med surg 3
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
Kidney/urinary system changes associated with aging
cortical tissue loss and smaller nephrons
reduced blood flow to kidneys
decreased tubule length
decreased GFR
nocturia
risk for dehydration
tendency to retain urine
weakened urinary sphincters and shortened urethra in women
Factors contributing to UTI
obstruction
stones
vesicoureteral reflux
DM
urine concentration/pH
gender
age
sexual activity
recent use of abx
virulence factors
Key features of Chronic Pyelonephritis
hypertension
inability to conserve sodium
decreased ability to concentrate urine
development of hyperkalemia and acidosis
Kidney issues, geriatric considerations
normal decline with aging (renal blood flow less than 10%/10 yrs)
concentrate urine less
decreased ability to excrete drugs including contrast/dyes
comorbidities (diabetes, htn)
prescribed meds
Chronic kidney disease (CKD) changes
metabolic changes
cardiac changes
hematologic and immunity changes
GI changes
cognitive and functional changes
CKD changes; metabolic
fluid and electrolyte balance is disrupted
acid-base balance is disrupted
CKD changes; cardiac
htn
hyperlipidemia
heart failure
pericarditis
CKD clinical manifestations
Hemodialysis nursing care
drugs
postdialysis assessment
htn
headache
nausea, vomiting
malaise, dizziness
muscle cramps/bleeding
Complications of Peritoneal Dialysis
peritonitis
pain
exit site/tunnel infections
poor dialysate flow
other complications
Risk for dehydration in renal issues due to…
lowering of concentration of urine
GFR normal values
90-120
60 for those 40+ yrs old
Serum creatinine value
males - 0.6-1.2 mg/dL
females - 0.5-1.1 mg/dL
increased levels means kidney impairment
decreased levels means decreased muscle mass
BUN value
10-20 mg/dL (older adults higher)
increased level means liver/kidney disease, dehydration or decreased kidney perfusion, high protein diet, infection, stress, steroid use, and GI bleeding
decreased level means malnutrition, fluid volume excess, or severe hepatic damage
BUN/creatinine ratio value
6-25
increased ratio means fluid volume deficit, obstructive uropathy, catabolic state, or high protein diet
decreased ration means fluid volume excess
We avoid ____ with CT contrast
metformin and shellfish
Assessing a pt undergoing kidney test/procedures with contrast
allergies?
asthma?
hay fever?
metformin?
assess renal status and hydration status
Factors contributing to urinary incontinence
drugs
disease
depression
inadequate resources
Drugs, urinary incontinence
CNS depressants/opioids - decrease pts LOC and urge to void → constipation
diuretics - frequent/large amounts of urine
multiple drugs - change in mental status or mobility, can irritate bladder
anticholinergic - affect both cognition and ability to void
disease, urinary incontinence
stroke, parkinsons, dementia, and other neuro disorders decrease mobility, sensation, or cognition
arthritis - decreases mobility and causes pain
depression, urinary incontinence
decreases the energy necessary to maintain continence
decreased self-esteem and feelings of self-worth decrease the importance to the pt of maintaining continence
inadequate resources, urinary incontinence
pts who need assistive devices may be afraid to ambulate w/o them
products the help manage incontinence are costly
no one may be available to assists them
60% of women ages…
65+ have incontinence
Urodynamic testing
seeing how much a pt can hold in before having to go
Types of incontinence
stress
urge
mixed
overflow
functional
Stress incontinence
involuntary loss of urine during activities that cause that increase abdominal and detrusor pressure; inability to tighten urethra
most common
Stress incontinence management
weight reduction
smoking cessation
pelvic muscle therapy
vaginal cone therapy
bladder training
estrogen therapy
electrical stim
magnetic resonance therapy
pessary devices
surgery
Urge incontinence
overactive bladder; involuntary loss of urine associated with a strong desire to urinate; inability to suppress the signal from the bladder muscle to the brain that it is time to go
Urge incontinence management
bladder therapy
pelvis muscle therapy
weight reduction
avoid bladder irritants (caffeine, alcohol)
smoking cessation
drug therapy
electrical stim
surgery
Mixed incontinence
combination of stress and urge incontinence
same management as urge/stress
Overflow incontinence
involuntary loss of urine associated with overdistention of the bladder when bladder capacity has reached its max; detrusor under activity, bladder outlet obstruction
Overflow incontinence management
bladder training
bladder compression
intermittent self-cath
drug therapy
nonsurgical treatment unless needed
Functional incontinence
leakage of urine caused by factors other than disease of the lower urinary tract
Functional incontinence management
habit training
prompted voiding is used to establish a predictable pattern
devices → intravaginal pessaries, penile clamps, condom cath
intermittent/long-term cath
Ways to prevent a UTI
drink 2-3L of fluid daily
get enough sleep and nutrition daily (better immune health)
change from spermicide use
avoid routinely delaying urination
Manage CAUTIs
maintain good hygiene during insertion and manipulation of cath
insert cath for appropriate use only
ensure properly trained personnel insert and maintain cath
routinely clean periurethral area
leave in only as long as needed
maintain unobstructed urine flow
secure cath to thigh/abd to avoid friction
consider alt to indwelling caths
Hydroureter
swollen ureter due to backup of urine
Hydronephrosis
one or both kidneys swell, urine doesn’t fully empty from body
how frequent for chronic pyelonephritis
two a year
CRP (c-reactive protein)
lab that shows inflammation
Hyperkalemia causes…
heart problems
Collaborative management example
having to deal with with both kidney damage and hypertension
MAP
60-75
Renal diet
lower protein since kidneys cannot manage it as well
What we assess in dialysis pts fistulas
thrill - feel woosh
bruit - hear woosh
if these are missing it means there is a clot → medical emergency
Dialysis disequilibrium syndrome
result of a rapid reduction in electrolytes; characterized by mental status changes and can include seizures or coma
Drain bag from dialysis should be…
clear, if it is cloudy there may be an infection
Lab assessments before surgery
urinalysis
blood type/screen
CBC or hemoglobin/hematocrit
clotting studies (PT, INR, aPTT)
electrolyte levels
serum creatinine level
pregnancy test
chest xray
ecg
Informed consent
surgeon obtains signed consent before sedation and/or surgery (risks and benefits)
nurse witness for speaking to the surgeon and that the pt is alert and oriented
nurse not responsible for providing detailed info about procedure
telephone requires two nurses
special permits - contrast/blood/MRI/implants
pt self-determination - only the pt can sign unless they are incapacitated, next of kin
older adults surgical risk
decreased
cardiac output, peripheral circulation
vital capacity, blood oxygenation
blood flow to kidneys, GFR
increased
BP
risk for skin damage, infection
sensory deficits
deformities related to osteoporosis/arthritis
Pts at risk for VTE
obese
40+
history of cancer or decreased CO
decreased mobility, immobile, spinal cord injury
history of VTE, PE, varicose veins, edema
oral contraceptives
smoking
hip fracture, total hip/knee surgery
PACU respiratory assessment
patent airway, adequate gas exchange
note artificial airway
rate, pattern, depth of breathing
breath sounds
accessory muscle use
snoring and stridor
respiratory depression or hypoxemia
Preventing wound infection
dressings - first change done by surgeon
drains - provide exit route for air, blood, bile
incision - well approximated
drug therapy, irrigation to treat wound infection
debridement
surgical management
Elective surgery
chose to
Emergent surgery
don’t need consent, two doctors musts say it is an emergency
Malignant hyperthermia
allergy; genetic factor that causes a pt to not be able to metabolize gases (anesthesia) the same and they could die
Common when waking up from anesthesia
puking, crying, swinging
Medicine and cardiac clearance
primary doctor assesses pt and labels if they are at risk for anesthesia
Urinanalysis checks for preoperative care
renal function and infections
CBC/WBC checks for in preoperative care
infection
Hemoglobin/hematocrit checks for in preoperative care
other issues if there is no sign of infection
Electrolyte levels check for in preoperative care
sodium and potassium
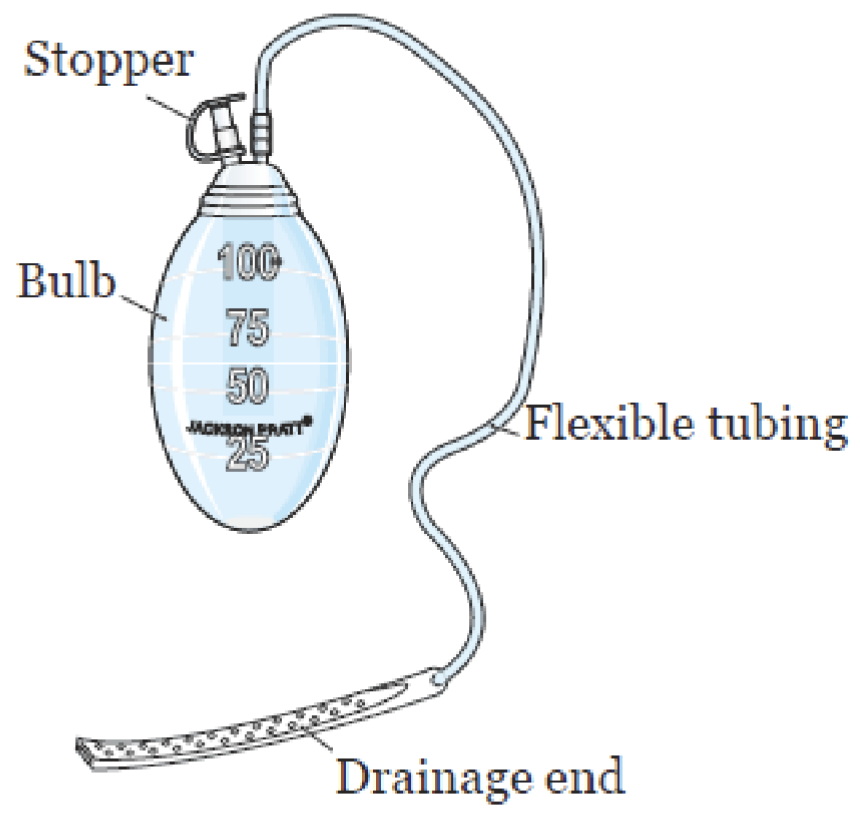
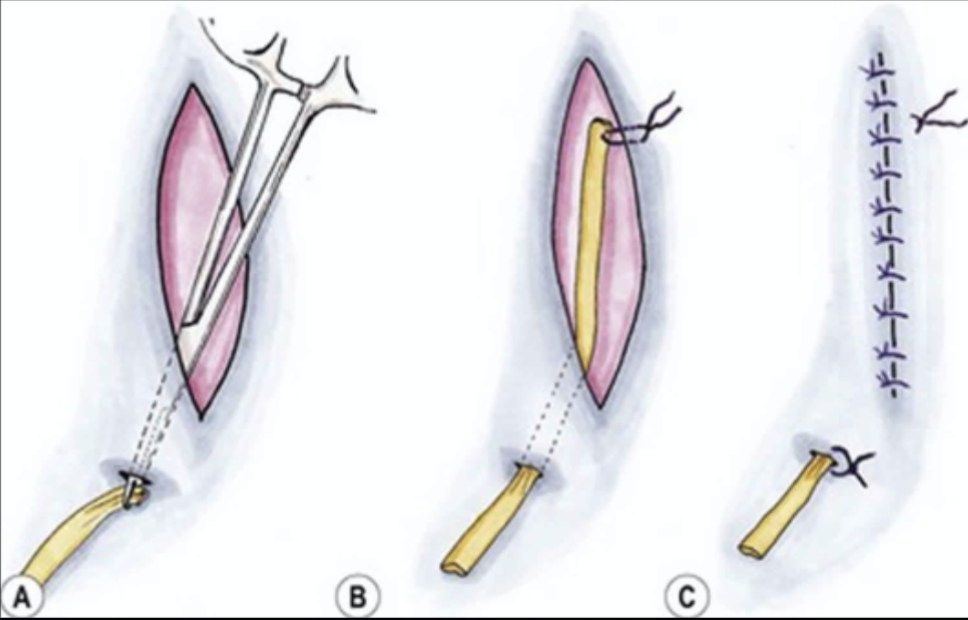
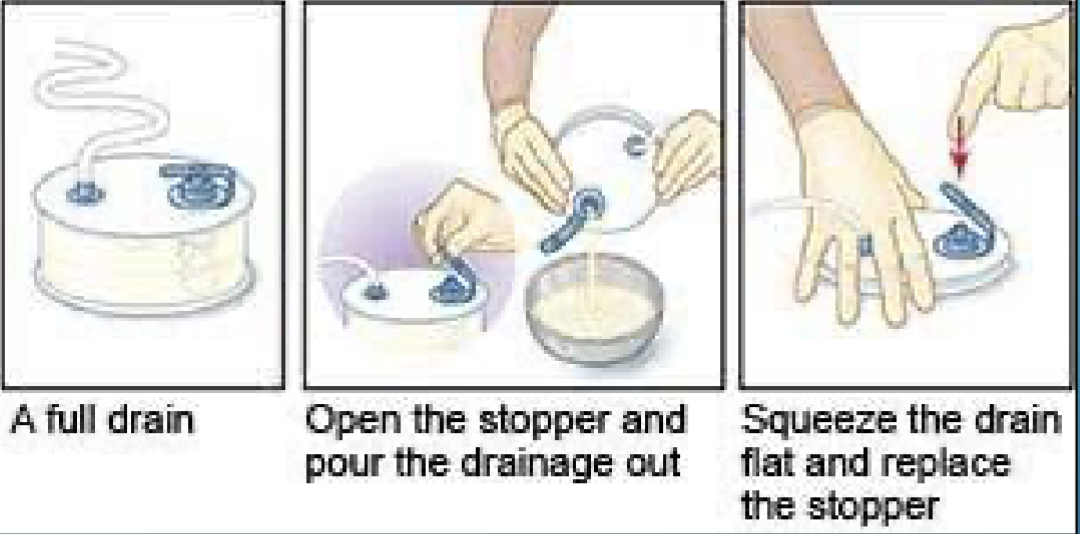
JP drain
used to collect drainage from wound when bulb is squeezed drawing out the fluid
Pen rose
used for a site with a small amount of drainage, a tube that allows fluid to seep in and drain out, with gauze catching it
Hemovac
used for larger surgeries due to more drainage room, vacuum pressure by remaining collapsed to pull fluid out
measure drainage by pouring it into a container
Serous drainage
clear, yellow; normal in early stages of the healing process
Sanguineous drainage
bright red, bloody; common right after a surgery (24-48hrs) but should decrease
Serosanguineous drainage
pinkish; normal transition from sanguineous to serous in would healing
Atelectasis
common during anesthesia and postop; partially lung collapse that could lead to infection and other respiratory complications
How can pain affect a pts condition after surgery?
it could make them not want to move which increases the chance for clots and have shallow breaths which could cause atelectasis or pneumonia
Diabetic ketoacidosis
hyperglycemia causing hypotension, polyuria, polydypsia, hyperventilation, fruity/acetone breath, tachycardia
Somogyi effect (rebound)
hypoglycemia at night leads to hyperglycemia in the morning
avoid with less insulin at night or a snack
Dawn phenomenon
hyperglycemia in the early morning
avoid by increasing insulin
Type 1 DM
acute onset; polyphagia, polydypsia, polyuria
Type 2 DM
gradual, insidious onset; polys + fatigue, recurrent infections, prolonged wound healing visual changes
Medical management of DM
nutrition therapy, physical activity, surgery (pancreas transplant), medication management
Basal insulin
long acting and type 1 DM can never be off of it
A1C
test measuring the average amount of sugar in your blood over the past few months used to diagnose prediabetes and to monitor treatment plans
Nursing management assessment of DM
blood glucose monitoring
labs
hypo/hyperglycemia
skin integrity
medication adherence
lifestyle
Hypoglycemia signs/symptoms
confusion, irritability, diaphoresis, tremors, hunger, weakness, visual disturbances
Hyperglycemia signs/symptoms
weakness
malaise
visual changes
polys
weight loss
Managing hypoglycemia with an alert and can eat pt
15 gm of quick acting oral CHO, repeat BG in 15 mins
repeat until BG is within normal range, then offer a protein snack
Managing hypoglycemia with a pt who is poorly responsive/unresponsive with no IV access
call rapid response and administer glucagon
Managing hypoglycemia with a pt who is poorly responsive/unresponsive with IV access
call rapid response and administer IV D50