Exam 2 (Part 2)
1/56
Earn XP
Description and Tags
Lecture 13, 14, 15
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
57 Terms
somatoform (definition)
excessive thoughts, feelings, and behaviors about a bodily sensation
disproportionate & persistent thoughts about the seriousness of symptom(s)
excessive time & energy devoted to symptom(s)
aberrant physical fixations that one overexaggerates
somatoform assessment
MMPI or MSPQ
MSPQ : uses pain free somatoform items
clients high in somatoform endorse many different types of symptoms
somatoform (& HiTOP)
somatoform is the outlier → normal personality measures do not reveal this measure of psychopathology
negative affectivity (neuroticism) is STRONGLY associated with internalizing
*considered the most tentative spectra
emotional dysfunction superspectrum connects small shared variance between somatofrom and internalizing
pain vs. somatoform
pain — subjective physical suffering
somatoform — experience of physical sensations that are disproportionate to, or unexplained by, a physical cause
somatoform (with pain)
patient with fibromyalgia whose symptoms aren’t responding to/managed by typical intervention
disproportionate & persistent thoughts about seriousness of pain symptoms
excessive time & energy devoted to pain symptoms
somatic symptom disorder (criteria)
one ore more somatic symptoms that are distressing or result in significant disruption of daily life
excessive thoughts, feelings, or behaviors related to the somatic symptoms or associated with health concerns as manifested by at least one of the following
disproportionate and persistent thoughts about the seriousness of one’s symptoms
persistently high level of anxiety about health or symptoms
excessive time and energy devoted to these symptoms or health concerns
state of symptomatic is persistent (typically more than 6 months)
somatic symptom disorder (contributory causes)
past experiences with illness in self, family, or media that create dysfunctional assumptions about symptoms
negative affect (especially when paired with suggestion and difficulty naming emotions)
secondary reinforcement : illness may bring comfort, attention, or release from responsibilities
somatic symptom disorder (risk factors)
comorbidity with depression and anxiety
more likely to be diagnosed in women
illness anxiety disorder / hypochondria (criteria)
preoccupation with having or acquiring a serious illness
somatic symptoms are not present, or, if present, are only mild in intensity. if another medical condition is present or there is a high risk for developing a medical condition, the preoccupation is clearly excessive or disproportionate
there is a high level of anxiety about health, and the individual is easily alarmed about personal health status
illness preoccupation has been present for at least 6 months
the illness related to preoccupation is not better explained by another disorder
somatic symptom disorder + health anxiety (interventions)
CBT : challenge illness beliefs, reinterpret bodily sensations, reduce checking/reassurance seeking
pain-focuses : relaxation, activity scheduling, cognitive restructuring, reinforcement of “no-pain” behaviors
antidepressants may reduce pain intensity/mood effects
medical management
functional neurological symptom disorder / conversion disorder (definition)
applied to patients who present neurobiological symptoms (numbness, blindness, paralysis, or fits) which are not consistent with a well-established organic cause
functional neurological symptom disorder (symptoms)
sensory
blindness or tunnel vision
deafness
anesthesia, including “glove anesthesia”
motor
paralysis or selective loss of function
aphonia (whispering without true laryngeal paralysis)
globus : feel of a lump in the throat
seizure-like symptoms
episodes resembling seizures
no matching EEG changes
often more thrashing and less injury than true seizures
functional neurological symptom disorder (causes)
psychodynamic
symptoms linked to unconscious conflict
behavioral
symptoms may provide negative reinforcement or positive reinforcement
neuroimaging
affected body parts are stimulated/moved → expected sensory/motor areas may show reduced activation while emotion regions (anterior cingulate, insula, orbitofrontal cortex) become more active
*emotion-processing networks can override normal sensory or motor processing
functional neurological symptom disorder (treatment)
stress-management approaches
behavior rehab for motor symptoms
CBT for seizures
hypnosis
factitious disorder / munchausen (definition)
a condition in which a person, without a malingering motive, acts as if they have an illness by deliberately producing feigning, or exaggerating symptoms, purely to attain (for themselves or for another) a patients role
factitious disorder imposed on another
a condition in which a person deliberately produces, feigns, or exaggerates the symptoms of someone in their care
dissociation disorder
disruptions in normally integrated functions of consciousness, memory, identity, or perception
*50-74% of people experience mild depersonalization/derealization at least once
what makes dissociation pathology?
symptoms become disruptive, create loss of needed information, or profduce jarring discontinuities in experience and sense of self
depersonalization (definition)
a feeling of detachment or estrangement from one’s self; feeling as if you are onlooking of your own body
depersonalization (symptoms)
detachment from the world and one’s self
embodiment, denoting unusual or changing experiences of the body
identity changes, a lack of congruence between one’s felt self and one’s words and action
derealization (definition)
an alteration in the perception of one’s surroundings so that a sense of reality of the external world is lot; the world you are experiencing does not seem real
derealization (symptoms)
sense of “fog”
see-through wall or veil separating you from surroundings
world appears lifeless, muted, or fake
objects/people look “wrong”
sounds are distorted
time speeds up or stands still
depersonalization/derealization (prevalence)
1-2% lifetime prevalence
mean onset of age 16
~80% chronic course
sex distribution about equal
depersonalization/derealization (associated clincial features)
mood and anxiety disorders commonly co-occur
avoidant, borderline, and obsessive-compulsive personality disorders are elevated (all marked by severe interpersonal distress)
episodes can feel frightening and may create fear of mental collapse
depersonalization/derealization (treatments)
no clearly effective medication/psychotherapy
clinical help for managing stressors and reducing anxiety
dissociative amnesia (definition)
an inability to recall important autobiographical information, usually of a traumatic or stressful nature, that is inconsistent with ordinary forgetting
*gaps often follow intolerably stressful circumstances such as combat, catastrophic events, suicide attempts, or other trauma
retrograde amnesia
when dissociative amnesia affects finding old memories
anterograde amnesia
when dissociative amnesia blocks the formation/storage of new memories
*very rare, typically reserved for neurological injuries/diseases
dissociative amnesia (case research)
primary deficit is episodic or autobiographical memory
implicit memory often remains available (explicit is impaired)
dissociative fugue (flight + amnesia)
subtype of dissociative amnesia
person not only becomes amnesic for parts of the past but also leaves home and may assume a new identity
when fugue remits, original amnesia often clears but is replaced by amnesia fro the fugue period
dissociative amnesia (treatment)
place person in a safe environment (memory may return when threat is removed)
hypnosis and certain sedating drugs
identity confusion
struggling with sense of self
identity alteration
shifts in identities, behaviors, and/or personas
manifestations of alters (or alternative identities) containing and expressing differing opinions, perceptions, and sense of self
individuals may notice a shift in a sense of how old they are, gender identity, preferences, skills, and memories
vocal pitch, body language, and physical reactivity to stress
identity confusion/alteration (criteria)
disruption of identity characterized by 2+ distinct personality states or possession-like states
recurrent gaps in recall for everyday events, important personal information, and/or traumatic events
disruption can be observed by others or self-reported by the patient
symptoms must not be better explained
alters
most frequently encountered identity is often called the host identity
switches can be rapid or gradual
amnesia across identities is often present, but may not be perfectly symmetrical
identity confusion/alteration (trauma theory)
DID begins in early repeated trauma and reflects an attempt to cope with helplessness and powerlessness
child may dissociate, fantasize, or imagine the abuse is happening to someone else
fantasy proneness and hypnotizability may function as vulnerability facts in a diathesis-stress model
*95% of DID patients report severe childhood abuse by some estimates
identity confusion/alteration (sociocognitive theory)
DID develops when a highly suggestible person learns to adopt and enact multiple identities
clinician suggestion, hypnosis, media portrayal, and cultural scripts may help shape the disorder
role enactment is not assumed to be consciously faked
number of alters sometimes increases with time in therapy
identity confusion/alteration (treatment)
trauma-based origin, aiming for integration of alters
psychodynamic insight-oriented (hypnosis)
eating disorders (definition)
persistent disturbances in eating behavior that impair health and daily functioning
maintained by…
distorted beliefs about weight/shape
emotional processes
powerful reinforcement loops
who is most affected by eating disorders?
anorexia nervosa
age onset : 16-20
U.S. lifetime prevalence : 0.9% women, 0.3% men
bulimia nervosa
age onset : 20-24
worldwide prevalence : 1%
U.S. : 1.5% women, 0.5% men
binge-eating disorder
age onset : 30-50
worldwide prevalence : 2%
U.S. : 3.5% women, 2% men
eating disorder (gender statistics)
approximately 3:1 ratio
high risk male subgroups : gay/bisexual men, wrestlers, jocks
*men often missed because concerns may focus on masculinity and overexercising rather than thinness
anorexia nervosa (definition, criteria)
definition
relentless pursuit of thinness leading to a significantly low body weight
criteria
restriction of energy intake resulting in a significant low body weight
intense fear of gaining weight or becoming fat
disturbance in weight / shape perception
anorexia nervosa (symptoms)
significant weight loss
dry, brittle hair and nails
feeling cold all the time
dizziness, fatigue, low energy
counting calories and/or dieting
saying they’re fat
exercising a lot
using laxatives and diuretics
anorexia nervosa (subtypes)
restricting type — extreme limitation of food intake
tight caloric control, slow eating, cutting food into tiny pieces, hiding/disposing food
binge-eating/purging type — in addition to restriction, includes bingeing and/or purging behaviors
purging includes vomiting, laxatives, diuretics, and enemas
compensatory exercise and fasting
anorexia nervosa (clinical presentation)
deny serious problem; fulfillment rather than alarm
thinness concealed
weight shape over-evaluation can persist even when body is severely compromised
anorexia nervosa (treatment)
re-feeding/weight restoration (can require hospitalization, intensive nutritional control, intravenous feeding)
family therapy for adolescence (Maudsley Model) works through phases of re-feeding→negotiation of new relationships→termination
antidepressants do NOT work
Maudsley Model
bulimia nervosa (definition, critera)
definition
recurrent episodes of binge eating (usually an unusually large amount of food in a short time with a loss of control)
inappropriate compensatory behavior (self induced vomiting, misuse of laxatives, fasting, or excessive exercise)
occurs at least once a week over 3 months
bulimia nervosa (clinical presentation)
typically normal weight range or slightly overweight
accompanied by feelings of shame and guilt
bulimia nervosa (risk factors)
thinness-focused settings (ballet, gymnastic, figure skating)
incredibly culturally bound
thin-ideal exposure, abundant food, private purging
greater exposure to Western media
bulimia nervosa (treatment)
CBT is the leading treatment involved in bulimia nervosa
CBT
meal planning
nutritional education
regularizing eating to disrupt bing/purge cycle
CBT
challenge all-or-nothing thinking
challenge “good/bad food” rules
challenge hot thoughts
*antidepressants can only reduce binge frequency
binge eating disorder (criteria)
A : recurrent episodes of binge eating characterized by BOTH of the following
eating, in a discrete period of time, an amount of food that is larger than whet most people would in a similar period of time under similar circumstances
a sense of lack of control over eating during the episode
B. the binge eating episodes are associated with 3+ of the following
eating much more rapidly than normal
eating until feeling uncomfortably full
eating large amounts of food when not feeling physically hungry
eating alone because of feeling embarrassed by how much one is eating
feeling disgusted with oneself, depressed, or very guilty afterward
C. marked distress regarding binge eating
D. occurs at least once a week for 3 months
*not associated with compensatory behavior
binge eating disorder (comorbidity)
Depression
68% anorexia nervosa
63% bulimia nervosa
OCD : common
Personality Disorders
58% of woemn
Substance abuse : frequently co-occurs in binge eating/purging subtypes
binge eating disorder (socio-cultural factors)
media and culture
exposure to western media, media in general (attitudes toward thinness)
internalization of thin idea
belief that thinness equals beauty and success
social comparison and peer evaluation
family influence
families exhibit rigid attitudes, high expectations, an focus on dieting
parental preoccupation with appearance
binge eating disorder (biological factors)
genetics
relatives of people with anorexia nervosa show 11.4x risk
relatives of people with bulimia show 3.7x risk
twin studies indicate anorexia and bulimia as heritable
serotonin
EDs may relate to serotonergic disruption
serotonin helps regulate mood, appetite, impulsivity, feeding behavior
reward sensitivity
food restriction may make anoretic cues more rewarding
patients with anorexia nervosa show greater reward-area activity to thin models
set points
body resists weight change through physiological “set point” pressures
binge eating disorder (risk factors)
perfectionism portrayed
bodily dissatisfaction
negative emotionality
being female and internalizing the thin ideal
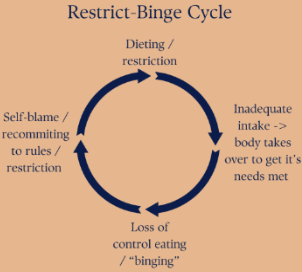
restrict-binge cycle