HTHSCI 2H03 - Cellular receptors and drug action
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
dissociation constant
K-1/K1 (rate of dissociation/rate of association)
T/F affinity is the inverse of the dissociation constant
True
drugs with a low Kd have a high affinity for the receptor
T/F a drugs affinity for a receptor tells us how well the drug binds to the receptor and the action of the drug at that receptor
False
A drug's affinity for a receptor tells us how well the drug binds to the receptor, but does not tell us anything about the action of the drug at that receptor
What are the two large categories that describe what a drug does at a receptor?
Agonists - mimic the effect of the endogenous ligand
Antagonists - prevent the endogenous ligand or agonists from binding, occupy the receptor site
Types of agonists
Full, partial, inverse
Full agonists
- Bind to the same receptor site as the endogenous ligand and produce the same biological effect as the endogenous ligand at that receptor site
-> ex: dexamethasone and cortisol
- If an agonist produces the full effect of the endogenous ligand, the drug is called a full agonist with high efficacy
Partial agonists
- If only a part of the endogenous effect is elicited, the drug is called a partial agonist
-> Aripiprazole produces a weaker biological effect at the dopamine receptor compared to dopamine
- Efficacy will always be lower than a full agonist
Inverse Agonists
- Bind to the same receptor site as the endogenous ligand, but induce the opposite response
- Only occurs when receptors have an intrinsic (basal) level of activity
-> Receptors exert a biological effect independent of the endogenous ligand "constitutive activity"
- has negative efficacy
- GABA-A receptor
-> agonists (ex: bezodiazepines) elicit a sedative effect
-> inverse agonists at this receptor exert anxiogenic effect
Agonism diagram
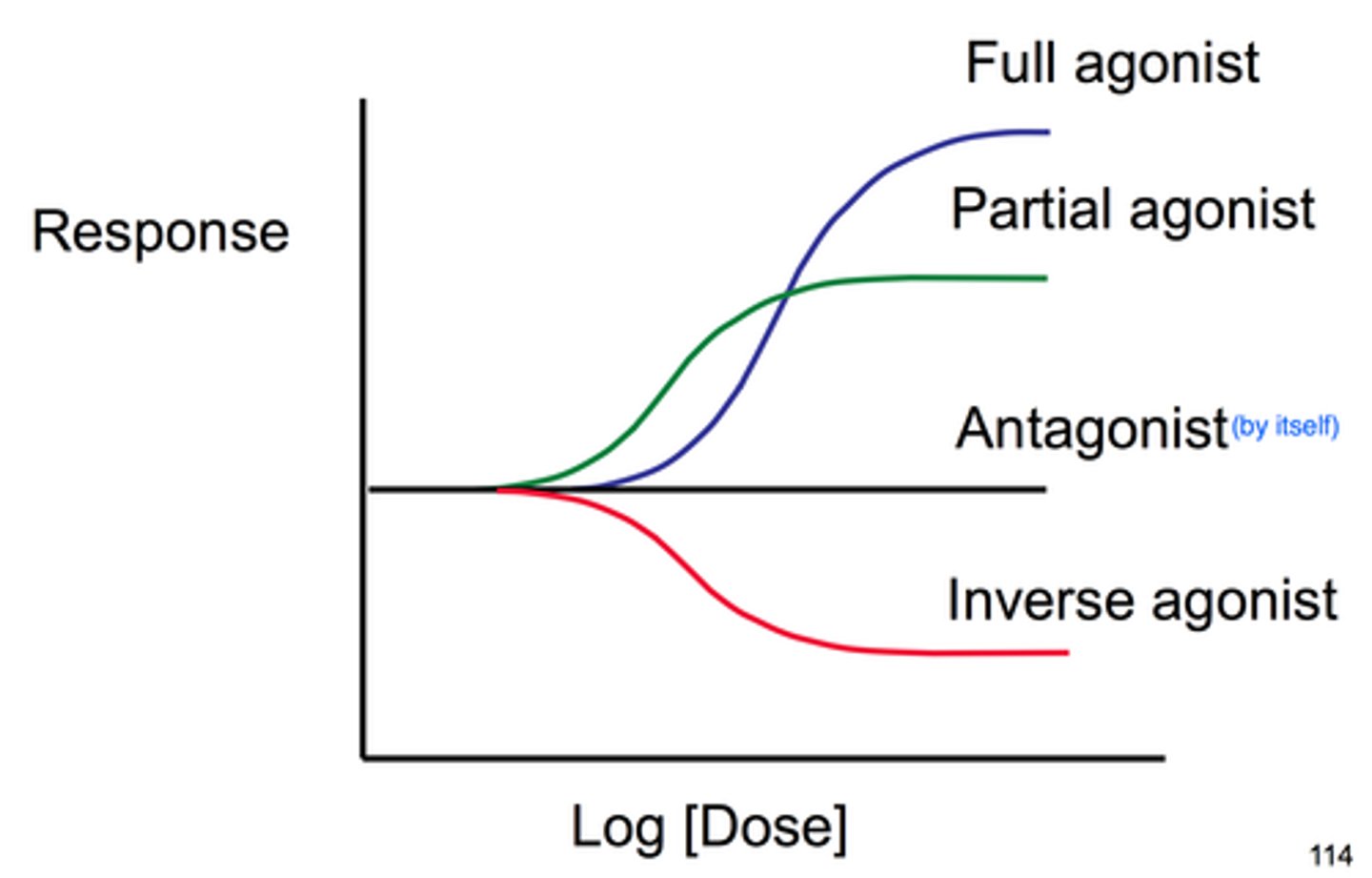
Antagonists
- Antagonists bind to the same receptor site as the endogenous ligand, but DO NOT stimulate the receptor
- occupy the receptor preventing the endogenous ligand from binding
Types of antagonists
- reversible: competitive and non-competitive
- irreversible
Reversible, competitive antagonists
- Antagonists compete for the same receptor binding site as the endogenous ligand
- When the antagonist is bound the receptor binding site, it blocks the endogenous ligand from binding
- A competitive antagonist always dissociates from the receptor
Reversible, non-competitive antagonists
- Binds to a site other than the endogenous receptor binding site "allosteric modulation"
- Prevents the endogenous ligand from binding at the receptor binding site
- PCP (phenylcyclidine) and ketamine are non-competitive antagonist of the NMDA receptor
Irreversible antagonists
- An antagonist that binds to the receptor binding site and does not dissociate from the receptor
- k-1 is equal to zero; Kd is very low, and affinity is very high
- Some biological weapons are irreversible antagonists
-> Cholinesterase inhibitors ("nerve gases")
- Some irreversible antagonists are highly useful
-> Aspirin (analgesia, anti-inflammatory, antiplatelet)
-> Omeprazole (gastroesophageal reflux disease; GERD)
Signaling mechanisms for drug effects
1. Intracellular Receptors
2. Receptors located on membrane spanning enzymes (like tyrosine kinase)
3. Receptors located on membrane spanning molecule that activates janus kinases (JAK)
4. Receptors located on membrane ion channels
5. G-protein coupled Receptors
G-protein coupled receptors and sub groups
- G-proteins stimulate effectors to produce intracellular changes
subgroups
- Gs (stimulatory)
- Gi (inhibitory)
- Gq (associated with the phosphatidylinositol pathway)
Effectors for G-proteins can be
Ion channels
Adenylyl cyclase (Gi or Gs)
Phospholipase C (Gq)
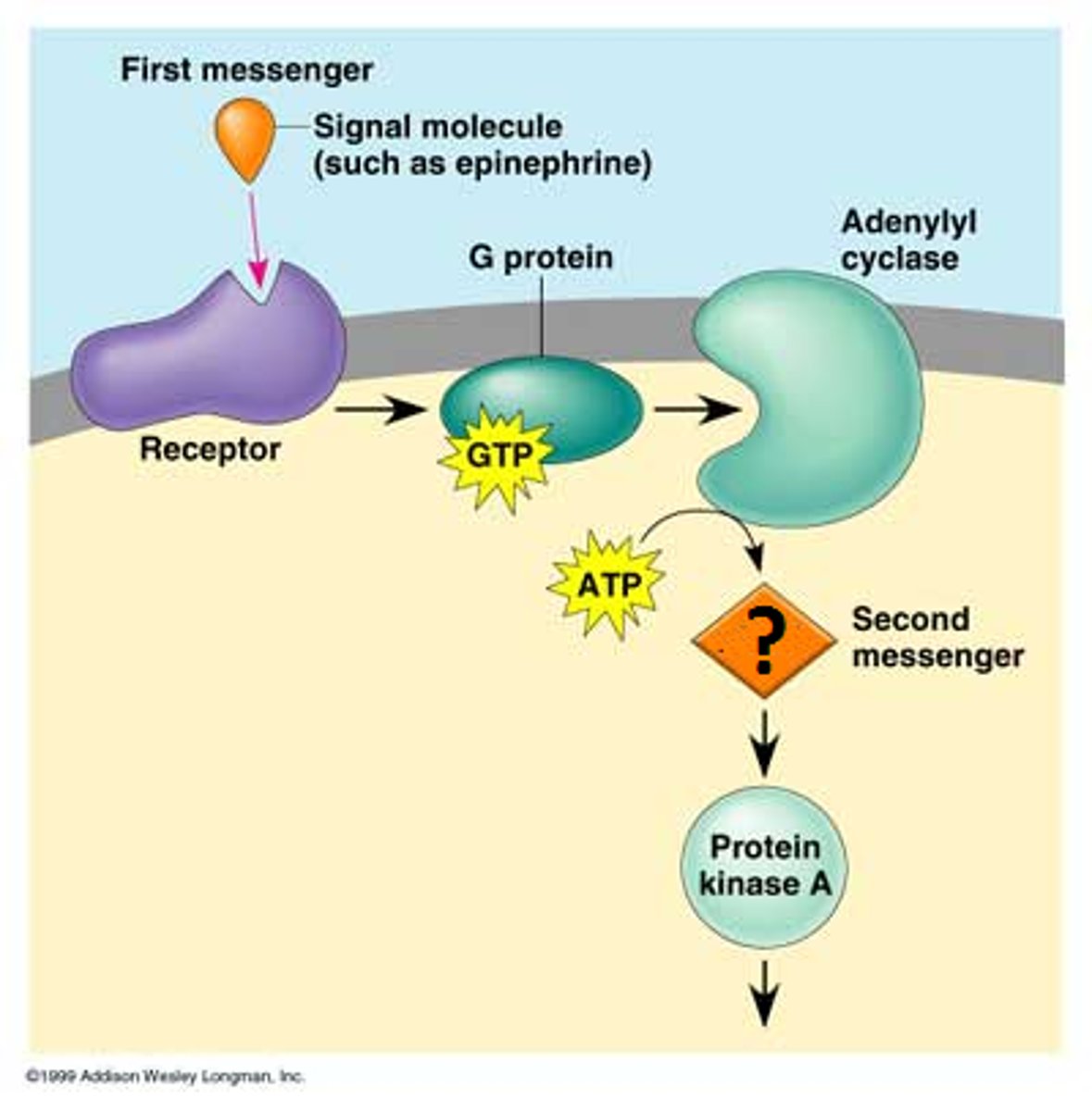
Cyclic AMP signal transduction pathway
- Adenylyl cyclase makes cAMP from ATP
- cAMP acts as a second messenger
Phosphatidylinositol signal transduction pathway
- PLC cleaves PIP to yield IP3 and DAG
- IP3 and DAG are second messengers
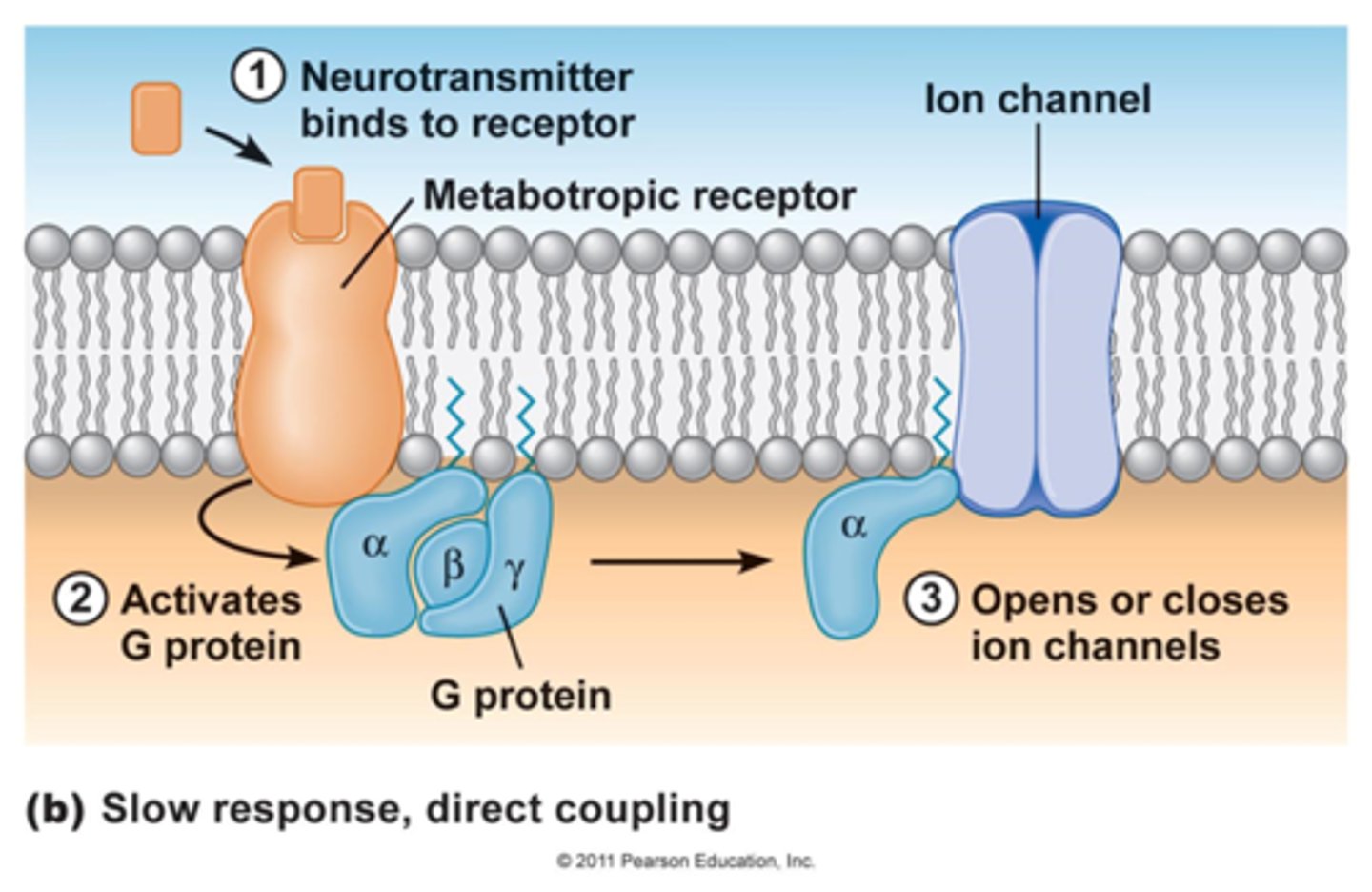
G-protein linked ion channels
- Stimulation of the G-protein induces opening of the ion channel
- cardiac muscarinic receptor
Cardiac atrial muscarinic receptor
- Coupled to a G-protein connected to a potassium channel
- When Ach binds the G protein is simulated and causes the potassium channel to open
- Potassium leaves the cell, hyperpolarizes the cell membrane and slows heart rate
Gs protein linked to adenylyl cyclase
Stimulates adenylyl cyclase (the effector), causing production of cAMP from ATP
cAMP (2nd messenger) binds to and activates protein kinases that activate enzymes by adding a phosphate group
Gi protein linked to adenylyl cyclase
Inhibits adenylyl cyclase, reducing production of cAMP from ATP
Less cAMP binds to and activates protein kinases that activate enzymes
Albuterol/salbutamol
- a bronchodilator
- Specific beta-2 adrenergic agonist
- Binding activates adenylyl cyclase via Gs protein
- increase in cAMP causes activation of enzymes that sequester and inactivate calcium and MLCK (myosin light chain kinase)
- Decreased levels of Ca2+ and MLCK leads to relaxation of the bronchial smooth muscle
Misoprostol
- peptic ulcer drug
- Binds to Gi-linked prostaglandin EP3 receptor
- Inhibits adenylyl cyclase
- cAMP production decreases, protein kinases are not activated by cAMP
- enzymes and pump that produce stomach acid are not activated and production of stomach acid decreases
- This drug also causes uterine contraction (less enzymes sequestering calcium) and is contraindicted in pregnancy
Phospholipase C (PLC)
- Phospholipase C (PLC) is activated by Gq proteins
- The cleaved PIP yields 2nd messengers
-> Inositol trisphosphate (IP3) & DAG (diacylglycerol)
- IP3 binds to the sarcoplasmic reticulum and stimulates the release of Ca2+ into the cytoplasm
- DAG binds to calcium channels on the cell membrane, facilitating the movement of extracellular calcium into the cell
- Calcium influx into the cytoplasm (both pathways) produces the biological response
Ergonovine
- binds to Gq-protein linked prostaglandin E1 receptors in the uterus and Gq-protein linked a1 adrenoceptors in the blood vessels
- Receptor binding stimulates PLC to produce IP3 and DAG
- IP3 binds to the sarcoplasmic reticulum and induces the release of Ca2+ into the cytoplasm
- Induces contraction of the uterus and blood vessels
- Can be used clinically to manage postpartum hemorrhage
- Monitor patient for dangerous increases in blood pressure
Why do we need 2nd messengers?
a) cells are surrounded by a lipid membrane and many endogenous ligands cannot cross. 2nd messengers are used to carry the signal from the surface receptor into the cell
b) a single ligand can induce the formation of lots of 2nd messenger, amplifying the signal
c) second messengers remain in the cytoplasm long after the ligand has dissociated from its receptor, inducing a long lasting response
d) all of the above
d: all of the above
most ligands are too large and not sufficiently fat soluble to enter the cell - 2nd messengers can carry the signal to appropriate intracellular targets and produce a larger and more sustained biological response than what would be produced from a single one-to-one drug-receptor interaction
The uterus contains beta2-adrenergic receptors. what would happen if a beta2-adrenergic agonist was administered to a person in active labour?
a) there would be no effect
b) the strength of uterine contractions would decrease, and the progression of labour would slow
c) the strength of uterine contractions would increase
d) the patient would stop breathing
B: the strength of uterine contractions would decrease, and the progression of labour would slow
drugs bind to any receptor for which it has affinity, causing unintended side effects