CHAPTER 7 (from summer endo-basic)
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
root canal system
follows the external contour of the tooth
the entire space in the dentin housing the pulp
root canal anatomy
essential for endodontic success
complexity is the norm, not the exception
as critical as diagnosis & treatment planning
a simple tapering canal with a single foramen is rare
all groups of teeth had at least one accessory foramen
canal morphology affects:
shaping & cleaning outcomes
more than the choice of instrumentation technique
root dimensions can be modified by:
aging
occlusion
disease (pathosis)
formation of secondary/tertiary dentin & cementum
pulp chamber
in the anatomic crown
root canal(s)
in the anatomic root
other key structures of root canal system
pulp horns
canal orifices
apical deltas & apical foramina
accessory, lateral, and furcation canals
root canal curves
faciolingually, which can be challenging to detect on standard x-rays
types of curves
gradual
sharp bends
complex shapes (double s-curves)
canal variation
the number of canals usually matches the number of roots, but some roots (like oval-shaped ones) can have multiple canals
accessory canals
form during root development
minute canals that extend in a horizontal, vertical, or lateral directions from the pulp to the periodontium
contents of accessory canals
connective tissue & vessel
pathological significance of accessory canals
allow irritants to pass from pulp to periodontium, potentially leading to periodontal disease or other issues
weine’s classification type I
(1)
single canal, single exit

weine’s classification type II
(2-1)
two separate canals, merging to one exit

weine’s classification type III
(2)
two canals throughout, two separate exits
weine’s classification type IV
(1-2)
one single canal, splitting into two exits

vertucci’s classification
an extended categorization
based on studies of cleared teeth with dye to reveal internal canal pathways
further strengthens the fact that root canal anatomy can be highly variable and complex
MX 2nd premolar
had the largest accessory foramina
only tooth that showed all eight possible configurations
most complicated apical morphologic structure — which might be a possible reason why root canal therapy may fail in premolar teeth
vertucci’s classification type I
(1-1)
a single canal extends from the pulp chamber to the apex

vertucci’s classification type II
(2-1)
two separate canals leave the pulp chamber and join short of the apex to form one canal

vertucci’s classification type III
(1-2-1)
one canal leaves the pulp chamber and divides into two in the root; the two then merge to exit as one canal

vertucci’s classification type IV
(2-2)
two separate, distinct canals extend from the pulp chamber to the apex

vertucci’s classification type V
(1-2)
one canal leaves the pulp chamber and divides short of the apex into two separate, distinct canals with separate apical foramina

vertucci’s vlassification type VI
(2-1-2)
two separate canals leave the pulp chamber, merge in the body of the root, and redivide short of the apex to exit as two distinct canals

vertucci’s classification type VII
(1-2-1-2)
one canal leaves the pulp chamber, divides and then rejoins in the body of the root, and finally redivides into two distinct canals short of the apex

vertucci’s vlassification type VIII
(3-3)
three separate, distinct canals extend from the pulp chamber to the apex

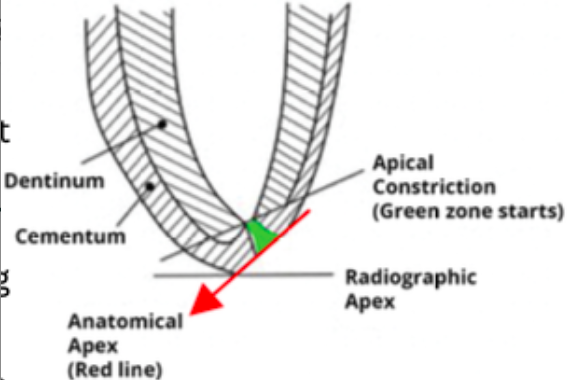
anatomy of the apical root
apical foramen
apical constriction
cementodentinal junction
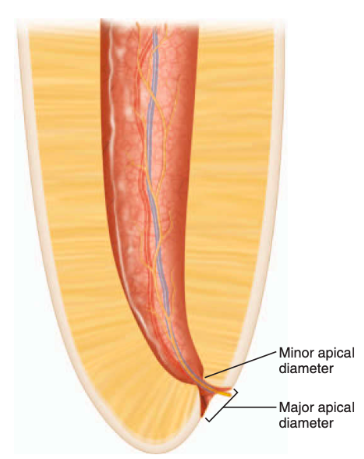
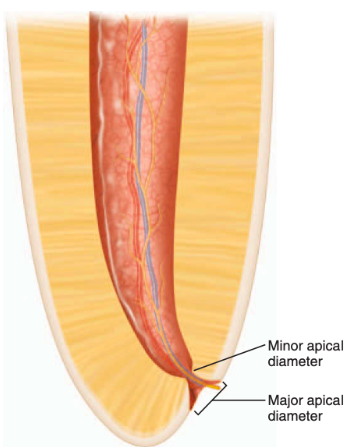
apical constriction
aka: minor foramen, minor diameter, or minor apical diameter
0.5 - 1.5 mm coronal to the apical foramen (major apical diameter)
reference point and apical termination for shaping, cleaning, and obturation of the root canal
apical foramen
aka: major foramen, major diameter, or major apical diameter
does not normally exit at the anatomic apex but rather is offset 0.5-3mm
the “circumference or rounded edge” that differentiates the termination of the cemental canal from the exterior surface of the root”
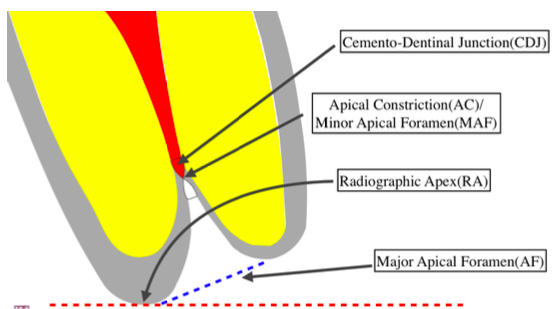
cementodentinal junction (CDJ)
1mm from the apical foramen
point in the canal where cementum meets dentin
where pulp tissue ends and periodontal tissues begin
generally not in the same area as the apical constriction
root apex
contains a variety of anatomic structures and tissue remnants, thus, has differing morphology
1mm from the apex
termination points when no bone or root resorption occurred
1.5 mm from the apex
termination points when only bone resorption occurred
2mm from the apex
termination points when both bone and root resorption occurred
radiographic apex
a more reliable reference point locating the apical constriction and apical foramen since it is difficult clinically
within 3 mm
root canal procedures are recommended to terminate at or ___ from the radiographic apex, depending on the pulpal diagnosis
apical pulp stump
prevents extrusion of irritating filling materials into the periradicular tissues
electronic apex locators
are reliable instruments that can help determine the working length of the root canal
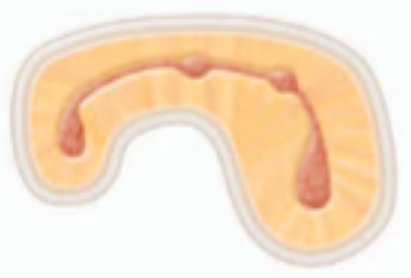
isthmus
can function as bacterial reservoirs
contains pulp or pulpally derived tissue
any root with two or more canals may have an isthmus
a narrow, ribbon-shaped communication between two root canals
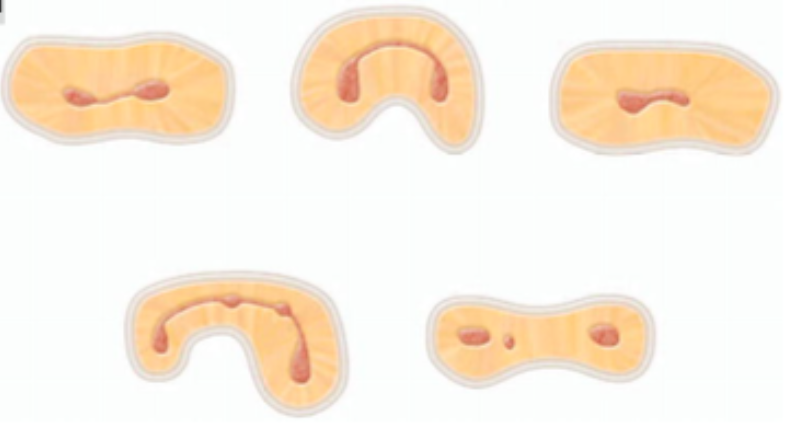
isthmus classifications type I
an incomplete isthmus
it is a faint communication between two canals

isthmus classifications type II
characterized by two canals with a definite connection between them (complete isthmus)

isthmus classifications type III
a very short, complete isthmus between two canals

isthmus classifications type IV
a complete or incomplete isthmus between three or more canals
isthmus classifications type V
marked by two or three canal openings without visible connections
