6. Pulmonary Anatomy + Lung Volumes
0.0(0)
Card Sorting
1/150
Earn XP
Description and Tags
For Exam 3, focus on bicarb, bicarb + pH, lung anatomy, O2 exchange + causes, and chart with dif. inspiratory/expiratory volumes
Last updated 12:27 AM on 4/4/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
151 Terms
1
New cards
Primary components of pulmonary system
1. Lungs
2. Thoracic cavity
3. Pleural space
4. Airway system
2
New cards
Lungs (covered by, contain, purpose, apex/base, 3 surfaces)
* Covered by visceral pleura
* Contain:
* Conducting airways
* Alveoli
* Connective tissue (interstitium)
* Purpose: provide large surface area for gas exchange
* Apex: superior aspect
* Base: inferior
* 3 surfaces:
* Costal space: lateral/ribs
* Medial: mediastinum
* Diaphragmatic: inferior
* Contain:
* Conducting airways
* Alveoli
* Connective tissue (interstitium)
* Purpose: provide large surface area for gas exchange
* Apex: superior aspect
* Base: inferior
* 3 surfaces:
* Costal space: lateral/ribs
* Medial: mediastinum
* Diaphragmatic: inferior
3
New cards
Anterior, posterior, and inferior lung borders
* Anterior: thin, sharp edge between mediastinum & costal surfaces
* Posterior: rounded; lies in paravertebral gutter; extends from C7-T10 (bottom of scapula to base of neck)
* Inferior: thin, sharp; separates base of lung from costal space
* Posterior: rounded; lies in paravertebral gutter; extends from C7-T10 (bottom of scapula to base of neck)
* Inferior: thin, sharp; separates base of lung from costal space
4
New cards
Hilum
* Triangular area on medial side of lung
* Site where “root structures” enter/leave lung
* Bronchi, blood vessels, lymph nerves
* Site where “root structures” enter/leave lung
* Bronchi, blood vessels, lymph nerves
5
New cards
Location of lungs in thorax (superior/inferior limits)
Superior limit:
* Apex rises 2-4 cm above medial 1/3 of clavicle
Inferior limits:
* Anterior: approximately 6th rib at mid-clavical line
* Lateral: 8th rib mid-axillary line
* Apex rises 2-4 cm above medial 1/3 of clavicle
Inferior limits:
* Anterior: approximately 6th rib at mid-clavical line
* Lateral: 8th rib mid-axillary line
6
New cards
How are lungs divided?
Segments according to bronchi
7
New cards
Right lung segments
* 10 segments
* RUL (right upper lobe): apical, posterior, anterior
* RML: lateral, medial
* RLL: superior, medial basal, anterior basal, lateral basal, posterior basal
* RUL (right upper lobe): apical, posterior, anterior
* RML: lateral, medial
* RLL: superior, medial basal, anterior basal, lateral basal, posterior basal
8
New cards
Left lung segments
* 8 segments
* LUL: apico-posterior, anterior, superior lingular, inferior lingular
* LLL: superior, anteriomedial basal, lateral basal, posterior basal
* LUL: apico-posterior, anterior, superior lingular, inferior lingular
* LLL: superior, anteriomedial basal, lateral basal, posterior basal
9
New cards
Describe the left medial lobe of the left lung
NONEXISTENT!
The left lung does not have a LML because that is where there is space for the heart
The left lung does not have a LML because that is where there is space for the heart
10
New cards
Healthy lung appearance (color, texture, size)
* Brownish pink (esp. in younger person)
* Elastic, spongy
* Proper size (not inflated)
* Elastic, spongy
* Proper size (not inflated)
11
New cards
Thoracic cavity
* Enclosed “airtight” cylinder (creates suction/vacuum)
* 2 lateral (pleural) cavities
* Each contains a lung
* Central area (mediastinum) contains heart, great vessels, trachea, esophagus
* 2 lateral (pleural) cavities
* Each contains a lung
* Central area (mediastinum) contains heart, great vessels, trachea, esophagus
12
New cards
Thoracic structures
* Anterior: sternum and costal cartilages
* Lateral: ribs, intercostal muscles, vessels, nerves
* Posterior: vertebral bodies
* Inferior: diaphragm
* Lateral: ribs, intercostal muscles, vessels, nerves
* Posterior: vertebral bodies
* Inferior: diaphragm
13
New cards
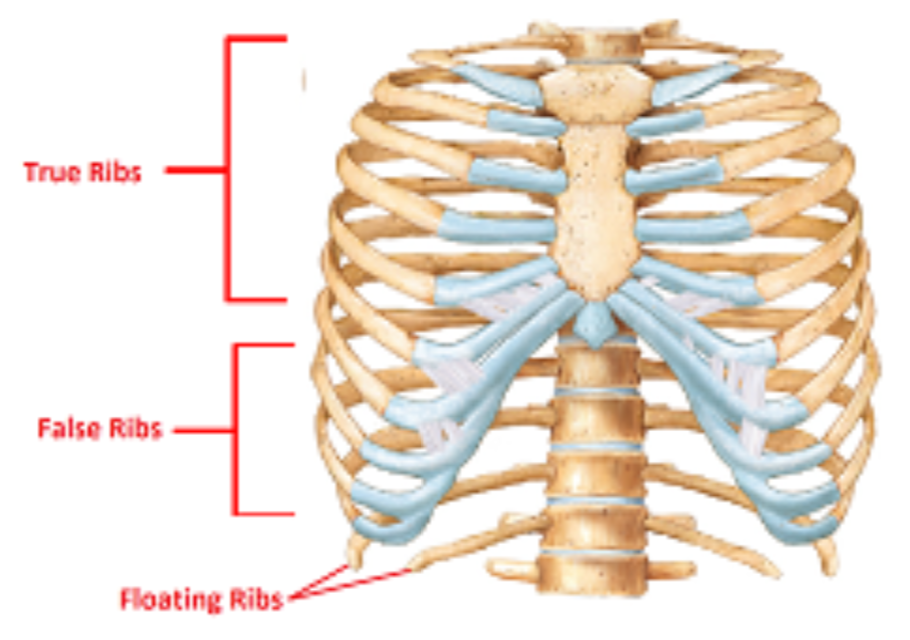
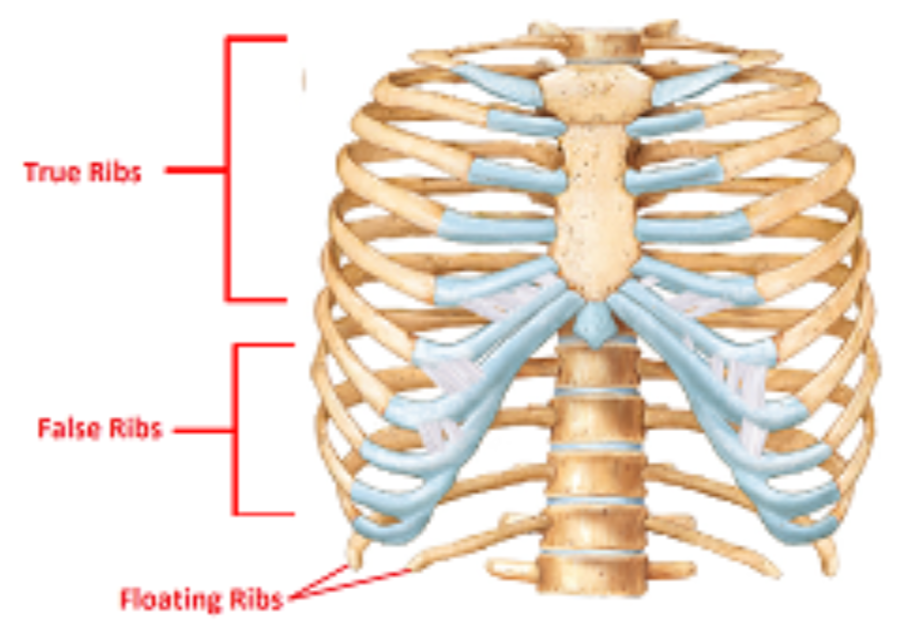
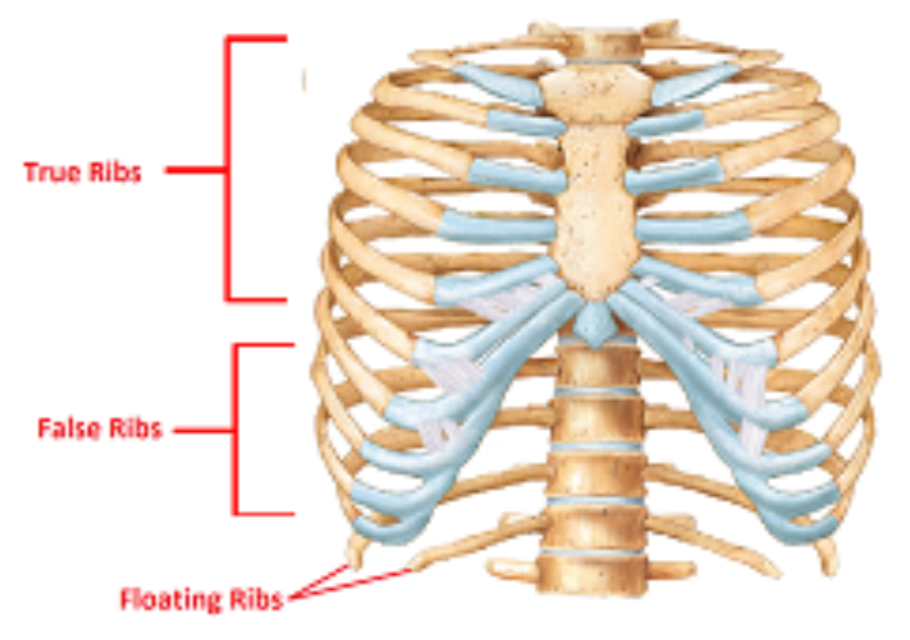
Types of ribs
1. True ribs
2. False ribs
3. Floating ribs
14
New cards
True ribs
* Ribs 1-7
* Attach to sternum via individual costal cartilages
* Attach to sternum via individual costal cartilages
15
New cards
False ribs
* Ribs 8-10
* Share attachment to sternum via common (shared) costal cartilage
* Share attachment to sternum via common (shared) costal cartilage
16
New cards
Floating ribs
* Ribs 11-12
* Cartilage attached to body wall
* Cartilage attached to body wall
17
New cards
Which type(s) of ribs are responsible for protecting the lungs?
* True ribs
* False ribs
* False ribs
18
New cards
Describe ribs’ attachment to thoracic vertebrae
* 2 facets on adjacent thoracic vertebrae
* Costovertebral joints
* Transverse process of thoracic vertebrae
* Costotranserve joints
* Synovial joints
* Costovertebral joints
* Transverse process of thoracic vertebrae
* Costotranserve joints
* Synovial joints
19
New cards
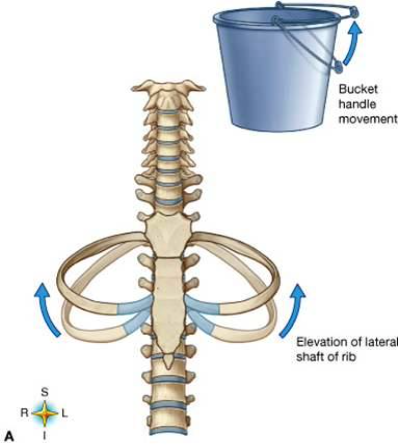
Lower rib movements
* Inspiration causes superior and lateral motion in frontal plane (bucket handle motion)
* Increases M-L dimensions of thorax
* Increases M-L dimensions of thorax
20
New cards
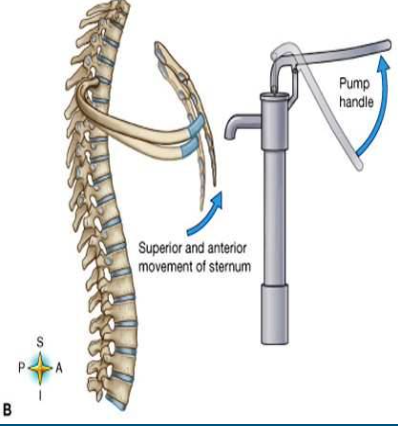
Upper rib movements
* Inspiration causes anterior and superior motion in sagittal plane (pump handle motion)
* Increases A-P dimension of upper thorax
* Increases A-P dimension of upper thorax
21
New cards
Pleura
* Membranes lining thorax
* Pariteal (outer) layer: lines thoracic cavity, diaphragm, mediastinum
* Visceral (inner) layer: covers outer surface of lungs
* Pariteal (outer) layer: lines thoracic cavity, diaphragm, mediastinum
* Visceral (inner) layer: covers outer surface of lungs
22
New cards
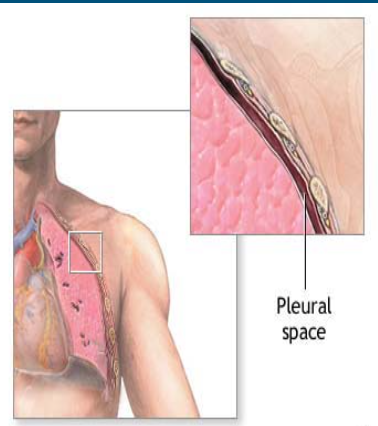
Pleural space
* Thin space between visceral and parietal pleura
* Small amount of pleural fluid to keep the layers in contact and provide lubrication
* Must have slight negative pressure (vacuum created by lymph)
* Keeps lungs inflated and able to follow thoracic wall during inspiration and expiration
* Small amount of pleural fluid to keep the layers in contact and provide lubrication
* Must have slight negative pressure (vacuum created by lymph)
* Keeps lungs inflated and able to follow thoracic wall during inspiration and expiration
23
New cards
Upper airway
1. Nose, mouth
2. Pharynx
1. Nasophyarynx
2. Orophyarynx
3. Larynx
24
New cards
Lower airway
1. Trachea
2. Bronchi
3. Bronchioles
4. Terminal bronchioles
5. Respiratory bronchioles
6. Alveolar ducts
7. Alveoli
Note: final 3 are apart of respiratory zone
25
New cards
Nose
* Two nasal passages continue posteriorly and inferiorly to nasopharynx
* Walls contain numerous folds of mucous membrane
* Warms/moistens (humidifies) air
* Traps foreign particles
* Mucous membranes can swell due to inflammation, infection (blocked airflow)
* Walls contain numerous folds of mucous membrane
* Warms/moistens (humidifies) air
* Traps foreign particles
* Mucous membranes can swell due to inflammation, infection (blocked airflow)
26
New cards
Pharynx
* Divided by soft palate into:
* Nasopharynx (from nasal passages)
* Oropharynx (from mouth)
* Laryngopharynx: lower end of pharynx, from tip of epiglottis to larynx (in airway) and esophagus
* Nasopharynx (from nasal passages)
* Oropharynx (from mouth)
* Laryngopharynx: lower end of pharynx, from tip of epiglottis to larynx (in airway) and esophagus
27
New cards
Larynx
“Voice box” at top of trachea
28
New cards
Lower airway: conducting zone (gas exchange, smooth muscle)
* Air in conducted between trachea and terminal bronchioles, but no gases are exchanged with blood
* Smooth muscle in bronchioles: site of bronchoconstriction in asthma and other inflammatory conditions
* Smooth muscle in bronchioles: site of bronchoconstriction in asthma and other inflammatory conditions
29
New cards
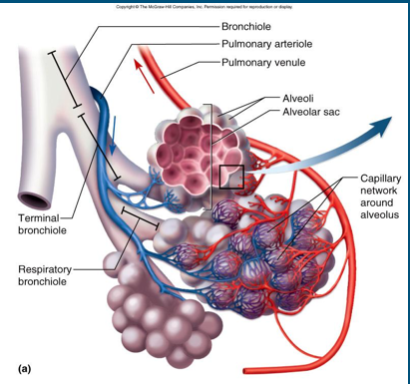
Lower airway: respiratory zone/unit (pulmonary acinus)
* Part of airway where gases are exchanged between alveoli and bloodstream
* Consists of:
* Respiratory bronchiole
* Alveolar duct
* Alveoli
* Consists of:
* Respiratory bronchiole
* Alveolar duct
* Alveoli
30
New cards
Alveolar wall
* Alveolar wall: thin layer of epithelial cells
* Squamous pneumocytes: flat, thin
* 95% of gas exchange area
* Granular pneumocytes: thick cells
* Makes surfactant (keeps lungs from sticking to each other)
* Squamous pneumocytes: flat, thin
* 95% of gas exchange area
* Granular pneumocytes: thick cells
* Makes surfactant (keeps lungs from sticking to each other)
31
New cards
Alveolar macrophages
* Free floating
* Ingest foreign debris
* Ingest foreign debris
32
New cards
Capillaries
* Form web around alveolar sacs
* Very close proximity to alveolus promotes easy gas exchange
* Very close proximity to alveolus promotes easy gas exchange
33
New cards
Alveolar-capillary (respiratory) membrane
* Single layer of alveolar cells
* Single layer of capillary cells
* Fused to a common basement membrane
* Very thin
* Single layer of capillary cells
* Fused to a common basement membrane
* Very thin
34
New cards
Ventilation
Process of moving air in and out of lungs
35
New cards
Mechanics of breathing
* Thorax must be able to change shape to change pressure gradients between atmosphere and alveoli
* Gradients must be able to overcome resistance in airways
* Gradients must be able to overcome resistance in airways
36
New cards
Muscles of inspiration
1. Diaphragm
2. Intercostals
3. Accessory muscles of inspiration
37
New cards
Muscles of expiration
1. Abdominals
2. Intercostals
38
New cards
Goal of inspiratory muscles
* Increase dimensions of thoracic cavity, which will
* Decrease intrathoracic pressure (create vacuum), causing
* Air to flow into lungs
* Decrease intrathoracic pressure (create vacuum), causing
* Air to flow into lungs
39
New cards
Diaphragm (importance, innervation, originates from, shape, contraction, primary effect)
* Primary inspiratory muscle (75% inspiratory work)
* Phrenic nerve (C3-C5)
* Originates from:
* Xiphoid, lower 6 ribs, and costal cartilage, arches, and crura from lumbar vertebrae
* Muscle fibers arch up and in to form central tendon
* Parachute shaped
* Contraction pulls central tendon downward, diaphragm flattens
* Primary effect: inc. vertical (S-I) dimension of thoracic cavity
* Phrenic nerve (C3-C5)
* Originates from:
* Xiphoid, lower 6 ribs, and costal cartilage, arches, and crura from lumbar vertebrae
* Muscle fibers arch up and in to form central tendon
* Parachute shaped
* Contraction pulls central tendon downward, diaphragm flattens
* Primary effect: inc. vertical (S-I) dimension of thoracic cavity
40
New cards
Respiratory effect of spinal injury above C3
Patient will likely be on vent because phrenic nerve (which innervates the diaphragm) runs from C3-C5
41
New cards
Diaphragmatic contractions affect on lower ribs
* Contraction moves lower ribs outward (bucket handle motion)
* How: fibers oriented so when they pull down, ribs rotate medially; lifted up and out to increase M-L dimension of lower thorax (secondary effect)
* How: fibers oriented so when they pull down, ribs rotate medially; lifted up and out to increase M-L dimension of lower thorax (secondary effect)
42
New cards
Effect of ribs being fixed in expansion (emphysema, SCI) on diaphragm
* Diaphragm is already in lower resting position
* Cannot descend much more to increase either S-I or M-L dimensions
* Cannot descend much more to increase either S-I or M-L dimensions
43
New cards
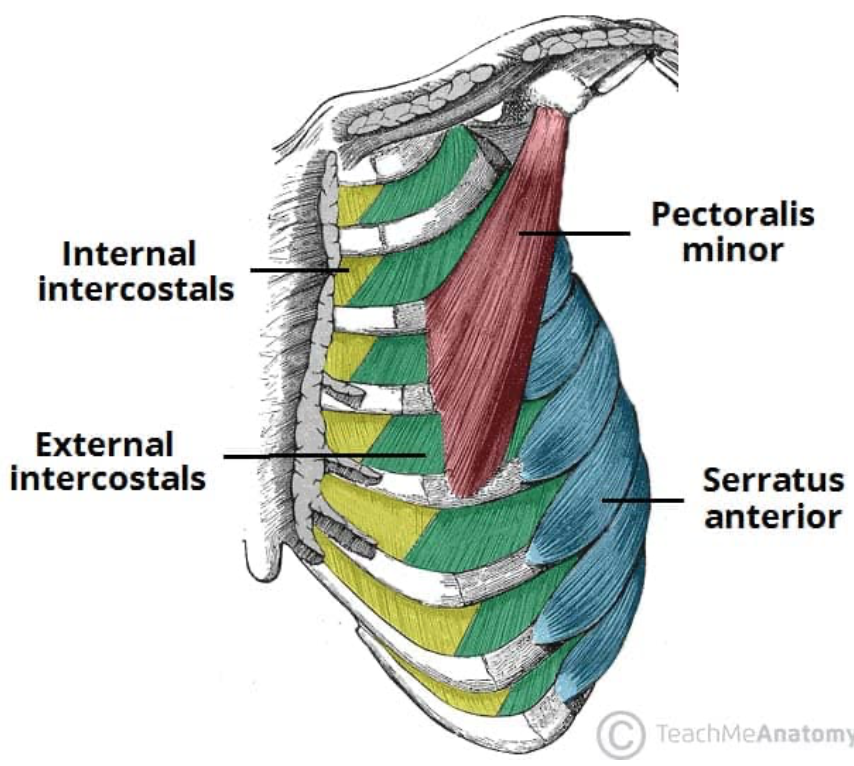
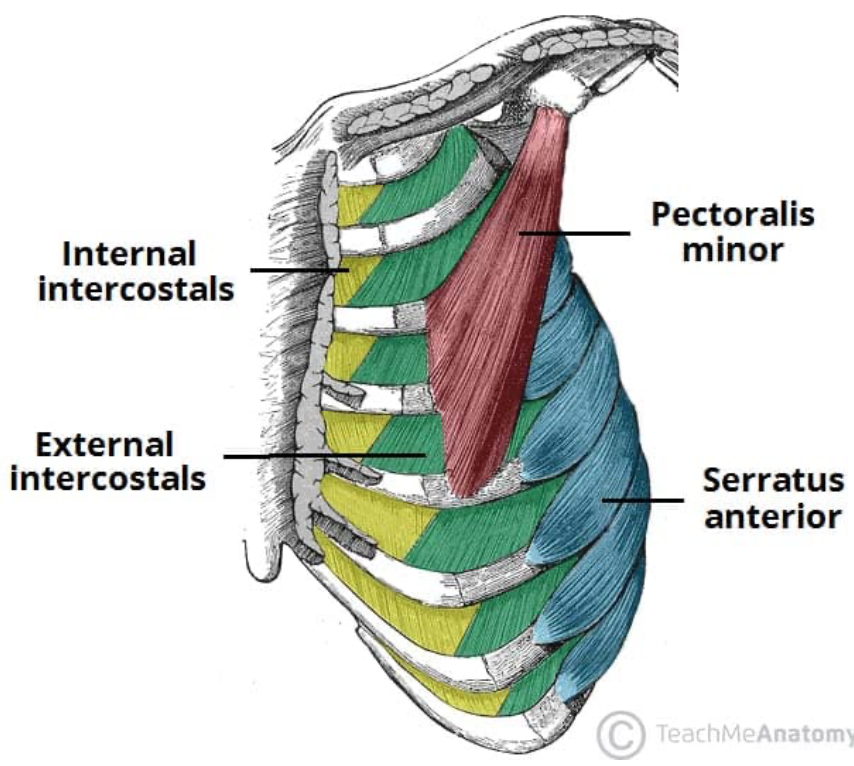
External intercostals
* Fibers run inferomedially (front of thorax) to upper border of next (inferior) rib
* Hands in front pockets direction
* Intercostal nerves (wrap around each rib)
* Hands in front pockets direction
* Intercostal nerves (wrap around each rib)
44
New cards
External intercostals: inspiration
* External intercostals generally active during inspiration
* Lift ribs up and out
* Increased M-L diameter (bucket handle)
* Possible active in some types of forced expiration
* Lift ribs up and out
* Increased M-L diameter (bucket handle)
* Possible active in some types of forced expiration
45
New cards
Accessory muscles of inspiration
1. Sternocleidomastoid (SCM)
2. Scalenes
3. Pectorals
4. Serratus anterior
46
New cards
Sternocleidomastoid (SCM) effect on inspiration (motion, dimensions, innervation)
* Primarily elevates sternum in sagittal plane (pump handle effect)
* Increases A-P dimension in upper thorax
* Innervated: spinal part CN 11
* Increases A-P dimension in upper thorax
* Innervated: spinal part CN 11
47
New cards
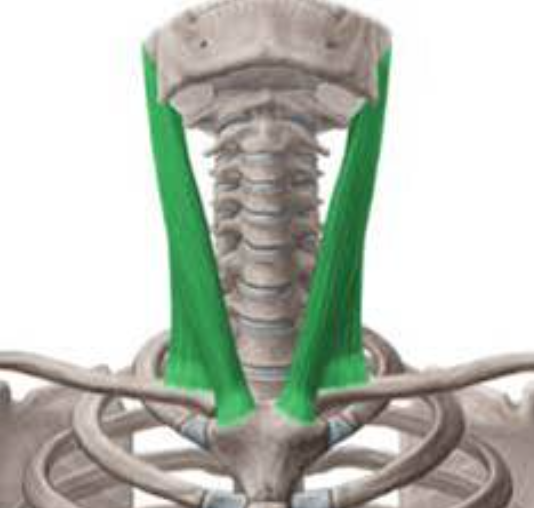
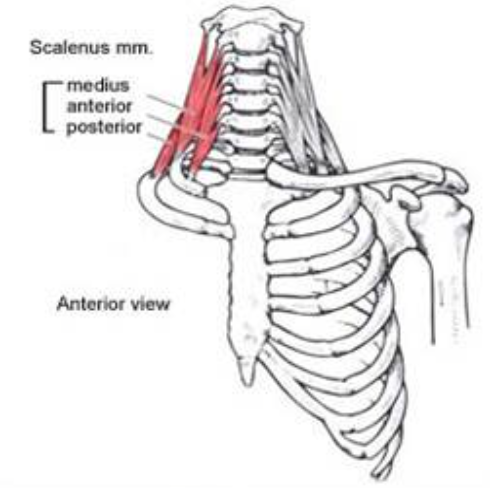
Scalenes (ant, middle, post) effect on inspiration
* Elevate upper ribs
* Work with SCM to inc. A-P dimension of thorax (pump handle)
* Innervated by ventral rami C3-C8 spinal nerve
* Work with SCM to inc. A-P dimension of thorax (pump handle)
* Innervated by ventral rami C3-C8 spinal nerve
48
New cards
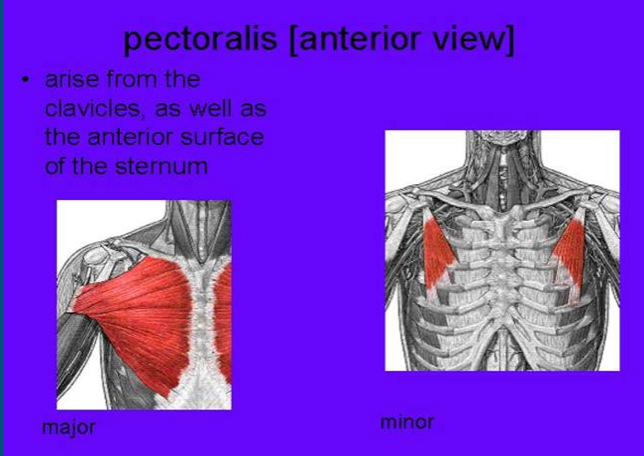
Pecs (major and minor) effect on inspiration
* Attach to sternum, costal cartilage, ribs 1-7
* If arms are fixed, pulls sternum and upper ribs forward, increasing A-P dimension of upper thorax (pump handle)
* Active in forced inspiration
* Pectoral nerve (C5-T1)
* If arms are fixed, pulls sternum and upper ribs forward, increasing A-P dimension of upper thorax (pump handle)
* Active in forced inspiration
* Pectoral nerve (C5-T1)
49
New cards
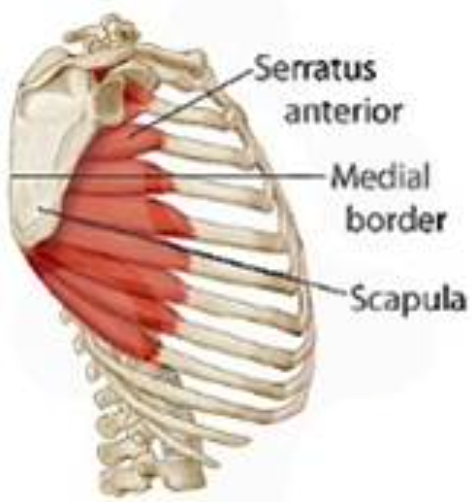
Serratus anterior effect on inspiration
* Exact role in inspiration debated
* Some evidence that if scapula is fixed, can pull ribs up and out
* If so, inc. M-L dimension of thorax
* **Long thoracic nerve (C5-C7)**
* Some evidence that if scapula is fixed, can pull ribs up and out
* If so, inc. M-L dimension of thorax
* **Long thoracic nerve (C5-C7)**
50
New cards
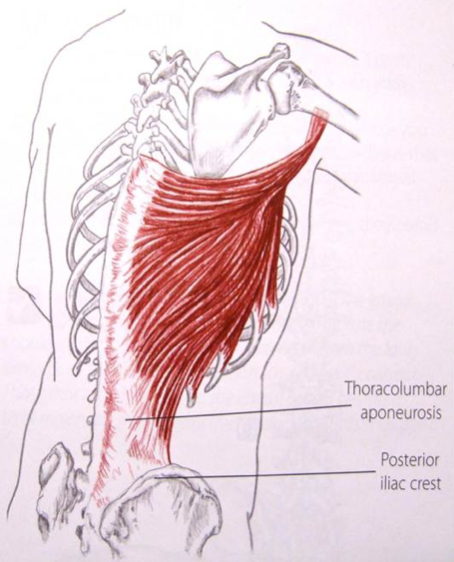
Lats as accessory to inspiration? Expiration?
* Typically active in deep inspiration
* Also helps in violent expiration (e.g. cough, sneeze)
* Only attaches to lower 3-4 ribs
* Perhaps able to stabilize thorax during deep inspiration and expiration
* Thoracodorsal nerve (C6-8)
* Also helps in violent expiration (e.g. cough, sneeze)
* Only attaches to lower 3-4 ribs
* Perhaps able to stabilize thorax during deep inspiration and expiration
* Thoracodorsal nerve (C6-8)
51
New cards
Other muscles that may be active during inspiration
* Traps, erector spine (thoracic), iliocostalis lumborum, quadratus lumborum, serratus posterior superior and inferior, levatores costarum, transversus thoracis, subclavius
* These muscles may either directly help inspiration, or provide stability so that other accessory muscles can work
* These muscles may either directly help inspiration, or provide stability so that other accessory muscles can work
52
New cards
Expiration
* Resting expiration is normally passive recoil of lungs and thorax
* No muscle activity, so no energy expending during expiration (healthy lungs)
* Elasticity of thorax and lungs must be greater than resistance in airway
* Certain diseases decrease elasticity or increase resistance in airway (increasing work of expiration)
* No muscle activity, so no energy expending during expiration (healthy lungs)
* Elasticity of thorax and lungs must be greater than resistance in airway
* Certain diseases decrease elasticity or increase resistance in airway (increasing work of expiration)
53
New cards
Accessory muscles of expiration
1. Abdominals
2. Intercostals
54
New cards
Abdominal muscles active in expiration
1. Rectus abdominis (ventral rami spinal nerve T6-12)
2. External obliques (T7-12)
3. Internal obliques (T7-12, L1)
4. Transversus abdominis (T7-12, L1)
55
New cards
How do abdominals aid expiration?
* All abdominals work to compress abdominal contents, forcing diaphragm upward to expel air more quickly (dec. S-I dimension of thorax)
* Important in rehabilitation: can be strengthened to assist expiration in various conditions
* Important in rehabilitation: can be strengthened to assist expiration in various conditions
56
New cards
Internal intercostals
* Fibers run inferolaterally to next lower rib (hands in back pockets)
* Primarily assist in expiration (some sources say parasternal portion may be active in inspiration)
* Primarily decrease M-L dimension of thorax
* Primarily assist in expiration (some sources say parasternal portion may be active in inspiration)
* Primarily decrease M-L dimension of thorax
57
New cards
Inspiration (dimensions of thoracic cavity, pressure in pleural space, movement of lungs, alveolar v. atmospheric pressure, air movement)
* Expand thoracic cavity in M-L, A-P, or both dimensions
* Negative pressure in pleural space (intrapleural pressure dec. creating vacuum)
* Lungs are drawn/sucked outward toward thoracic wall
* **Alveolar pressure < atmospheric pressure**
* Lungs expand
* Air flows into lungs
* Negative pressure in pleural space (intrapleural pressure dec. creating vacuum)
* Lungs are drawn/sucked outward toward thoracic wall
* **Alveolar pressure < atmospheric pressure**
* Lungs expand
* Air flows into lungs
58
New cards
Pressure gradients during inspiration (pleural vs. alveolar pressure for pre, during, and end of inspiration)
Pre-inspiration:
* Pleural pressure: -5 cmH2O
* Alveolar pressure: 0 (same as atmosphere)
During inspiration:
* Pleural pressure: -7 cmH2O (becomes more negative)
* Alveolar pressure: -2 (air flows in from atmosphere)
End of inspiration:
* Pleural pressure: -8 cmH2O
* Alveolar pressure: 0 cmH2O (equal to atmosphere - air stops flowing in)
* Pleural pressure: -5 cmH2O
* Alveolar pressure: 0 (same as atmosphere)
During inspiration:
* Pleural pressure: -7 cmH2O (becomes more negative)
* Alveolar pressure: -2 (air flows in from atmosphere)
End of inspiration:
* Pleural pressure: -8 cmH2O
* Alveolar pressure: 0 cmH2O (equal to atmosphere - air stops flowing in)
59
New cards
Inspiration at rest vs. increased activity
Mechanism: muscular action
* At rest: inspiration caused by diaphragm
* Increased activity: accessory muscles of inspiration become active depending on depth and frequency of inspiration
* At rest: inspiration caused by diaphragm
* Increased activity: accessory muscles of inspiration become active depending on depth and frequency of inspiration
60
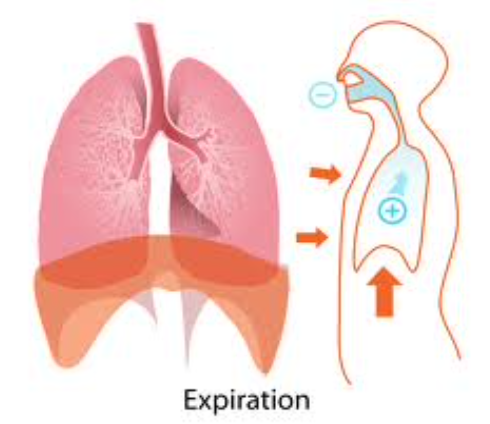
New cards
General strategy of expiration
* Decrease size of chest cavity
* Lungs recoil (squeezed slightly)
* **Alveolar pressure > atmospheric pressure**
* Air forced out of lungs
* Lungs recoil (squeezed slightly)
* **Alveolar pressure > atmospheric pressure**
* Air forced out of lungs
61
New cards
Gradients during normal expiration (how does intrapleural and alveolar pressure change; movement of air)
* Intrapleural pressure increases from -8 to -5 cmH2O
* Alveolar pressure increases from 0 to +1 cmH2O
* Air is pushed out of lungs
* Alveolar pressure increases from 0 to +1 cmH2O
* Air is pushed out of lungs
62
New cards
Gradients during forced expiration (how does intrapleural and alveolar pressure change; result)
* Intrapleural pressure can increase to +30 cmH2O
* Alveolar pressure can increase to + 38 cmH2O
* Air is forced out much more quickly
* Alveolar pressure can increase to + 38 cmH2O
* Air is forced out much more quickly
63
New cards
What happens if pleural pressure > pressure inside airways?
* Airways can collapse
* Decreased volume of air leaving lungs
* Decreased volume of air leaving lungs
64
New cards
Expiration at rest vs. with increased activity
Mechanism: muscular action
* Rest: no muscle activity; lung and chest cavity relax because of elastic recoil/rebound
* Increased activity: accessory muscles (abs, internal intercostals) become active as
* More force is needed
* Respiratory rate increases (must get air out more quickly)
* Rest: no muscle activity; lung and chest cavity relax because of elastic recoil/rebound
* Increased activity: accessory muscles (abs, internal intercostals) become active as
* More force is needed
* Respiratory rate increases (must get air out more quickly)
65
New cards
MIP: Maximum Inspiratory Pressure (definition, normal female, normal male)
* Highest pressure produced during forced inspiration
* Normal female: 108 - (0.61 x age)
* Normal male: 120 - (0.41 x age)
* Normal female: 108 - (0.61 x age)
* Normal male: 120 - (0.41 x age)
66
New cards
MEP: Maximum Expiratory Pressure (definition, normal female, normal male)
* Highest pressure during forced expiration
* Normal female: 131 - (0.86 x age)
* Normal male: 174 - (0.83 x age)
* Normal female: 131 - (0.86 x age)
* Normal male: 174 - (0.83 x age)
67
New cards
Significance of MIP and MEP
* Can detect respiratory muscle weakness better than other pulmonary function tests (PFTs)
* Can be used to determine if patient needs intubation/ventilator
* If MIP/MEP are too low, intubation/ventilation is indicated
* Values can be used to set resistance when training respiratory muscles
* Can be used to determine if patient needs intubation/ventilator
* If MIP/MEP are too low, intubation/ventilation is indicated
* Values can be used to set resistance when training respiratory muscles
68
New cards
Ventilation: need for lung/thoracic compliance
* Thoracic cavity, lungs, airway should be flexible
* Not too much resistance to inspiration
* But also sufficiently elastic recoil to cause expiration
* Not too much resistance to inspiration
* But also sufficiently elastic recoil to cause expiration
69
New cards
Compliance (definitions, too low, too high)
* Ease at which lung can be inflated
* Change in lung volume for a given change in pressure
* Too low: restricts inspiration
* Too high: not enough recoil
* Change in lung volume for a given change in pressure
* Too low: restricts inspiration
* Too high: not enough recoil
70
New cards
Primary factors affecting compliance
1. Elasticity of lung and chest wall
2. Surface tension in alveoli
71
New cards
Elasticity
* Network of elastin and collagen in alveolar walls
* Surrounds bronchi and vasculature
* Correct proportion of elastin and collagen provides balance between strength and elasticity
* Disrupted by certain diseases
* Note: ribs must also move easily at synovial joints on vertebrae, no restrictions from intercostal structures, etc.
* Surrounds bronchi and vasculature
* Correct proportion of elastin and collagen provides balance between strength and elasticity
* Disrupted by certain diseases
* Note: ribs must also move easily at synovial joints on vertebrae, no restrictions from intercostal structures, etc.
72
New cards
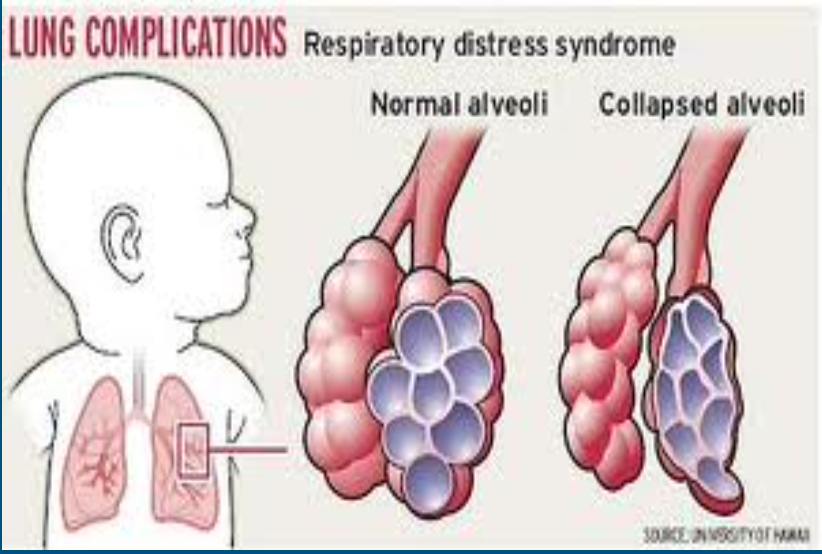
Surface tension in alveoli (effect normally, effect if too high)
* Inner walls of alveoli tend to stick together because of surface tension
* If surface tension is too high, alveoli collapse, making it impossible to inflate lungs
* If surface tension is too high, alveoli collapse, making it impossible to inflate lungs
73
New cards
Surfactant (what is it, where is it produced, what does it do, premature babies)
* Oily substance
* Produced by granular pneumocytes within alveoli
* Decreases surface tension (so lungs don’t stick together too much), allowing alveoli to be inflated
* Premature babies may lack surfactant
* Often intubated and their lungs are sprayed with surfactant
* Produced by granular pneumocytes within alveoli
* Decreases surface tension (so lungs don’t stick together too much), allowing alveoli to be inflated
* Premature babies may lack surfactant
* Often intubated and their lungs are sprayed with surfactant
74
New cards
What does resistance to airflow in lungs depend on?
1. Viscosity of gas (air)
2. Length of tube (airway)
3. Radius of tube (airway lumen)
75
New cards
Equation for airway resistance
\[ 8(viscosity)(length) \] / ∏(radius)^4
76
New cards
Describe effect of radius on resistance
* Radius indirectly effects resistance (because it is in denominator)
* Because it is raised to the 4th power, a small change in airway radius (lumen) will have a large effect on resistance
* Because it is raised to the 4th power, a small change in airway radius (lumen) will have a large effect on resistance
77
New cards
Sites of airway resistance
* 70-80% total airway resistance provided by large airways (> 2 mm diameter)
* Small airways have narrow lumens but
* Total X-sectional area of small airways is large, so total resistance is low
* Airflow in smaller airways is laminar, not turbulent
* Small airways have narrow lumens but
* Total X-sectional area of small airways is large, so total resistance is low
* Airflow in smaller airways is laminar, not turbulent
78
New cards
Physiologic control of airway lumen
* Bronchioles contain rings of smooth muscle under __autonomic control__
* Sympathetic: norepinephrine ➡️ bronchodilation
* Parasympathetic: acetylcholine ➡️ bronchoconstriction
* Also, local chemicals and inflammation (histamine) cause bronchoconstriction
* Sympathetic: norepinephrine ➡️ bronchodilation
* Parasympathetic: acetylcholine ➡️ bronchoconstriction
* Also, local chemicals and inflammation (histamine) cause bronchoconstriction
79
New cards
Additional features of ventilation
1. Minute ventilation
2. Dead space
3. Alveolar ventilation
80
New cards
Minute ventilation/minute respiratory volume (definition, equations, normal)
* Amount of air that is inspired (or expired) in one minute
* V = tidal volume x respiratory rate
* Normal = 6 liters
* V = tidal volume x respiratory rate
* Normal = 6 liters
81
New cards
Dead space (definition, included structures, normal)
* Part of airway where no gas is exchanged with blood
* Consists of all parts of airway EXCEPT respiratory zone/unit
* Normal = 150 mL
* Consists of all parts of airway EXCEPT respiratory zone/unit
* Normal = 150 mL
82
New cards
Alveolar ventilation
* Air entering respiratory zone/unit during each minute of breathing
* VA = respiratory rate x (Vt - dead space)
* Normal = 4.2
* VA = respiratory rate x (Vt - dead space)
* Normal = 4.2
83
New cards
Lung volumes and capacities (what affects lung values, how are lung values measured)
* Lungs can inspire/expire certain amounts of air during various types of breathing
* Normal values may vary according to age, gender, size of person (and thus, size of lungs)
* Values affected by pulmonary diseases, inactivity, etc.
* These volumes and capacities often measured clinically to assess lung function
* Normal values may vary according to age, gender, size of person (and thus, size of lungs)
* Values affected by pulmonary diseases, inactivity, etc.
* These volumes and capacities often measured clinically to assess lung function
84
New cards
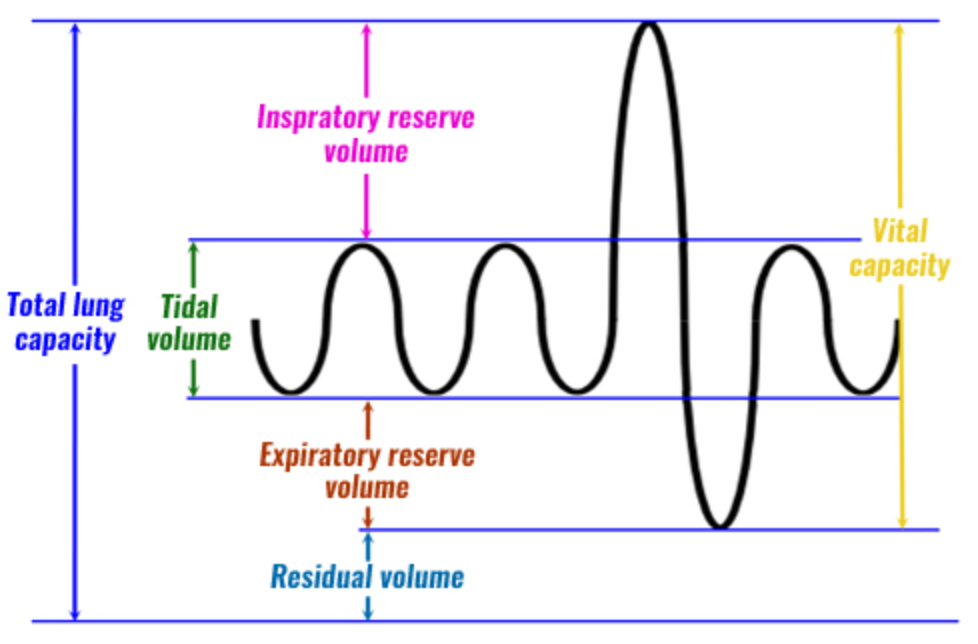
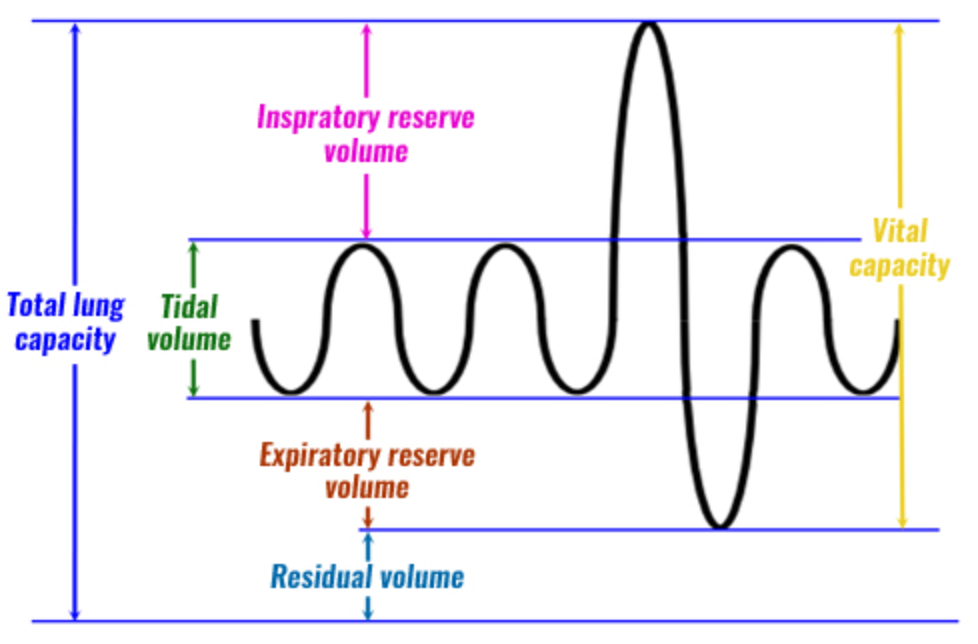
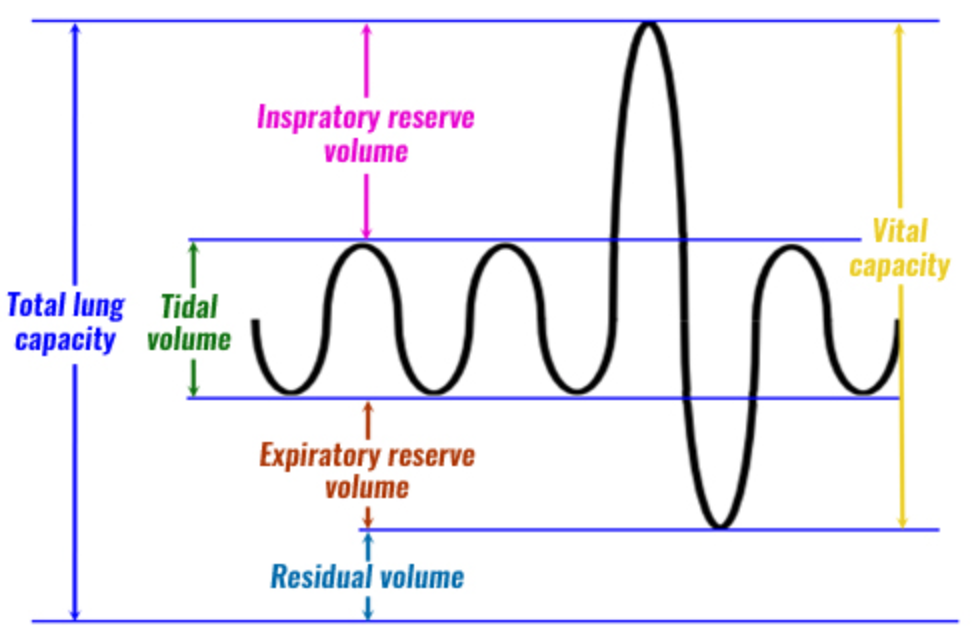
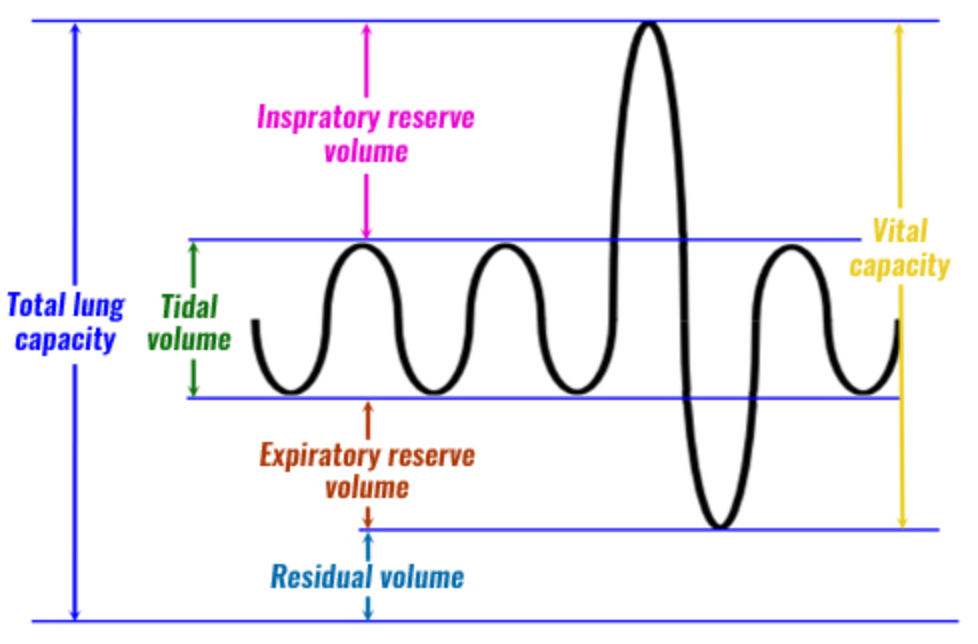
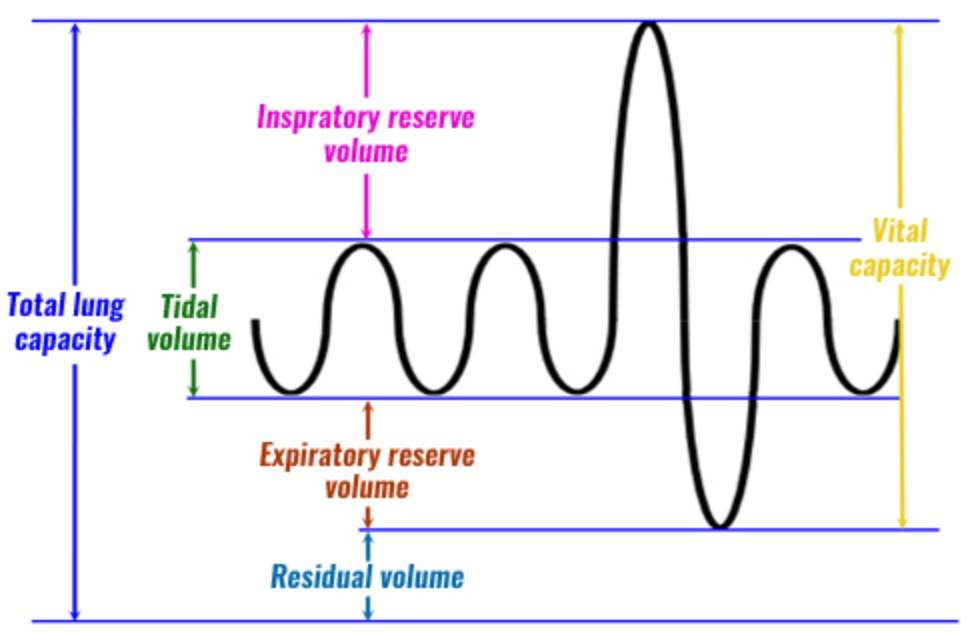
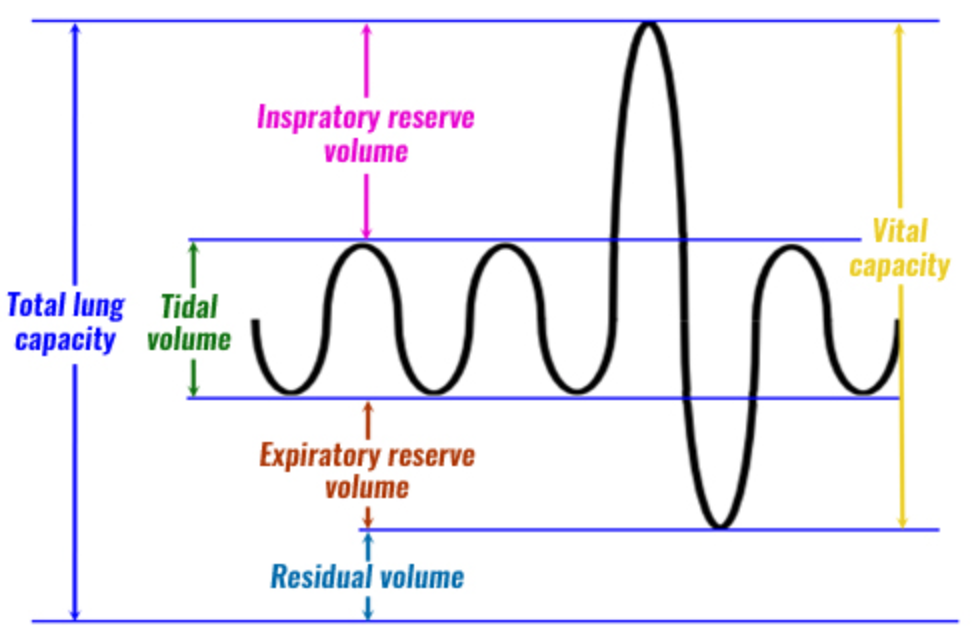
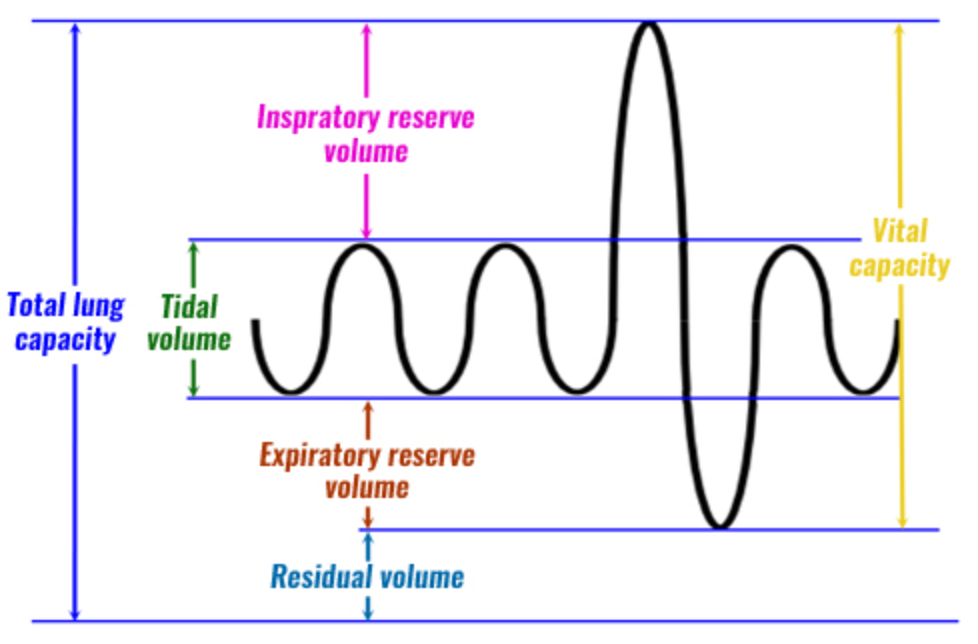
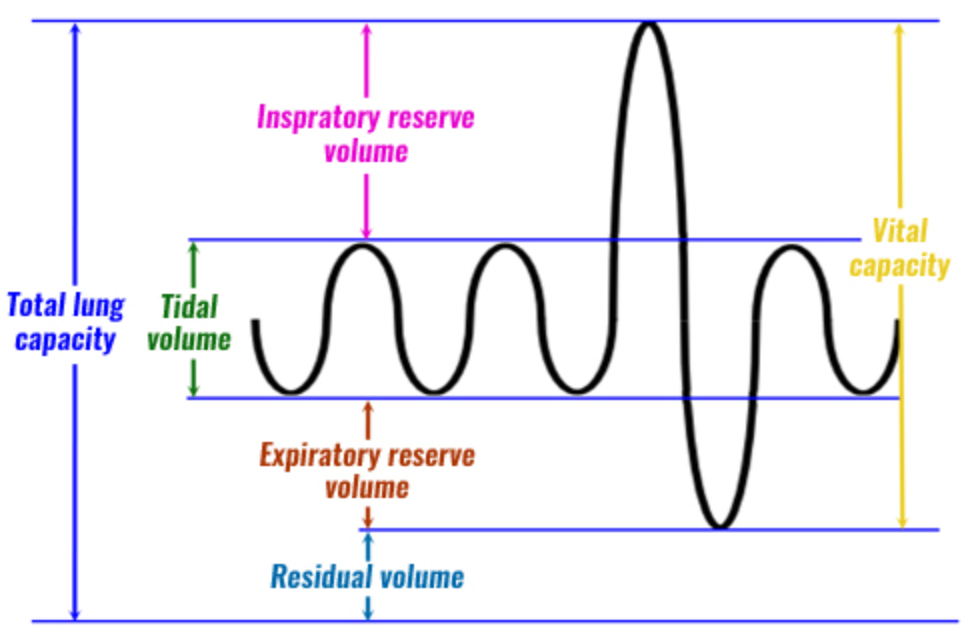
Pulmonary volumes
1. Tidal volume (Vt)
2. Inspirator reserve volume (IRV)
3. Expiratory reserve volume (ERV)
4. Residual volume (RV)
85
New cards
Tidal volume (Vt) (definition, normal value)
* Amount of air inhaled (or exhaled) with each normal breath
* Normally = 0.5 liters
* Normally = 0.5 liters
86
New cards
Inspiratory reserve volume (IRV) (definition, normal value)
* Extra air that can be inspired at the end of resting (tidal volume) inspiration
* Normally = 3 liters
* Normally = 3 liters
87
New cards
Expiratory reserve volume (ERV) (definition, normal value)
* Extra air that can be expired at the end of resting (tidal volume) expiration
* Normally = 1.1 liters
* Normally = 1.1 liters
88
New cards
Residual volume (RV) (definition, normal value, measured)
* Air remaining in lungs after maximal (forced) expiration
* Normally = 1.2 liters
* Requires sophisticated lab equipment to measure (not easily determined)
* Normally = 1.2 liters
* Requires sophisticated lab equipment to measure (not easily determined)
89
New cards
Pulmonary capacities
1. Inspiratory capacity
2. Functional residual capacity
3. Vital capacity
4. Total lung capacity
90
New cards
Inspiratory capacity (definition, equation, normal)
* Amount of air that can be inspired after normal expiration
* Inspiratory capacity = Vt + IRV
* Normal = 3.5 liters
* Inspiratory capacity = Vt + IRV
* Normal = 3.5 liters
91
New cards
Functional residual capacity (definition, equation, normal)
* Amount of air that is left in lungs after normal expiration
* = ERV + RV
* Normal = 2.3 liters
* = ERV + RV
* Normal = 2.3 liters
92
New cards
Forced vital capacity (FVC) (definition, importance, equation, normal)
* Maximal amount of air that can be expired after max inspiration
* Best overall indication of ventilation capacity
* FVC = Vt + IRV + ERV
* Normal = 4.6 liters
* Best overall indication of ventilation capacity
* FVC = Vt + IRV + ERV
* Normal = 4.6 liters
93
New cards
Total lung capacity (definition, equation, normal)
* Maximal amount of air lungs can hold
* = Vt + RV
* Normal = 5.8 liters
* = Vt + RV
* Normal = 5.8 liters
94
New cards
Physiological functions of lungs
1. Provide O2 to body, remove CO2 from body
2. Help maintain acid-base balance
3. Help maintain body temperature (evaporative heat loss)
4. Delivers certain meds into bloodstream
5. Helps filter, metabolize toxins in blood
95
New cards
What do ABGs (arterial blood gases) measure?
1. Arterial O2
2. Arterial CO2
96
New cards
Key issues in O2/CO2 metabolism
1. Partial pressures of O2/CO2
2. Pulmonary circulation
3. Ventilation-perfusion relationships
4. Gas exchange
5. Transport of gases in blood
6. Control of respiration
97
New cards
Partial pressures of O2/CO2
* Each gas exerts pressure proportional to:
* Percent/fraction of the gas in the mixture
* Barometric pressure
* Fraction inspired O2 (FiO2)
* Dry atmospheric air: 0.21
* Percent/fraction of the gas in the mixture
* Barometric pressure
* Fraction inspired O2 (FiO2)
* Dry atmospheric air: 0.21
98
New cards
PO2
* PO2 inspired air = FiO2 x barometric pressure
* Inspired air is humidified and saturated with water vapor before it reaches lungs
* Thus, pressure of water vapor must be subtracted from atmospheric pressure
* Normal PO2 = 150 mmHg
* Inspired air is humidified and saturated with water vapor before it reaches lungs
* Thus, pressure of water vapor must be subtracted from atmospheric pressure
* Normal PO2 = 150 mmHg
99
New cards
PO2 reaching alveoli
* PO2 of inspired air continues to dec. as it travels down airway and mixes with CO2 until it reaches alveoli
* Normal alveolar PO2 = 104 mmHg (slightly lower than PO2 inspired)
* Normal alveolar PO2 = 104 mmHg (slightly lower than PO2 inspired)
100
New cards
Factors effecting PAO2 (partial pressure of O2)
* Ventilatory (breathing rate)
* Direct relationship (inc. rate = inc. PAO2)
* Diseases that affect airway or gas exchange
* Direct relationship (inc. rate = inc. PAO2)
* Diseases that affect airway or gas exchange