Salvo: Thyroid Dysfunction and Pharmacotherapy
1/65
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
primary hypothyroidism
inadequate secretion of thyroid hormones from the thyroid gland
secondary hypothyroidism
pituitary or hypothalamic failure
hypothyroidism s/s
· Weight gain
· Dry skin
· Cold intolerance/sensitivity
· Constipation
· Myalgias
· Bradycardia
· Weakness
· Depression
· Fatigue
· Coarse skin and hair
· Hoarse voice
· Slowed speech
hyperthyroidism s/s
· Nervousness
· Anxiety
· Irritability
· Heat intolerance
· Palpitations
· Easily fatigued
· Weight loss (with increased appetite)
· Warm, smooth, moist skin
· Fine tremor
· Increased frequency of bowel movements
· Fine hair
5 causes of primary hypothyroidism
o Hashimoto's disease
o Iodine deficiency
o Surgical removal of all or part of the thyroid
o Thyroid gland ablation with radioactive iodine
o Medications
what is the cause of secondary hypothyroidism
pituitary failure
what are the causes of hyperthyroism
all considered thyrotoxicosis
o Graves' disease
o Iodine-induced (excess intake, exposure to radiographic contrast media)
o Medications (Excessive doses of levothyroxine)
lab values in hypothyroidism
HIGH TSH
low total T3, total T4, and free T4
lab values of hyperthyroidism
LOW TSH
high total T3, total T4, and free T4
2 parts of hyperthyroidism diagnosis
high free T4 and low TSH
Biotin impact on thyroid labs
biotin > 5000mcg/day can falsely increase T3 and T4 and falsely decrease TSH
hold biotin for 24-48 hours before testing
3 goals of thyroid disease therapy
· Resolution of signs and symptoms
· Safe and effective medication use
· Medication adherence
brand names of levothyroxine
synthroid, levoxyl, levothroid, unithroid
what is levothyroxine
synthetic L-isomer of T4/thyroxine
when should follow-up/monitoring be done with levothyroxine
at 6 weeks (full effect seen)
what is considered the most sensitive and clinically relevant measurement of thyroid function
TSH
why should we try to keep patients on the same thyroid product/brand of medication
FDA’s current determination of bioequivalence provides no guarantee that a patient’s effectively absorbed dose will remain constant enough to stabilize TSH levels if patient is switched from product to product
LT4/levothyroxine dosing in age >12 without cardiac disease
1.6-1.7 mcg/kg/day
levothyroxine/LT4 dosing in older adults with known cardiac disease
1 mcg/kg/day (use IBW in obese pts)
or start 12.5-25mcg/day and titrate to full replacement dose
IV: PO conversion of levothyroxine
0.75:1
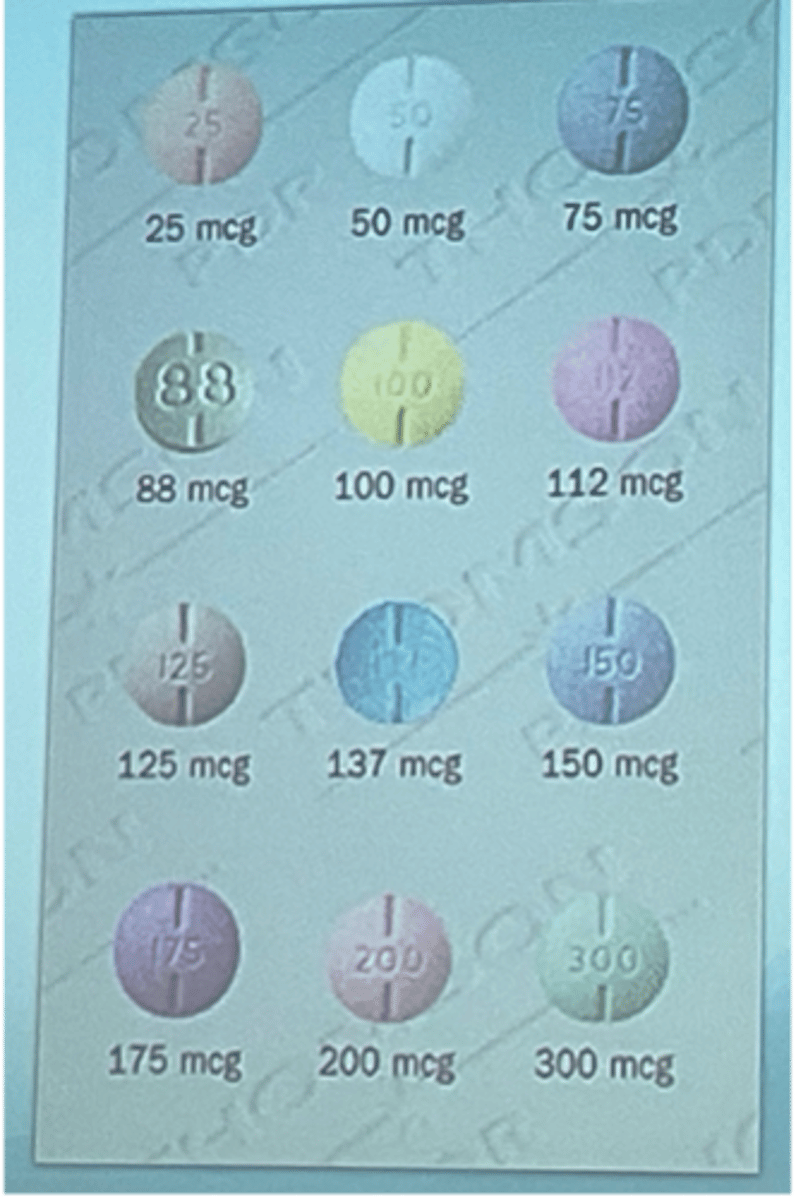
doses of levothyroxine
doses usually increase by 12-25 mcg
pregnancy dosing of levothyroxine
Will need an increased dose
after delivery, adjust to pre-pregnancy dose
TSH goals in 1st vs 2nd and 3rd trimester of pregnancy
§ 1st trimester <2.5mIU/L
§ 2nd and 3rd trimester: < 3 mIU/L
what drugs can cause decreased absorption of levothyroxine (need a dose increase)
Aluminum hydroxide, calcium, ferrous, dietary fiber, espresso, bile acid sequestrants, PPIs, H2Ras
what diseases can cause decreased absorption of levothyroxine (need a dose increase)
§ Mucosal disease (i.e. celiac disease, gastric bypass)
what drugs can cause increased clearance of levothyroxine (need a dose increase)
rifampin, carbamazepine, phenytoin, and phenobarbital
what 2 factors can cause a decreased conversion of T4 to T3 and will need an increased dose of levothyroxine
amiodarone, selenium deficiency
what 3 factors may need a dose decrease with levothyroxine
-increasing age
-post-delivery of a baby
-withdrawal of an interacting product
how to to titrate LT4 when monitoring TSH levels
adjust dose by 10-20%
consider available strengths
what does euthyroid mean
TSH levels in the normal range
monitoring frequency once a patient is euthyroid
monitor q 6-12 months
over treatment risks with levothyroxine
o HF, AF, angina, MI
o Osteoporotic effects (in postmenopausal women)
under treatment risks with levothyroxine
o Continued symptoms of hypothyroidism
o Depression
o Obstetric complications
when to take levothyroxine (pt counseling)
· Take 30 mins before food (and other meds)
o Or 2 hours after food/interacting products
o Or at bedtime
what should levothyroxine not be taken within 4 hours of?
Calcium or iron supplement or bile acid sequestrant
liothyronine brand name
cytomel
what is liothyronine
synthetic T3
starting and usual dose of liothyronine (cytomel)
starting: 25 mcg/day
usual dose: 25-75 mcg/day
dosing of liothyronine (cytomel) in those with cardiac disease or elderly
5 mcg PO QD
liotrix
o Combination of synthetic T4 and T3 in a ratio of 4:1
o High cost and lack therapeutic rationale
desiccated thyroid (thyroid USP)
o Contains T3 and T4
o Animal protein-derived
what are the 3 treatment options for hyperthyroidism
· Antithyroid medications (thionamides)
· Radioactive iodine
· Surgery
methimazole (MMI) brand name
tapazole
dose forms and frequency of methimazole (tapazole)
5mg and 10 mg tablets
administered 2-3 x day
what is the preferred thioamide
methimazole
methimazole use in pregnancy
· Use in 2nd and 3rd trimesters of pregnancy with lowest effective dose
when is the max effect of methimazole seen
4-8 weeks
propylthiouracil (PTU) MOA
inhibits conversion of T4 to T3
propylthiouracil dose forms and frequnecy
50 mcg tablet
admin 3-4 times/day
use of propylthiouracil in pregnancy
· Preferred treatment in 1st trimester of pregnancy, in thyroid storm, and in those unable to tolerate MMI
what is a concern with propylthiouracil
possible hepatotoxicity
monitoring timing of MMI and PTU
· Assess thyroid function in 4-6 weeks --> improvement should be noted
· Once stable/euthyroid, monitor thyroid function q 2 months
· Continue treatment for a minimum of 12-24 months
o After remission occurs, follow up every 6 to 12 months
what 2 things should be monitored with MMI and PTU
CBC and LFTs
major ADRs of thionamides (MMI and PTU)
o Agranulocytosis (usually within first 3 months)
§ Flu-like symptoms (fever, malaise)
§ Granulocyte count (< 200-500/mm^3)
§ Do NOT use other thionamide
o Hepatotoxicity
lab values for agranulocytosis
granulocyte count (<200-500/mm^3)
minor ADRs of thionamides (MMI and PTU)
o Rash (maculopapular)
o Arthralgias
o GI intolerance
o Fever
o Benign transient leukopenia (WBC < 4000/mm^3)
§ Cross-sensitivity ~50%
iodide MOA
blocks release of thyroid hormone and thyroid hormone synthesis and decreases gland size and vascularity
what are the 3 uses of iodide
· prepare Graves' disease patient for surgery, quickly achieve euthyroid, or following radioactive iodine
symptoms improve in 2-7 days
MOA of radioactive iodine (131 I)
· Concentrates in the thyroid and disrupts hormone synthesis
when is radioactive iodine the agent of choice (3 circumstances)
· Graves' disease, toxic autonomous nodules, and toxic MNGs
contraindication of radioactive iodine
pregnancy
when to withdraw/start thionamide with radioactive iodine use
withdraw the thionamide 4-6 days before use
restart 4 days after radioactive iodine treatment
surgery for hyperthyroidism requirement
· Must be euthyroid before undergoing
o Can use meds
pros/cons of surgery for hyperthyroidism
· Rapid onset and highest efficacy
· Most invasive and costly
· Surgical complications are low
beta blockers in hyperthyroidism
· Symptomatic relief
· Adjunct treatment with thioamides, iodides, I-131, or in preparation for surgery
which beta blocker is used for hyperthyroidism? dose?
propanolol 20-40 mg QID