Passive Care - Exam 1 (modalities)
1/153
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
154 Terms
Electrophysical agents (EPAs)
electric stimulation, heat therapy, cold therapy, mechanical energy, light
EPAs are ______, rarely are they the sole therapeutic intervention
complementary
EPAs affect the patient’s ____ in the treatment area (change internal environment)
physiology
Passive care
Dr applies the intervention to pt, pt passively received therapy
Active care
Pt has to perform an activity to achieve a therapeutic effect
Does the cause of injury change the process of healing
NO!
4 stages of healing
hemostasis (sec/min)
inflammatory/acute (hr/days/wks)
proliferation/repair (wks/mo)
remodeling/maturation (mo/yrs)
Hemostasis
initial blood clotting to stop bleeding
Purpose of Inflammatory/acute phase
defend against foreign intruders (infection)
removing damaged tissue and debris
immobilize area
Avascular/poorly vascularized tissue
won’t heal well
Signs of inflammation
heat, red, swelling, pain, loss of function (Virchow)
Inflammatory/acute phase is characterized by
vasodilation
increased capillary permeability
phagocytosis by neutrophils and macrophages
Inflammatory chemicals that cause pain
bradykinin
prostaglandins
serotonin (pain-spasm cycle)
What is the goal of the inflammtory/acute phase
limit extent of inflammation and preserve ROM via active care
**non-damaged tissue needs protection + PRICE
Proliferation/repair phase is characterized as
angiogenesis (new capillaries)
fibroblasts, chondroblasts, osteoblasts
In the Proliferation/repair phase, the extracellular matrix contains
type III collagen (weak, disorganized, begin cross-linking)
proteoglycans
What is the goal of the proliferation/repair phase
encourage and increase proliferation
decrease pain and swelling
increase pain-free ROM
begin non-weight bearing proprioceptive training
Remodeling/maturation phase is characterized by
scar contraction (can lead to joint adhesion and loss of motion)
decrease blood vessels
Type III collagen gets replaced by _____ during the remodeling/maturation phase
type I
What is the goal of the remodeling/maturation phase
increase pain-free ROM
progress proprioceptive training
regain full strength + normal biomechanics
protect + strengthen residual joint stability
Secondary enzymatic injury
lysosomal enzymes released
not specific
damage to surrounding uninjured tissue
Secondary hypoxic injury (hemorrhage/clotting/edema/spasm/hematoma)
lead to decreased O2 and nutrition
damage to surrounding uninjured tissue
Tension on connective tissue causes
increased collagen fibril diameter and #
cross-linking
collagen fibril packing density
Collagen fibers that are aligned in an organized, parallel fashion forms
greatest # of cross-linking and possess optimal strength
Physiologic effects of electrical stimulation
decrease pain and muscle spasm
reduce edema
stimulate exercise by muscle contraction
stimulate healing
Electricity (flow of electrons)
requires source of electrons
driving force = electron imbalance
path = conductor
River comparison to fluid flow
electrons are drops of water in a river
current (flow of electrons) in the flow of the river (ampere)
voltage is the waterfall…height of waterfall inc = potential energy inc
Types of Resistance
length of conductor
cross sectional area
temperature
Monophasic/Galvanic/Direct Current (DC)
current flow in one direction
net charge = positive and negative electrode
charge builds in tissue
Biphasic/Alternating Current (AC)
flow of electrons changes direction regularly (changes polarity)
net charge = balance or unbalanced
wave form = symmetrical or asymmetrical
shape = sinusoidal, square, rectangular, triangular
An equal electrical charge in both phases of a biphasic/alternating current will
minimize/eliminate polarity effect in tissues
Phase duration
time it takes current to leave isoelectric line to when it returns
Monophasic
phase duration and pulse duration are SAME
Biphasic
TWO phase durations for each pulse
Tissues respond to
phase duration (NOT pulse duration)
Amplitude
intensity or magnitude of the current
**Sensory response before motor
Peak current
max amp of current regardless of duration
A-beta is close to ____ and has a ____ threshold and therefore is stimulated first
skin; lower
The deeper the penetration, the more neuron recruitment and there
muscle fiber recruitment possible
Average current
amount of current supplied over a period of time
**Too high → tissue damage
Strength duration curve
relationship btw amp (strength) of electrical current and phase duration
If the charge of the strength duration curve is sufficient to overcome capacitance of a nerve fiber it will
depolarize
Short strength duration curves require a ______ for a nerve response
higher amplitude
Long strength duration curves require a ______ for a nerve response
lower intensity
Targeting capacitance (alter phase duration and amplitude)
use patient feedback
Patient reports tingling but no muscle twitch, which fibers are stimulated
A-beta fibers ( no A-alpha motor neurons)
Muscle contraction - which fibers are stimulated
exceeded A-alpha motor neurons
Burning/needling sensation - which fibers are stimulated
exceeded A-delta fiber capacitance
If peak amplitude fails to exceed rheobase, what occurs
nerve will not depolarize regardless of phase duration
Chronaxie
time/phase duration required to depolarize a nerve fiber when a peak current is 2x rheobase
What provides the greatest comfort for the patient
amplitude is 2x rheobase
phase duration is slightly greater than chronaxie
Frequency
number of pulses or cycles generated per second (pps or Hz)
Frequency affects the number of _______ elicited during the stimulation
action potentials
Higher frequency leads to
summation (motor neuron = tetany)
Absolute refractory period
rate limiting factor of number of impulses that can be generated by a nerve
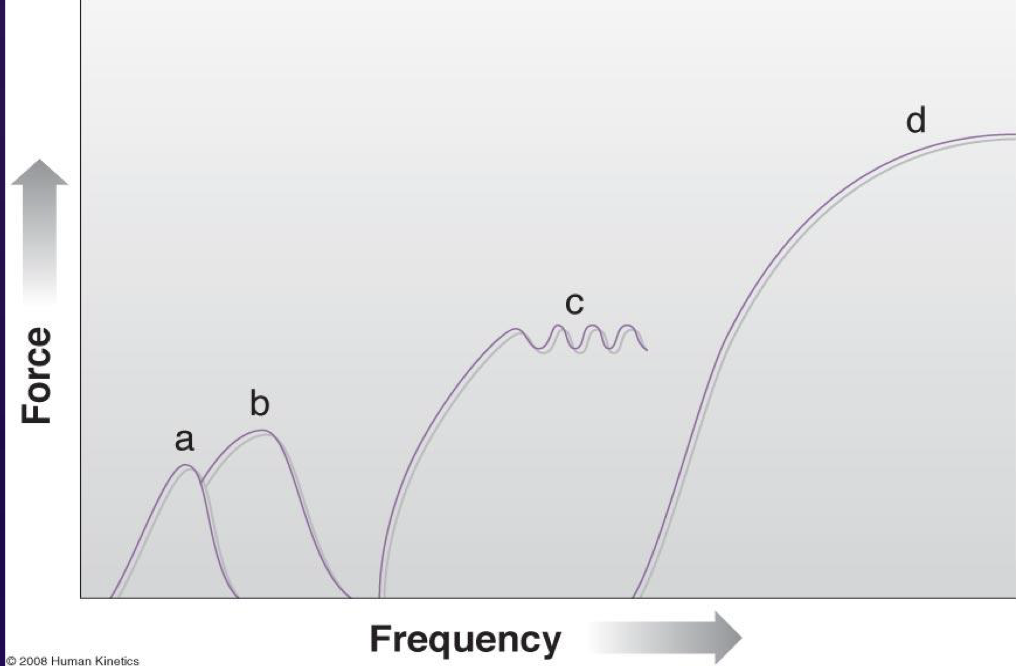
Temporal summation of muscle contraction
A - single twitch (cx and rx)
B - summation (force from 2 twitches, no rx)
C - unfused tetanus
D - fused tetanus (stays cx, no time to rx)
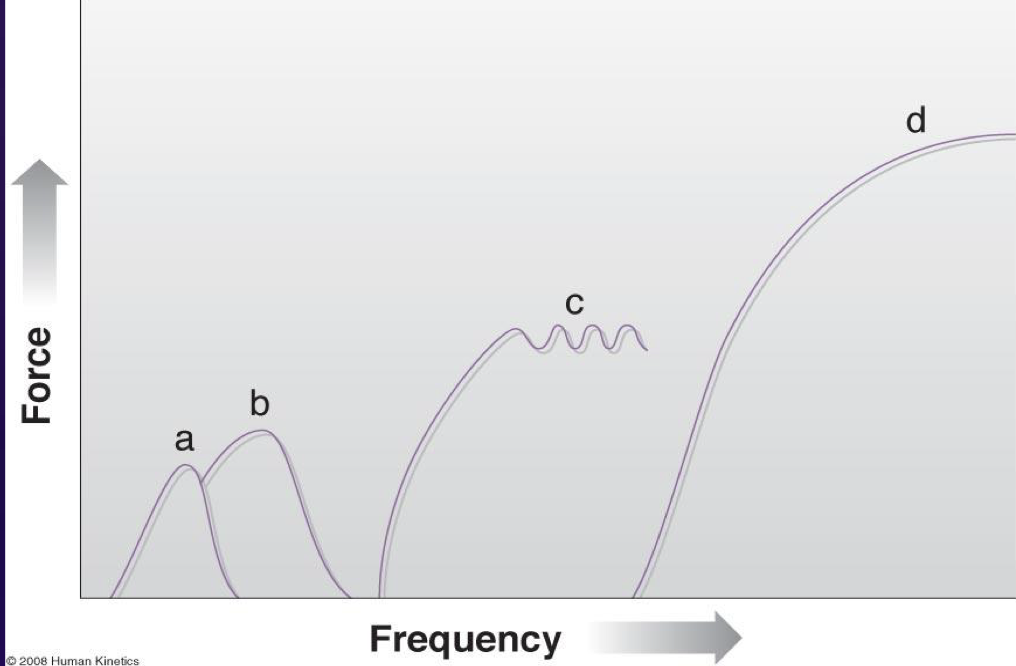
Which temporal summation do we want
D - fused tetanus (stays cx, no time to rx)
Wedensky’s inhibition
stimulation at high frequency near refractory period of sensory nerve
>1000 Hz
Action potential failure
What does Wedensky’s inhibition result in
anesthesia (no pain) between the electrodes
Low frequency generators
<1000 Hz (produce action potentials)
Medium/Treatment frequency generators
1000-100,000 Hz
Interferential - 3000-5000Hz
Russian - 2500 Hz
Intrinsic duty cycle of 10ms on and 10ms off (10:10) creates a
burst frequency of 50Hz
High frequency generators
>100,000 Hz
**can burn pt
**Diathermy uses this
Electrode considerations - there must be ____ leads to complete a circuit
2
If electrodes are placed close together, the current is concentrated in
superficial tissues
If electrodes are farther apart the current has the potential to take a deeper path through the
nerve and blood vessels that have less resistance
Electricity doesn’t go through what substance well
air
Monopolar electrode configuration
two or more unequal electrodes (1 active, 1 dispersive)
used w/monophasic or biphasic
Reasons for monopolar electrode configuration placement
leads placed far away creates deeper penetration
greater comfort at dispersive pad
creates an electrical field w/specific polarity
Bipolar electrode configuration
2 equal sized electrodes
used w/monophasic or biphasic
**MC in TENS
Quadripolar electrode configuration
two separate medium frequency currents placed as cross currents
**MC in Interferential
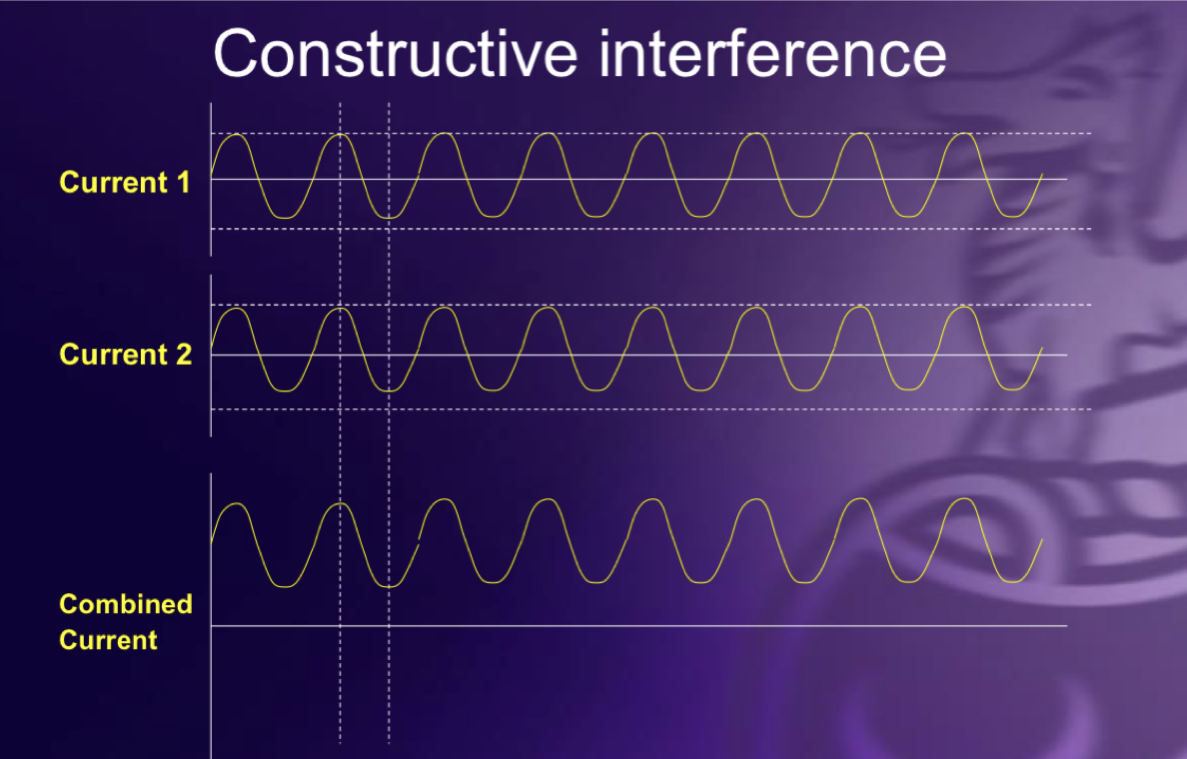
Constructive interference
2 sinusoidal waves exactly in phase combine
waves supplement each other
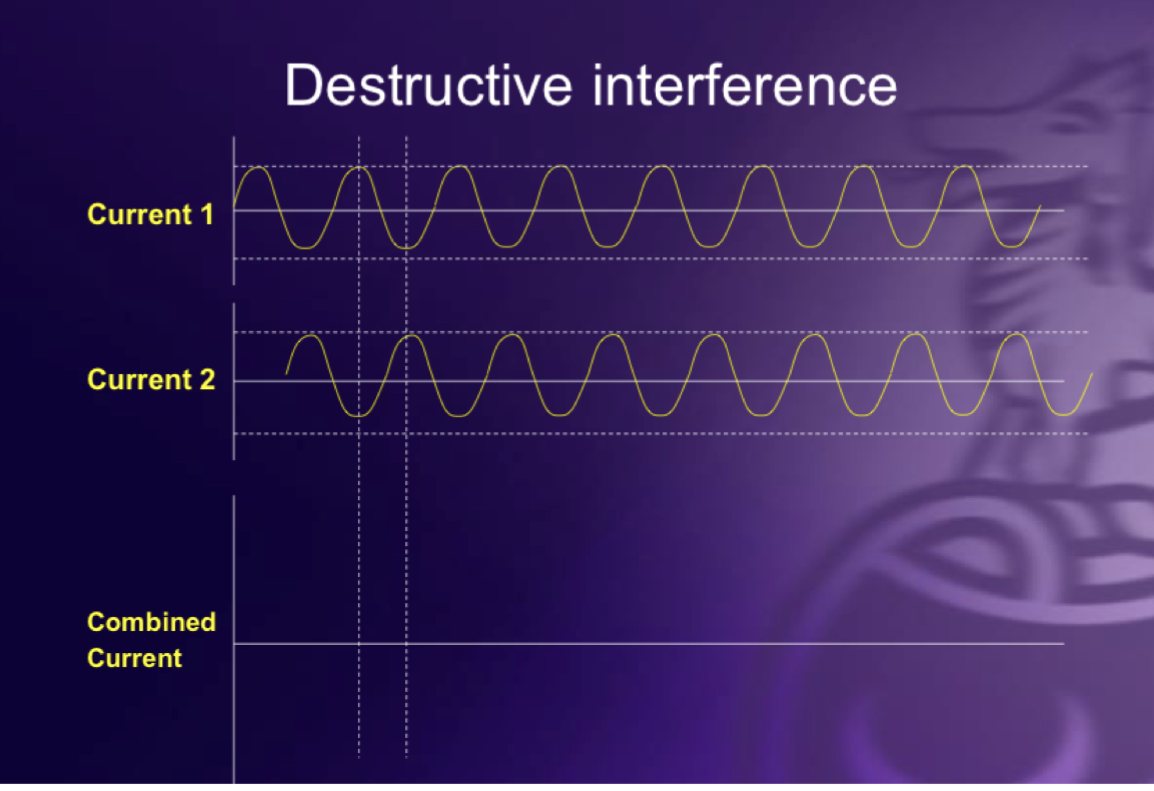
Destructive interference
2 sinusoidal eaves exactly OUT of phase
results in cancellation of both waves
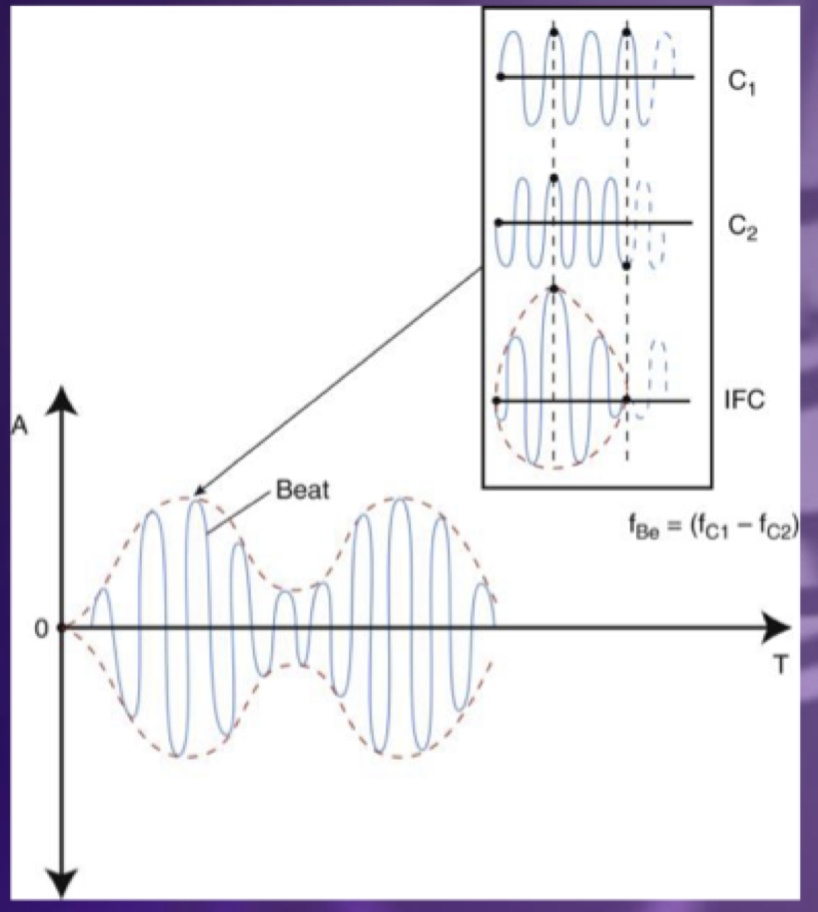
Heterodyne interference
combination of constructive and destructive interference
results in a wave with a beat effect
True Interferential current (3000-5000Hz)
2 channels, 4 electrodes (quadripolar electrode placement)
most intense where currents cross
treatment frequency is based on type of pain
Pre-modulated (pain relief)
1 channel, 2 electrodes (bipolar electrode placement)
interference occurs in machine, not body
Vector scan (larger tx area)
2 channels, 4 electrodes (quadripolar electrode placement)
cloverleaf pattern rotates
Stereodynamic
3 channels, 6 electrodes
3D interference pattern (6 petal flower shape)
Effects of IFC
pain reduction
muscle strengthening or re-education
slow bowel transit and increase circulation (not much evidence)
Interferential Treatment (beat) frequency for pain
acute = 80-150
subacute = 1-150
chronic = 1-15
Interferential treatment time and amplitude for pain
15-20min
amplitude = pt comfort
Pre-mod treatment (beat) frequency and duty cycle for strength
40-60 Hz
10:50 w/ramp time
Pre-mod treatment amplitude
pt comfort
Contraindications for Interferential and Russian Current
anterior cervical area, through chest/head
pacemakers, ICD, metal implants
abdomen/pelvis/lumbar areas of pregnant women in 1st tri
epilepsy, areas of hemorrhage, damaged skin
confused and unreliable pts
unknown etiology
Risks of interferential current
skin irritation
diathermy devices (10ft away)
Indications of Russian current
muscle re-education + retard atrophy
muscle strengthening
decrease muscle spasm through fatigue
Carrier frequency, burst frequency, and pulse rate of Russian current
carrier = 2500 Hz
burst = 50 Hz
pulse rate = 50 Hz
The carrier frequency of Russian current results in
maximally summated muscle contraction
In order to cause tetanus muscle contractions, the pulse rate has to be at least
>35 Hz
**Notes: more doesn’t cause stronger cx it promotes fatigue
Russian Current amplitude
pt tolerance
Russian current duty cycle for muscle strengthening (retard atrophy/retrain muscle)
10:50 (on/off percentage = 16.7%)
10 contractions
Russian current duty cycle for muscle fatigue (spasms)
10:10
Russian current ramp time
0.5-2 seconds
mimics voluntary contractions + eases pt into stimulation
What ramp time is the closest to actual physiological muscle contraction
0.5
Electrode placement always needs to be
parallel to muscle fibers
at motor points (btw belly and tendon/musculotendon junction)
Russian current electrode configurations
monopolar (2 unequal sized electrodes) - active electrode over target
bipolar (2 equal sized electrodes) - single muscle protocol
quadripolar (4 electrodes) - agonist/antagonists
Russian current - quadripolar 1 channel w/split lead for one muscle
used for larger muscles (single muscle protocol)
Russian current - 2 channels w/Simultaneous Co-contract
used for larger muscles (core muscles)
bilateral muscles contract together
Russian current - Reciprocal protocol
channel 1 is on while channel 2 is off
agonist and antagonist contracts alternately
Too much overlap in reciprocal russian can cause
agonist/antagonist fights