CHAPTER 11: HOST MODULATION & IMPLANT THERAPY
1/51
Earn XP
Description and Tags
ppt + discussion
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
host modulation therapy (HMT)
used in addition to SRP and surgery
modifies or reduces destructive aspects and regulates protective aspects of the host response
adjunctive approach to conventional periodontal therapy targeting the patient’s immune-inflammatory response, which drives tissue breakdown
purpose of host modulation therapy (HMT)
periodontal stability
enhance wound healing
aims to reduce excessive inflammation
risk factors of host modulation therapy (HMT)
addresses the host side of the host-bacterial interaction
produces excessive inflammatory processes to enhance wound healing and periodontal stability
addresses factors that adversely affect host response (ex: smoking, diabetes, genetic susceptibility)
drug classes that evaluated as HMTs:
BMPs
NSAIDs
growth factors
tetracyclines
bisphosphonates
enamel matrix proteins
comprehensive management of host modulation therapy
patient education
bacterial reduction (SP)
site-specific antibacterial treatment
risk factor modification
surgery if needed
host modulation therapy (HMT) agents
NSAIDs
bisphosphonates
sub-antimicrobial-dose doxycycline (SDD)
NSAIDs
systemic use can significantly slow alveolar bone loss
inhibit prostaglandin (PGE2), which regulates bone resorption
stopping it may cause a “rebound effect” with accelerated bone loss
not indicated as adjunctive HMT due to serious side effects and the need for long-term daily use
risk of NSAIDs
GI problems
hemorrhage
higher fragility of bone
—due to daily use for up to 3 years showed benefits however these can be an effect:
bisphosphonates
inhibits osteoclast activity, shown to enhance alveolar bone status in studies.
bone-seeking agents that inhibit bone resorption by disrupting osteoclast activity
not approved for periodontal disease; discouraged due to risk primarily with intravenous use
risk of bisphosphonates
osteonecrosis of the jaws (ONJ)
sub-antimicrobial-dose doxycycline (SDD)
must not be used as monotherapy
can be combined with local antimicrobial delivery systems
only FDA-approved systemically administered HMT adjunct to SRP for chronic periodontitis
acts via:
enzyme, cytokine reduction
MMP (MMP-8 and MMP-9) inhibition
osteoblast stimulation—not an antibiotic effect
MMP → matrix metalloproteinases (ex: Periostat)
indications of sub-antimicrobial-dose doxycycline (SDD)
chronic and aggressive periodontitis as adjunct to SRP
in refractory cases and high-risk patients (smokers, diabetics, osteoporotic, genetically susceptible)
contraindications of sub-antimicrobial-dose doxycycline (SDD)
children <12 years
allergy to tetracycline
pregnancy / lactation
disadvantage: may reduce efficacy of oral contraceptives
benefits of sub-antimicrobial-dose doxycycline (SDD)
gains in attachment
reduced probing depth
stimulates osteoblasts
no resistance risk at 20mg dose
effective even in high-risk patients (e.g., smokers)
dosage of sub-antimicrobial-dose doxycycline (SDD)
20mg BID for 3–9 months → first round of SRP
SDD + local delivery (atridox) + SRP
demonstrated >2mm improvement in attachment gains and probing depth reductions vs SRP alone (p<0.0001) in a 6-month, 180 patient trial
locally administered HMTs
used as adjuncts to surgical procedures to stimulate regeneration
topical NSAIDs have not been approved
examples of FDA-approved locally administered HMTs
enamel matrix proteins (Emdogain)
bone morphogenetic proteins (rhBMP-2 / INFUSE)
recombinant human platelet-derived growth factor-BB (GEM 215)
discovery of osseointegration
in the 1950s, Per-Ingvar Bränemark discovered an intimate bone-to-titanium apposition while studying blood circulation in bone (a serendipitous breakthrough)
his implants anchored prosthetic teeth in edentulous jaws; the first patient was treated in 1965
subsequent studies confirmed 15-year success with CP titanium implants using a strict unloaded healing protocol.
the standard early implant designs
screw-shaped threaded cylindric implant
osseointegration
clinically defined as asymptomatic rigid fixation
historically defined as direct structural and functional connection between living bone and implant surface without soft tissue
initial healing of osseointegration
mirrors bone fracture repair
immobility: movement >150 μm prevents osteoblast differentiation → fibrous scar tissue → nonintegration
temperature: bone necrosis occurs if overheating during drilling exceeds 47°C for 1min
bone maturation
steady remodeling state reached after 18 months
progresses from fast-growing, poorly mineralized woven bone to slow-growing, dense lamellar bone
primary stability (placement) of osseointegration
depends on implant geometry and bone quantity/quality
secondary stability (over time) of osseointegration
depends on implant surface and percentage of bone contact
peri-implant soft tissues
includes:
oral epithelium, sulcular epithelium
a sulcus, long junctional epithelial attachment
underlying connective tissue — similar to teeth
implant
bone is in direct contact with the implant
lacks PDL, cementum, and Sharpey’s fibers
long junctional epithelium
attaches to titanium via basal lamina and hemidesmosomes
peri-implant “biologic width”
3-4mm or 4-4.5mm
combined height of epithelial attachment and supracrestal connective tissue
connective tissue fibers
cannot insert into the implant surface
run mostly parallel or in a cuff-like circular orientation, forming a soft tissue “seal”
laser-microgrooved surfaces can stop epithelial down-growth and establish perpendicular connective tissue insertion
keratinized tissue
not required for long-term success
may cause pain or discomfort during oral hygiene due to mobility of nonkeratinized mucosa
not a strict prerequisite for success, but its absence Increases susceptibility to peri-implant problems and patient discomfort during oral hygiene.
soft tissue grafting can augment it
vascular supply
scarcer than around teeth; no contribution from PDL
peri-implant tissues respond to plaque with inflammation similar to periodontal tissues
probe stops in healthy tissue
1.5mm coronal to alveolar crest (above the bone)
clinical consequences (teeth vs. implants)
lack of resiliency:
implants lacks PDL, so they are rigidly attached and cannot move to compensate for occlusal disharmony
overload can cause microfractures and bone loss
growth:
implants placed before growth completion will not migrate or erupt with natural teeth
can lead to occlusal problems; therefore, contraindicated in growing patients
maintenance:
long-term success requires meticulous plaque control
frequent maintenance visits are recommended every 3-4 months
comprehensive periodontal management
patient education & oral hygiene
high-quality SRP + local delivery
host modulation (SDD)
risk factor modification
surgery + HMT if indicated
implant geometry: macrodesigns
blade implants
pins & disks implants
subperiosteal implants
transmandibular staple implants
blade implants
<50% success at 5 years
thin, flat metal plates inserted into the jawbone
removal required sacrificing significant surrounding bone
designed for narrow ridges where standard implants won’t fit
popular in the past, but now rarely used due to lower long-term success (attributed to biotolerance, not osseointegration)
relied on fibroosseous integration → fibrous scar tissue at the bone-implant interface → mistakenly thought to mimic the pdl
high-speed drilling can cause:
necrosis
marsupialization
epithelial downgrowth
transmandibular implants
used for severely resorbed mandibles
now largely obsolete due to safer alternatives
requires major surgery under general anesthesia
a metal plate placed through the entire lower jaw (mandible)
stable implant: 93% survival at 5 years but 10-15% complication rate
pins & disks implants
fibrous encapsulation and infection led to implant loss
pins:
small metal pins inserted into bone
used to stabilize dentures or other implants
limited use today
disk implants:
flat, circular implants placed laterally into bone
designed for thin jawbones
also mostly outdated
subperiosteal implant
used when there is insufficient bone height
placed on top of the bone but under the gum
<50% survival at 5-10 years; rarely used today
custom metal framework supports prosthetic teeth
fibrous encapsulation and rapid bone resorption led to abandonment
root form implants
ITI hollow cylinder
IMZ solid cylinder
screw-shaped
ITI hollow cylinder
developed by Straumann (formerly ITI)
hollow cylindrical design placed into bone
early version of modern implant systems
allows bone ingrowth to grow into the hollow space
disappointing survival rates → withdrawn from use
IMZ solid cylinder
developed in Germany (IMZ system)
aimed to mimic natural tooth movement
eventually fell out of favor due to mechanical complications
solid cylindrical implant with an internal shock-absorbing element
89.9% at 60 months, but only 38% at 10 years
screw-shaped
parallel or tapered geometry
most widely used implant today
high success rate and long-term stability
root-form design that mimics natural tooth roots
threaded design disperses axial forces in multiple directions
surgically inserted into bone and integrates via → osseointegration
implant surface: microdesign
additive processes
subtractive processes
surface free energy
additive processes
you add material onto the implant
like coating or layering something on top
makes the surface more friendly for bone to attach
ex:
plasma spraying
hydroxyapatite coating
calcium phosphates → increase surface roughness and accelerate initial bone cell adaptation
subtractive processes
you remove material from the implant
like scratching or roughening the surface
helps the bone grip the implant better
rough surfaces → speed bone apposition but may increase ion leakage and macrophage adherence
ex:
machining, acid etching
blasting-promote favorable cellular responses
increased bone formation at the microscopic level
surface free energy
related idea → wettability (how easily liquid spreads)
how well the implant surface attracts liquids (like blood)
if not → healing is slower
if it attracts liquid well → bone cells stick better
bone-to-implant interface rigidity
the predominant biomechanical factor for load-bearing success
soft tissue interface quality
critical for stable marginal bone levels long-term
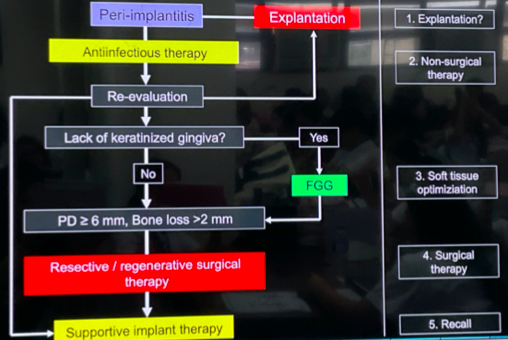
treatment sequence for peri-implant infection