Lecture 4 Benign Osseous Neoplasms
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
96 Terms
What are the only pediatric tumors that are characteristically in the epiphysis?
-Chondroblastoma
What are almost always abutting an articular surface, don’t have a sclerotic margin, and are in middle-aged individuals?
-Giant Cell tumor
Giant Cell Tumor
-AKA Osteoclastoma
-Quasi malignant (80% benign, 5-8% of primary malignancies, 15% of benign osseous neoplasms)
-Most common at 20 to 40 years of age
Giant Cell common locations
-Knee (most common)
-Distal radius
-Proximal humerus
-Sacrum
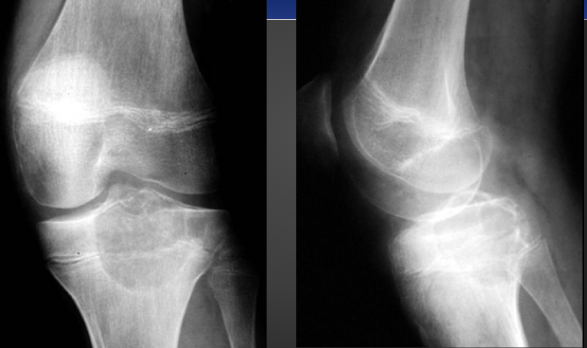
Imaging Feature of Giant Cell Tumor
-Geographic lytic lesion eccentrically located within the metaphysis about the knee, without a sclerotic margin
-In long bone 90% will have subarticular extension
-80 to 90% will not show sclerotic margin
-Multiloculate and septated
-Expansile
-Imaging cannot differentiate malignant from benign
What is indicated by fluid-fluid levels on advanced imaging?
-Aneurysmal bone cyst
Giant Cell Tumor on X-ray

Osteochondroma
-Most common benign skeletal tumor
-75% develop before the age of 20
-Males more commonly affected
-2 types pedunculated & sessile
Clinical Presentation of Osteochondroma
-Most asymptomatic and found incidentally
-Painless hard mass
-Pedunculated may fracture
-May cause compression and irritation on adjacent structures
-Pain and rapid growth suggest malignant degeneration
Cartilaginous cap over how much is concerning for malignant degeneration in osteochondroma?
-Over 1.5 cm
Most common area for Osteochondroma?
-Knee and the humerus
-Adjacent to growth plates and pointing away from articulations
Imaging Features of Osteochondroma
-Corticomedullary continuity
-Pedunculated (thin stalk with large distal cap that is covered in hyaline cartilage)
-Sessile (Broad based osseous excrescence with possible overlying cartilaginous cap)
-Potential sign of accommodation of adjacent osseous structures or signs of soft tissue irritation
Pedunculated Osteochondroma on X-ray

Sessile Osteochondroma on X-ray

Sessile Osteochondroma in Knee on X-ray

Hereditary Multiple Exostoses
-AKA osteochondromatosis
-Multiple osteochondromas that may cause severe boney deformity
-80% discovered by 10 years of age
Clinical Presentation of Hereditary Multiple Exostoses
-5 to 25% malignant degeneration
-Possible symptoms associated with deformity
Distribution of Hereditary Multiple Exostoses
-Knee
-Ankle
-Shoulder
-Hip
-Wrist (madelung-like deformity)
HME on X-ray

Brahma Bull Appears (HME) on X-ray

Madelung-like Deformity on X-ray (HME)

Hemangioma
-Solitary Vascular Neoplasm
-Slow growing
-Most common benign tumor of the spine
-Most common in over 40 years old & females
-2 types cavernous (spine & skull) & Capillary (Ribs, pelvis, metaphyses of long bones)
Clinical Presentation of Hemangioma
-Most are asymptomatic
-Rarely locally aggressive
-Expansion rarely results in neurologic symptoms
Most common location of Hemangiomas
-75% are in the spin and skull
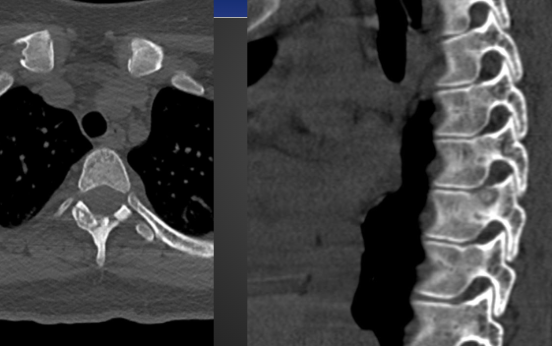
Hemangioma Radiograph Features
-Vertically striated vertebra (Jail bar aka corduroy cloth appearance)
-Lace-like trabeculae in long bones
-Sand dollar, sunburst, or spoke wheel appearance in skull
Hemangiomas on MRI are?>
-High signal on both T1 and T2 due to high fat content
Hemangioma on X-ray (sunburst/sandollar)

Hemangioma in Finger on X-ray

Osteoma
-Exophytic osseous neoplasm
-Usually solitary and in sinuses (Frontal > Ethmoid > Maxillary > Sphenoid)
-Rarely outside of skull
Clinical Presentation of Osteoma
-Most are asymptomatic but can cause chronic sinusitis when obstructing sinus drainage
-Associated with Gardener’s Syndrome (multiple osteomas, Familial adenomatous polyposis, dental abnormalities)
Osteoma on X-ray

Enostoma
-AKA bone island
-Hamartoma of bone
-Essentially an osteoma within the medullary canal
-Any age but adults are more common than children
-Usually solitary and asymptomatic
Distribution of Enostoma
-Long bones (epiphyseal and metaphyseal)
-Medullary
-Ischium
-Ilium
-Sacrum
Imaging Features of Enostoma
-Well defined purely sclerotic lesion that is typically <1cm and shows a ‘brush border’ margin
-Round or oval
-Long axis aligned with the weight bearing trabeculae
-May change size
-Occasionally warm on bone scan
Enostoma on X-ray

Osteoid Osteoma
-In patients 10 to 25 years of age (males more common)
-Cortically based osseous lesion that is highly vascularized and secretes prostaglandins
-Treated with excision or radiofrequency ablation
Classic presentation of Osteoid Osteoma
-Severe pain, worse at night, relieved by aspirin
DDX of Osteoid Osteoma
-Osteoblastoma (based on size)
-Brodie abscess
-Fatigue fracture
Distribution of Osteoid Osteoma
-50% in femur and tibia
-20% hand/feet
-10% spine (neural arch)
Imaging Feature of Osteoid Osteoma
-Central lucent nidus with surrounding sclerosis and solid periosteal reaction
-Cortically based
-Central calcific fleck
-One of the few neoplasms that is better visualized on CT than MRI
Osteoid Osteoma on X-ray

Osteoid Osteoma in the Spine on CT
10% of Osteoid Osteoma will show what?
-Painful scoliosis with lesion at the apex on the concave side
DDX for poorly visualized lesions of Osteoid Osteoma are?
-Fatigue stress fracture and intracortical abscess
Osteoblastoma
-Histologically identical to osteoid osteoma (a giant osteoid osteoma)
-Rare
-Peak age of 10 to 20 years old
-Males more common in
Clinical presentation of Osteoblastoma
-Pain (less severe than OO)
-not nocturnal
-Not relieved by aspirin
-50% of spinal will have a painful scoliosis
-Possible spinal stenosis
Distribution of Osteoblastoma
-Spine 35-50% (posterior elements, thoracolumbar, lower cervical)
-Long bones 30% (metaphysis > diaphysis; lower extremity)
-Hands/feet (dorsal talus; carpal/tarsals)
Osteoblastoma in the spine on Imaging
-Expansile lesion of neural arch
-4-6cm
-thinned cortex
-mostly lucent
-DDX ABC and GCT
Osteoblastoma in the Extremities on imgaing
-Lytic and expansile
-Sparing of the epiphysis
-Lucent nidus >2cm
-Limited peripheral sclerotic reaction
Osteoblastoma on X-ray

What is the most common painless tumor in the hands and feet?
-Enchondroma
Enchondroma
-Most common benign tumor of the hands and feet
-age between 10 to 30 years of age
Enchondroma clinical presentation
-Painless unless complications are present (fracture & malignant degeneration)
Enchondroma clinical Distribution
-Small tubular bones of hands and feet (proximal phalanx is the most common)
-Large tubular bones (femur, tibia, humerus)
Enchondroma Imaging features
-Central geographic lesion in any part of the tubular bone (hands & feet)
-Long bones will have ICE lesion
-Endosteal scalloping <2/3 the width of the cortex (in large bones)
-Stippled calcification 50%
-MRI shows marked hyperintensity on T2 due to high water content in cartilage
Enchondroma on X-ray

Enchondroma on X-ray (knee)
Enchondroma Malignant degeneration on X-ray

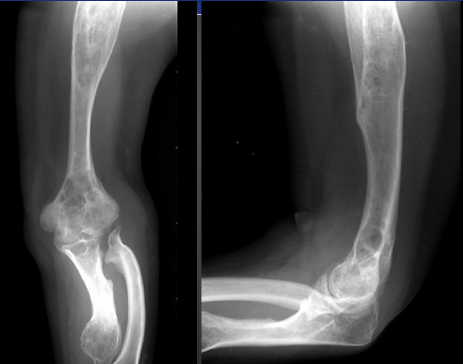
Enchondromatosis
-AKA Ollier’s disease
-Uncommon
-Multiple enchondromas that can be very large and cause severe deformity
-Chance of malignant transformation 10-50%
Enchondromatosis on X-ray

Enchondromatosis on X-ray (not in hands)
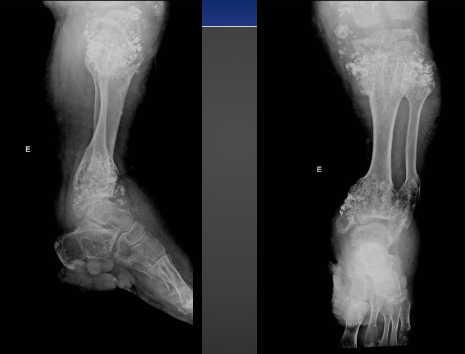
Maffucci Syndrome
-Rare
-Multiple enchondromas with soft tissue hemangiomas
-Malignant transformation in 25 to 50%
Maffucci Syndrome on X-ray
Chondroblastoma
-AKA Codman’s Tumor
-Uncommon chondral tumor
-Peak incidence in 10 to 25 years of age
-More common in males
-Begin to form before physeal closure
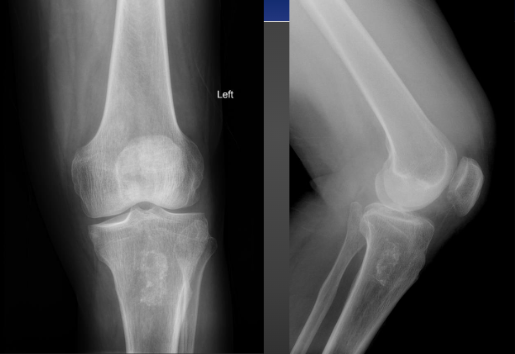
Lytic patellar lesion should be what?
-Chondroblastoma
-Enchondroma
-Giant Cell Tumor
Clinical Presentation of Chondroblastoma
-Pain and tenderness
-Possible soft tissue swelling
-Joint effusion
Distribution of Chondroblastoma
-90% medullary
-Located in the apophyses and epiphyses of long bones
Imaging features of Chondroblastoma
-3 to 6 cm geographic lytic lesion in the apophysis or epiphysis of a long bone in a young patient
-30% show solid or laminated periosteal reaction
-30% show joint effusion
-50% show internal calcification
Chondroblastoma on X-ray
Non-Ossifying Fibroma/Fibrous Cortical Defect
-Very common fibrous lesion
-Males more affected
-30 to 40% of asymptomatic children
FCD age?
-4 to 8
NOF age?
-8-20
Fibroxanthoma age?
-over 20
Clinical Presentation of NOF/FCD
-Typically asymptomatic unless pathologic fracture occurs
-No malignant transformation
-Heals with sclerosis and progressive involution
Distribution of NOF/FCD
-Ankle and knee are common
NOF/FCD Imaging Features
-Called a ‘blister of bone’ because of eccentric, mildly expansile appearance
-Geographic lytic lesion with fibrous “ground glass” matrix
-Multiloculated (soap bubble appearance)
NOF/FCD on X-ray

Simple Bone Cysts is almost always in the?
-Proximal humerus
-Proximal femur
Simple Bone Cyst
-AKA unicameral bone cyst
-Not a true neoplasm
-Peak incidence at 3 to 14 years of age
-More common in males
Clinical Presentation of Simple Bone Cyst
-Asymptomatic until fracture (2/3 present with fracture)
-30 to 40 % reoccur after resection
-No malignant potential
Imaging Features of Simple Bone Cyst
-Centrally located, mildly expansile, unilocular, geographic lytic lesion in the proximal humerus or femur
-Fracture shows fallen fragment sign
Fallen Fragment Sign on X-ray
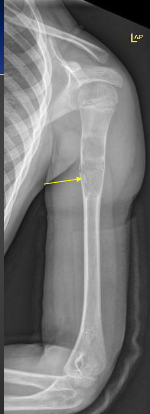
Simple Bone Cyst on X-ray
Aneurysmal Bone Cyst
-Peak incidence in 5 to 20 (80% being less than 18)
-More common in females
-Often seen as a secondary lesion in other primary neoplasms/neoplasm-like processes (GCT, Chondroblastoma, Osteoblastoma, Osteosarcoma, NOF)
Clinical Presentation of Aneurysmal bone cyst
-Acute pain and swelling
-Often post traumatic or post surgical
-Common in neural arch, resembling an osteoblastoma, so pain and signs of stenosis may be present
Distribution of Aneurysmal Bone Cyst
-80% in tubular bones and spine/pelvis
-Most common benign lesion of clavicle
-Eccentric and within metaphysis/diaphysis
Most common benign lesion in clavicle?
-Aneurysmal Bone cyst
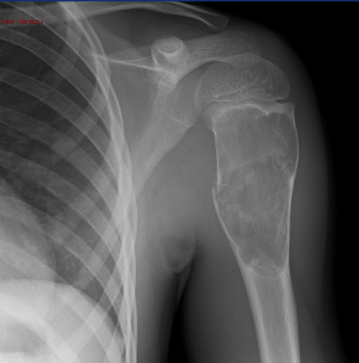
Imaging Feature of Aneurysmal Bone Cyst
-Rapidly expansile, eccentric, soap bubbly, lytic lesion in a young patient
-Often shows fluid-fluid levels on MRI
-Possible periosteal buttressing (may look like codman’s triangle)
-Saccular ballooning of cortex
ABC on X-ray

Cortical buttressing (ABC) on X-ray

Intraosseous Lipoma
-Most common soft tissue tumor but uncommon in bone
-age ranges are 5 to 70 years old
Clinical Presentation of Intraosseous Lipoma
-Aching Pain 70%
-Asymptomatic 30%
What is the most common calcaneal bone lesion?
-Intraosseous Lipoma
Imaging Features of Intraosseous Lipoma
-Geographic lucency that may have a central calcification called a cockade sign
Intraosseous Lipoma on X-ray
