HA lec Thorax and Lungs
1/46
Earn XP
Description and Tags
kapoy mnako
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
above the clavicles
Supraclavicular
below the clavicles
Infraclavicular
between the scapulae
Interscapular
below the scapulae
Infrascapular
the lowermost portions
Bases of the lungs- Upper, middle, and lower lung fields
______ is primarily automatic controlled by respiratory centers in the brainstem.
Breathing
principal muscle of inspiration
Diaphragm
Diaphragm contracts, descends in the chest and expands the thoracic cavity, compressing the abdominal contents and pushing out the abdominal wall.
As thorax expands, intrathoracic pressure decreases, drawing air trough the tracheobronchial tree into the alveoli or distal air sacs, filing the expanding air.
Oxygen diffuses into the adjacent pulmoonary capillaries as CO2 exchanges from blood into the alveoli.
Inspiration
chest wall and lungs recoil and the diaphragm relaxes and rises passively. As air flows outward, the chest and abdomen return to their resting positions.
Expiration
This position examine posterior thorax and lungs.
Patient’s arms should be folded across the chest with hands resting, of possible, on the opposite shoulders. This position swings the scapulae laterally and increases access to the lung fiields. Then ask patient to lie down.
Patient Sitting
Normal Respiratory rate:
14-20 times a minute
Test chest expansion. Place your thumbs at about the level of the ______, with your fingers loosely grasping and parallel to the lateral rib cage. As you position your hands, slide them medially just enough to raise a loose fold of skin on each side between your thumb and the spine.
10th ribs
Ask the patient to inhale deeply. Watch the distance between your thumbs as they move apart during inspiration, and feel for the range and symmetry of the rib cage as it expands and contracts. This is sometimes termed _________.
lung excursion
________ refers to the palpable vibrations transmitted through the bronchopulmonary tree to the chest wall as the patient is speaking.
Fremitus
To detect fremitus, use either the ____ (the bony part of the palm at the base of the fingers) or the _____ surface of your hand to optimize the vibratory sensitivity of the bones in your hand. Ask the patient to repeat the words “ninety-nine” or “one-one-one.” If fremitus is faint, ask the patient to speak more loudly or in a deeper voice.
ball or ulnar
is typically more prominent in the interscapular area than in the lower lung fields and is often more prominent on the right side than on the left. It disappears below the diaphragm.
Fremitus
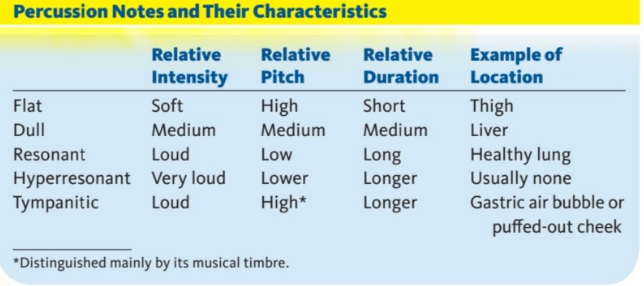
sets the chest wall and underlying tissues in motion, producing audible sound and palpable vibrations
Percussion
Percussion helps you establish whether the underlying tissues are air-filled, fluid-filled, or solid. It penetrates only____ to ____ into the chest, however, and will not help you to detect deep-seated lesions.
5 cm to 7 cm
Study this
Percuss one side of the chest and then the other at each level in a _______ pattern, as shown by the numbers below. Omit the areas over the scapulae—the thickness of muscle and bone alters the percussion notes over the lungs. Identify and locate the area and quality of any abnormal percussion note
ladderlike
estimate the extent ofdiaphragmaticexcursion by determining the distance between the level ofdullness on full expiration and the level of dullness on full inspiration, normally about ______.
3 to 5.5 cm.
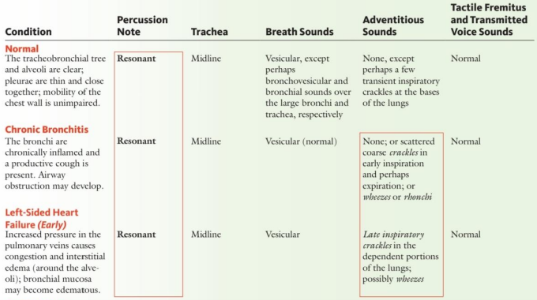
They are heard through inspiration, continue without pause through expiration, and then fade away about one third of the way through expiration.
Vesicular, or soft and low pitched.
with inspiratory and expiratory sounds about equal in length, at times separated by a silent interval. Detecting differences in pitch and intensity is often easier during expiration.
Bronchovesicular
with a short silence between inspiratory and expiratory sounds. Expiratory sounds last longer than inspiratory sounds.
Bronchial, or louder, harsher and higher in pitch
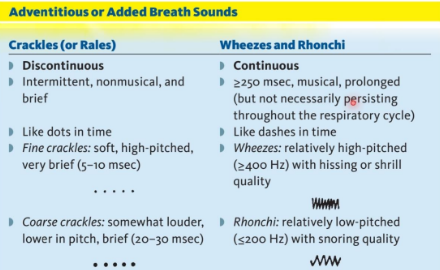
Listen for any __________ sounds that are superimposed on the usual breath sounds. Detection of adventitious sounds—crackles (sometimes called rales), wheezes, and rhonchi—is an important part of your examination, often leading to diagnosis of cardiac and pulmonary conditions
Adventitious (Added) Sounds
Study this
If you hear abnormally located bronchovesicular or bronchial breath sounds, assess _______. With a stethoscope, listen in symmetric areas over the chest wall as you assess any abnormal vocal resonances suspicious for pneumonia or pleural effusion.
transmitted voice sounds
Position: patient should lie comfortably with arms somewhat abducted. Examine a patient having difficulty breathing in the sitting position or with the head of the bed elevated to a comfortable level.
supine position
Compare both sides of the chest, using the ball or ulnar surface of your hand. Fremitus is usually decreased or absent over the precordium. When examining a woman, gently displace the breasts as necessary.
Percuss the anterior and lateral chest, again comparing both sides. The heart normally produces an area of dullness to the left of the sternum from the ___ to the ___ interspaces. Percuss the left lung lateral to the area of dullness.
Assessment of tactile fremitus.
3rd to the 5th
The thorax in a _______ is wider than it is deep. Its lateral diameter is larger than its anteroposterior diameter.
Normal Adult
Note depression in the lower portion of the sternum. Compression of the heart and the great vessels may cause mursmurs.
Funnel Chest (Pectus Excavatum)
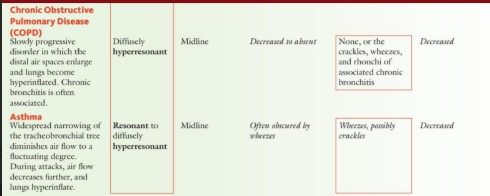
There is an increased anteroposterior diameter. This shape is normal during infancy, and often accompanies aging and chronic obstructive pulmonary disease.
Barrel Chest
The sternum is displaced anteriorly, increasing the anteroposterior diameter. The coastal cartilages adjacent to the protruding sternum are depressed.
Pigeon Chest (Pectus Carinatum)
Multiple rib fractures may result in paradoxical movements of the thorax. As descent of the diaphragm decreases intrathoracic pressure, on inspiration the injured area caves inward; on expiration, it moves outward.
Traumatic Flail Chest
Abnormal spinal curvatures and vertebral rotation deform the chest. Distortion of the underlying lungs may make interpretation of lung findings very difficult.
Thoracic Kyphoscoliosis
Crackles have two leading explanations.
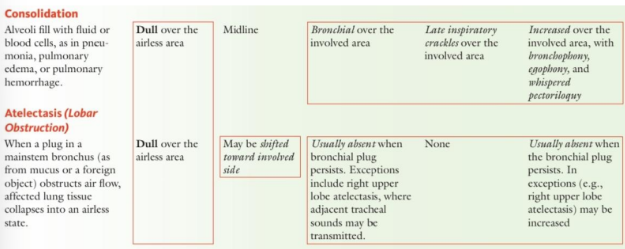
(1) They result from a series of tiny explosions when small airways, deflated during expiration, pop open during inspiration. This mechanism probably explains the late inspiratory crackles of interstitial lung disease and early heart failure.
(2) Crackles result from air bubbles flowing through secretions or lightly closed airways during respiration. This mechanism probably explains at least some coarse crackles.
may begin in the first half of inspiration but must continue into late inspiration. They are usually fine, fairly profuse, and persist from breath to breath. They appear first at the bases of the lungs, spread upward as the condition worsens, and shift to dependent regions with changes in posture. Causes include interstitial lung disease (such as pulmonary fibrosis) and early heart failure.
Late inspiratory crackles
appear and end soon after the start of inspiration. They are often coarse and relatively few in number. Expiratory crackles are sometimes associated. Causes include chronic bronchitis and asthma.
Early inspiratory crackles
are heard in bronchiectasis but are not specific for this diagnosis. Wheezes and rhonchi may be associated.
Midinspiratory and expiratory crackles
occur when air flows rapidly through bronchi that are narrowed nearly to the point of closure. They are often audible at the mouth as well as through the chest wall. Causes of wheezes throughout the chest include asthma, chronic bronchitis, COPD, and heart failure (cardiac asthma). In asthma, wheezes may be heard only in expiration or in both phases of the respiratory cycle. Rhonchi suggest secretions in the larger airways. In chronic bronchitis wheezes and rhonchi often clear with coughing.
Occasionally in severe obstructive pulmonary disease, the patient is unable to force enough air through the narrowed bronchi to produce wheezing. The resulting silent chest is ominou
and warrants immediate attention.
Persistent localized wheezing suggests partial obstruction of a bronchus, seen with a tumor or foreign body. It may be inspiratory, expiratory, or both.
Wheezes
It is often louder in the neck than over the chest wall. It indicates a partial obstruction of the larynx or trachea, and demands immediate attention.
stridor
A wheeze that is entirely or predominantly inspiratory is called.
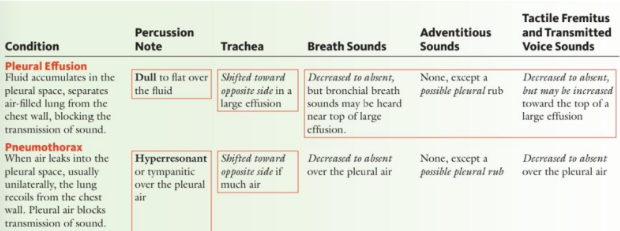
Inflamed and roughened pleural surfaces grate against each other as they are momentarily and repeatedly delayed by increased friction. These movements produce creaking sounds known as a __________________, usually during expiration.
______resemble crackles acoustically, although they are produced by different pathologic processes. The sounds may be discrete, but sometimes are so numerous that they merge into a seemingly continuous sound. A rub is usually confined to a relatively small area of the chest wall, and typically is heard in both phases of respiration. When inflamed pleural surfaces are separated by fluid, the rub often disappears.
pleural rub (or pleural friction rub)
A _______ is a series of precordial crackles synchronous with the heart beat, not with respiration. Best heard in the left lateral position, it is due to mediastinal emphysema (pneumomediastinum).
mediastinal crunch
Study this
Study this
Study this
Study this