Macroscopic Skin Lesions
1/21
Earn XP
Description and Tags
LOs -- (1) Describe skin lesions, explaining and illustrating each of the following: size, type (eg, vesicle, bulla), color, configuration (eg, annular, targetoid, discoid), arrangement (eg, solitary, grouped, linear, reticular), and distribution and location. (2) Explain the importance of physical examination of the skin.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
22 Terms
Why to examine skin
Thorough skin exam is done to assess for new or changing skin lesions
have to know what abnormal skin looks like because a change of skin lesions can cause skin cancer, like melanoma
Skin lesion description
Area of skin that has abnormal growth or appearance compared to surrounding skin
Primary and secondary lesions
Primary vs Secondary Lesions
Primary skin lesions are abnormal skin conditions present at birth or acquired over a lifetime.
Secondary skin lesions are the result of manipulated or irritated primary skin lesions. For example, if a nevus (collection of melanocytes) is scratched until it bleeds and scabs, the scab would be an example of a secondary skin lesion.
Medical language for skin lesions has been standardized to include
size, type, color, configuration, arrangement and distribution
Size for lesions - what to report
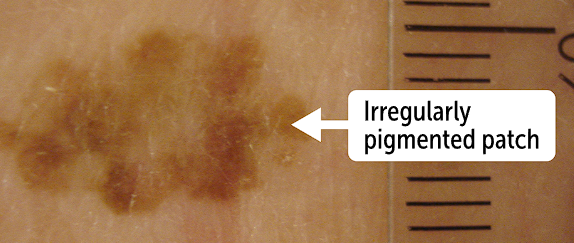
Report the width and the height of the lesion, which is measured in mm or cm
“there is a 7 mm by 14 mm patch”
Usually, a pigmented lesion larger than 6mm in size will raise suspicion for malignancy
Types of lesion - may need to palpate the lesion to see if its depressed, raised or flat
When palpating lesion, looking for swelling or consistency
Consistency will range from hard to soft depending on composition of the lesion
Bullae are elevated lesions and a fluid filled while papules are firm on palpation, but also elevated
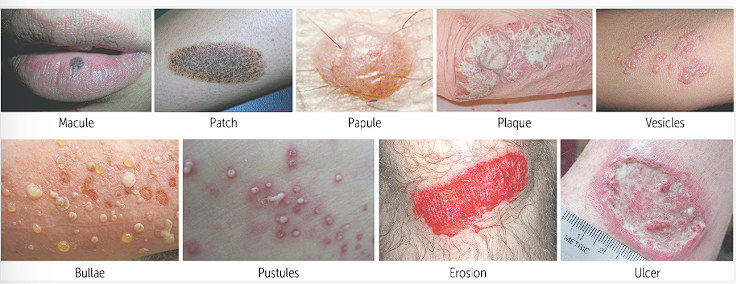
Chart of lesions
Macule | A flat lesion <1 cm in size without elevation or depression |
Patch | A flat lesion >1 cm in size without elevation or depression |
Papule | An elevated, solid lesion <1 cm in size |
Plaque | An elevated, solid lesion >1 cm in size |
Vesicles | Circumscribed elevations of the skin containing clear fluid, <1 cm in diameter |
Bullae | Circumscribed elevations of the skin containing clear fluid, >1 cm in diameter |
Pustules | Papules containing a purulent exudate that may be white, yellow, or greenish-yellow |
Erosion | Skin lesion with loss of epidermis |
Ulcer | Skin lesion with loss of epidermis and dermis (deeper than erosion) |
Macule is smaller than a patch, both raised (macule is less than 1 cm, patch is over 1 cm)
Papule is elevated and solid, but smaller than 1cm while plaque is over 1 cm
Vesicles and bullae are circumscribed elevations of skin with clear fluid, but vesicles are less than 1 cm and bullae are more than 1 cm in diameter
Erosion occurs with loss of epidermis
Ulcers are skin lesions with loss of epidermis and dermis, which is deeper than erosion
Pustules are papules that contain purulent exudate, yellow, white or greenish
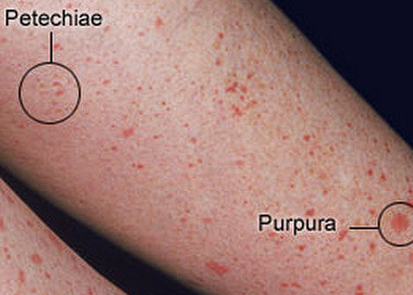
Petechiae vs Purpura
Purpura are flat <1cm spots with less than 4mm in diameter
Can be purple/red spots and patches on skin and mucous membrane, including the lining of the mouth
Petechiae are flat lesions, greater than 1 cm and have a diameter that is from 4-10 mm
Color of skin lesions can vary both lighter and darker than original skin tone
Old scars can sow white and necrotic lesions will be dark purple or black
A bruise can be yellow, green
Skin lesions are usually associated with inflammation, so they tend to be erythematous
Patients with dark skin have increased melanin, which can make dark lesions stand out less
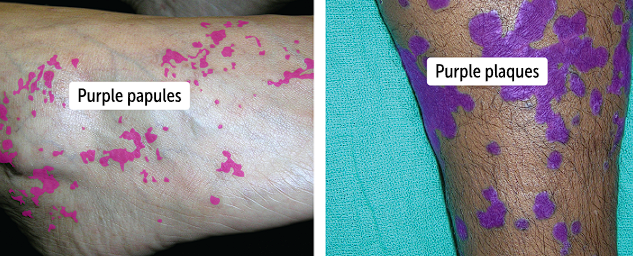
Lichen planus is a chronic inflammatory disease that can impact skin, nails or oral mucosa, and has the 6 Ps to describe it
Pruritic (itchy), purple, polygonal, planar, papules and plaques
Lichen planus papules can range from pink to violate papules that coalesce to form plaques
Configuration refers to the
shape of an individual lesion, whether is round, square or oval
is it symmetric or asymmetric?
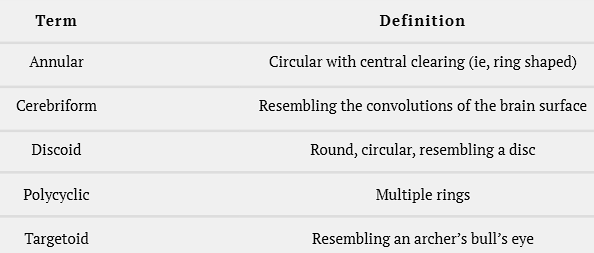
other shape descriptions are annular, cerebriform, discoid, polycyclic and targetoid
Annular is circular with central clearing, kind of ring shaped
Cerebriform resemble how the brain looks
Discoid is round and circular, like a disc
Polycyclic has multiple rings
Targetoid looks like a bull’s eye
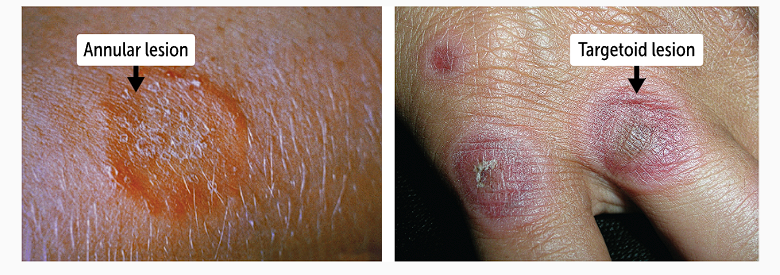
Shape of lesions do not point to a specific diagnosis, but can narrow the differential
can differential tinea corporis annular lesions from the targetoid lesions in patients with erythema multiforme
also patients with SLE tend to have discoid lesions, including at fingers
Discoid lupus erythematosus is a chronic cutaneous lupus erythematosus, where the cutaneous lesions arise as apart of full blown systemic lupus erythematosus (SLE)
Lesions have small risk of progressing to squamous cell carcinoma, due to chronic inflammation
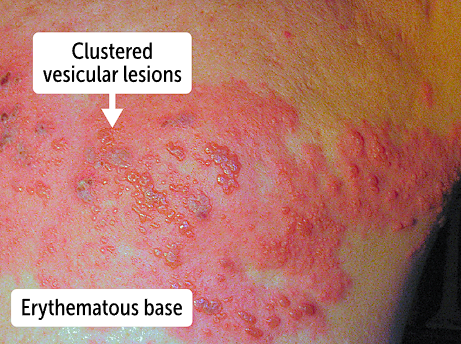
Arrangement of lesions
Some lesions are solitary, others are in specific arrangements or patterns
Arrangement of lesions are linear, grouped or reticular
groups of vesicles are in linear arrangement shown in this picture

Group arrangement is apparent on left picture — herpes labialis
Reticular (net-like) arrangement that occurs in livedo reticularis (blue molting of skin due to poor circulation)
Distribution and location of the lesion
Distribution refers to whether the lesion is singular, in a discrete location or localized to a specific body part or widespread lesion location
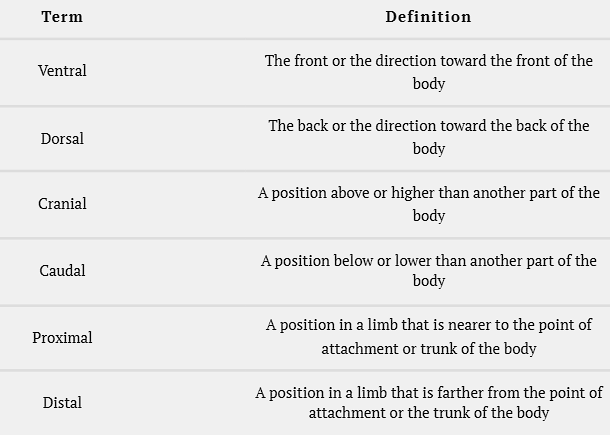
Location refers to the anatomical position of where the lesion is on patients body
Use ventral, dorsal, cranial, caudal, proximal, distal
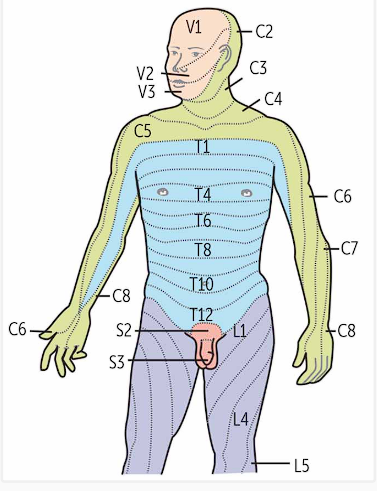
Lesions follow a dermatomal distribution which is based on a skin map that has various layers supplied by a unique spinal nerve root
Herpes zoster, known as shingles, is a painful vesicular rash in dermatomal distribution secondary to reactivation of varicella zoster virus, which is a dsDNA virus
Will cause pain, medicate for pain control
Borders
Esp important for lesions that are pigmented
Lesions with regular borders are most likely benign (mole) while the irregular borders are more likely malignant, as in melanoma
Skin lesion for melanoma, use ABCDE guide
Asymmetry
Border
Color
Diameter
Evolution
A 3-year-old boy is brought to the pediatrician by his mother who reports that he has a mark on his forearm that she first observed shortly after birth. On examination, you note a flat lesion that is 3.0 cm in diameter. Which of the following is the best term to describe this lesion?
Macule
Papule
Patch
Plaque
Vesicle
Patch because its a flat lesion over 1cm in size, unlike the macule that is less than 1 cm
Melanoma has the worst prognosis of all skin cancers, and sun exposure is one of the major risk factors. One way to recognize concerning lesions is by noting the ABCDE of melanoma. What does the B stand for?
Basaloid
Big
Border
Brown
Bumpy
Border
A 47-year-old woman presents to the dermatologist with a lesion of the left nasal ala that has been present for 3 months. On palpation, the lesion feels raised. You measure the diameter to be 0.5 cm. Which of the following is the best term to describe this lesion?
Erosion
Macule
Papule
Patch
Bulla
Papule, because that’s an elevated solid lesion less than 1 cm in size