in maintaining the resting membrane potential
majority (98%) of potassium is in intracellular fluid due to the Na⁺/K⁺ pump
since a relatively small amount of K⁺ is in the extracellular fluid (ECF), a slight change in the K⁺ load in the ECF can have a pronounced effect on the plasma K⁺ conc → huge effect on membrane excitability
plasma concentration is tightly controlled by kidneys
renal handling is complex
filtered K⁺ is almost completely reabsorbed in proximal tubule
most K⁺ in urine is from controlled K⁺ secretion in distal parts of nephron
secreted by principal cells
secretion is regulated to maintain desired K⁺ concentration
H⁺ secretion
important in regulating acid-base balance
secreted via
proximal tubule
intercalated cells of distal collecting tubules
extent secreted is dependent on acidity of body fluids → pH range of blood must be kept between pH 7.35 → 7.45
↑ [H⁺] = ↑ acidity → ↑ H⁺ secretion
↓ [H⁺] = ↑ alkalinity → ↓ H⁺ secretion
rate of secretion affected by K⁺ in distal parts of kidney (opposite effect)
↑ K⁺ secretion = ↓ H⁺ secretion
↑ H⁺ secretion = ↓ K⁺ secretion
kidney/renal function tests
used to indicate the health of the kidneys
blood tests
plasma/serum creatinine concentration → useful for chronic rather than acute kidney disease
↓GFR = ↑ plasma creatinine levels
blood urea nitrogen
urine tests
urinalysis → colour, turbidity, protein, pH, specific gravity, sediment and supernatant
urine protein
microalbuminuria
creatinine clearance
renal clearance
involves the liver, lungs and kidneys
is the volume of blood from which a substance/drug is completely removed by the kidneys per unit time (i.e. mL/min) per kg of body weight
reflects the excretion of a particular substance into the urine by the kidneys
drugs differ greatly in the rate at which they are excreted by the kidney
is an indirect measure of:
GFR
tubular reabsorption
tubular secretion
renal blood flow
CL renal = (urine flow rate x urine concentration)/plasma concentration
creatinine
is a waste product that comes from the normal wear and tear of muscles in the body
a breakdown product of creatine phosphate in muscle cells
usually produced at a constant rate
creatinine clearance (CrCl) rate
is used as a measure of renal function, and is a better indicator of than serum creatinine
is the vol. of plasma that is cleared of creatinine per unit time
is an approx. measure of the GFR
compares creatinine in a 24hr urine sample to blood creatinine levels from one blood sample
GFR and creatinine clearance
GFR is usually estimated (eGFR) from the results of a creatinine blood test and is normalised for body surface area → units are mL/min/1.73m²
for males: CrCl = [(140-age) x Wt] / [0.815 x Secr]
CrCl = creatinine clearance (mL/min)
age = years
Secr = serum creatinine (μmol/L)
Wt = ideal or actual weight, whichever is lower (kg)
for females: multiply the estimated value by 0.85
blood urea nitrogen (BUN)
test measures amount of nitrogen in blood that comes from the waste product urea
protein breakdown → urea
reflects GFR and urine-concentrating capacity
BUN rises if:
kidneys are not able to remove nitrogen from blood normally
may be due to:
↓ GFR = ↑ plasma urea concentration
heart failure
dehydration
diet high in protein
BUN drops if:
liver disease/damage
regulation of fluid balance involves…
ECF volume - includes circulating plasma volume
ECF osmolality - solute concentration
ECF volume
controlled by maintenance of salt balance
Na+ load determines ACF volume
primarily controlled by aldosterone
important in long term control of arterial BP
↓ ECF volume = ↓ arterial BP and vice versa
ECF osmolality
controlled by maintenance of water balance
primarily controlled via aldosterone
important in prevention of detrimental osmotic movement of water between ECF and ICF
↑ ECF osmolality (hypertonicity) → H2O leaves the cells → cells shrink
↓ ECF osmolality (hypotonicity) → H2O enters cells → cells swell
causes of hypertonicity (dehydration)
(in hypertonicity, H2O leaves the cells → cells shrink)
insufficient H2O intake
excessive H2O loss
diabetes insipidus (urinating a lot)