Medium Confidence Level NAVLE Questions
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
Dog with major bleeding needing a blood transfusion. You have several units of blood available from different donors. Which of these are used in the major crossmatch for blood products to be transfused to a dog?
A. Donor red blood cells, recipient plasma
B. Donor red blood cells, donor plasma
C. Recipient red blood cells, donor plasma
D. Recipient red blood cells, recipient plasma
A. Donor red blood cells, recipient plasma
In a major crossmatch, you are looking to see if the factors in the plasma of the recipient are going to react to the donated red blood cells.
A minor crossmatch involves recipient red blood cells and donor plasma
A 10 year old female spayed German shepherd dog presents for collapse and difficulty breathing. Your physical exam shows pale mucous membranes, a fluid wave in the abdomen, and a splenic mass. Aspiration of the abdominal fluid shows hemorrhagic effusion that does not clot. Which of the following is commonly found with your presumed diagnosis?
A. Factor VIII deficiency
B. Hypercalcemia
C. Von Willebrand's disease
D. Tumor lysis syndrome
E. Disseminated intravascular coagulation
E. Disseminated intravascular coagulation
The presumed diagnosis based on the given signalment, physical findings, and diagnostics is splenic hemangiosarcoma, which is often associated with DIC.
Which of these are used in the minor cross match for blood products when looking for a compatible blood donor for a dog?
A. Recipient red blood cells, recipient plasma
B. Recipient red blood cells, donor plasma
C. Donor red blood cells, donor plasma
D. Donor red blood cells, recipient plasma
B. Recipient red blood cells, donor plasma
In a minor crossmatch, you are looking to see if the factors in the plasma of the donor are going to react to the recipient's red blood cells.
A 10-year old mixed breed dog presents for a 1-month history of anorexia, lethargy, and inappetance. Physical exam reveals pale mucous membranes and a mild tachycardia. The
CBC shows:
MCV 50 fl (66-77 fl)
MCH 12 pg (21-26 pg)
MCHC 25 %g/dl (32-36.3 %g/dl)
HCT 22% (35-57%)
reticulocyte 40,000/ul (<80,000/ul)
What is the most likely diagnosis for this dog?
A. Babesiosis
B. Congenital portosystemic shunt
C. Iron deficiency
D. Anemia of chronic disease
E. Mycoplasma felis infection
C. Iron deficiency
CBC shows a microcytic, hypochromic, non-regenerative anemia.
Reticulocyte counts under 60,000/ul are typically considered non-regenerative in most labs. This is consistent with chronic iron deficiency. This most common reason for chronic blood loss is gastrointestinal tract disease such as an ulcer or cancerous lesion.
An adult intact male mixed breed stray dog presents for lethargy and inappetance. The physical exam reveals pale and icteric mucous membranes, and a fever of 103.5F (39.7 C). The dog has a PCV of 22% (35-57%), total protein of 4.9 (5.4-7.5 g/dl). The urinalysis shows hemoglobinuria. A blood smear shows pyriform-shaped structures inside the red blood cells. What is the most likely diagnosis?
A. Babesia infection
B. Acetaminophen toxicity
C. A primary immune-mediated hemolytic anemia
D. A Leukocytozoon infection
E. Ingestion of large amounts of onions
A. Babesia infection
The pyriform structures in the RBCs reveal the diagnosis. Leukocytozoon only occurs in birds.
A 5-year-old medium sized, spayed female mixed breed dog presents for lethargy, decreased appetite, and shifting leg lameness. On physical exam, you note a mild generalized lymphadenopathy and 103.7°F temperature. On orthopedic exam, no overt lameness is noted when trotted out. However, you detect pain on palpation and manipulation of the right carpus and left hock. Upon questioning the owner further, the dog accompanied the owner on a camping trip a few weeks ago. The owner removed six ticks from the dog. He has also seen tapeworm segments in her bedding since returning. You submit blood and urine for a minimum database as well as additional testing to confirm your suspicions. While you await your results, which antibiotic would be the most appropriate to prescribe?
A. Cefpodoxime
B. Clindamycin
C. Doxycycline
D. Amoxicillin
E. Trimethoprim/sulfamethoxazole
F. Cephalexin
C. Doxycycline
Dog is most likely suffering from a tick-borne disease. Doxycycline is the treatment of choice for most tick-borne diseases, therefore it would be the most appropriate choice. Since confirmatory titer testing can take up to a few weeks for results, it is appropriate to start empirical therapy while awaiting results.
Von Willebrand's Disease (vWD) is a bleeding disorder in which von Willebrand factor is affected. It may be present in decreased amounts, function abnormally, or not be present at all. A certain breed of dog is highly predisposed to having this disease. It is important to be aware of this condition as surgery in such a patient can result in non-stop bleeding. Which breed is most commonly affected by this condition?
A. Standard Poodle
B. Doberman Pinscher
C. Saint Bernard
D. German Shepherd
E. Flat Coated Retriever
F. Dalmatian
B. Doberman Pinscher
Dobermans are predisposed to having Type I vWD. In this situation there are decreased amounts of von Willebrand factor present in the blood. This is an autosomal dominant disease. None of the other breeds listed are predisposed to vWD.
A 6-year old male neutered Springer Spaniel presents for lethargy and difficulty walking. The owner reports that over the past week, the dog has become increasingly listless with decreased appetite and seems stiff as though he is "walking on eggs". You examine the dog and find joint pain and effusion bilaterally affecting the carpi, tarsi, stifle, and elbow. The dog also appears uncomfortable on firm spinal palpation. T-103.1 F (39.5 C), HR-118 bpm, RR-30 bpm with intermittent panting. The remainder of your physical exam is within normal limits. You perform a complete blood count and chemistry panel revealing the following:
Hematocrit - 32% (Normal 36%-50%)
White Blood Cell Count - 14,500/ul (Normal 7,000-17,000/ul)
Thrombocytes - 195,000/ul (Normal 200,000-900,000/ul)
Calcium - 10.8 mg/dl (Normal 8-11 mg/dl)
Phosphorus - 2.9 mg/dl (Normal 2.4-4.9 mg/dl)
Total Protein - 6.9 g/dl (Normal 5.5-7.3 g/dl)
Alkaline Phosphatase - 78 IU/l (Normal 10-80 IU/l)
Alanine Aminotransferase - 18 IU/l (Normal 3-33 IU/l)
Blood Urea Nitrogen - 17 mg/dl (Normal 10-22 mg/dl)
Creatinine - 1.1 mg/dl (Normal 0.5-2.2 mg/dl)
Glucose - 91 mg/dl (Normal 60-125 mg/dl)
Urinalysis was within normal limits and urine culture was negative. Radiographs of the affected joints show joint effusion and no bony abnormalities. You perform arthrocentesis of each carpus, the left elbow and right tarsus. You are able to aspirate up to about 0.3ml from each joint; the fluid is thin and turbid; you submit the fluid for analysis. The protein level in the joint fluid ranges from 3.2-3.5 g/dl and the nucleated cell counts are 12,000-18,000 cells/ul consisting primarily of neutrophils, approximately 90% of which are nondegenerate. Smaller numbers of mononuclear cells are present. Culture of the synovial fluid is negative and a panel for tick titers is all negative.
Which of the following treatments is most appropriate based on the presumptive diagnosis?
A. Arthroscopy and amoxicillin
B. Enalapril and furosemide
C. Prednisone and azathioprine
D. Plasma transfusion and intravenous fluids
E. Doxycycline and enrofloxacin
C. Prednisone and azathioprine
IMPA is often classified as being erosive or nonerosive. This case is an example of the nonerosive form based on the lack of radiographic evidence of cartilage or subchondral bone destruction. The erosive form is rare and is thought to account for <1% of the cases of IMPA.
Nonerosive IMPA can be associated w/ systemic infectious, inflammatory, or neoplastic dz or rxns to drugs or vax but it is most commonly idiopathic with no association to another disease process. In the described case, no risk factors or signs of concurrent disease were mentioned. Tick-borne arthropathy is less likely with the negative tick titers obtained, but since not every type of tick can be tested for, some clinicians may opt to treat with an antibiotic like doxycycline concurrently with the immunosuppressive drugs.
IMPA CS: anorexia, weight loss, fever, lethargy, and lymphadenopathy. Up to 25% of dogs present with only nonspecific signs of systemic illness and without apparent gait abnormality or joint effusion. It is an important consideration for dogs with fever of unknown origin and may be the cause up to 20% of the time. IMPA is diagnosed by synovial fluid analysis although additional baseline diagnostics are indicated to screen for potential systemic or infectious causes. Normal synovial fluid is clear and viscous with <2.5 g/dl protein and <3,000 cells/ul with predominantly mononuclear cells. Joint fluid in IMPA may be thin, turbid, and increased in volume with higher amounts of protein and cells, often primarily nondegenerate neutrophils.
Tx of idiopathic IMPA centers on immunosuppressive therapy, often starting with prednisone and sometimes including an additional immunosuppressive drug such as azathioprine or cyclophosphamide. About 80% of dogs will respond to immunosuppressive doses of prednisone; however, about one half of dogs require long-term or additional drug therapy to maintain remission.
Which of the following is a common finding on a complete blood count in a dog with a ruptured splenic hemangiosarcoma?
A. Schistocytes
B. Thrombocytosis
C. Neutropenia
D. Eosinophilia
E. Heinz body anemia
A. Schistocytes
Schistocytes are fragmented red blood cells that are mechanically broken up due to the irregular vessels and fibrin strands they pass through in hemangiosarcoma patients. Other typical findings on a CBC in a patient with hemangiosarcoma are thrombocytopenia, anemia (although not with Heinz bodies), and leukocytosis.
What stimulates antidiuretic hormone (ADH) secretion in the horse?
A. Hyperosmolality and decreased circulating blood volume
B. Hypoosmolality and decreased circulating volume
C. Hyperosmolality and increased circulating blood volume
D. Hypoosmolality and increased circulating volume
A. Hyperosmolality and decreased circulating blood volume
In the horse, as in other species, ADH increases renal water reabsorption and urine osmolality by increasing permeability of the collecting tubules. Osmoreceptors in the hypothalamus detect subtle changes in plasma osmolality. If osmolality rises, you will hope to see ADH secretion so that the urine excreted would be more concentrated. The same is true if circulating volume decreases; thus, a lesser volume of water would be lost. When ADH secretion does not occur or if the kidneys are unable to respond to ADH, this is likely diabetes insipidus, and animals will be very polyuric, polydipsic and have extremely dilute urine.
In June, you are asked to examine an 8 year old horse which has been out in a California pasture for over a month. The horse is thin and mildly depressed. There is a tremor of the lips and tongue, and when feed is offered, the lips are pulled back indicating marked dystonia of the facial muscles. The horse is unable to prehend the feed. Which of the following causes should you look for to match these clinical signs?
A. Sarcocystis
B. Lead
C. Yellow star thistle
D. Aberrant strongyle migration
E. Ethylene glycol
C. Yellow star thistle
Yellow star thistle is Centaurea solstitialis. In some horses which ingest large quantities, it can cause nigropallidal encephalomalacia, which is loss of the globus pallidus and substantia nigra, and extrapyramidal nuclei, which control muscles of prehension. Loss of these nuclei causes tremors and dystonia of the lip muscles and tongue. Centaurea repens (Russian knapweed) can also cause similar lesions.
Which of these recommendations is appropriate for a horse that has chronic obstructive pulmonary disease?
A. Feed a pelleted ration rather than hay
B. Treat with broad spectrum antibiotics
C. Maintain the horse in a stable whenever possible
D. Treat daily with atropine
A. Feed a pelleted ration rather than hay
Environmental factors and dust are thought to play a major role in the pathogenesis of COPD. An alternative to feeding pellets is to soak hay prior to feeding to reduce the dust taken in when eating. Stabled horses are much more likely to develop signs. Atropine can be given to bronchodilate in emergencies for acute attacks but should not be given routinely, as it can predispose to development of colic. Antibiotics would not be an effective recommendation because the disease is not infectious (there is no bacterial component to treat in most cases).
A 7 year old male Clydesdale horse presents for exercise intolerance and noisy breathing. On your exam, you note mild inspiratory dyspnea with an audible whistling sound on inspiration. What is the most likely diagnosis?
A. Sinusitis
B. Asthma
C. Intrathoracic large airway obstruction
D. Laryngeal hemiplegia
D. Laryngeal hemiplegia
In this condition, the recurrent laryngeal nerve is damaged. Interestingly, the left side is almost always the side that is affected. An actual cause is usually not found, although direct trauma and certain toxins can cause laryngeal hemiplegia. It is thought to be a hereditary disorder. An intrathoracic large airway obstruction and asthma would both cause more expiratory dyspnea. Sinusitis may cause nasal discharge but is not likely to cause the signs this horse is showing.
You are evaluating a 4-year-old Thoroughbred for intermittent epistaxis. Upon examination of skull radiographs (see image), what is the most likely diagnosis for the epistaxis?
A. Ethmoid hematoma
B. Exercise-induced pulmonary hemorrhage
C. Guttural pouch mycosis
D. Nasal adenocarcinoma
A. Ethmoid hematoma
These lesions are angiomatous masses that originate from the mucosal lining of the ethmoid conchae or walls of the maxillary or frontal sinus. Guttural pouch mycosis also can result in epistaxis but typically has no radiographic changes. Although horses can get tumors in the nasal passages, this is relatively rare. Exercise-induced pulmonary hemorrhage also can result in epistaxis, but the blood originates from the lungs. In the radiograph provided, notice the smooth, well-defined soft tissue mass in the sinus region of this horse. No osseous changes or fluid lines are apparent in this radiograph. In this particular case (ethmoid hematoma), the soft tissue mass is actually dorsal to the ethmoid turbinates (ethmoids are normal appearance in this case). Upon surgical removal, a definitive diagnosis of ethmoid hematoma was confirmed.
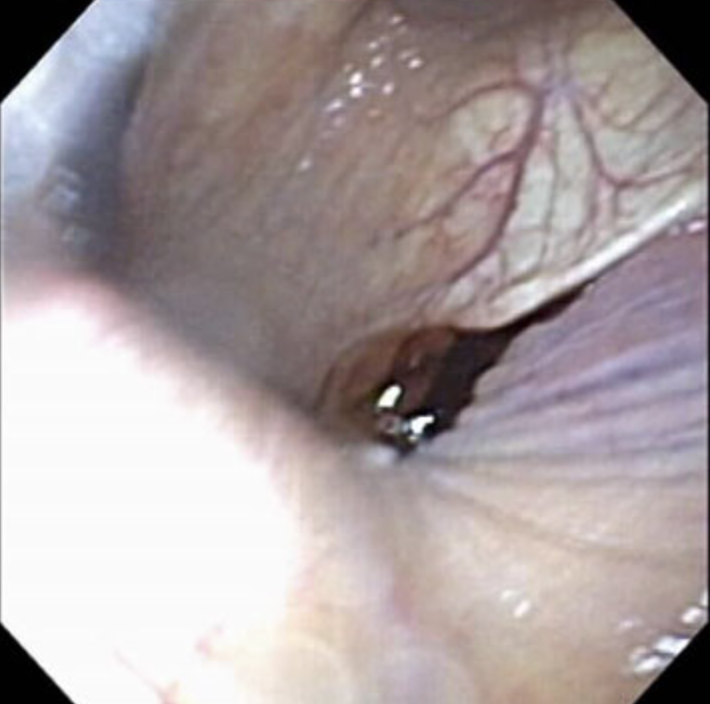
You are examining a 7 year old Thoroughbred gelding for severe bilateral epistaxis. After the epistaxis has decreased, endoscopy of the pharynx reveals blood from the left guttural pouch opening (see image). What is the most appropriate treatment for hemorrhage from guttural pouch mycosis?
A. Pass endoscope into affected guttural pouch and cauterize involved vasculature
B. Surgical occlusion of involved arteries (i.e. internal or external carotid artery) under general anesthesia
C. Lavage guttural pouch with antifungals
D. Tie off the left common carotid artery
B. Surgical occlusion of involved arteries (i.e. internal or external carotid artery) under general anesthesia
Guttural pouch mycosis has several different clinical presentations. In some horses, epistaxis is observed, while in others, cranial nerve deficits such as dysphagia may be observed. When hemorrhage is present, the disease is advanced and more aggressive therapy must be pursued. In this case, surgical occlusion of the involved arteries is necessary (i.e. embolization coils or balloons). If you lavaged the guttural pouch in this case, you may exacerbate the bleeding. Passage of the endoscope may also disrupt the clot and cause further hemorrhage. Furthermore, cauterization of the vessels involved using an endoscope is not possible. Tying off the left common carotid artery seems like a good idea, but because of the circular blood flow in the brain, hemorrhage will continue.
Which of these receptors plays the most important role in causing airway dilation in response to catecholamine secretion?
A. Beta-1 adrenergic receptors
B. Beta-2 adrenergic receptors
C. Alpha-2 adrenergic receptors
D. Alpha-1 adrenergic receptors
B. Beta-2 adrenergic receptors
Beta-2 adrenergic receptors are abundant through the lung, and stimulation produces smooth muscle relaxation and bronchodilation. This can be exploited pharmacologically in bronchoconstrictive diseases, where giving a beta-2 agonist such as terbutaline can cause bronchodilation and reduce clinical signs. Alpha receptors are less abundant in the lung and play no important role in regulation of airway diameter. Beta-1 receptors are more important in the heart.
You are presented with a 6-month old colt with a 5-day history of lethargy, intermittent diarrhea, weight loss, and ventral edema. A quick check of the PCV and TP reveal a PCV of 30% (28-42%) and TP of 3.2 g/dl (6.8-8.2 g/dl). Abdominal ultrasound (see image) demonstrates thickening of the small intestinal wall. What is the most likely diagnosis based on signalment, history and clinical findings?
A. Clostridioides difficile enteritis
B. Salmonella infection
C. Intermittent jejunal intussusception
D. Lawsonia intracellularis infection

D. Lawsonia intracellularis infection
Although not as commonly as in pigs, L. intracellularis can infect horses (and other species). Similar to pigs, the infection usually involves weanling-age horses and causes thickening of the small intestine and hypoproteinemia. The low protein is commonly observed as ventral edema clinically. Both Clostridioides and Salmonella can cause diarrhea at any age but are not as commonly associated with ventral edema. Intussusceptions do occur but also typically result in colic.
A 4-year old male Thoroughbred horse presents to you for colic. During your work up, you note a painful enlargement at the root of the mesentery on rectal palpation. You suspect that the cause of the horse's colic are adults from the egg shown in the picture below. Which of the following drugs effectively kills the adult organisms that can cause this condition?
A. Piperonyl butoxide
B. Praziquantel
C. Rifampin
D. Metronidazole
E. Ivermectin
E. Ivermectin
Colic with an associated painful mass at the root of the mesenery is suspicious for verminous arteritis caused by damage to the cranial mesenteric artery and its branches by Strongylus vulgaris. The strongyle egg shown in the picture confirms the cause in this question. A number of anthelmintics are effective including benzimidazoles, pyrantel and ivermectin.
Praziquantel is effective against tapeworms. Rifampin and metronidazole are antibacterial drugs. Piperonyl butoxide is a pesticide synergist used in insecticide mixtures in horses.
On a hot July day in Michigan, an adult horse develops acute depression, high fever (104.5F) and subsequently has profuse watery diarrhea. On presentation to your hospital, the horse's heart rate is 80 beats/min, respiratory rate is 36 breaths/min and temperature is 103.4F. After your physical examination, you perform some routine clinicopathologic tests with the below results:
PCV- 56%
Total Protein- 8 gm/dL
Lactate- 5.2 mmol/L
White blood cell count- 2500 cells/microliter
Neutrophil count- 625 cells/microliter with toxic changes
Band neutrophil count-300 cells/microliter
You have the horse moved to an isolation stall and also notice that it seems to be very sore in the forelimbs. Based on the clinical signs and examination, what would be a top-rule out and how would you confirm your suspicion?
A.Cantharidin toxicity (Blister beetle toxicity), Supportive test- Measure blood cantharidin concentrations
B.Clostridium chauvoei type A, Supportive test- Measure clostridial toxins via ELISA
C.Neorickettsii risticii, Supportive test- a PCR of blood or feces
D.Salmonella typhimurium, Supportive test- Culture of feces
C. Neorickettsii risticii, Supportive test- a PCR of blood or feces
The clues that best indicate PHF are the time of year (disease usually occurs in the summer in the northern states), the high fever and diarrhea, and the presence of laminitis. The horse is also dehydrated and has a profound leukopenia, both consistent with PHF. Salmonella also causes diarrhea and leukopenia, and could be a viable choice, but Salmonella can occur at any time of the year; moreover, laminitis is not as often seen with Salmonella. This question has a practical aspect to it as horses often present with the described history and physical examination findings, and the veterinarian has to decide if he or she wants to treat specifically for PHF; the drug of choice is oxytetracycline. In this clinical situation, you as a veterinarian would have to start treatment empirically as your PCR test will take several days to get results. The good news is that PHF is very susceptible to oxytetracycline.
Which of the following is false concerning abdominal paracentesis in a horse?
A. Bitch catheter is commonly used
B. Nucleated cells are usually less than 5,000/uL and total protein is less than 2.5 gm/dL if normal
C. Usually performed to the left of midline
D. Normal color is usually yellow
C. Usually performed to the left of midline
It is not recommended to perform an abdominal paracentesis to the left of midline as you are more likely to hit an organ such as the spleen. It is usually performed just to the right of midline. All other choices are true about abdominal paracentesis in a horse.