BIOL 2048 - Autonomic Nervous system
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
21 Terms
roles of the ANS
homeostasis —> sensory input leads to either hormonal or neuronal response
pupilaary dilation
dilation and constriction of blood vessels
force and rate of heart beat
secretion of glands
energy metabolism - liver and skeletal muscle
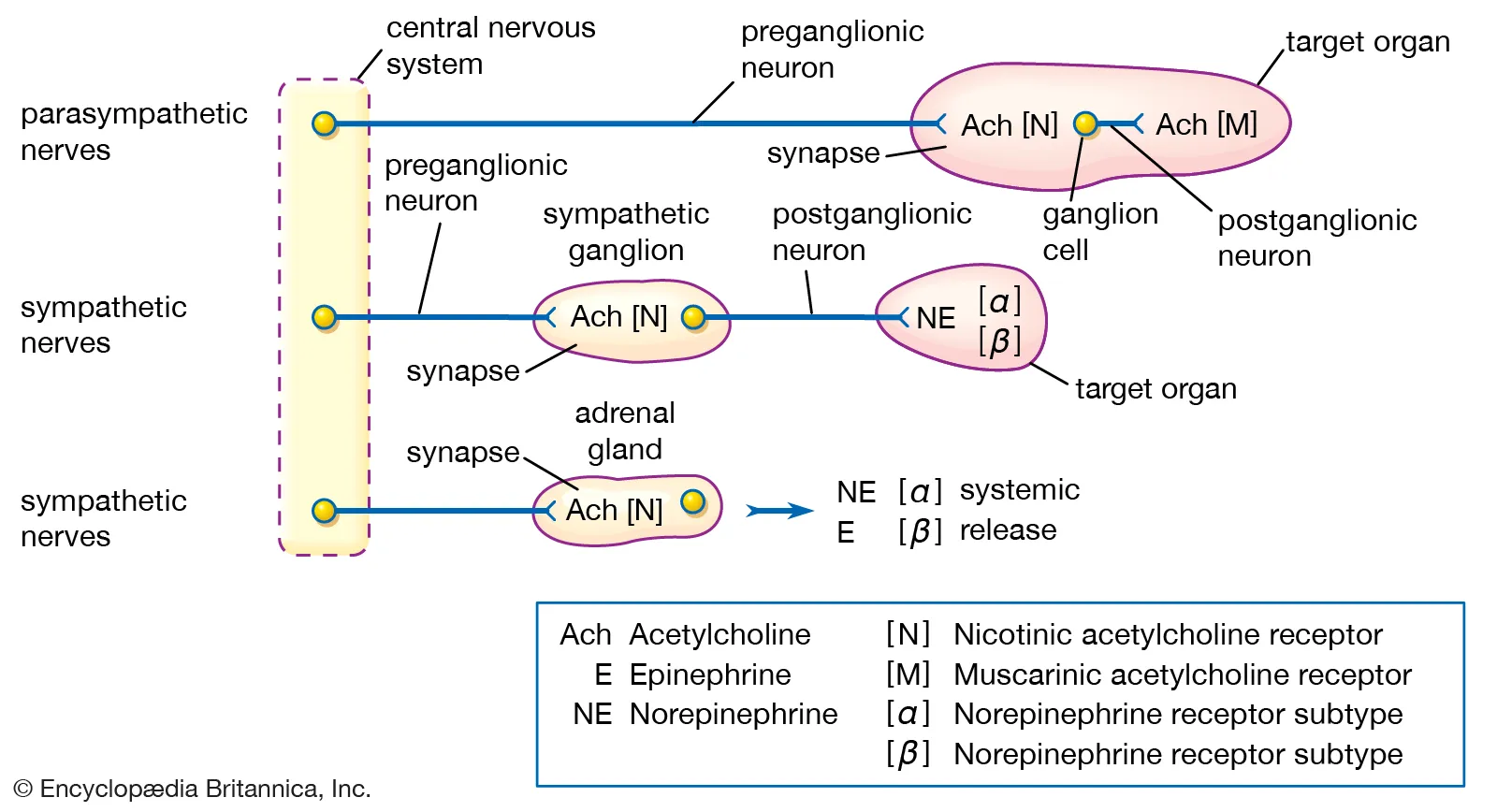
anatomy of the ANS
GANGLION
the first point of contact between the CNS and target tissue
a group of nerve cell bodies
outside the CNS
the preganglionic neurons is in the CNS, the postganglionic is in the target tissue
sympathetic NS
innervation from the spinal chord and the medulla
organs are innervated at different levels of the CNS
diffuse innervation —> few axons innervate an organ which is enough to maintain function but not enough for fine motor movements
EXCEPTIONS TO THE GENERAL RULES
the kidneys post ganglionic neuron to the smooth muscle of the vascular bed releases dopamine instead of Ach
for the adrenal gland: theres no synapse in the paravertebral sympathetic ganglion
the synapse for teh adrenal gland is directly on the gland which releases Ach and activates nicotinic receptors
parasympathetic NS
ganglia close to target organ
widespread distribution of post ganglionic neuron in medulla or sacral segment of spinal chord
discrete innervation of target tissues
co-ordination of the ANS
regiond of the brain co-ordinate actions of the ANS
amygdala: main limbic region for emotion
hypothalamus: main integration centre
reticular formation: most direct influence over autonomic function
general rules of the ANS
Ach regulated synapse at all ganglia in the ANS
in the sympathetic NS transmission at the postganglionic synapse usually involves noradrenaline acting on alpha/ beta adrenoreceptors
in the parasympathetic NS transmission at the postganglionic synapse usually involves Ach acting on muscarinic receptors
enteric nervous system
innervated by both parasympathetic and sympathetic NS
PS and S NS dont directly innervate the tissue —> they innervate the submucosal and myenteric plexus which innervates tissue
chemoreceptors in gut send signals through the plexus to the CNS
dysautonomia - disregulation of the ANS
damage to autonomic nerves
fainting standing up, dizziness, sweating, inability to alter HR when excersising, digestive problems, urinary problems, vision problems
post ganglionic sympathetic synapse
noradrenaline is the main transmitter at the post ganglionic sympathetic synapse
EXCEPTIONS
sweat glands —> uses Ach
resistance blood vessels in skeletal muscle which when activated drives vasodilation, done by adrenaline
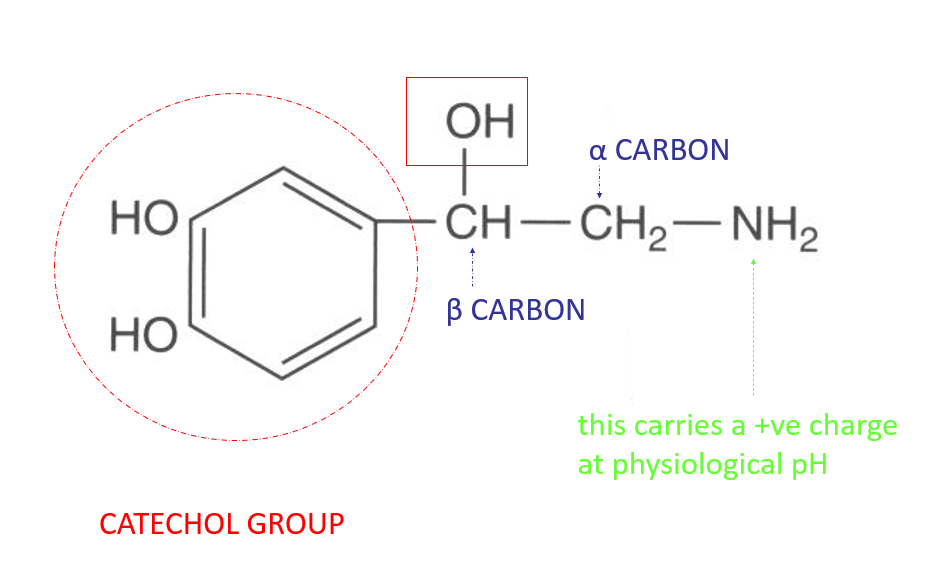
structure of noradrenaline
positive charge at physiological pH
catechol group
modification of the alpha and beta carbon will distinguish the family members from one another
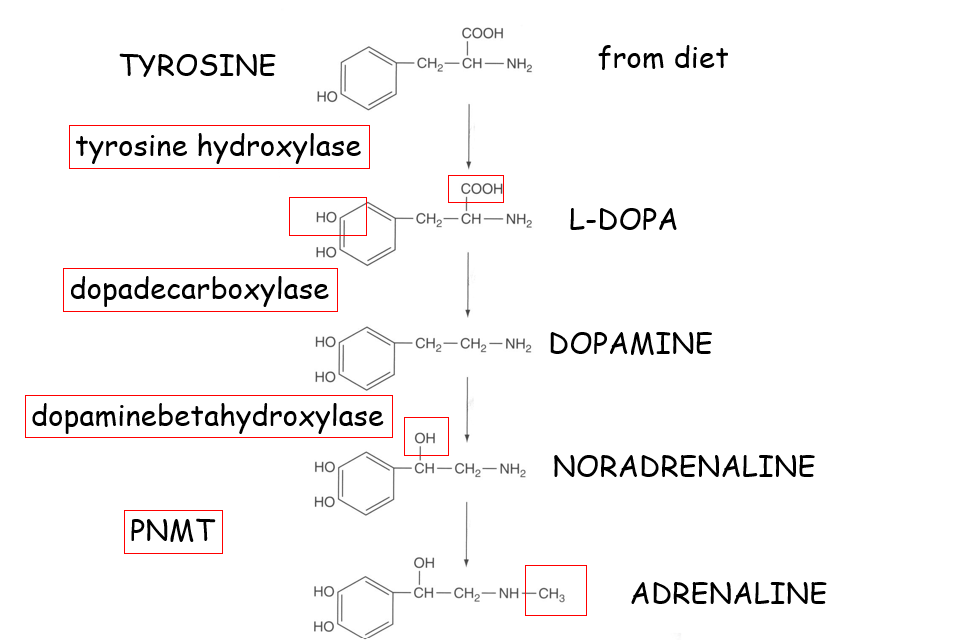
synthesis of noradrenaline
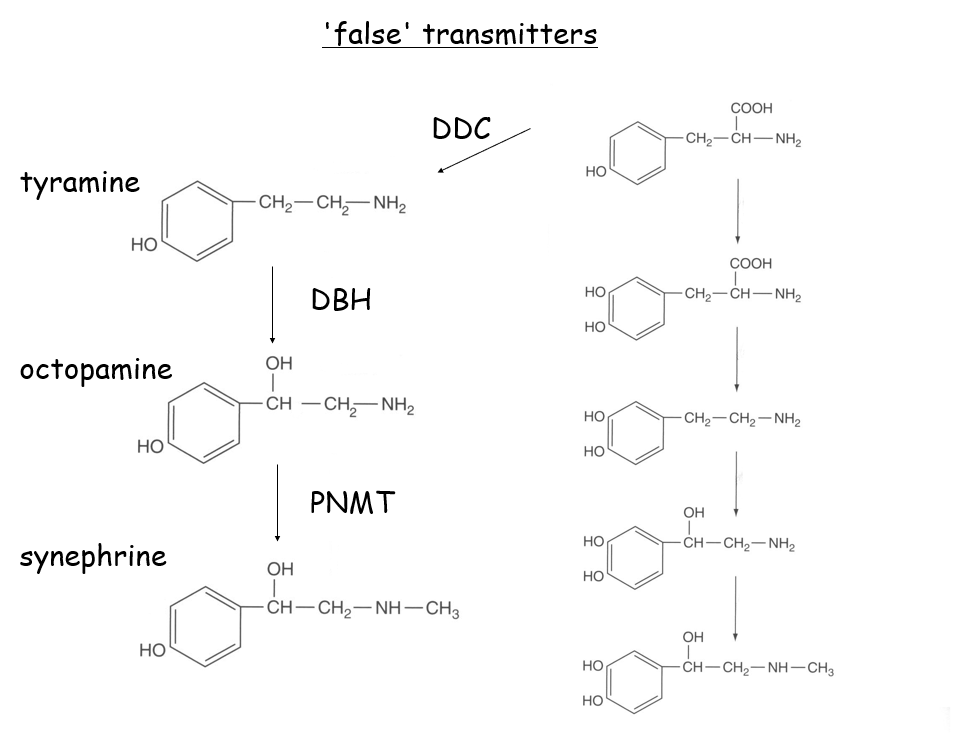
false transmitters and interfering drugs
FALSE TRANSMITTERS
enzymes must carry out reactions in the correct order otherwise false transmitters formed
tyramine, octopamine, synephrine
INTERFERING DRUGS
alpha methyl tyrosine is a competitive inhibitor for tyrosine hydroxylase —> used to treat phaeochromocytoma
alpha methyl dopa can interfere with NArd transmission
parkinsons disease
depletion of dopamine —> loss of motor function of neurons that dopamine controls
can treat by giving the substrate for dopamine - levodopa as well as carbidopa which inhibits dopa decarboxylase
carbidopa cant cross the blood brain barrier so L dopa—> dopamine only in the brain
prevents dopamine outside the brain which is toxic
release of NAdr
energy dependent
stored in vesicles w ATP and chromogranin
drugs that interfere w release of NAdr:
Reserpine: increases effect of sympathetic NS by causing vasoconstriction
antihypertensive w a side effect of depression
Guanethidine: antihypertensive w a saide effect of orthostatic hypertension
inability to control fast chages in bp
uptake mechanisms of NAdr
UPTAKE 1
via noradrenaline transporter
high affinity, low capacity
located in the nerve terminal
Na/K ATPase
requires Na gradient and ATP
drugs that block uptake 1 are antidepressants such as cocaine and impramine
UPTAKE 2
low affinity, high capacity
clears lots of NAdr but not quickly
once uptake 1 has been exhausted, uptake 2 takes over
extraneuronal
cotransport of NAdr with sodium
inhibited by cortisol
not substrate dependent - can be used for other nts
release and metabolism of NAdr
RELEASE
indirect sympathomimetics
indirect because they don’t increase the sympathetic NS on their own nut increase adrenaline which mimics the effect of the SNS
drugs that stimulate the release: tyramine from food, ephedrine in cold medicines and amphetamine in psychostimulants
METABOLISM
two enzymes: MAO, catechol O methyl transferases (COMT)
metabolites: 3 methoxy 4 hydroxymandelic acid and 3 methoxy 4 hydroxyphenylglycol —> used to measure ANS function
can interfere w this pathway w MAO inhibitors (iproniazid)
adrenoreceptors
SUBTYPES OF RECEPTORS
all GPCRs
alpha subtype has isoforms 1 and 2
beta subtype has 3 isoforms 1,2,3
ALPHA SUBTYPE
a1 subtype found on synaptic neuron and is coupled to a Gq receptor which when bound will cause contraction of smooth muscle
increases IP3 and DAG
a2 subtype found in the presynaptic neuron and controls a feedback loop —> when NAdr binds to autoreceptor it inhibits the release of NAdr
Gai decreases activity of calcium channels
BETA SUBTYPE
all stimulate cAMP formation (Gas)
all subtypes located in differnt place
b1: controls
cardiac acceleration
lipolysis
gut motility
renin release
b2 located in the bronchi and controls:
bronchodilation
vasodilation of blood vessels to skeletal muscles
glycogen breakdown
b adrenoreceptor antagonists
propranolol: non selective b blocker
antihypertensive
atenolol is a selective b1 antagonist —> cardioselective
slows down cardiac output
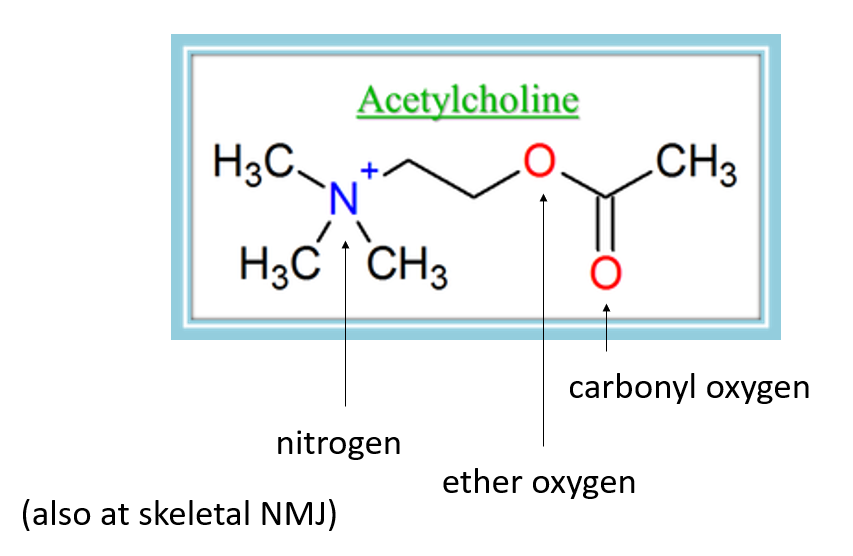
Ach synthesis and inhibition
Ach regulates the ANS function at ganglia and the parasympathetic postganglionic synapse
Substrates are acetyl CoA and choline
rate limiting step is the uptake of choline by a choline transporter at teh presynaptic terminal
choline acteyltransferase combines acetyl coa and choline and choline produced as a subproduct
vesamicol can inhibit the choline transporter
Inactivation of Ach
Ach degraded in the synaptic cleft by acetylcholinesterase —> choline and acetic acid
Achesterase has an anionic site which attracts a +ve charge from N and estertic site which binds the carboxyl oxygen
receptors for Ach
Dales experiment proved that there was more than one type of receptor for Ach
nicotinic recptors at ganglia, muscarinic receptors at post ganglionic synapse
some natural products can have a sympathomimetic or parasympathomimetic effect
muscarine, tobacco, atropine
MUSCARINIC RECEPTOR
GPCRs
specific to PSNS found in the postganglionic fibre
muscarine acts as an agonist, no effect on the nicotinic receptors
activates the PSNS
decreases HR
vasodilation
increased digestive tract
sweating and salivation
receptor subtypes
M1 in the CNS —> located in the enteric NS and so can indirectly control gut motility
M2 in the heart
M3 located in diff glands
antaginsts of the M receptors include atropine and pirenzipine
NICOTINIC RECEPTOR
ligand gated sodium ion channel
there are 5 subunits total and 2 subunits which allow 2 ach molecules to be bound (a subunits)
receptor subtypes: Nn1/Nn2 (operate at the ganglia) or Nm type (NMJ)
Ach and nicotine are agonists
antagonists: polybismethonium family, classically hexamethonium
inhibits both the SNS and PNS by blocking the nicotinic receptor
members of the family with low no of carbons are particularly selective for the Nm type receptor whilst high no of carbons select for the Nn type —> distinguishes between inhibition of whole NS or just the NMJ