lung volumes, lung capacities, pulmonary function tests
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
difference between volume and capacity
volume — 1 value
capacity — sum of multiple volumes
tidal volume
amount of air trapped and expired during normal breath
400-700 mL/kg
inspiratory reserve volume
additional air a person can inhale after a normal inspiration
includes the tidal volume
expiratory reserve volume
additional air a person can exhale after normal exhalation
residual volume
amount of air remaining in lungs after ERV is expired
“dead air”
1-1.2 L
what happens to residual volume as we age
it increases naturally
dead space
the volume of air within the respiratory system that does not participate in gas exchange
inspiratory capacity
amount of air inspired and expired with normal breathing PLUS the amount of air a person can inspire after normal inspiration
IC = tidal volume + IRV
vital capacity
max volume of air that can be forecully expired after max inspiration
decreases with age
VC = tidal volume + IRV + ERV
functional residual capacity
not limited to but INCLUDES amount of air remaining in lungs after normal passive expiration
FRC = ERV + RV
total lung capacity
max volume of air the lungs can hold
TLC = VC + RV
TLC = IC + FRC
what is the average total lung capacity for men
7 L
what is the average total lung capacity for women
5 L
physiological dead space
anatomical + alveolar dead space
anatomical dead space
the volume of gas contained in the non respiratory conducting airways (no gas exchange)
total volume of air from nose / mouth to terminal bronchioles
~150 ml in healthy people
alveolar dead space
volume of gas in alveolar ventilation with little to no perfusion
referred to as “wasted ventilation”
V/Q mismatch
negligible in healthy population (25-50 mL)
higher in obstructive diseases
pulmonary function tests
non invasive
measure lung volumes, lung capacities, rates of flow
determines restrictive and obstructive, severity, progression
what specific things are measured by PFTs
tidal volume
FEV1
vital capacity
how easily CO2 can diffuse from lungs to bloodstream (DLCO)
spirometry PFT
provides basic lung volumes and ESTIMATES other volumes
open circuit, closed circuit
cheaper and quicker
ESTIMATES RESIDUAL VOLUME
body plethysmography PFT
complete test for all lung capacities and volumes
uses nitrogen and helium
DIRECT MEASURE OF TLC, FRC, RV
DLCO
measures diffusion capacity of carbon monoxide to evaluate alveolar capillary membrane diffusion integrity
(carbon monoxide because hemoglobin has high affinity for it)
FEV1 (forced expiratory volume in 1 second)
should be 80-120% normal value
FVC (forced vital capacity)
max volume expired as rapidly as possible after max inspiration
should be 80-120% normal value (4-5 L is norm)
FEV1 / FVC ratio based on predicted values
age
biological sex
height
weight
ethnicity
FEV1/FVC ratio based on absolute value
norm is 0.8
0.85 if children not fully grown
0.7 is lower limit of normal
GOLD 1 stage of COPD (mild)
FEV1 % of predicted >/= 80
GOLD 2 stage of COPD (moderate)
FEV1 % of predicted 50-79
GOLD 3 stage of COPD (severe)
FEV1 % of predicted 30-49
GOLD 4 stage of COPD (very severe)
FEV1 % of predicted <30
what GOLD stage do PTs normally see people in
GOLD stage 2 (FEV1 % predicted of 50-79)
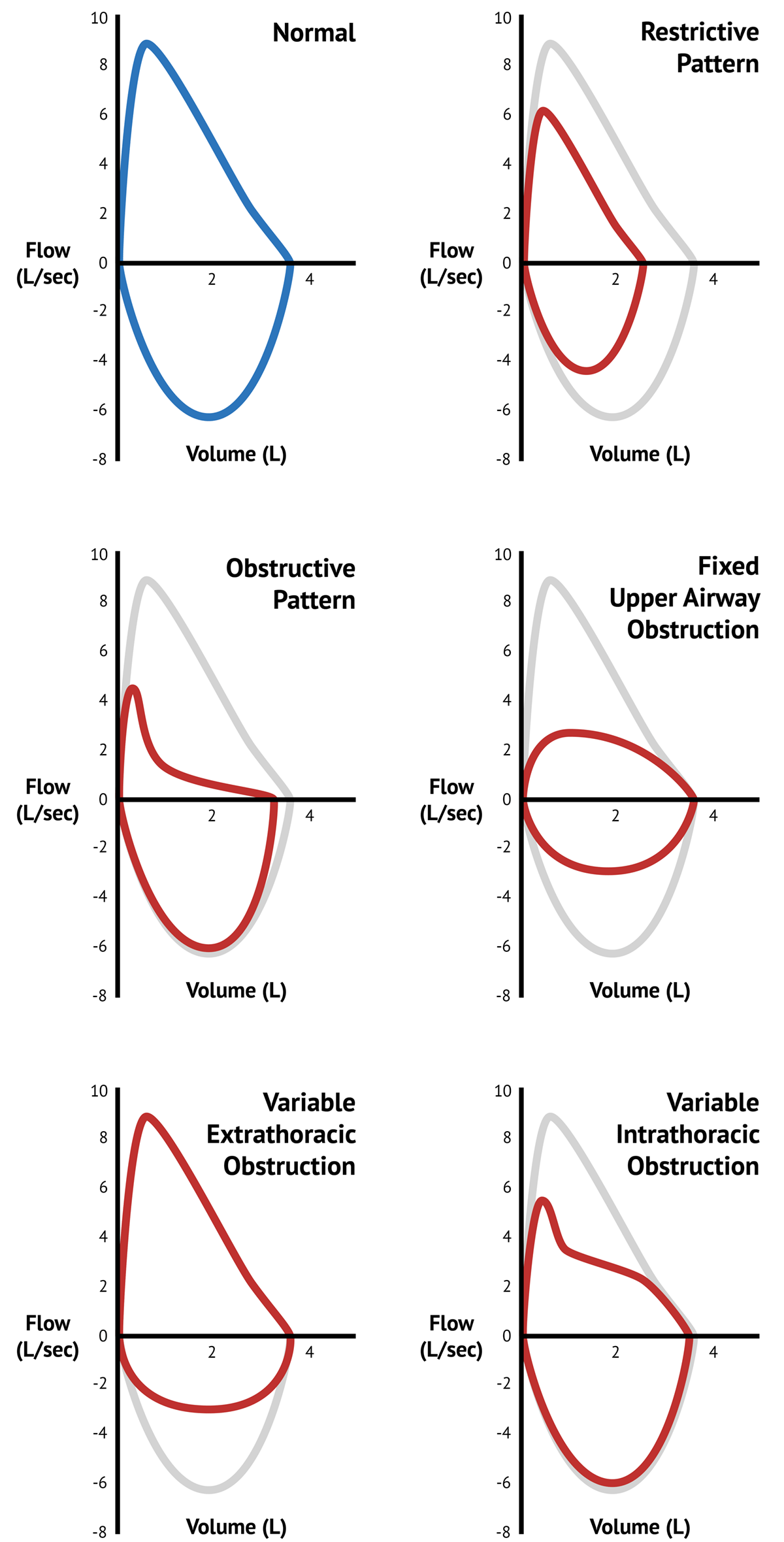
flow loop graph
shows what happens with forced inspiration and forced expiration
what happens to the flow loop graph in restrictive diseases
entire loop is shrunk
“shrunken egg”
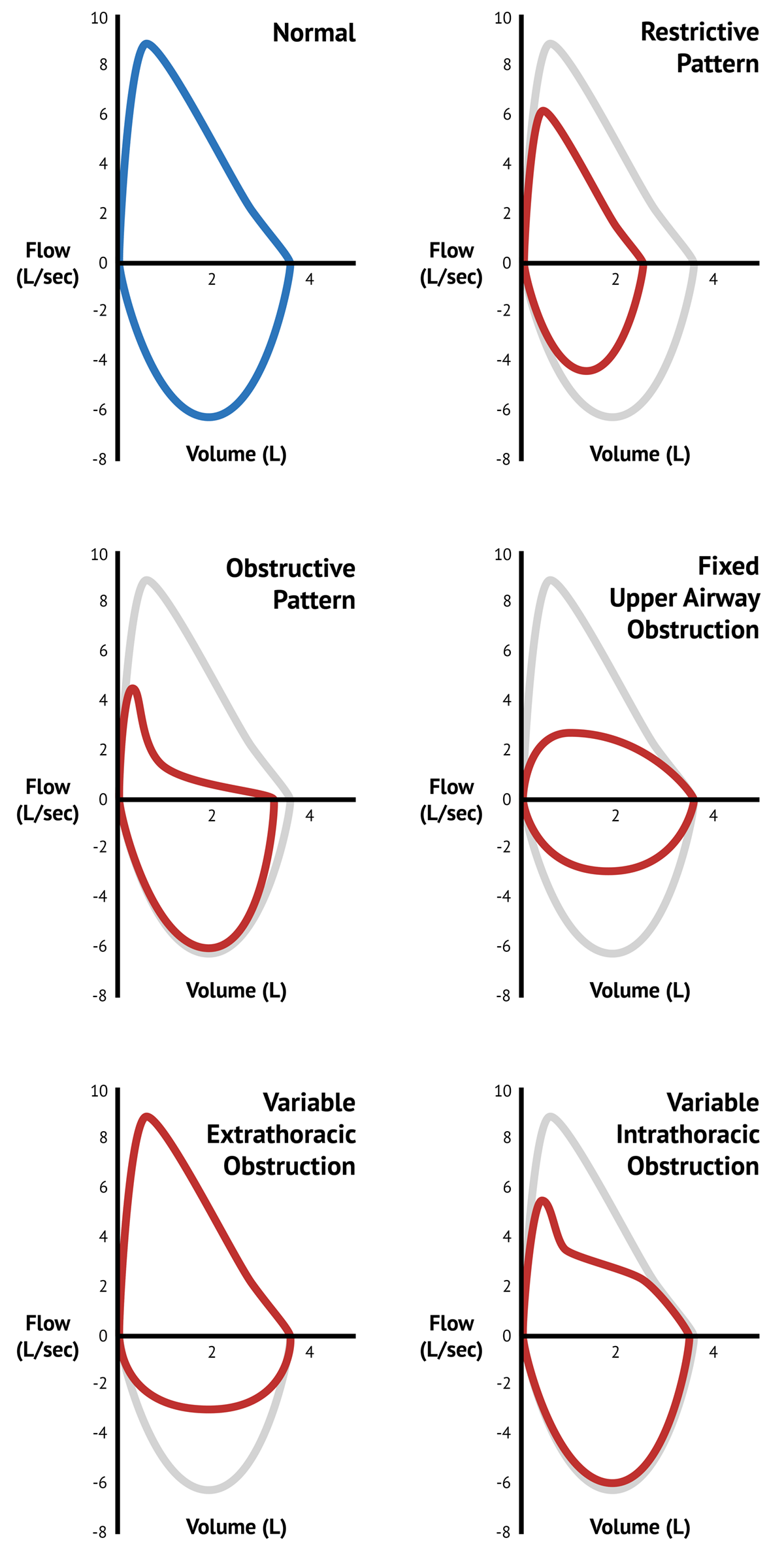
what happens to the flow loop graph in obstructive diseases
“scooped out”
if FEV1 increases by 12% or more, the FVC increases by 200 ml or more, or there is a 15% increase in FEF 25-27, what does this tell us
the disease is reversible
FEF 25-27%
forced expiratory flow volume from point 25% to 75% of FVC has been exhaled
used to capture medium to small airways
differential diagnosis for asthma and smokers
maximum voluntary ventilation
max breathing capacity at rest x 1 min (L/min)
patient pants as fast and deep as possible for 15 seconds
indicates inspiratory muscle strength at max exertion
what happens when minute ventilation = max voluntary ventilation
there is no reserve
VERY DANGEROUS
what type of disorder does an FEV1/FVC ratio of >0.7 indicate
restrictive
what type of disorder does an FEV1/FVC ratio of <0.7 indicate
obstructive
what should you do if a patient’s FEV1/FVC ratio is >0.7
they likely have a restrictive disorder:
evaluate FVC and TLC
evaluate DLCO
what should you do if a patient’s FEV1/FVC ratio is <0.7
they likely have an obstructive disorder:
grade severity with GOLD criteria
check reversibility (>12% — asthma, <10% — COPD)